
Evolution of Bioamplifiers: From Vacuum Tubes to Highly Integrated Analog Front-Ends

 ,
, 
Abstract
:1. Introduction
- (1)
- Demands of diagnostics in clinical practice;
- (2)
- Technical capabilities for recording, processing, and analyzing signals in analog and digital forms;
- (3)
- Possibilities of using computer technologies.
- Transistors (bipolar and field effects): Ross patented a metal oxide semiconductor (MOS) transistor in 1955.
- Integrated operational amplifiers: Planar integrated circuit technology appeared in a patent from Fairchild Semiconductor in 1959 (R. Noyce) [11], as well as MOS integrated circuit in 1962 (S. R. Hoffstein), and the first commercial integrated monolithic operational amplifier uA702 based on planar technology was sold in 1964.
- Integrated instrumental amplifiers;
- Integral analog and analog-to-digital front-end chip (analog front-end (AFE)).
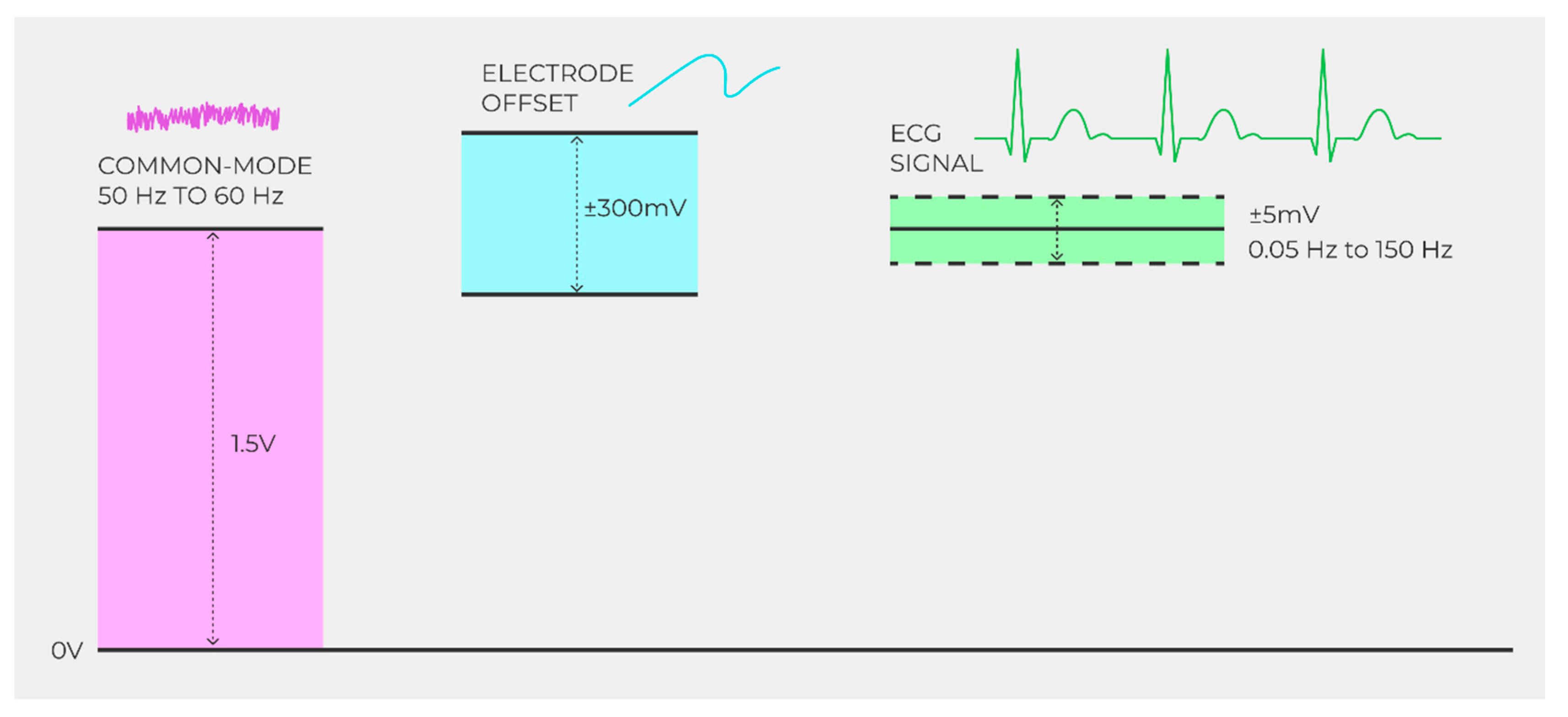
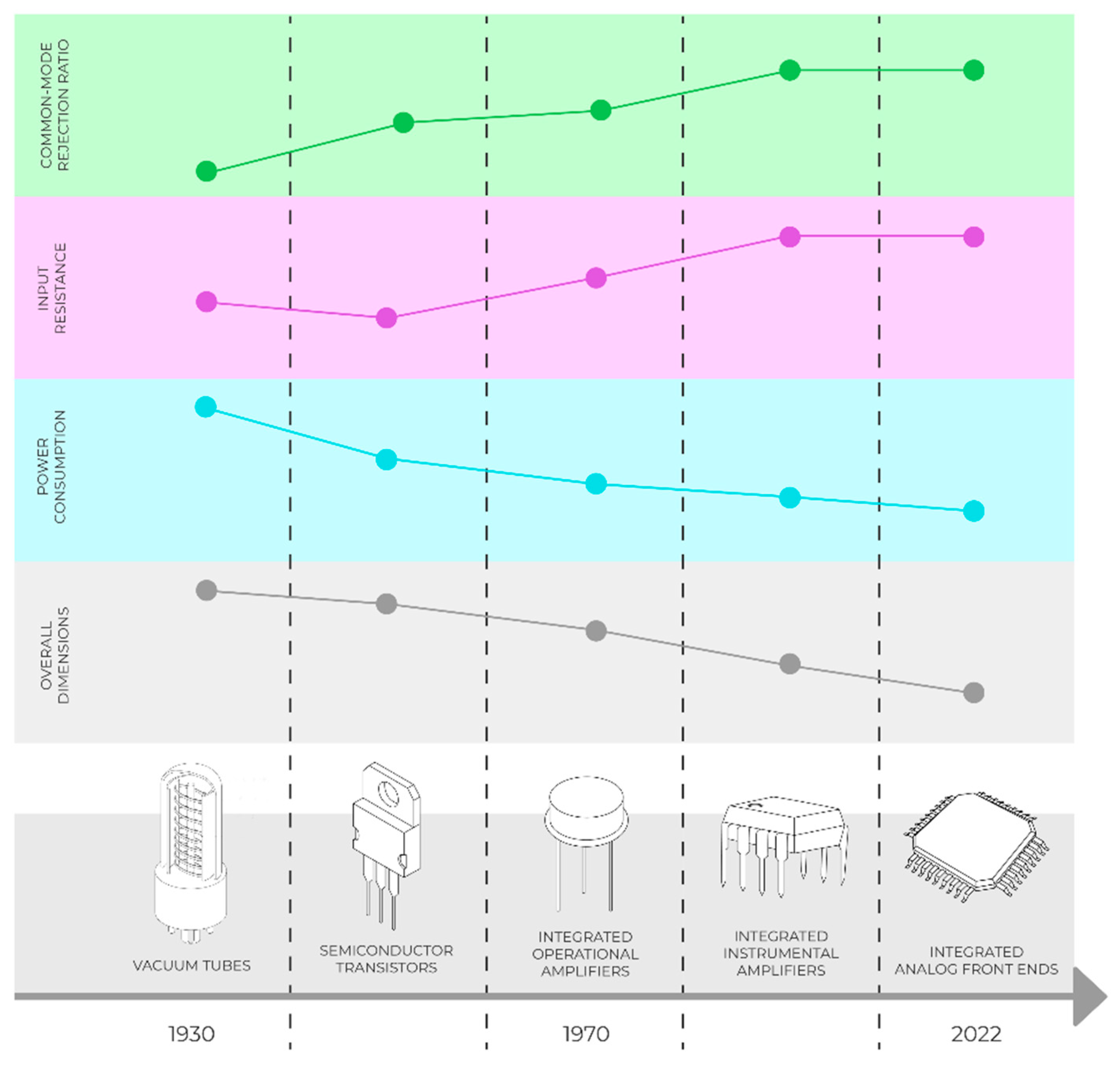
- Increasing the common mode rejection ratio (CMRR) (50 or 60 Hz of noise, namely high-frequency noise)
- Increasing the bioamplifier input resistance (due to the rather high resistance of the electrode–skin system);
- Reduction of power consumption (which is especially important for portable devices);
- Reducing the mass size of bioamplifiers;
- Expansion of functional capabilities;
- Improvement of operational properties.
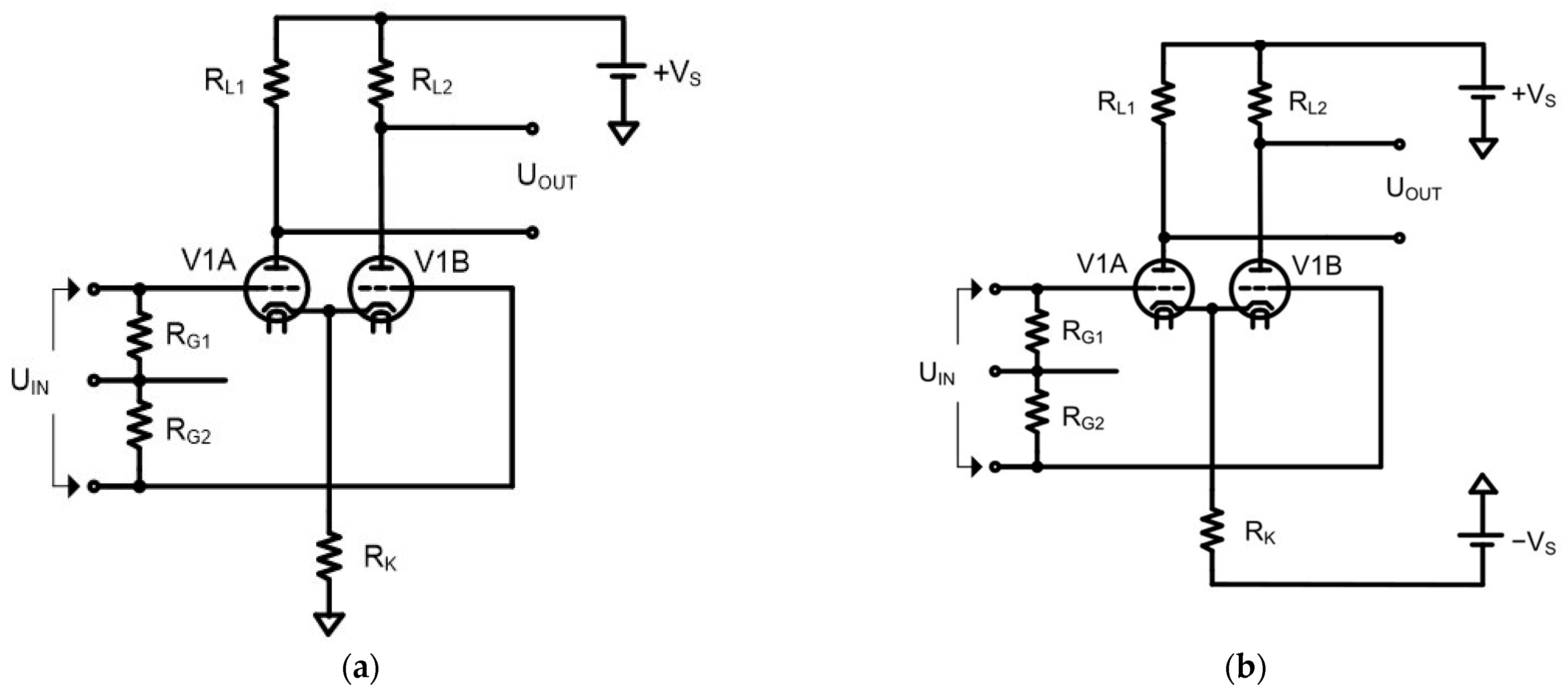
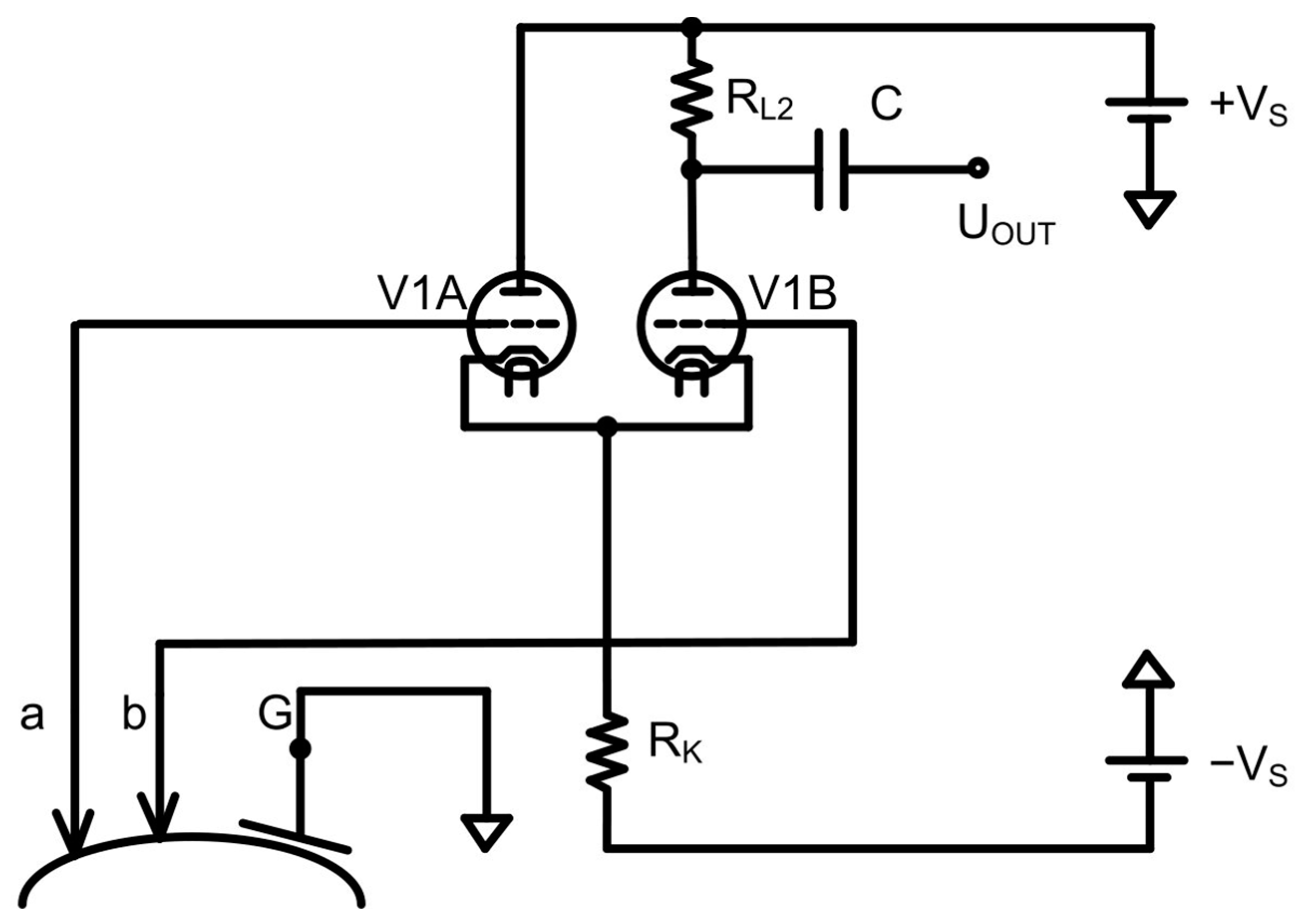
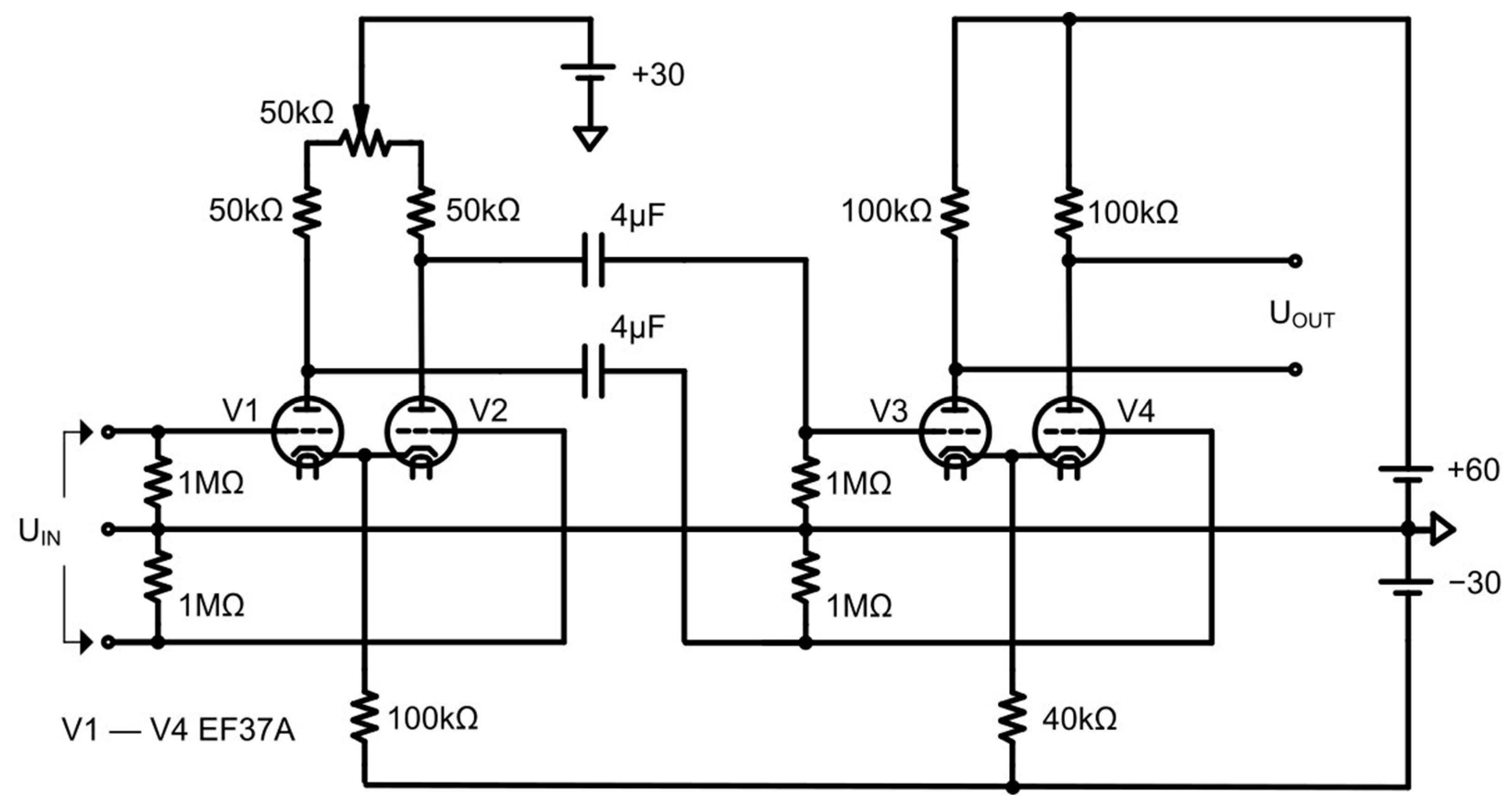
2. Bioamplifiers in Vacuum Tubes
- They require a high anode supply voltage and high external power supply from the line voltage;
- Insufficient noise immunity is caused by the fact that the passive electrodes are remote from the amplifier unit.
- Insufficient suppression of common-mode noise owing to variation in the parameters of the tubes of the input stages;
- The input impedance of the preamplifier is rather small (about MOhms).
3. Discrete Semiconductor Transistor-Based Bioamplifiers (Bipolar and Field)
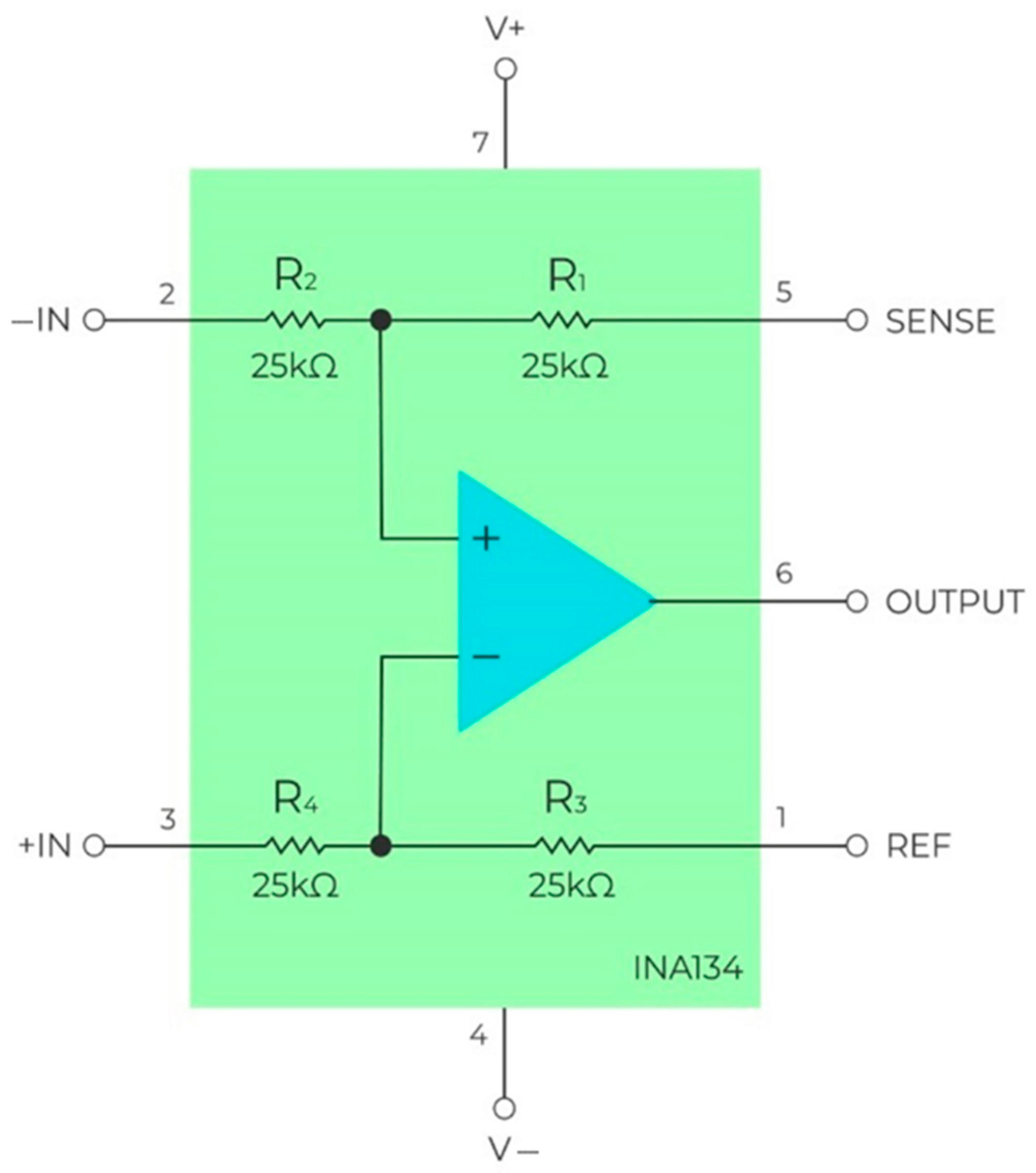
4. Bioamplifiers on Monolithic Integrated Operational Amplifiers
- If TR = 1%, the worst-case CMRR value is 34 dB.
- If TR = 0.1%, the worst-case CMRR value is 54 dB.
- High common mode rejection ratio;
- High thermal stability of input cascades;
- Small nonlinear distortions of the input signal;
- A wide range of supply voltage variation;
- Low power consumption from the power supply.
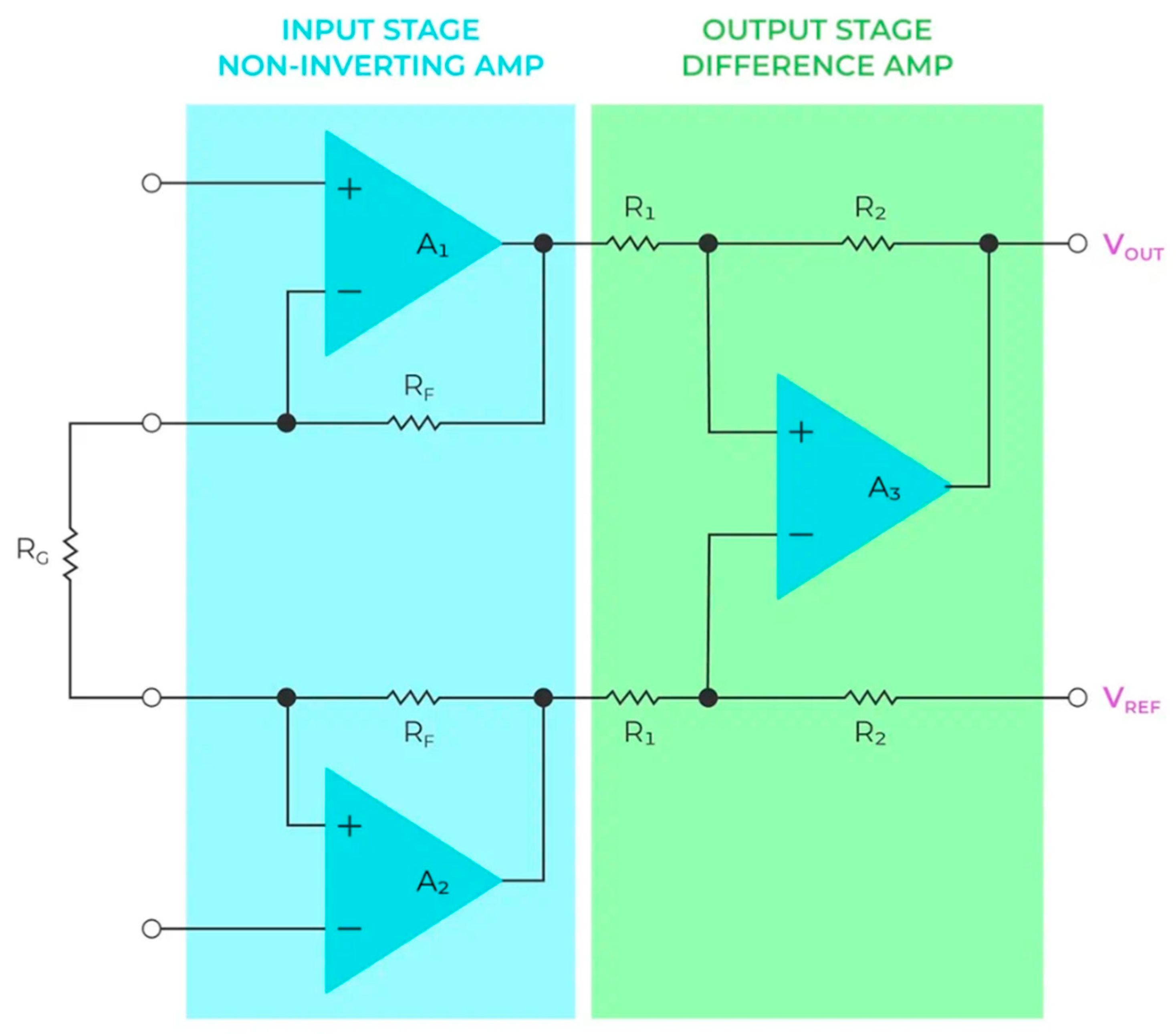
5. Bioamplifiers on Monolithic Instrumentation Amplifiers
6. Bioamplifiers on Integrated Analog Front-Ends
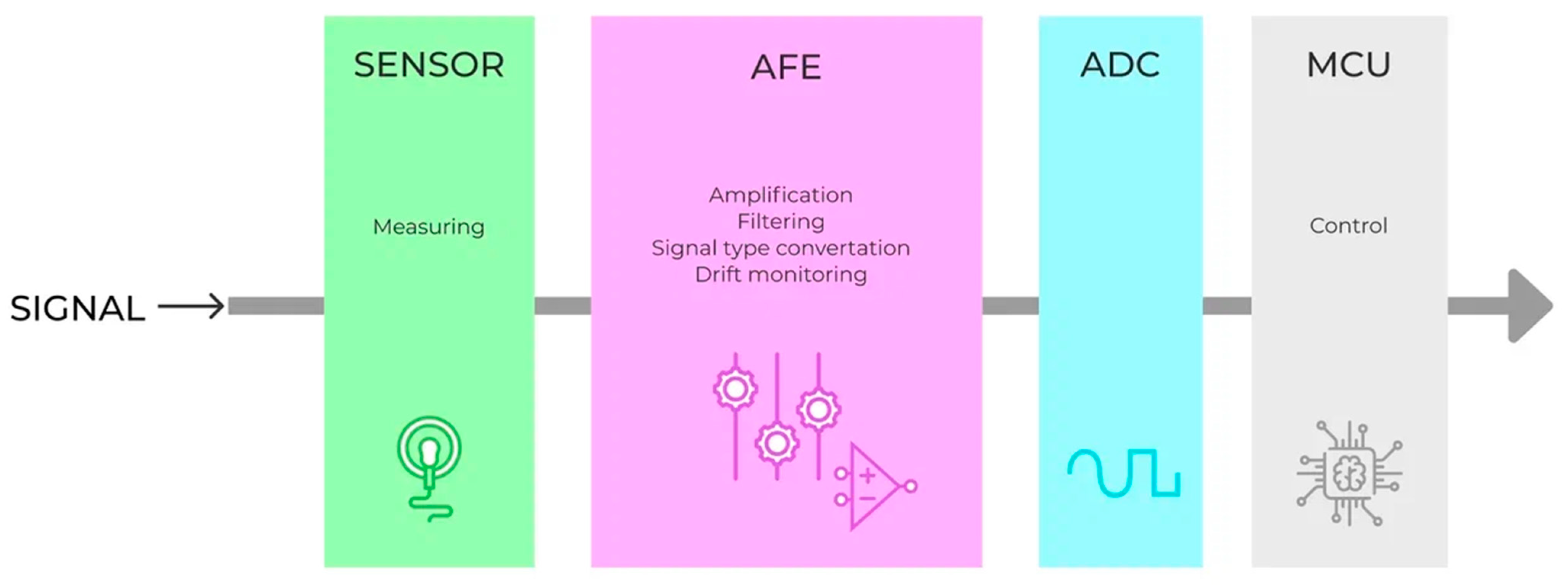
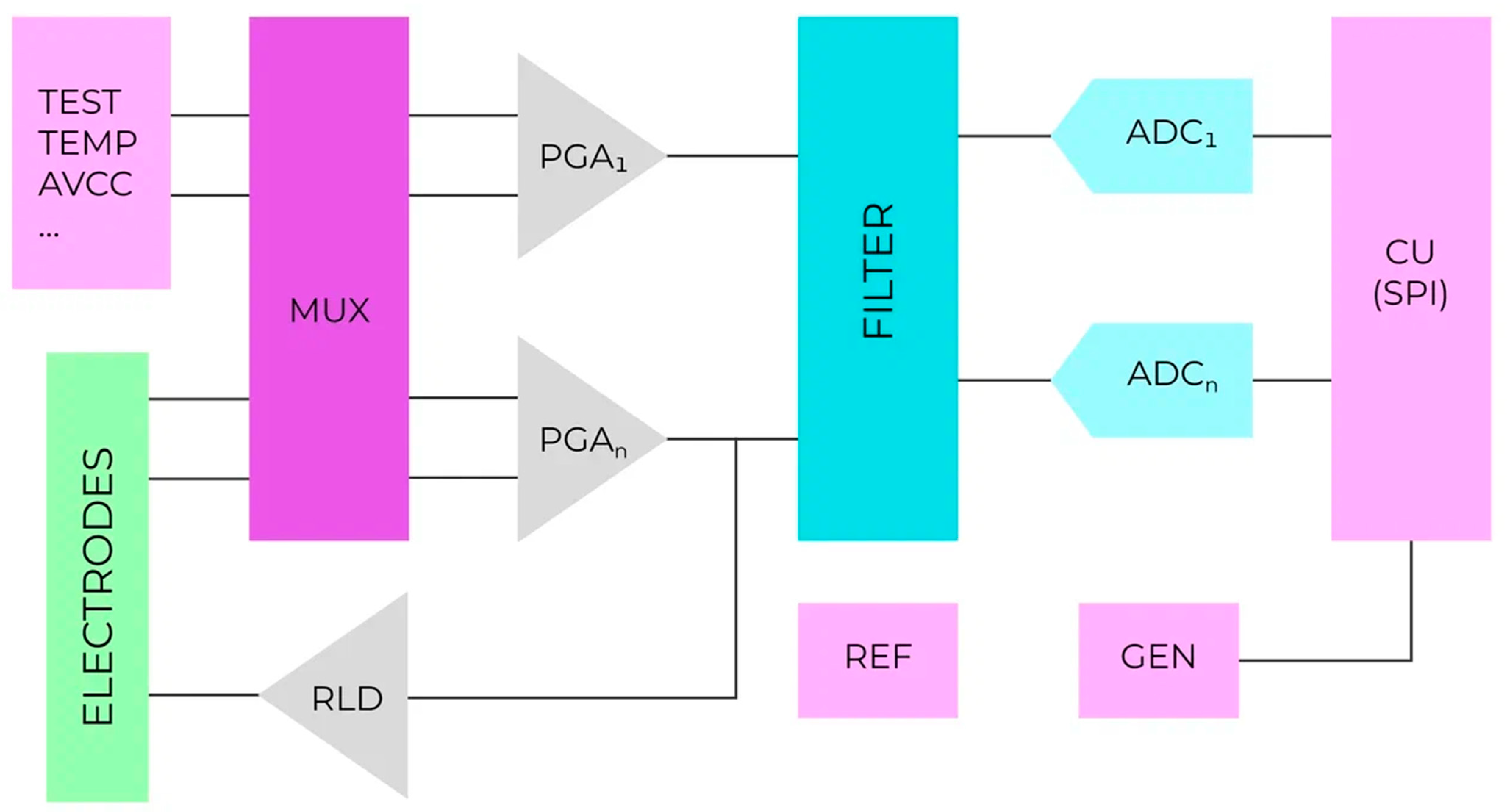
6.1. Basic Information about Integrated Analog Front-Ends
- -
- Analog units (operational amplifiers, comparators, filters, etc.) are required to convert and preprocess the input analog signal.
- -
- Analog-to-digital and digital-to-analog converters;
- -
- A digital interface to transmit data and control the entire system;
- -
- Power subsystem (linear voltage converter, reference voltage source, battery charging circuit, and power supply supervisor).
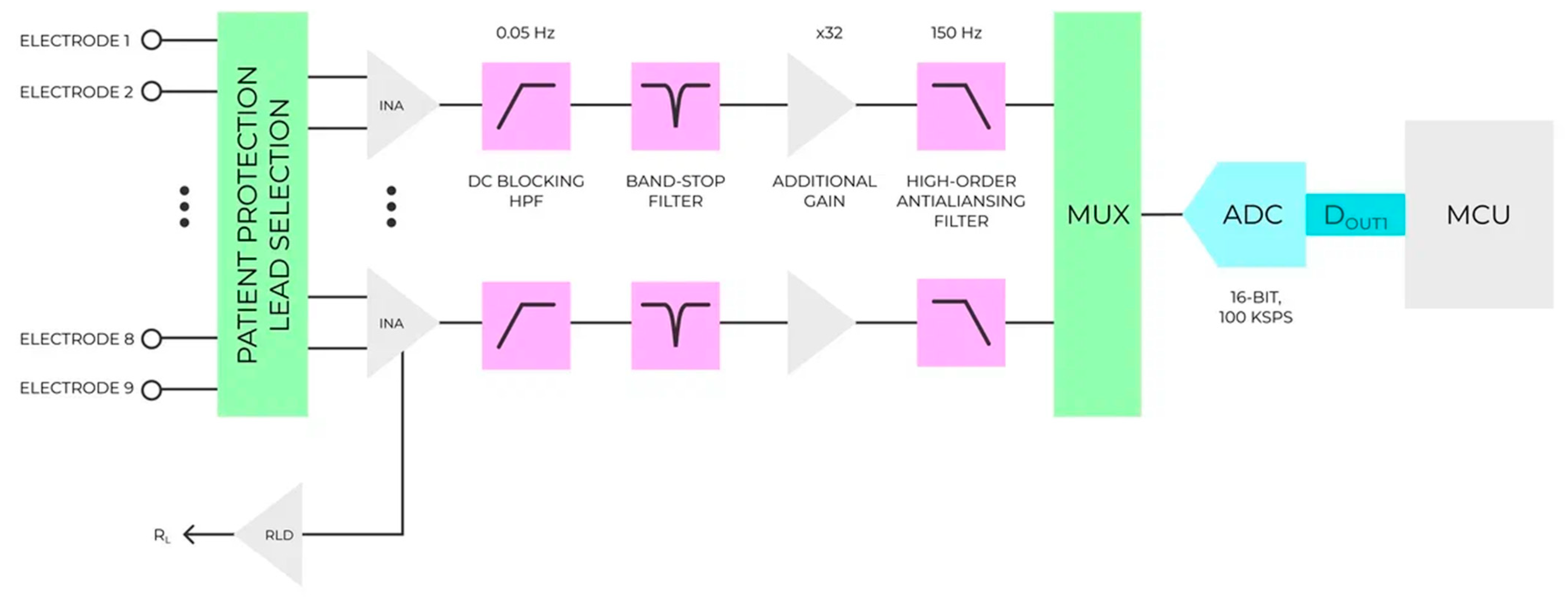
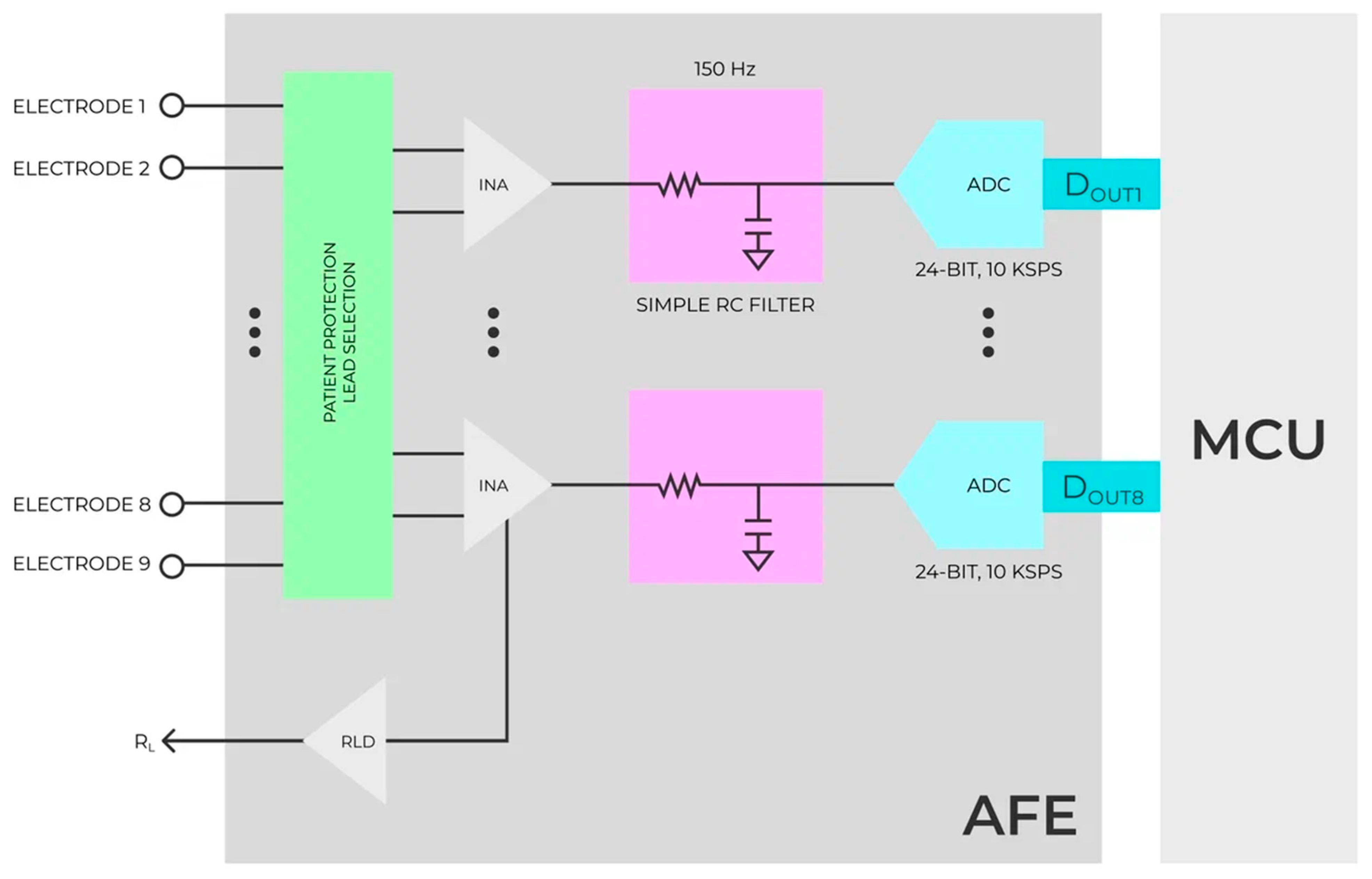
6.2. Analog Front-End Solutions for Biopotencia: Registration
- Changing the sampling rate for each of the signal registration channels;
- Changing the amplification factor of the input signal;
- Changing the cutoff frequency of built-in high-frequency filters
- Changing the analog-to-digital conversion bit rate.
6.3. AFEs on the Market
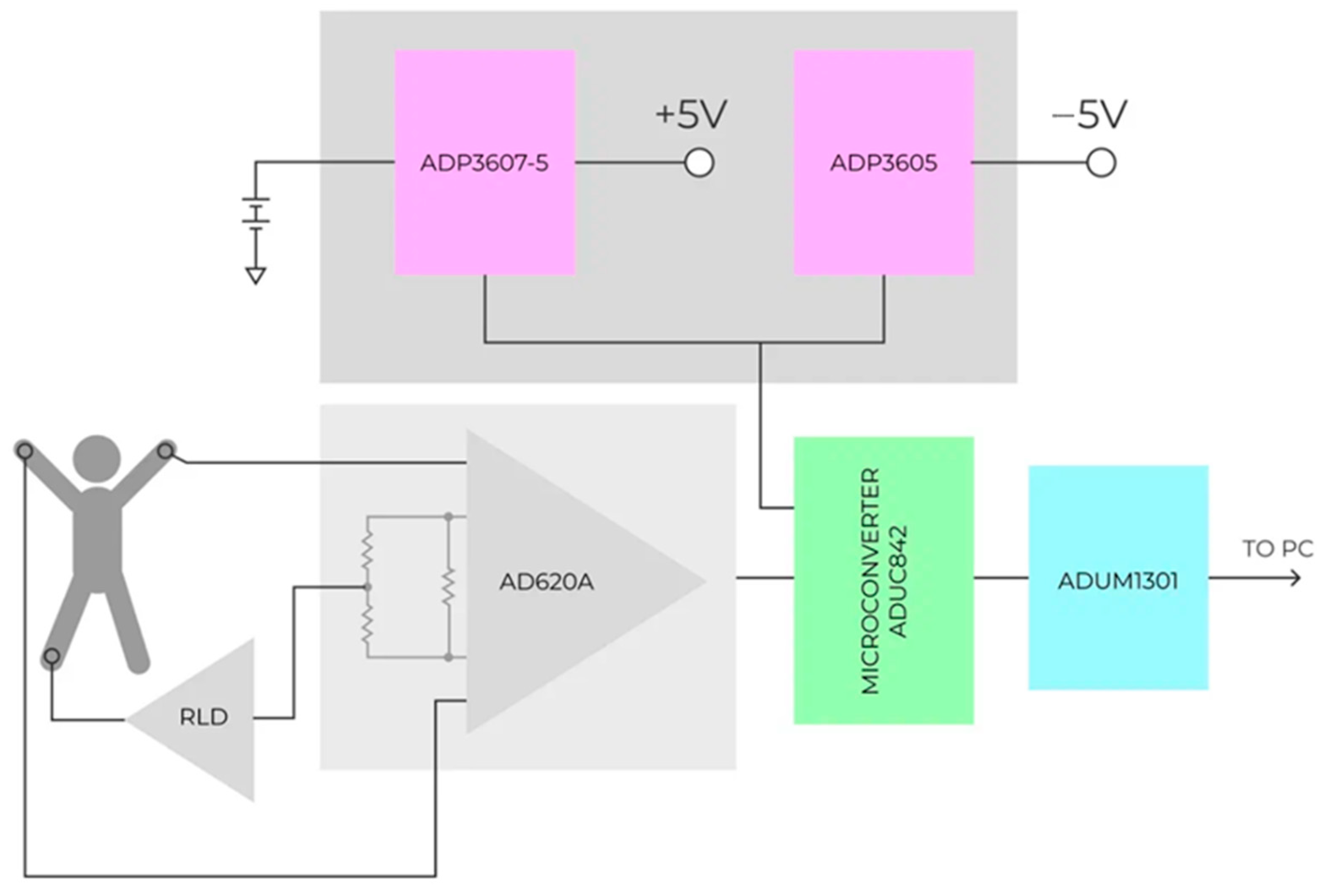
7. Implementation of AFEs in Real Applications
7.1. Articles Overview and Statistics
7.2. Application of AFEs for ECG Registration
7.3. Application of AFEs for EEG Registration
7.4. Application of AFEs for EMG Registration
7.5. Application of AFEs for EOG Registration and Special Purposes
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cajavilca, C.; Varon, J.; Sternbach, G.L. Luigi Galvani and the foundations of electrophysiology. Resuscitation 2009, 80, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Barold, S.S. Willem Einthoven and the Birth of Clinical Electrocardiography a Hundred Years Ago. Card. Electrophysiol. Rev. 2003, 7, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Thakor, N.V. Bipotentials and Electrophysiology Measurement; Johns Hopkins School of Medicine: Baltimore, MD, USA, 2000. [Google Scholar]
- Caceres, C.A.; Dreifus, L.S. Clinical Electrocardiography and Computers; Academic Press: New York, NY, USA; London, UK, 1970. [Google Scholar]
- Tompkins, W.J.; Webster, J.G. Design of Microcomputer-Based Medical Instrumentation; Prentice-Hall, Inc.: Englewood, NJ, USA, 1981. [Google Scholar]
- GOST 60601-2-51-2008; Medical Electrical Equipment—Part 2-51. Particular Requirements for Safety, including Essential Performance, of Recording and Analyzing Single Channel and Multichannel Electrocardiographs. Standardinform: Moscow, Russia, 2009.
- IEC 60601-2-25:2011; Medical Electrical Equipment—Part 2-25: Particular Requirements for the Basic Safety and Essential Performance of Electrocardiographs. IEC: Geneva, Switzerland, 2011.
- Kligfield, P.; Gettes, L.S.; Bailey, J.J.; Childers, R.; Deal, B.J.; Hancock, E.W.; Van Herpen, G.; Kors, J.A.; Macfarlane, P.; Mirvis, D.M.; et al. Recommendations for the Standardization and Interpretation of the Electrocardiogram. Circulation 2007, 115, 1306–1324. [Google Scholar] [CrossRef] [Green Version]
- Samuel Seely. Electron-Tube Circuits; McGraw-Hill Book Company, Inc.: New York, NY, USA, 1950. [Google Scholar]
- Toennies, J.F. Amplifier. U.S. Patent 2147940, 18 October 1937. [Google Scholar]
- Noyce, R. Semiconductor Device-and-Lead Structure. U.S. Patent US2981877A, 30 July 1959. [Google Scholar]
- Adrian, E.D.; Matthews, B.H.C. The interpretation of potential waves in the cortex. J. Physiol. 1934, 81, 440–471. [Google Scholar] [CrossRef] [PubMed]
- Blumlein, A. Thermionic Valve Amplifying Circuit. U.S. Patent 2185367, 2 January 1937. [Google Scholar]
- Donaldson, P.E. Electronic Apparatus for Biological Research; Butterworths Scientific Publications: London, UK, 1958. [Google Scholar]
- Guha, S.K. Some Aspects of Medical Electronics. IETE J. Res. 1967, 13, 201–206. [Google Scholar] [CrossRef]
- Livenson, A.R. Electromedical Apparatus; Medicine: Moscow, Russia, 1975. [Google Scholar]
- Smith, J.R., Jr. New Low-Level A-C Amplifier Provides Adjustable Noise Cancellation and Automatic Temperature Compensation. NASA Tech Brief. Brief 63-10003, March 1964. Available online: https://core.ac.uk/reader/10244550 (accessed on 29 June 2022).
- Fontenier, G. A sensitive, high impedance cardiac rhythm follower. Med. Biol. Eng. Comput. 1972, 10, 175–178. [Google Scholar] [CrossRef]
- Verigo, N.I.; Olifer, B.M.; Savelyev, V.I.; Sherman, A.M. PEKS-01 Portable Electrocardioscope. Transl. Meditsinskaya Tekhnika 1972, 3, 57–59. [Google Scholar] [CrossRef]
- Furman, K.I.; Lupu, N.Z. Cardiac monitoring and telemetering system. J. Appl. Physiol. 1963, 18, 840–842. [Google Scholar] [CrossRef]
- Unzhin, R.V.; Rozenblat, V.V. A transistor device for remote recording of heart rate, respiration, and movements. Transl. Bull. Eksperimental’noi Biol. Meditsiny 1964, 57, 117–120. [Google Scholar] [CrossRef]
- Super Matched Bipolar Transistor Pair Sets New Standards for Drift and Noise. National Semiconductor Application Note 222. 1979. Available online: https://www.ti.com/lit/an/snoa626b/snoa626b.pdf?ts=1658742009874&ref_url=https%253A%252F%252Fwww.google.com.hk%252F (accessed on 29 June 2022).
- Holmer, N.-G.; Lindstrom, K. An Electrometer Amplifier with Low Input Capacitance and Large Input Dynanic Range. IEEE Trans. Biomed. Eng. 1972, BME-19, 162–164. [Google Scholar] [CrossRef]
- Cox, J.W., Jr.; Laughter, J.S., Jr.; Brandon, C.W., III; Keller, F.W.; Dowdie, R.F.; Phillips, H.A.; Mirvis, D.M. A system oriented electrocardiographic amplifier. Cardiovasc. Res. 1979, 13, 238–241. [Google Scholar] [CrossRef] [PubMed]
- INA134 Audio Differential Line Receiver. Burr-Brown Corporation Data Sheet PDS-1390A. 1997. Available online: https://www.ti.com/lit/ds/symlink/ina134.pdf?ts=1658673414565 (accessed on 29 June 2022).
- Carter, B.; Mancini, R. Op Amps for Everyone, 5th ed.; Newnes: Cambridge, MA, USA, 2017; p. 484. [Google Scholar]
- Gudaitis, A.M. Virtual Right Leg Drive and Augmented Right Leg Drive Circuits for Common Mode Voltage Reduction in ECG and EEG Measurements. U.S. Patent 5,392,784, 28 February 1995. [Google Scholar]
- Wayne, S. Finding the Needle in a Haystack: Measuring small differential voltages in the presence of large common-mode voltages. Analog. Dialogue 2000, 34, 34-01. [Google Scholar]
- Beerwinkle, K.R.; Burch, J.J. A Low-Power Combination Electrocardiogram-Respiration Telemetry Transmitter. IEEE Trans. Biomed. Eng. 1976, BME-23, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Oberg, T. A Circuit for Contact Monitoring in Electrocardiography. IEEE Trans. Biomed. Eng. 1982, 29, 361–364. [Google Scholar] [CrossRef]
- Breuer, D. Some techniques for precision monolithic circuits applied to an instrumentation amplifier. IEEE J. Solid-State Circuits 1968, 3, 331–341. [Google Scholar] [CrossRef]
- Huijsing, J.H. Instrumentation amplifiers: A comparative study on behalf of monolithic integration. IEEE Trans. Instrum. Meas. 1976, IM-25, 227–231. [Google Scholar] [CrossRef]
- Smither, M.; Pugh, D.; Woolard, L.C.M.R.R. analysis of the 3-op-amp instrumentation amplifier. Electron. Lett. 1977, 13, 594–599. [Google Scholar] [CrossRef]
- Brokaw, P.; Timko, M.P. An improved monolithic instrumentation amplifier. IEEE J. Solid-State Circuits 1975, 10, 417–423. [Google Scholar] [CrossRef]
- Krabbe, H. Monolithic Data Amplifier. Differential instrumentation amplifier on a single chip has high input impedance, single-resistor gain adjustment, adjustable output bias, output-current sensing. Analog Dialogue 1972, 6, 3–5. [Google Scholar]
- Greef, R. Instruments for us in electrode process research. J. Phys. E Sci. Instrum. 1978, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Bergey, G.E.; Squires, R.D.; Sipple, W.C. Electrocardiogram Recording with Pasteless Electrodes. IEEE Trans. Biomed. Eng. 1971, BME-18, 206–211. [Google Scholar] [CrossRef]
- James, G.W.; Paul, M.H.; Wessel, H.U. Precision digital heart rate meter. J. Appl. Physiol. 1972, 32, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Thakor, N.V.; Webster, J.G. Ground-Free ECG Recording with Two Electrodes. Biomed. Eng. 1980, BME-27, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.W. Development of Modular Laboratory Equipment for Instruction in Biomedical Instrumentation. IEEE Trans. Biomed. Eng. 1978, BME-25, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Webster, J.G.; Nimunkar, A.J.; Powell, R. Medical Instrumentation. In Application and Design, 5th ed.; Wiley: Hoboken, NJ, USA, 2018. [Google Scholar]
- Virtanen, J.; Parkkonen, L.; Ilmoniemi, R.J.; Pekkonen, E.; Näätänen, R. Biopotential amplifier for simultaneous operation with biomagnetic instruments. Med. Biol. Eng. Comput. 1997, 35, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.K.; Kim, N.H.; Kim, S.H.; Kim, J.L. The development of high precision EEG amplifier for the computerized EEG analysis. In Proceedings of the 17th International Conference of the Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–23 September 1995; Volume 2, pp. 1651–1652. [Google Scholar]
- Badillo, L.; Leija, L.; Valentino, A.; Gutierrez, J.; Igartua, L.; Hernandez, P.; Alvarado, C. Sixteen channels Holter to EEG signal. In Proceedings of the 19th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 30 October–2 November 1997; Volume 4, pp. 1472–1473. [Google Scholar]
- Reske, D.; Moussavi, Z. Design of a web-based remote heart-monitoring system. In Proceedings of the Second Joint 24th Annual Conference and the Annual Fall Meeting of the Biomedical Engineering Society, Houston, TX, USA, 23–26 October 2002; Volume 3, pp. 1847–1848. [Google Scholar]
- Van Doren, C.L. Grasp Stiffness as a Function of Grasp Force and Finger Span. Motor Control 1998, 2, 352–378. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.D.; Peckham, P.H.; Kilgore, K.L. Tri-state myoelectric control of bilateral upper extremity neuroprostheses for tetraplegic individuals. IEEE Trans. Rehabil. Eng. 1996, 4, 251–263. [Google Scholar] [CrossRef]
- Wisana, I.D.G.; Nugraha, P.; Rachman, R. Development of a Low-Cost and Effisient ECG devices with IIR Digital Filter Design. Indones. J. Electron. Electromed. Eng. Med. Inform. 2021, 3, 21–28. [Google Scholar]
- Farooq, A.; Aroos, S.; Mumtaz, L.; Mazhar, M.; Baig, N.A.; Jafri, I.; Khaliq, A. Low-Cost Portable ECG Monitoring Device for Inaccessible Areas in Pakistan. Sir Syed Univ. Res. J. Eng. Technol. 2022, 12, 8–13. [Google Scholar] [CrossRef]
- Triwiyanto, E.Y.; Lamidi, M.R.M. Recent Technology and Challenge in ECG Data Acquisition Design: A Review. In Proceedings of the 2021 International Seminar on Application for Technology of Information and Communication (iSemantic), Semarangin, Indonesia, 18–19 September 2021; pp. 144–150. [Google Scholar] [CrossRef]
- Faruk, N.; Abdulkarim, A.; Emmanuel, I.; Folawiyo, Y.Y.; Adewole, K.S.; Mojeed, H.A.; Oloyede, A.A.; Olawoyin, L.A.; Sikiru, I.A.; Nehemiah, M.; et al. A comprehensive survey on low-cost ECG acquisition systems: Advances on design specifications, challenges and future direction. Biocybern. Biomed. Eng. 2021, 41, 474–502. [Google Scholar] [CrossRef]
- Hartmann, E. ECG Front-End Design is Simplified with MicroConverter. Analog Dialogue 2003, 37, 1–5. [Google Scholar]
- Li, G.; Wang, L.L.; Wang, Y.; Lin, L.; Jiang, W.; Lu, S.C.; Besio, W.G. A new kind of monitor for ophthalmic operation. J. Phys. Conf. Ser. 2005, 13, 345–348. [Google Scholar] [CrossRef]
- Kolasa, B.; Holt, H.; Duff, M. Discussion Between CareFusionand Analog Devices: Optimizing Performance and Lowering Power in an EEG Amplifier. Analog Devices Tech. Artic. 2011, MS-217, 1–5. [Google Scholar]
- Jin-ling, Z.; Lei, S.; Ya-chi, W.; Zhi-chen, Z. An ECG 7-lead monitoring system designing based on lower-power. In Proceedings of the ICME International Conference on Complex Medical Engineering, Beijing, China, 25–28 May 2013; pp. 154–159. [Google Scholar]
- Yang, G.; Su, X.; Zhao, L.; Cui, S.; Meng, Q.; Pei, W.; Chen, H. Research of portable community-oriented health monitoring terminal. In Proceedings of the 8th World Congress on Intelligent Control and Automation, Jinan, China, 7–9 July 2010; pp. 2979–2984. [Google Scholar]
- Wu, C.; Li, G.; Pommerenke, D.J.; Khilkevich, V.; Hess, G. Characterization of the RFI Rectification Behavior of Instrumentation Amplifiers. In Proceedings of the IEEE Symposium on Electromagnetic Compatibility, Signal Integrity and Power Integrity (EMC, SI & PI), Long Beach, CA, USA, 30 July–3 August 2018; pp. 156–160. [Google Scholar]
- Wu, Z.; Liu, J.; Ma, J. A novel cranial electrotherapy stimulation system with arbitrary waveform stimulation. In Proceedings of the 7-th International Conference on Biomedical Engineering and Informatics, Dalian, China, 14–16 October 2014; pp. 517–521. [Google Scholar]
- Petkos, K.; Koutsoftidis, S.; Guiho, T.; Degenaar, P.; Jackson, A.; Greenwald, S.E.; Brown, P.; Denison, T.; Drakakis, E.M. A high-performance 8 nV/√Hz 8-channel wearable and wireless system for real-time monitoring of bioelectrical signals. J. Neuroeng. Rehabil. 2019, 16, 156. [Google Scholar] [CrossRef]
- Babušiak, B.; Borik, Š. Bio-Amplifier with programmable gain and adjustable leads. In Proceedings of the 36th International Conference on Telecommunications and Signal Processing (TSP), Rome, Italy, 2–4 July 2013; pp. 616–619. [Google Scholar]
- Babusiak, B.; Borik, S.; Gala, M. Bio-amplifier with Programmable Gain and Adjustable Leads for Basic Measurement of Bioelectric Signals. In Information Technologies in Biomedicine; Advances in Intelligent Systems and Computing, Volume 284; Piętka, E., Kawa, J., Wieclawek, W., Eds.; Springer: Cham, Switzerland, 2014; Volume 4. [Google Scholar]
- Joshi, S.; Wakankar, A.; Khambete, N. Design and implementation of low power compact amplifier circuitry for wearable biosignal device. In Proceedings of the International Conference on Computing Communication Control and automation (ICCUBEA), Pune, India, 12–13 August 2016. [Google Scholar]
- Wang, Y.; Wunderlich, R.; Heinen, S. A low noise wearable wireless ECG system with body motion cancellation for long term homecare. In Proceedings of the IEEE 15th International Conference on e-Health Networking, Applications and Services (Healthcom 2013), Lisbon, Portugal, 9–12 October 2013; pp. 507–511. [Google Scholar]
- Chen, X.; Wang, Z.J. Design and Implementation of a Wearable, Wireless EEG Recording System. In Proceedings of the 5th International Conference on Bioinformatics and Biomedical Engineering, Wuhan, China, 10–12 May 2011. [Google Scholar]
- Abhishek, B.; Poojary, A.G.; Rao, M.V.A.; Narayanan, S. Low Power Portable EEG for Continuous Monitoring with Active Electrodes. In Proceedings of the Texas Instruments India Educators’ Conference, Bangalore, India, 4–6 April 2013; pp. 332–339. [Google Scholar]
- Puyol, R.; Lenzi, G.; Barg, G.; Arnaud, A. A portable, high density EEG acquisition system. In Proceedings of the 7th Argentine School of Micro-Nanoelectronics, Technology and Applications, Buenos Aires, Argentina, 15–16 August 2013; pp. 32–37. [Google Scholar]
- Valle, B.G.D.; Cash, S.S.; Sodini, C.G. Wireless behind-the-ear EEG recording device with wireless interface to a mobile device (iPhone/iPod touch). In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5952–5955. [Google Scholar]
- Rai, K.; Thakur, K.K.; Mane, P.K.; Panigrahi, N. Designing Low Cost Yet Robust EEG Acquisition System. In Proceedings of the IEEE International Symposium on Smart Electronic Systems (iSES) (Formerly iNiS), Rourkela, India, 16–18 December 2019; pp. 390–395. [Google Scholar]
- Sarhang-Nejad, M.; Temes, G.C. A high-resolution multibit Sigma Delta ADC with digital correction and relaxed amplifier requirements. IEEE J. Solid-State Circuits 1993, 28, 648–660. [Google Scholar] [CrossRef]
- Aziz, P.M.; Sorensen, H.V.; Vn der Spiegel, J. An overview of sigma-delta converters. IEEE Signal Process. Mag. 1996, 13, 61–84. [Google Scholar] [CrossRef]
- McKee, J.J.; Evans, N.E.; Wallace, D. Sigma-delta analogue-to-digital converters for ECG signal acquisition. In Proceedings of the 18th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Amsterdam, Netherlands, 31 October–3 November 1996; Volume 1, pp. 19–20. [Google Scholar]
- Berry, D.; Duignan, F.; Hayes, R. An Investigation of the use of a High Resolution ADC as a “Digital Biopotential Amplifier”. In Proceedings of the 4th European Conference of the International Federation for Medical and Biological Engineering, IFMBE, Antwerp, Belgium, 23–27 November 2008; Vander Sloten, J., Verdonck, P., Nyssen, M., Haueisen, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; Volume 22. [Google Scholar]
- Lie, D.; Das, V.; Hu, W.; Liu, Y.; Nguyen, T. A Low-Power CMOS Analog Front-End IC with Adjustable On-Chip Filters for Biosensors. Open J. Appl. Biosens. 2013, 2, 104–111. [Google Scholar] [CrossRef]
- Chou, S.T.; Huang, S.H.; Hong, Z.H.; Chen, W. A 40 Gbps optical receiver analog front-end in 65 nm CMOS. In Proceedings of the IEEE International Symposium on Circuits and Systems (ISCAS), Seoul, Korea, 20–23 May 2012; pp. 1736–1739. [Google Scholar]
- Hwang, Y.; Lin, H. A New CMOS Analog Front End for RFID Tags. IEEE Trans. Ind. Electron. 2009, 56, 2299–2307. [Google Scholar] [CrossRef]
- Ng, K.A.; Chan, P.K. A CMOS analog front-end IC for portable EEG/ECG monitoring applications. IEEE Trans. Circuits Syst. I Regul. Pap. 2005, 52, 2335–2347. [Google Scholar] [CrossRef]
- Kim, Y.J.; Cho, S.E.; Um, J.Y.; Chae, M.K.; Bang, J.; Song, J.; Jeon, T.; Kim, B.; Sim, J.Y.; Park, H.J. A Single-Chip 64-Channel Ultrasound RX-Beamformer Including Analog Front-End and an LUT for Non-Uniform ADC-Sample-Clock Generation. IEEE Trans. Biomed. Circuits Syst. 2017, 11, 87–97. [Google Scholar] [CrossRef]
- Yoon, Y.; Duan, Q.; Yeo, J.; Roh, J.; Kim, J.; Kim, D. A Delta–Sigma Modulator for Low-Power Analog Front Ends in Biomedical Instrumentation. IEEE Trans. Instrum. Meas. 2016, 65, 1530–1539. [Google Scholar] [CrossRef]
- Soundarapandian, K.; Berarducci, M. Analog Front-End Design for ECG Systems Using Delta-Sigma ADCs. Texas Instruments application Report 2010. Available online: https://www.ti.com/lit/an/sbaa160a/sbaa160a.pdf?ts=1658751056068&ref_url=https%253A%252F%252Fwww.google.com.hk%252F (accessed on 29 June 2022).
- Seidl, M. Analog Front-End Design with Texas Instruments’ Tooling Landscape. Application Note SBAA534—2022. Available online: https://www.ti.com/lit/an/sbaa534/sbaa534.pdf?ts=1658745163170&ref_url=https%253A%252F%252Fwww.google.com.hk%252F (accessed on 29 June 2022).
- ADS129x Low-Power, 8-Channel, 24-Bit Analog Front-End for Biopotential Measurements. Texas Instruments Data sheet SBAS459K–JANUARY 2010–REVISED AUGUST 2015. Available online: https://www.ti.com/lit/ds/symlink/ads1296r.pdf (accessed on 29 June 2022).
- MAX30003 Ultra-Low Power, Single-Channel Integrated Biopotential (ECG, R-to-R Detection) AFE, Maxim Integrated Data Sheet 19-8558; Rev 2; 9/2019. Available online: https://www.stg-maximintegrated.com/en/products/analog/data-converters/analog-front-end-ics/MAX30003.html (accessed on 29 June 2022).
- ADAS1000-3/ADAS1000-4 Low Power, Three Electrode Electrocardiogram (ECG) Analog Front End. Analog Devices Data Sheet D10997-0-1/2015(B). Available online: https://www.analog.com/media/en/technical-documentation/data-sheets/adas1000-3_1000-4.pdf (accessed on 29 June 2022).
- AD8232 Single-Lead, Heart Rate Monitor Front End. Analog Devices Data Sheet D10866-0-6/2018(C). Available online: https://www.analog.com/media/en/technical-documentation/data-sheets/ad8232.pdf (accessed on 29 June 2022).
- Vijay, V.; Reddy, C.V.S.K.; Pittala, C.S.; Vallabhuni, R.R.; Saritha, M.; Lavanya, M.; Venkateswarlu, S.C.; Sreevani, M. ECG performance validation using operational transconductance amplifier with bias current. Int. J. Syst. Assur. Eng. Manag. 2021, 12, 1173–1179. [Google Scholar] [CrossRef]
- Lu, T.C.; Liu, P.; Gao, X.; Lu, Q.Y. A Portable ECG Monitor with Low Power Consumption and Small Size Based on AD8232 Chip. Mech. Mater. 2014, 513–517, 2884–2887. [Google Scholar] [CrossRef]
- Huda, N.; Khan, S.; Abid, R.; Shuvo, S.B.; Labib, M.M.; Hasan, T. A Low-cost, Low-energy Wearable ECG System with Cloud-Based Arrhythmia Detection. In Proceedings of the IEEE Region 10 Symposium (TENSYMP), Dhaka, Bangladesh, 5–7 June 2020; pp. 1840–1843. [Google Scholar]
- Sani, S. Design and Implementation of a Low-Cost ECG Monitoring System Using ARM Cortex-M4 Family Microcontroller. In Proceedings of the IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 10–12 January 2021. [Google Scholar]
- Briginetsa, S.; Volkov, A.; Martinov, G.; Veselkov, A. Development of a mobile heart monitor based on the ECG module AD8232. Am. Inst. Phys. 2015, 10, 1–7. [Google Scholar]
- Gifari, M.W.; Zakaria, H.; Mengko, R. Design of ECG Homecare:12-Lead ECG Acquisition using Single Channel ECG Device Developed on AD8232 Analog Front End. In Proceedings of the 5-th International Conference on Electrical Engineering and Informatics, Denpasar, Indonesia, 10–11 August 2015; pp. 371–376. [Google Scholar]
- Agung, M.A.; Basari. 3-lead acquisition using single channel ECG device developed on AD8232 analog front end for wireless ECG application. AIP Conf. Proc. 2017, 1817, 040015. [Google Scholar]
- Yusof, M.A.; Hau, Y.W. Mini Home-Based Vital Sign Monitor with Android Mobile Application (my Vital Gear). In Proceedings of the IEEE-EMBS Conference on Biomedical Engineering and Science (IECBES), Sarawak, Malaysia, 3–6 December 2018; pp. 150–155. [Google Scholar]
- Kanani, P.; Padole, M. Recognizing Real Time ECG Anomalies Using Arduino, AD8232 and Java; Springer Nature: Singapore, 2018; Volume 905, pp. 54–64. [Google Scholar]
- Iskandar, W.J.; Roihan, I.; Koestoer, R.A. Prototype low-cost portable electrocardiogram (ECG) based on Arduino-Uno with Bluetooth feature. AIP Conf. Proc. 2019, 2193, 050019. [Google Scholar]
- Rahman, M.M.; Rimon, M.A.; Hoque, M.A.; Sammir, M.R. Affordable Smart ECG Monitoring Using Arduino & Bluetooth Module. In Proceedings of the 1st International Conference on Advances in Science, Engineering and Robotics Technology, Dhaka, Bangladesh, 3–5 May 2019. [Google Scholar]
- Çelebi, M. Portable ECG Monitoring Device Design Based on ARDUINO. In Proceedings of the Medical Technologies Congress (TIPTEKNO), Antalya, Turkey, 19–20 November 2020. [Google Scholar]
- Hamad, A.M.; Jasim, A.D. Jasim Remote ECG signal monitoring and classification based on Arduino with AD8232 sensor. Univ. Thi-Qar J. Eng. Sci. 2021, 11, 95–101. [Google Scholar]
- Patil, P.; Bhole, K. Real time ECG on internet using Raspberry Pi. In Proceedings of the International Conference on Communication, Computing and Internet of Things (IC3IoT), Chennai, India, 15–17 February 2018; pp. 267–270. [Google Scholar]
- Lili, T.; Wei, H. Portable ECG Monitoring System Design. In Proceedings of the 3rd International Conference on Electronic Information Technology and Computer Engineering (EITCE), Xiamen, China, 18–20 October 2019; pp. 1370–1373. [Google Scholar]
- Bravo-Zanoguera, M.; Cuevas-González, D.; García-Vázquez, J.P.; Avitia, R.L.; Reyna, M.A. Portable ECG System Design Using the AD8232 Microchip and Open-Source Platform. Multidiscip. Digit. Publ. Inst. Proc. 2019, 42, 49. [Google Scholar]
- Bravo-Zanoguera, M.; Cuevas-González, D.; Reyna, M.A.; García-Vázquez, J.P.; Avitia, R.L. Fabricating a Portable ECG Device Using AD823X Analog Front-End Microchips and Open-Source Development Validation. Sensors 2020, 20, 5962. [Google Scholar] [CrossRef]
- Kusumah, I.H.; Artiyasa, M.; Al-Bukhori; Khoiri, M.I.; Ramadhan, A.D.; Supiyandi. Blood Pressure Measurement using Wrist PPG and ECG. In Proceedings of the 6th International Conference on Computing Engineering and Design, Sukabumi, Indonesia, 15–16 October 2020. [Google Scholar]
- Chatterjee, A.; Pal, S.; Mitra, M. PPT Based Portable Cuffless Systolic Blood Pressure Estimation. In Proceedings of the Calcutta Conference (CALCON), Kolkata, India, 28–29 February 2020; pp. 142–147. [Google Scholar]
- Ji, X.; Ning, C.; Zhao, C.; Zhang, X. Design of the HRV Analysis System Based on AD8232. In Proceedings of the 3rd International Symposium on Mechatronics and Industrial Informatics (ISMII 2017), Zhuhai, China, 30–31 October 2015; pp. 230–234. [Google Scholar]
- Abidin, Z.; Siwindarto, P.; Muttaqin, A. Portable Heart Beat Monitoring System Using Three-Lead Configuration. In Proceedings of the Electrical Power, Electronics, Communications, Controls and Informatics Seminar (EECCIS), Batu, Indonesia, 9–11 October 2018; pp. 173–176. [Google Scholar]
- Potdar, R.M.; Meshram, M.R.; Kumar, R. Heart Rate Monitoring with Real Time ECG using AD-8232. Int. J. Res. Anal. Rev. (IJRAR) 2019, 2661, 699–705. [Google Scholar]
- Turner, J.; Zellner, C.; Khan, T.; Yelamarthi, K. Continuous heart rate monitoring using smartphone. In Proceedings of the IEEE International Conference on Electro Information Technology (EIT), Lincoln, NE, USA, 14–17 May 2017; pp. 324–326. [Google Scholar]
- Utomo, T.P.; Nuryani, N. QRS peak detection for heart rate monitoring on Android smartphone. In Proceedings of the International Conference on Science and Applied Science, Qingdao, China, 29–30 July 2017. [Google Scholar]
- Wang, Z.; Wang, F.; Ji, X. Analysis of Autonomic Nervous System Based on HRV. In Proceedings of the 4th International Conference on Mechanical, Control and Computer Engineering (ICMCCE), Hohhot, China, 24–26 October 2019; pp. 309–314. [Google Scholar]
- Hendra, M.; Kurniawan, D.; Chrismiantari, R.V.; Utomo, T.P.; Nuryani, N. Drowsiness detection using heart rate variability analysis based on microcontroller unit. In Proceedings of the 9th International Conference on Physics and Its Applications (ICOPIA), Surakarta, Indonesia, 14 August 2018. [Google Scholar]
- Chhabra, M.; Kalsi, M. Real Time ECG monitoring system based on Internet of Things (IoT). Int. J. Sci. Res. Publ. 2017, 7, 547–550. [Google Scholar]
- Mishra, A.; Chakraborty, B. AD8232 based Smart Healthcare System using Internet of Things (IoT). Int. J. Eng. Res. Technol. (IJERT) 2018, 7, 13–16. [Google Scholar]
- Bhosale, V.K.; Bhosale, K.R. Healthcare Based on IoT using Arduino and AD8232 Hearth Rate Monitoring Chip. Asian J. Converg. Technol. 2017, 3, 1–12. [Google Scholar]
- Pereira, M.; Nagapriya, K.K. A Novel IoT Based Health Monitoring System Using LPC2129. In Proceedings of the 2nd IEEE International Conference on Recent Trends in Electronics Information & Communication Technology (RTEICT), Bangalore, India, 19–20 May 2017; pp. 564–568. [Google Scholar]
- Rajanna, R.R.; Natarajan, S.; Vittal, P.R. An IoT Wi-Fi Connected Sensor for Real Time Heart Rate Variability Monitoring. In Proceedings of the IEEE Third International Conference on Circuits, Control, Communication and Computing, Bangalore, India, 3–5 October 2018. [Google Scholar]
- Sharma, A.K.; Saini, L.M. IoT based Diagnosing Myocardial Infarction through Firebase Web Application. In Proceedings of the Third International Conference on Electronics Communication and Aerospace Technology [ICECA 2019], Coimbatore, India, 12–14 June 2019; pp. 190–195. [Google Scholar]
- Ghifari, A.F.; Perdana, R.S. Minimum System Design of The IoT-Based ECG Monitoring. In Proceedings of the International Conference on ICT for Smart Society (ICISS), Bandung, Indonesia, 19–20 November 2020. [Google Scholar]
- Kubov, V.I.; Dymytrov, Y.Y.; Stojanović, R.; Kubova, R.M.; Škraba, A. A Feasible IoT System for Monitoring PPG and ECG Signals by using Low-cost Systems-on-chips and HTML Interface. In Proceedings of the 9th Mediterranean Conference on Embedded Computing (MECO), Budva, Montenegro, 8–11 June 2020. [Google Scholar]
- Yol, Y.; Ozdemir, M.A.; Akan, A. Design of Real Time Cardiac Arrhythmia Detection Device. In Proceedings of the Medical Technologies Congress (TIPTEKNO), Izmir, Turkey, 3–5 October 2019. [Google Scholar]
- Bhat, T.; Bhat, S.; Manoj, T. A Real-Time IoT Based Arrhythmia Classifier Using Convolutional Neural Networks. In Proceedings of the IEEE International Conference on Distributed Computing, VLSI, Electrical Circuits and Robotics (DISCOVER), Udupi, India, 30–31 October 2020; pp. 79–83. [Google Scholar]
- Moghadas, E.; Rezazadeh, J.; Farahbakhsh, R. An IoT Patient Monitoring based on Fog computing and Data Mining: Cardiac Arrhythmia Usecase. Internet Things 2020, 11, 100251. [Google Scholar] [CrossRef]
- Gowtham, A.; Anirudh, L.; Sreeja, B.S.; Aakash, B.A.; Adittya, S. Detection of Arrhythmia using ECG waves with Deep Convolutional Neural Networks. In Proceedings of the Fourth International Conference on Electronics, Communication and Aerospace Technology (ICECA-2020), Coimbatore, India, 5–7 November 2020; pp. 1390–1396. [Google Scholar]
- Simanjuntak, J.E.; Khodra, M.L.; Manullang, M.C. Design Methods of Detecting Atrial Fibrillation Using the Recurrent Neural Network Algorithm on the Arduino AD8232 ECG Module. In Proceedings of the Earth and Environmental Science, South Lampung, Indonesia, 25–26 October 2019. [Google Scholar]
- Abidin, Z.; Jaya, L.A.; Siwindarto, P.; Tanno, K. ECG Signal Processing Using Fuzzy Classification for Sudden Cardiac Death Prediction. In Proceedings of the 50th International Symposium on Multiple-Valued Logic (ISMVL), Miyazaki, Japan, 09–11 November 2020; pp. 111–116. [Google Scholar]
- Samson, V.R.; Sai, U.B.; Rao, P.M.; Eswar, K.K.; Kumar, S.P. Automatic Oxygen Level Control of Patient Using Fuzzy Logic and Arduino. In Proceedings of the International Conference on Big Data Analytics and computational Intelligence (ICBDACI), Chirala, Andhra Pradesh, India, 23–25 March 2017; pp. 98–102. [Google Scholar]
- Camacho-Perea, A.; Maya-Martinez, S.U.; Tovar-Corona, B.; Erick, D. Electrocardiographic Signal as a Biometric Feature. In Proceedings of the 14th International Conference on Electrical Engineering, Computing Science and Automatic Control (CCE), Mexico City, Mexico, 20–22 October 2017. [Google Scholar]
- Potdar, R.M.; Meshram, M.R.; Kumar, R. Implementation of AD8232 ECG Signal Classification Using Peak Detection Method for Determining RST Point. Indones. J. Artif. Intell. Data Min. (IJAIDM) 2019, 2, 61–66. [Google Scholar]
- Wang, X.; Li, X.; Leung, V.C. Artificial Intelligence-Based Techniques for Emerging Heterogeneous Network: State of the Arts, Opportunities, and Challenges. Artif. Intell. Enabled Netw. 2015, 3, 1379–1391. [Google Scholar] [CrossRef]
- Chowdhury, M.H.; Hossain, Q.D.; Saha, P.; Rahaman, M.M. Design, fabrication and performance evaluation of a three electrode ECG recorder. In Proceedings of the International Conference on Innovations in Science, Engineering and Technology (ICISET), Dhaka, Bangladesh, 28–29 October 2016. [Google Scholar]
- Rahman, M.A.; Samin, M.J.; Al Hasan, Z. Remote ECG Monitoring and Syncope Detection System Using Deep Learning. In Proceedings of the 2nd ICAICT, Dhaka, Bangladesh, 28–29 November 2020; pp. 201–206. [Google Scholar]
- Sugunakar, M.B.S.; Maruthy, K.N.; Srinivas, C.H.; Johnson, P. A comparative study between single lead AD8232 heart rate monitor and standard electrocardiograph to acquire electrocardiographic data for cardiac autonomic function testing. Indian J. Sci. Technol. 2021, 14, 534–540. [Google Scholar] [CrossRef]
- Sun, C.; Liao, J.; Wang, G.; Li, B.; Meng, M.Q. A Portable 12-Lead ECG Acquisition System. In Proceedings of the International Conference on Information and Automation, Yinchuan, China, 26–28 August 2013; pp. 368–373. [Google Scholar]
- Cristea, C.; Pasarica, A.; Andruseac, G.; Dionisie, B.; Rotariu, C. A Wireless ECG Acquisition Device for Remote Monitoring of Heart Rate and Arrhythmia Detection. In Proceedings of the 5th IEEE International Conference on E-Health and Bioengineering, Iasi, Romania, 19–21 November 2015. [Google Scholar]
- Du, L.; Yan, Y.; Wu, W.; Mei, Q.; Luo, Y.; Li, Y.; Wang, L. Towards a smart Holter system with high performance analogue front-end and enhanced digital processing. In Proceedings of the 35th Annual International Conference of the IEEE EMBS, Osaka, Japan, 3–7 July 2013; pp. 1210–1213. [Google Scholar]
- Que, C.; Liu, Q.; Ai, Q.; Chen, K. Design and realization of 12-lead electrocardiosignal acquisition and processing system. In Proceedings of the 13th International Computer Conference on Wavelet Active Media Technology and Information Processing (ICCWAMTIP), Chengdu, China, 16–18 December 2016; pp. 436–439. [Google Scholar]
- Gnecchi, J.A.G.; Herrejón, A.D.; Anguiano, A.D.; Patiño, A.M.; Espinoza, D.L. Advances in the Construction of ECG Wearable Sensor Technology: The ECG-ITM-05 eHealth Data Acquisition System. In Proceedings of the Ninth Electronics, Robotics and Automotive Mechanics Conference, Cuernavaca, Mexico, 19–23 November 2012; pp. 338–342. [Google Scholar]
- Malcangi, M. Acquisition and processing of the physiologic signal to prevent driving accidents. In Proceedings of the 6-th European Embedded Design in Education and Research, Milan, Italy, 11–12 September 2014; pp. 212–215. [Google Scholar]
- Barabino, G.; Pani, D.; Dessi, A.; Raffo, L. A Configurable biopotentials acquisition module suitable for fetal electrocardiography studies. In Proceedings of the International Conference on Big Data Analytics and computational Intelligence (ICBDACI), Turin, Italy, 7–9 May 2015; pp. 479–483. [Google Scholar]
- Wu, C.; Zhang, Y.; Hong, C.; Chiueh, H. Implementation of ECG Signal Processing Algorithms for Removing Baseline Wander and Electromyography Interference. In Proceedings of the 8th IEEE International Conference on Communication Software and Networks, Beijing, China, 4–6 June 2016; pp. 118–121. [Google Scholar]
- Talavera, J.R.; Mendoza, E.A.; Dávila, N.M.; Supo, E. Implementation of a real-time 60 Hz interference cancellation algorithm for ECG signals based on ARM cortex M4 and ADS1298. In Proceedings of the IEEE XXIV International Conference on Electronics, Electrical Engineering and Computing (INTERCON), Cusco, Peru, 15–18 August 2017. [Google Scholar]
- Martínez-Suárez, F.; Alvarado-Serrano, C. Prototype of an Ambulatory ECG Monitoring System with R Wave Detection in Real Time Based on FPGA. In Proceedings of the 16th International Conference on Electrical Engineering, Computing Science and Automatic Control (CCE), Mexico City, Mexico, 11–13 September 2019. [Google Scholar]
- Liu, J.; Zhou, Y. Design of a novel portable ECG monitor for heart health. In Proceedings of the Sixth International Symposium on Computational Intelligence and Design, Hangzhou, China, 28–29 October 2013; pp. 257–260. [Google Scholar]
- De Oliveira Igor, H.; Cene, V.H.; Balbinot, A. Portable electrocardiograph through android application. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 6780–6783. [Google Scholar]
- Abtahi, F.; Snäll, J.; Aslamy, B.; Abtahi, S.; Seoane, F.; Lindecrantz, K. Biosignal PI, an Affordable Open-Source ECG and Respiration Measurement System. Sensors 2015, 15, 93–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abtahi, F.; Aslamy, B.; Boujabir, I.; Seoane, F.; Lindecrantz, K. An Affordable ECG and Respiration Monitoring System Based on Raspberry PI and ADAS1000: First Step towards Homecare Applications. IFMBE Proc. 2015, 48, 5–8. [Google Scholar]
- Hafid, A.; Benouar, S.; Kedir-Talha, M.; Abtahi, F.; Attari, M.; Seoane, F. Full Impedance Cardiography Measurement Device Using Raspberry PI3 and System-on-Chip Biomedical Instrumentation Solutions. J. Biomed. Health Inform. 2018, 22, 1883–1894. [Google Scholar] [CrossRef]
- Přeučil, T.; Novotný, M. Low-Cost Portable ECG. In Proceedings of the 8th Mediterranean conference on embedded computing (MECO), Budva, Montenegro, 10–14 June 2019. [Google Scholar]
- Arulmozhivarman, P.; Reddy, G.R.; Tatavarti, R. Low-cost EEG Signal Acquisition System. In Proceedings of the ISSNIP Biosignals and Biorobotics Conference: Biosignals and Robotics for Better and Safer Living (BRC), Rio de Janeiro, Brazil, 18–20 February 2013. [Google Scholar]
- Liao, J.C.; Shih, W.Y.; Huang, K.J.; Fang, W.C. An online recursive ICA based real-time multichannel EEG system on chip design with automatic eye blink artifact rejection. In Proceedings of the International Symposium on VLSI Design, Automation, and Test (VLSI-DAT), Hsinchu, Taiwan, 22–24 April 2013. [Google Scholar]
- Chen, J.; Li, X.; Mi, X.; Pan, S. A High Precision EEG Acquisition System Based on the Compact PCI Platform. In Proceedings of the 7th International Conference on BioMedical Engineering and Informatics (BMEI 2014), Dalian, China, 14–16 October 2014; pp. 511–516. [Google Scholar]
- Acharya, D.; Rani, A.; Agarwal, S. EEG data acquisition circuit system Based on ADS1299EEG FE. In Proceedings of the 4th International Conference on Reliability, Infocom Technologies and Optimization (ICRITO) (Trends and Future Directions), Noida, India, 2–4 September 2015. [Google Scholar]
- Gani, H.S.; Wijaya, S.K.; La Ode Husein, Z.T. Development of EEG Data Acquisition System based on FPGA Zedboard. In Proceedings of the 5th International Conference on Instrumentation, Communications, Information Technology, and Biomedical Engineering (ICICI-BME), Bandung, Indonesia, 6–7 November 2017; pp. 246–250. [Google Scholar]
- Lee, S.; Shin, Y.; Kumar, A.; Kim, M.; Lee, H. Dry Electrode-based Fully Isolated EEG/fNIRS Hybrid Brain-monitoring System. IEEE Trans. Biomed. Eng. 2018, 66, 1055–1068. [Google Scholar] [CrossRef] [PubMed]
- Uktveris, T.; Jusas, V. Development of a Modular Board for EEG Signal Acquisition. In Proceedings of the 5th International Conference on Mathematics and Computers in Sciences and Industry (MCSI), Corfu, Greece, 25–27 August 2018; pp. 95–101. [Google Scholar]
- Wang, Z.; Li, W.; Chen, C.; Sun, C.; Chen, W. A multichannel reconfigurable EEG acquisition system design with felt-based soft material electrodes. In Proceedings of the International Instrumentation and Measurement Technology Conference (I2MTC), Houston, TX, USA, 14–17 May 2018. [Google Scholar]
- Zhao, Z.; Ivanov, K.; Lubich, L.; Mumin, O. Signal Quality and Electrode-Skin Impedance Evaluation in the Context of Wearable Electroencephalographic Systems. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 4965–4968. [Google Scholar]
- Wang, Z.; Chen, C.; Li, W.; Yuan, W.; Han, T.; Sun, C.; Tao, L.; Zhao, Y. A Multichannel EEG Acquisition System with Novel Ag NWs/PDMS Flexible Dry Electrodes. In Proceedings of the 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 1299–1302. [Google Scholar]
- Gao, K.-P.; Shen, G.-C.; Zhao, N.; Jiang, C.-P. Wearable Multifunction Sensor for the Detection of Forehead EEG Signal and Sweat Rate on Skin Simultaneously. IEEE Sens. J. 2020, 20, 10393–10404. [Google Scholar] [CrossRef]
- Shen, P.; Liu, Y.; Xiong, W.; He, A.; Zhang, M. A Real-Time Impedance Measurement System for EEG Based on Embedded System. In Proceedings of the 13th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics (CISP-BMEI), Chengdu, China, 17–19 October 2020; pp. 681–685. [Google Scholar]
- Bateson, A.D.; Asghar, A.U. Development and Evaluation of a Smartphone-Based Electroencephalography (EEG) System. IEEE Access 2021, 9, 75650–75667. [Google Scholar] [CrossRef]
- Apriadi, W.; Gani, H.S.; Prayitno, P.; Ibrahim, N.; Wijaya, S.K. Development of multithread acquisition system for high quality EEG signal measurement. J. Phys. Conf. Ser. 2021, 1816, 012072. [Google Scholar] [CrossRef]
- Tao, P.; Liu, W.; Tang, X. Human surface EHG acquisition and analysis system based on DM6446. In Proceedings of the International Conference on Medical Imaging Physics and Engineering, Shenyang, China, 19–20 October 2013; pp. 265–268. [Google Scholar]
- Mastinu, E.; Ortiz-Catalan, M.; Håkansson, B. Analog Front-Ends comparison in the way of a portable, low-power and low-cost EMG controller based on Pattern Recognition EMBC. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 2111–2114. [Google Scholar]
- Mastinu, E.; Håkansson, B.; Ortiz-Catalan, M. Low-cost, open-source bioelectric signal acquisition system. In Proceedings of the 14th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Eindhoven, Netherlands, 9–12 May 2017; pp. 19–22. [Google Scholar]
- Pancholi, S.; Joshi, A.M. Improved Classification Scheme using Fused Wavelet Packet Transform based Features for Intelligent Myoelectric Prostheses. IEEE Trans. Ind. Electron. 2020, 67, 8517–8525. [Google Scholar] [CrossRef]
- Zhou, R.; Wang, K.; Li, M. Design of a sEMG Signal Acquisition Instrument for Physical Rehabilitation Training. In Proceedings of the 10th International Symposium on Computational Intelligence and Design, Hangzhou, China, 9–10 December 2017; pp. 136–139. [Google Scholar]
- Favretto, M.A.; Cossul, S.; Andreis, F.R.; Balotin, A.F.; Marques, J.L.B. High Density Surface EMG System Based on ADS1298-front end. Lat. Am. Trans. 2018, 16, 1616–1622. [Google Scholar] [CrossRef]
- Ravariu, C.; Babarada, F.; Arhip, J.; Manea, E.; Pârvulescu, C. Personalized Mio-electrical Monitoring System Based on ADS1298 and MIM Electrodes. In Proceedings of the International Conference—10th Edition Electronics, Computers and Artificial Intelligence, Iasi, Romania, 28–30 June 2018. [Google Scholar]
- Zhao, Y.; Li, F.; Xu, L. A sEMG-Based Hand Motions Recognition System with Dimension-Reduced FFT. In Proceedings of the Chinese Control and Decision Conference (CCDC), Nanchang, China, 3–5 June 2019; pp. 1415–1420. [Google Scholar]
- De Jager, K.; Mentink, M.; Lancashire, H.; Al-Aja, Y. Characterization of a multi-channel multiplexed EMG recording system: Towards realizing variable electrode configurations. In Proceedings of the IEEE Biomedical Circuits and Systems Conference (BioCAS), Nara, Japan, 17–19 October 2019. [Google Scholar]
- Pancholi, S.; Joshi, A.M. Electromyography-Based Hand Gesture Recognition System for Upper Limb Amputees. IEEE Sens. Lett. 2019, 3, 5500304. [Google Scholar] [CrossRef]
- Pancholi, S.; Joshi, A.M. A Fast and Accurate Deep learning framework for EMG-PR based Upper-limb Prosthesis Control. In Proceedings of the International Symposium on Smart Electronic Systems (iSES) (Formerly iNiS), Chennai, India, 14–16 December 2020; pp. 206–207. [Google Scholar]
- Ossaba, A.T.; Tigreros, J.J.J.; Cami, J. Open-Source Multichannel EMG Armband design. In Proceedings of the IX International Congress of Mechatronics Engineering and Automation (CIIMA), Cartagena, Colombia, 4–6 November 2020. [Google Scholar]
- Teja, S.S.; Embrandiri, S.S.; Chandrachoodan, N.; Reddy, R. EOG based virtual keyboard. In Proceedings of the 41st Annual Northeast Biomedical Engineering Conference (NEBEC), Troy, NY, USA, 17–19 April 2015. [Google Scholar]
- Borchardt, A.R.; Schiavon, L.S.; Silva, L.G.L.; Junior, A.A.S.; Lucas, M.G. Acquisition and Comparison of Classification Algorithms in Electrooculogram Signals. Braz. Congr. Biomed. Eng. 2022, 83, 1999–2003. [Google Scholar]
- Gnecchi, J.A.; Herrejón, A.D.; Anguiano, A.D.; Sanchez, D.I.; Espinoza, D.L. Evaluation of Analog vs. ASIC Input/Filter Stage for Multimodal Biopotential Wearable Sensor Data Acquisition. In Proceedings of the Ninth Electronics, Robotics and Automotive Mechanics Conference, Cuernavaca, Mexico, 19–23 November 2012; pp. 359–364. [Google Scholar]
- Zhao, D.; Wang, L.; Cheng, S. Adaptive Deep Brain Stimulation System Based on ADS1292. In Proceedings of the 7th International Conference on Bioinformatics and Computational Biology, Hangzhou, China, 21–23 March 2019; pp. 83–87. [Google Scholar]
- Alexander, J. Single-Chip Micro Mote in EEG, fMRI, and TMS Systems; Electrical Engineering and Computer Sciences University of California: Berkeley, CA, USA, 2022; Available online: https://www2.eecs.berkeley.edu/Pubs/TechRpts/2022/EECS-2022-136.pdf (accessed on 29 June 2022).
- Komorowski, D.; Pietraszek, S.; Grzechca, D. The wireless system for EGG signal acquisition. In Proceedings of the 19th IEEE International Conference on Electronics, Circuits, and Systems (ICECS 2012), Seville, Spain, 9–12 December 2012; pp. 372–375. [Google Scholar]
- Ravariu, C.; Ursutiu, D.; Babarada, F.; Arhip, J.; Arama, S.S.; Radulian, G.; Samoila, C. Remote measurements of the electrical gastric signals-between theory and practice. In Proceedings of the 11th International Conference on Remote Engineering and Virtual Instrumentation (REV), Porto, Portugal, 26–28 February 2014; pp. 281–284. [Google Scholar]
- Ji, N.; Jiang, Y.; Yang, Z.; Jing, X.; Wang, H. An active electrode design for weak biosignal measurements. In Proceedings of the IEEE 13th International Conference on Signal Processing (ICSP), Chengdu, China, 6–10 November 2016; pp. 502–507. [Google Scholar]
- Jiang, Y.; Ji, N.; Wang, H.; Liu, X.; Geng, Y. Comparison of different shielding methods in acquisition of physiological signals. In Proceedings of the 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 2325–2328. [Google Scholar]
- Teferra, M.N.; Hobbs, D.A.; Clark, R.A.; Reynolds, K.J. Electronic-Textile 12-Lead Equivalent Diagnostic Electrocardiogram Based on the EASI Lead Placement. IEEE Sens. J. 2022, 22, 5994–6001. [Google Scholar] [CrossRef]
- Park, H.; Kim, M.K.; Malandraki, G.A.; Lee, C.H. Fabrication of Skin-Mountable Flexible Sensor Patch for Monitoring of Swallowing Function. Biomed. Eng. Technol. 2021, 1, 863–876. [Google Scholar]
- Zhang, Z.; Wang, Y.; Miao, K.; Ying, X. Design of Wireless Motion Sensor Node. J. Phys. Conf. Ser. 2021, 1792, 012014. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Z.; Li, Y.; Liu, C.; Guo, Y.X.; Lian, Y. A 2.89 μW Dry-Electrode Enabled Clockless Wireless ECG SoC for Wearable Applications. IEEE J. Solid-State Circuits 2016, 51, 2287–2298. [Google Scholar] [CrossRef]
- Kosari, A.; Breiholz, J.; Liu, N.; Calhoun, B.H.; Wentzloff, D.D. A 0.5 V 68 nW ECG Monitoring Analog Front-End for Arrhythmia Diagnosis. J. Low Power Electron. Appl. 2018, 8, 27. [Google Scholar] [CrossRef] [Green Version]
- Mondal, S.; Hsu, C.-L.; Jafari, R.; Hall, D. A dynamically reconfigurable ECG analog front-end with a 2.5 × data-dependent power reduction. In Proceedings of the 2017 IEEE Custom Integrated Circuits Conference (CICC), Austin, TX, USA, 30 April–3 May 2017. [Google Scholar]
- George, L.; Gargiulo, G.D.; Lehmann, T.; Hamilton, T.J. Concept Design for a 1-Lead Wearable/Implantable ECG Front-End: Power Management. Sensors 2015, 15, 29297–29315. [Google Scholar] [CrossRef] [Green Version]
- Pakkirisami Churchill, K.K.; Ramiah, H.; Chong, G.; Chen, Y.; Mak, P.-I.; Martins, R.P. A Fully-Integrated Ambient RF Energy Harvesting System with 423-μW Output Power. Sensors 2022, 22, 4415. [Google Scholar] [CrossRef] [PubMed]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ADS1292R | ADAS1000 | MAX30003 | AD8232 | |
|---|---|---|---|---|
| Manufacturer | Texas Instruments | Analog Devices | Maxim Integrated | Analog Devices |
| Channel amount | 2 | 5 | 1 | 1 |
| CMRR | 120 dB | 105 dB | 100 dB | 80 dB |
| Power consumption | 335 uW/channel | Up to 21 mW | 240 μW/channel | 170 μA |
| Power source | Analog: 2.7–5.2 V Digital: 1.7–3.6 V | 3.15–5.5 V | 1.1–2 V | 2–3.5 V |
| Amplification | 1, 2, 3, 4, 6, 8 or 12 | 1.4, 2.1, 2.8 or 4.2 | 20–160 | 100 |
| ADC resolution | 24 | Up to 19 | 18 | External ADC |
| Sampling frequency | 125–8000 Hz | 2, 16, 128 kHz | 125–512 Hz | External ADC |
| Signal-to-noise ratio | 107 dB | 100 dB | 77.2 (Amp = 20) 96.5 (Amp = 160) | External ADC |
| Right Leg Drive | Yes | Yes | No | Yes |
| Interface | SPI | SPI | SPI | Analog out |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anisimov, A.A.; Belov, A.V.; Sergeev, T.V.; Sannikova, E.E.; Markelov, O.A. Evolution of Bioamplifiers: From Vacuum Tubes to Highly Integrated Analog Front-Ends. Electronics 2022, 11, 2402. https://doi.org/10.3390/electronics11152402
Anisimov AA, Belov AV, Sergeev TV, Sannikova EE, Markelov OA. Evolution of Bioamplifiers: From Vacuum Tubes to Highly Integrated Analog Front-Ends. Electronics. 2022; 11(15):2402. https://doi.org/10.3390/electronics11152402
Chicago/Turabian StyleAnisimov, Aleksei A., Alexander V. Belov, Timofei V. Sergeev, Elizaveta E. Sannikova, and Oleg A. Markelov. 2022. "Evolution of Bioamplifiers: From Vacuum Tubes to Highly Integrated Analog Front-Ends" Electronics 11, no. 15: 2402. https://doi.org/10.3390/electronics11152402
APA StyleAnisimov, A. A., Belov, A. V., Sergeev, T. V., Sannikova, E. E., & Markelov, O. A. (2022). Evolution of Bioamplifiers: From Vacuum Tubes to Highly Integrated Analog Front-Ends. Electronics, 11(15), 2402. https://doi.org/10.3390/electronics11152402