
Neural Network Helps Determine the Hemorrhagic Risk of Cerebral Arteriovenous Malformation


Abstract
:1. Introduction
2. Materials and Methods
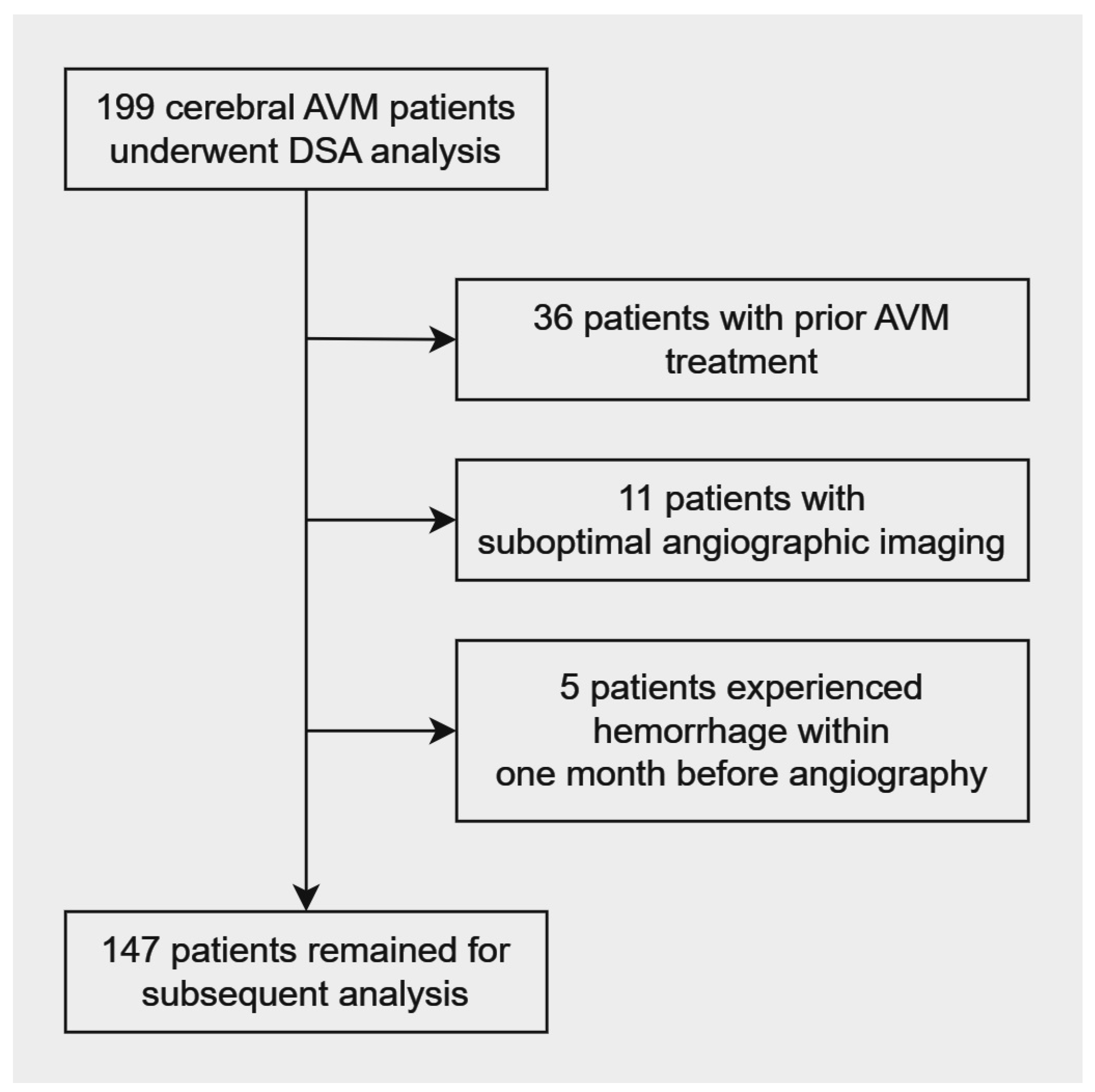
2.1. Patient Selection
2.2. Study Parameters
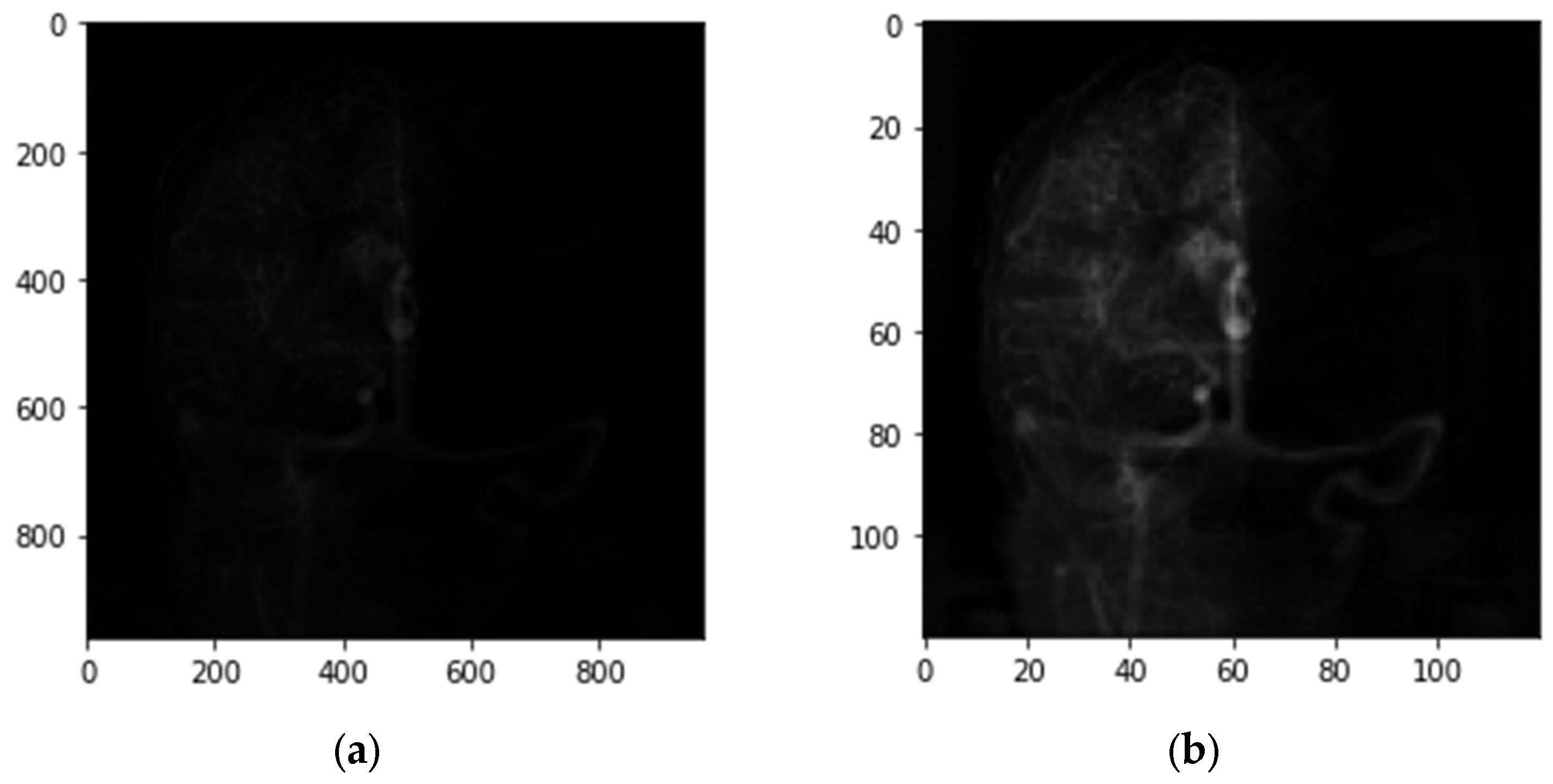
2.3. DSA Acquisition
2.4. Angioarchitecture
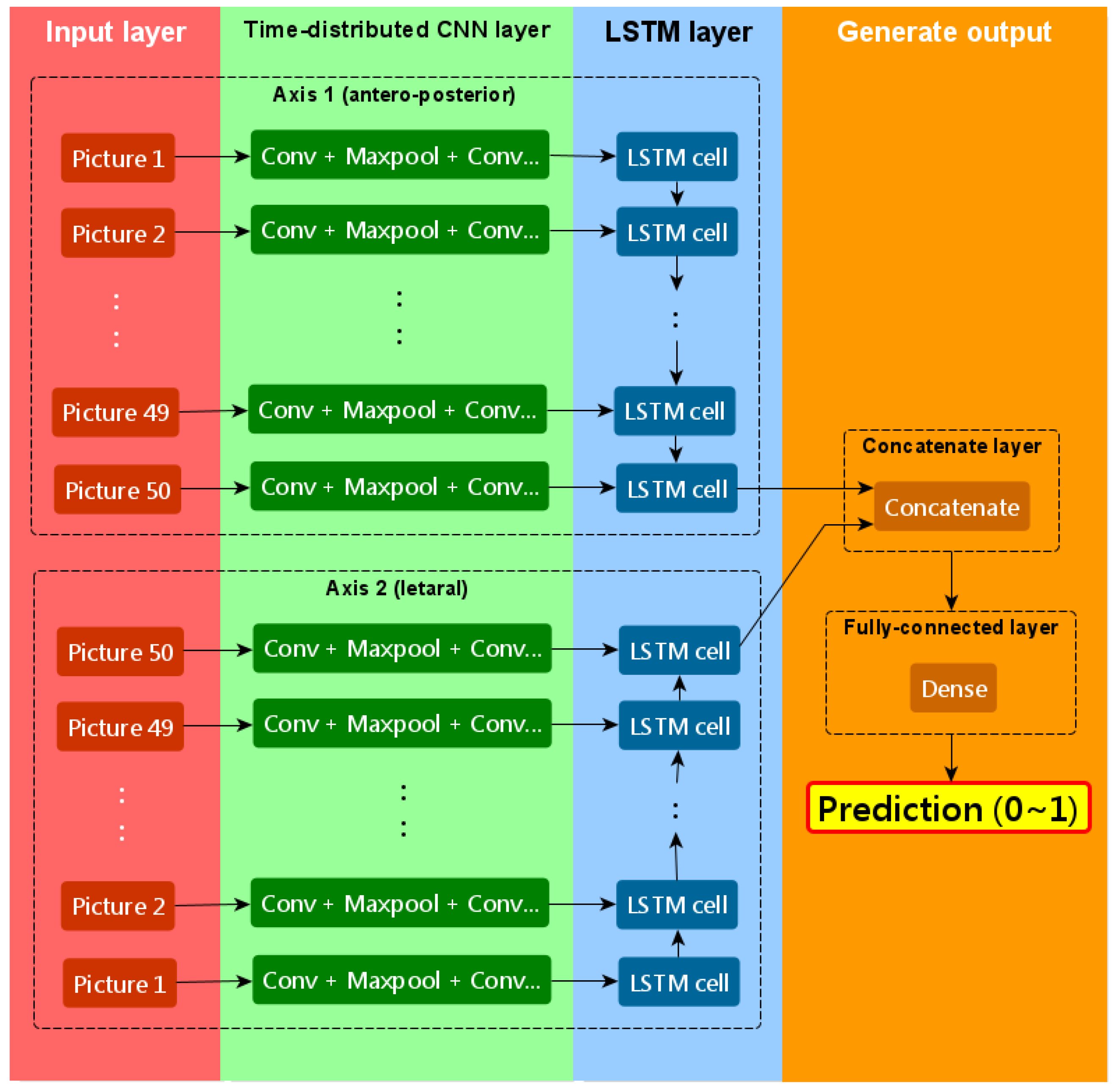
2.5. Neural Network Analysis
2.6. Statistical Analysis
3. Results
3.1. Logistic Regression
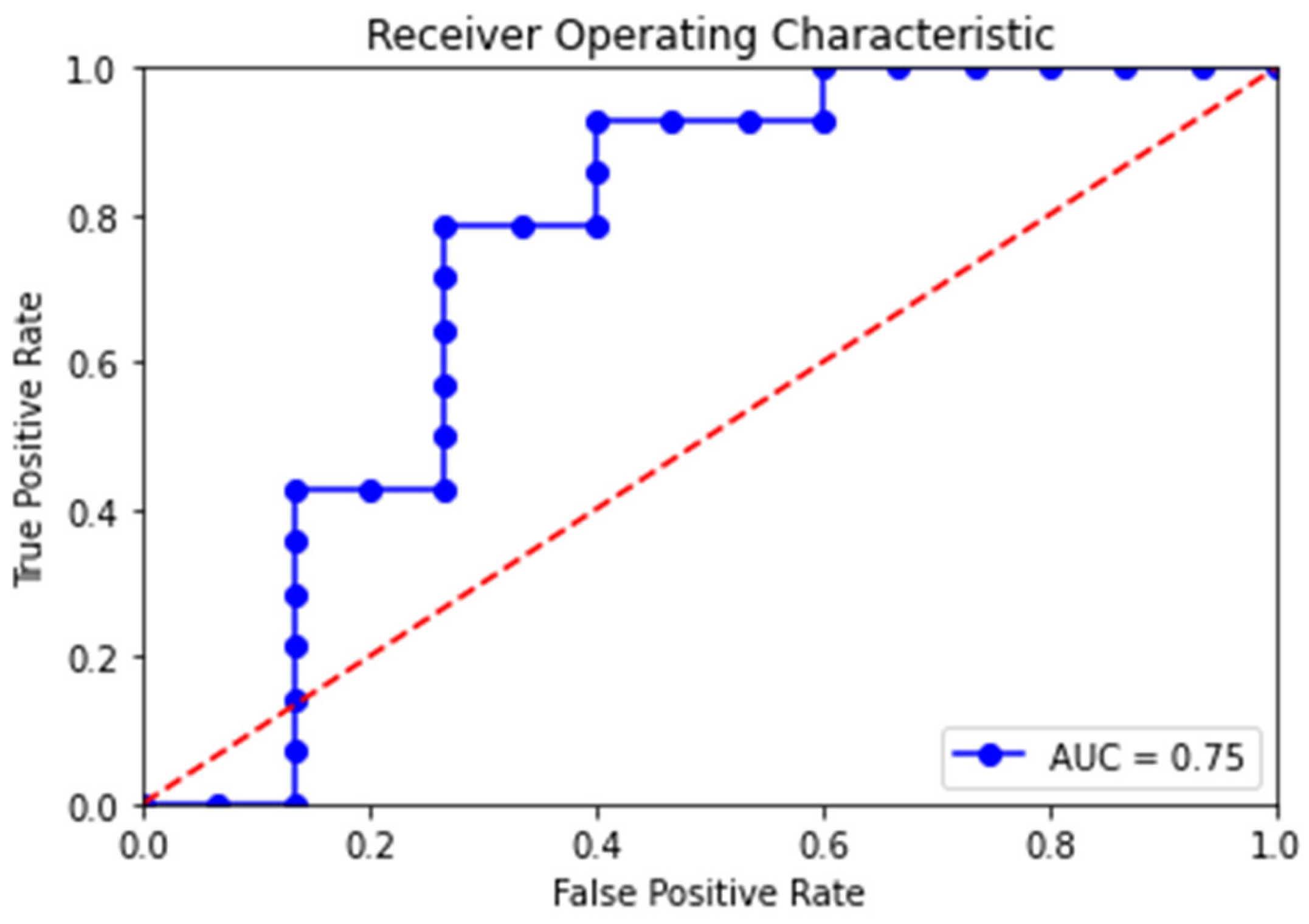
3.2. Neural Network Analysis
4. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Shahi, R.; Warlow, C. A systematic review of the frequency and prognosis of arteriovenous malformations of the brain in adults. Brain 2001, 124 Pt 10, 1900–1926. [Google Scholar] [CrossRef]
- Berman, M.F.; Sciacca, R.R.; Pile-Spellman, J.; Stapf, C.; Connolly, E.S., Jr.; Mohr, J.P.; Young, W.L. The epidemiology of brain arteriovenous malformations. Neurosurgery 2000, 47, 389–396. [Google Scholar] [CrossRef]
- Mohr, J.P.; Parides, M.K.; Stapf, C.; Moquete, E.; Moy, C.S.; Overbey, J.R.; Salman, R.A.-S.; Vicaut, E.; Young, W.L.; Houdart, E.; et al. Medical management with or without interventional therapy for unruptured brain arteriovenous malformations (ARUBA): A multicentre, non-blinded, randomised trial. Lancet 2014, 383, 614–621. [Google Scholar] [CrossRef]
- Stefani, M.A.; Porter, P.J.; terBrugge, K.G.; Montanera, W.; Willinsky, R.A.; Wallace, M.C. Angioarchitectural factors present in brain arteriovenous malformations associated with hemorrhagic presentation. Stroke 2002, 33, 920–924. [Google Scholar] [CrossRef]
- Pollock, B.E.; Flickinger, J.C.; Lunsford, L.D.; Bissonette, D.J.; Kondziolka, D. Factors that predict the bleeding risk of cerebral arteriovenous malformations. Stroke 1996, 27, 1–6. [Google Scholar] [CrossRef]
- Stapf, C.; Mast, H.; Sciacca, R.R.; Choi, J.H.; Khaw, A.V.; Connolly, E.S.; Pile-Spellman, J.; Mohr, J.P. Predictors of hemorrhage in patients with untreated brain arteriovenous malformation. Neurology 2006, 66, 1350–1355. [Google Scholar] [CrossRef]
- Duong, D.H.; Young, W.L.; Vang, M.C.; Sciacca, R.R.; Mast, H.; Koennecke, H.-C.; Hartmann, A.; Joshi, S.; Mohr, J.P.; Pile-Spellman, J. Feeding artery pressure and venous drainage pattern are primary determinants of hemorrhage from cerebral arteriovenous malformations. Stroke 1998, 29, 1167–1176. [Google Scholar] [CrossRef]
- Stefani, M.A.; Porter, P.J.; terBrugge, K.G.; Montanera, W.; Willinsky, R.A.; Wallace, M.C. Large and deep brain arteriovenous malformations are associated with risk of future hemorrhage. Stroke 2002, 33, 1220–1224. [Google Scholar] [CrossRef]
- Hernesniemi, J.A.; Dashti, R.; Juvela, S.; Vaart, K.; Niemela, M.; Laakso, A. Natural history of brain arteriovenous malformations: A long-term follow-up study of risk of hemorrhage in 238 patients. Neurosurgery 2008, 63, 823–829. [Google Scholar] [CrossRef]
- Spetzler, R.F.; Hargraves, R.W.; McCormick, P.W.; Zabramski, J.M.; Flom, R.A.; Zimmerman, R.S. Relationship of perfusion pressure and size to risk of hemorrhage from arteriovenous malformations. J. Neurosurg. 1992, 76, 918–923. [Google Scholar] [CrossRef]
- Todaka, T.; Hamada, J.; Kai, Y.; Morioka, M.; Ushio, Y. Analysis of mean transit time of contrast medium in ruptured and unruptured arteriovenous malformations: A digital subtraction angiographic study. Stroke 2003, 34, 2410–2414. [Google Scholar] [CrossRef]
- Abecassis, I.J.; Xu, D.S.; Batjer, H.H.; Bendok, B.R. Natural history of brain arteriovenous malformations: A systematic review. Neurosurg. Focus 2014, 37, E7. [Google Scholar] [CrossRef]
- Ellis, M.J.; Armstrong, D.; Vachhrajani, S.; Kulkarni, A.V.; Dirks, P.B.; Drake, J.M.; Smith, E.R.; Scott, R.M.; Orbach, D.B. Angioarchitectural features associated with hemorrhagic presentation in pediatric cerebral arteriovenous malformations. J. Neurointerv. Surg. 2013, 5, 191–195. [Google Scholar] [CrossRef]
- Kim, H.; Al-Shahi Salman, R.; McCulloch, C.E.; Stapf, C.; Young, W.L.; Coinvestigators, M. Untreated brain arteriovenous malformation: Patient-level meta-analysis of hemorrhage predictors. Neurology 2014, 83, 590–597. [Google Scholar] [CrossRef]
- Lin, T.M.; Yang, H.C.; Lee, C.C.; Wu, H.M.; Hu, Y.S.; Luo, C.B.; Guo, W.Y.; Kao, Y.H.; Chung, W.Y.; Lin, C.J. Stasis index from hemodynamic analysis using quantitative DSA correlates with hemorrhage of supratentorial arteriovenous malformation: A cross-sectional study. J. Neurosurg. 2020, 132, 1574–1582. [Google Scholar] [CrossRef]
- Mark, D.J.; Brittany, S.; Mario, Z. A Rational Approach to the Management of Cerebral Arteriovenous Malformations. World Neurosurg. 2022, 159, 338–347. [Google Scholar]
- Shakur, S.F.; Brunozzi, D.; Hussein, A.E.; Linninger, A.; Hsu, C.-Y.; Charbel, F.T.; Alaraj, A. Validation of cerebral arteriovenous malformation hemodynamics assessed by DSA using quantitative magnetic resonance angiography: Preliminary study. J. Neurointerv. Surg. 2018, 10, 156–161. [Google Scholar] [CrossRef]
- Chang, W.; Loecher, M.W.; Wu, Y.; Niemann, D.B.; Ciske, B.; Aagaard-Kienitz, B.; Kecskemeti, S.; Johnson, K.M.; Wieben, O.; Mistretta, C.; et al. Hemodynamic changes in patients with arteriovenous malformations assessed using high-resolution 3D radial phase-contrast MR angiography. AJNR Am. J. Neuroradiol. 2012, 33, 1565–1572. [Google Scholar] [CrossRef]
- Feng, R.; Badgeley, M.; Mocco, J.; Oermann, E.K. Deep learning guided stroke management: A review of clinical applications. J. Neurointerv. Surg. 2017, 10, 358–362. [Google Scholar] [CrossRef]
- Waljee, A.K.; Higgins, P.D.R. Machine learning in medicine: A primer for physicians. Am. J. Gastroenterol. 2010, 105, 1224–1226. [Google Scholar] [CrossRef]
- Chen, X.; Lei, Y.; Su, J.; Yang, H.; Ni, W.; Yu, J.; Gu, Y.; Mao, Y. A Review of Artificial Intelligence in Cerebrovascular Disease Imaging: Applications and Challenges. Curr. Neuropharmacol. 2022, 20, 1359–1382. [Google Scholar] [CrossRef]
- Tao, W.G.; Yan, L.C.; Zeng, M.; Chen, F.H. Factors affecting the performance of brain arteriovenous malformation rupture prediction models. BMC Med. Inform. Decis. Mak. 2021, 21, 142. [Google Scholar] [CrossRef]
- Hong, J.-S.; Lin, C.-J.; Lin, Y.-H.; Lee, C.-C.; Yang, H.-C.; Meng, L.-H.; Lin, T.-M.; Hu, Y.-S.; Guo, W.-Y.; Chu, W.-F.; et al. Machine learning application with quantitative digital subtraction angiography for detection of hemorrhagic brain arteriovenous malformations. IEEE Access 2020, 8, 204573. [Google Scholar] [CrossRef]
- Park, A.; Chute, C.; Rajpurkar, P.; Lou, J.; Ball, R.L.; Shpanskaya, K.; Jabarkheel, R.; Kim, L.H.; McKenna, E.; Tseng, J.; et al. Deep Learning-Assisted Diagnosis of Cerebral Aneurysms Using the HeadXNet Model. JAMA Netw. Open 2019, 2, 195600. [Google Scholar] [CrossRef]
- Huang, P.-W.; Peng, S.-J.; Pan, D.H.-C.; Yang, H.-C.; Tsai, J.-T.; Shiau, C.-Y.; Su, I.-C.; Chen, C.-J.; Wu, H.-M.; Lin, C.-J.; et al. Compactness index: A radiosurgery outcome predictor for patients with unruptured brain arteriovenous malformations. J. Neurosurg. 2022, 138, 241–250. [Google Scholar] [CrossRef]
- Joint Writing Group of the Technology Assessment Committee American Society of Interventional and Therapeutic Neuroradiology; Joint Section on Cerebrovascular Neurosurgery a Section of the American Association of Neurological Surgeons and Congress of Neur; Atkinson, R.P.; Awad, I.A.; Batjer, H.H.; Dowd, C.F.; Furlan, A.; Giannotta, S.L.; Gomez, C.R.; Gress, D.; et al. Reporting terminology for brain arteriovenous malformation clinical and radiographic features for use in clinical trials. Stroke 2001, 32, 1430–1442. [Google Scholar] [CrossRef]
- Guo, W.-Y.; Lee, C.-C.; Lin, C.-J.; Yang, H.-C.; Wu, H.-M.; Wu, C.-C.; Chung, W.-Y.; Liu, K.-D. Quantifying the Cerebral Hemodynamics of Dural Arteriovenous Fistula in Transverse Sigmoid Sinus Complicated by Sinus Stenosis: A Retrospective Cohort Study. AJNR Am. J. Neuroradiol. 2016, 38, 132–138. [Google Scholar] [CrossRef]
- Gross, B.A.; Du, R. Natural history of cerebral arteriovenous malformations: A meta-analysis. J. Neurosurg. 2013, 118, 437–443. [Google Scholar] [CrossRef]
- Costa, L.; Wallace, M.C.; Ter Brugge, K.G.; O’Kelly C’ Willinsky, R.A.; Tymianski, M. The natural history and predictive features of hemorrhage from brain arteriovenous malformations. Stroke 2009, 40, 100–105. [Google Scholar] [CrossRef]
- Yamada, S.; Takagi, Y.; Nozaki, K.; Kikuta, K.-I.; Hashimoto, N. Risk factors for subsequent hemorrhage in patients with cerebral arteriovenous malformations. J. Neurosurg. 2007, 107, 965–972. [Google Scholar] [CrossRef]
- Young, W.L.; Kader, A.; Pile-Spellman, J.; Ornstein, E.; Stein, B.M. Arteriovenous malformation draining vein physiology and determinants of transnidal pressure gradients. The Columbia University AVM Study Project. Neurosurgery 1994, 35, 389–395, discussion 95–96. [Google Scholar] [CrossRef]
- Miyasaka, Y.; Kurata, A.; Tokiwa, K.; Tanaka, R.; Yada, K.; Ohwada, T. Draining vein pressure increases and hemorrhage in patients with arteriovenous malformation. Stroke 1994, 25, 504–507. [Google Scholar] [CrossRef]
- Miyasaka, Y. Arteriovenous malformation draining vein physiology and determinants of transnidal pressure gradients. Neurosurgery 1995, 36, 1234–1236. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Number of Samples | Number of Hemorrhagic Samples | Number of Non-Hemorrhagic Samples | |
|---|---|---|---|
| Training set | 118 | 59 | 59 |
| Test set | 29 | 14 | 15 1 |
| Total n = 147 (100%) | Hemorrhage n = 73 (50%) | Non-Hemorrhage n = 74 (50%) | p Value 1 | |
|---|---|---|---|---|
| Age at diagnosis | 39.9 ± 14.4 | 33.7 ±16.9 | 0.019 | |
| Male, no. (%) | 85 (58) | 43 (59) | 42 (57) | 0.403 |
| Female, no. (%) | 62 (42) | 30 (40) | 32 (45) | |
| Seizure, no. (%) | 37 (25) | 9 (12) | 28 (38) | 0.01 |
| Headache, no. (%) | 66 (45) | 31 (42) | 35 (47) | 0.38 |
| Focal neurologic deficit, no. (%) | 36 (24) | 18 (25) | 18 (24) | 0.41 |
| Spetzler–Martin grade | 0.33 | |||
| Grade I, no. (%) | 40 (27) | 20 (27) | 20 (27) | |
| Grade II, no. (%) | 49 (33) | 23 (31) | 26 (35) | |
| Grade III, no. (%) | 40 (27) | 20 (27) | 20 (27) | |
| Grade IV, no. (%) | 17 (12) | 9 (12) | 8 (11) | |
| Grade V, no. (%) | 1 (1) | 1 (2) | 0 (0) |
| Hemorrhage n = 73 (50%) | Non-Hemorrhage n = 74 (50%) | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| p Value | Odds Ratio (95% CI) | p Value | Odds Ratio (95% CI) | |||
| Clinical factors | ||||||
| Age at diagnosis, year, mean (range) | 33.7 ± 16.9 | 39.9 ± 14.4 | 0.019 | 1.00 (−0.04–0.05) | 0.073 | 0.979 (0.957 −1.002) |
| Male, no. (%) | 41 (55) | 44 (60) | 0.666 | 1.14 (0.60–2.20) | ||
| Angioarchitecture | ||||||
| Deep location, no. (%) | 25 (34) | 18 (24) | 0.188 | 1.62 (0.79–3.33) | ||
| Single venous drainage, no. (%) | 43 (59) | 21 (28) | 0.001 1 | 3.61 (1.82–7.19) | 0.017 2 | 2.48 (1.23–5.78) |
| Exclusive superficial venous drainage, no. (%) | 32 (44) | 40 (54) | 0.216 | 0.66 (0.34–1.27) | ||
| Exclusive deep venous drainage, no. (%) | 30 (41) | 10 (14) | 0.001 1 | 4.46 (1.98–10.07) | 0.005 2 | 3.19 (1.32–7.69) |
| Periventricular drainage, no. (%) | 13 (18) | 7 (9) | 0.14 | 2.01 (0.78–2.63) | ||
| Venous sac, no. (%) | 13 (18) | 29 (39) | 0.005 1 | 0.34 (0.16–0.72) | 0.044 2 | 0.43 (0.190–0.975) |
| Intranidal venous sac, no. (%) | 12 (16) | 18 (24) | 0.238 | 0.61 (0.27–1.38) | ||
| Venous stenosis, no. (%) | 25 (34) | 18 (24) | 0.188 | 1.62 (0.79–3.73) | ||
| Multivariate Regression Model (n = 147) 1 | Training Set (n = 118) 2 | Test Set (n = 29) 3 | |
|---|---|---|---|
| Accuracy (%) | 100 (69) | 118 (100) | 22 (76) |
| True positive (%) | 46 (73) | 59 (100) | 11 (79) |
| False positive (%) | 18 (24) | 0 (0) | 4 (27) |
| True negative (%) | 56 (76) | 59 (100) | 11 (73) |
| False negative (%) | 27 (37) | 0 (0) | 3 (21) |
| Area under ROC curve | 0.757 | 0.999 | 0.748 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.-Y.; Chen, J.-C. Neural Network Helps Determine the Hemorrhagic Risk of Cerebral Arteriovenous Malformation. Electronics 2023, 12, 4241. https://doi.org/10.3390/electronics12204241
Wang K-Y, Chen J-C. Neural Network Helps Determine the Hemorrhagic Risk of Cerebral Arteriovenous Malformation. Electronics. 2023; 12(20):4241. https://doi.org/10.3390/electronics12204241
Chicago/Turabian StyleWang, Kuan-Yu, and Jyh-Cheng Chen. 2023. "Neural Network Helps Determine the Hemorrhagic Risk of Cerebral Arteriovenous Malformation" Electronics 12, no. 20: 4241. https://doi.org/10.3390/electronics12204241
APA StyleWang, K. -Y., & Chen, J. -C. (2023). Neural Network Helps Determine the Hemorrhagic Risk of Cerebral Arteriovenous Malformation. Electronics, 12(20), 4241. https://doi.org/10.3390/electronics12204241