A Review on the Role of Blockchain Technology in the Healthcare Domain

 ,
,  and
and
Abstract
:1. Introduction
2. Blockchain Technology
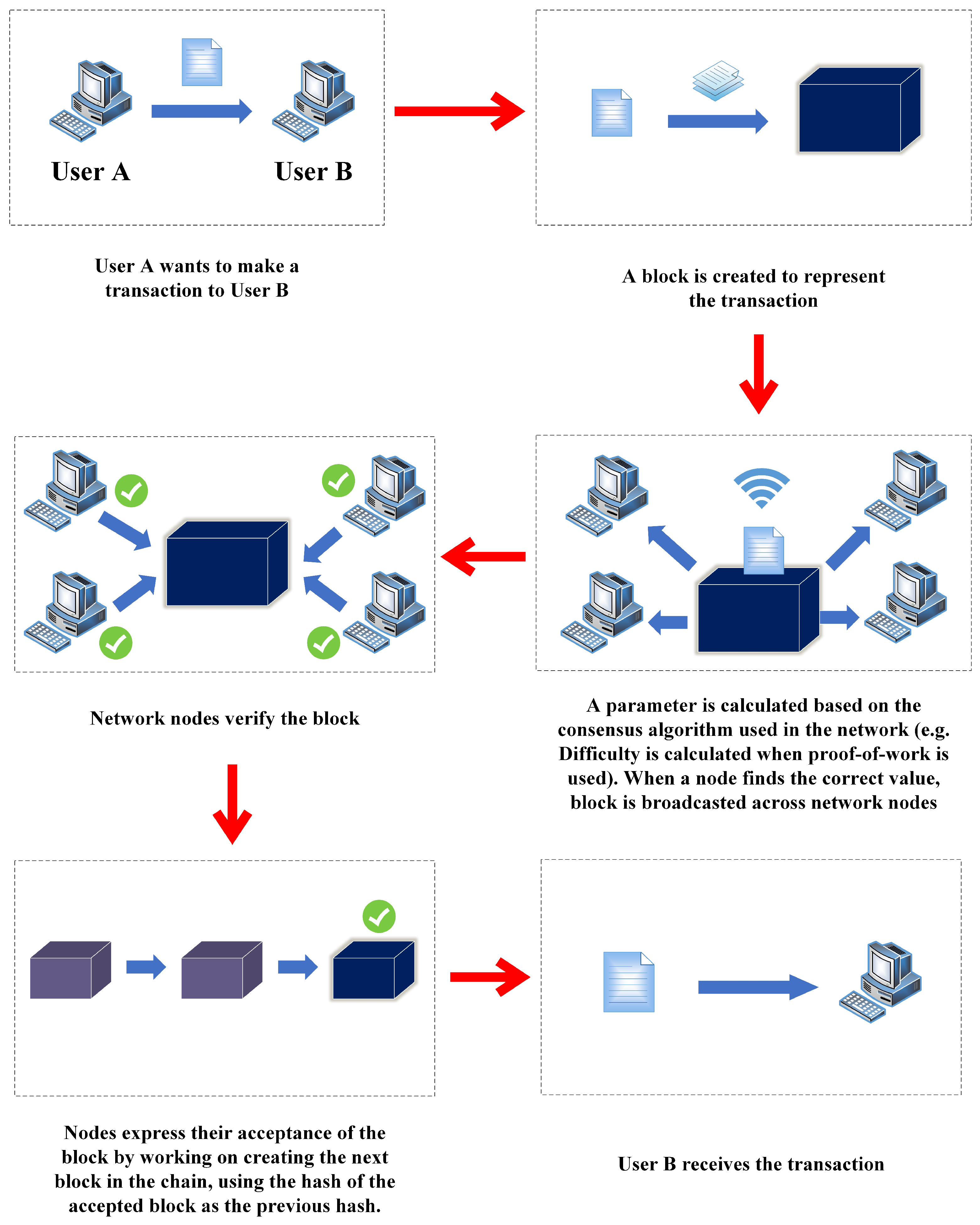
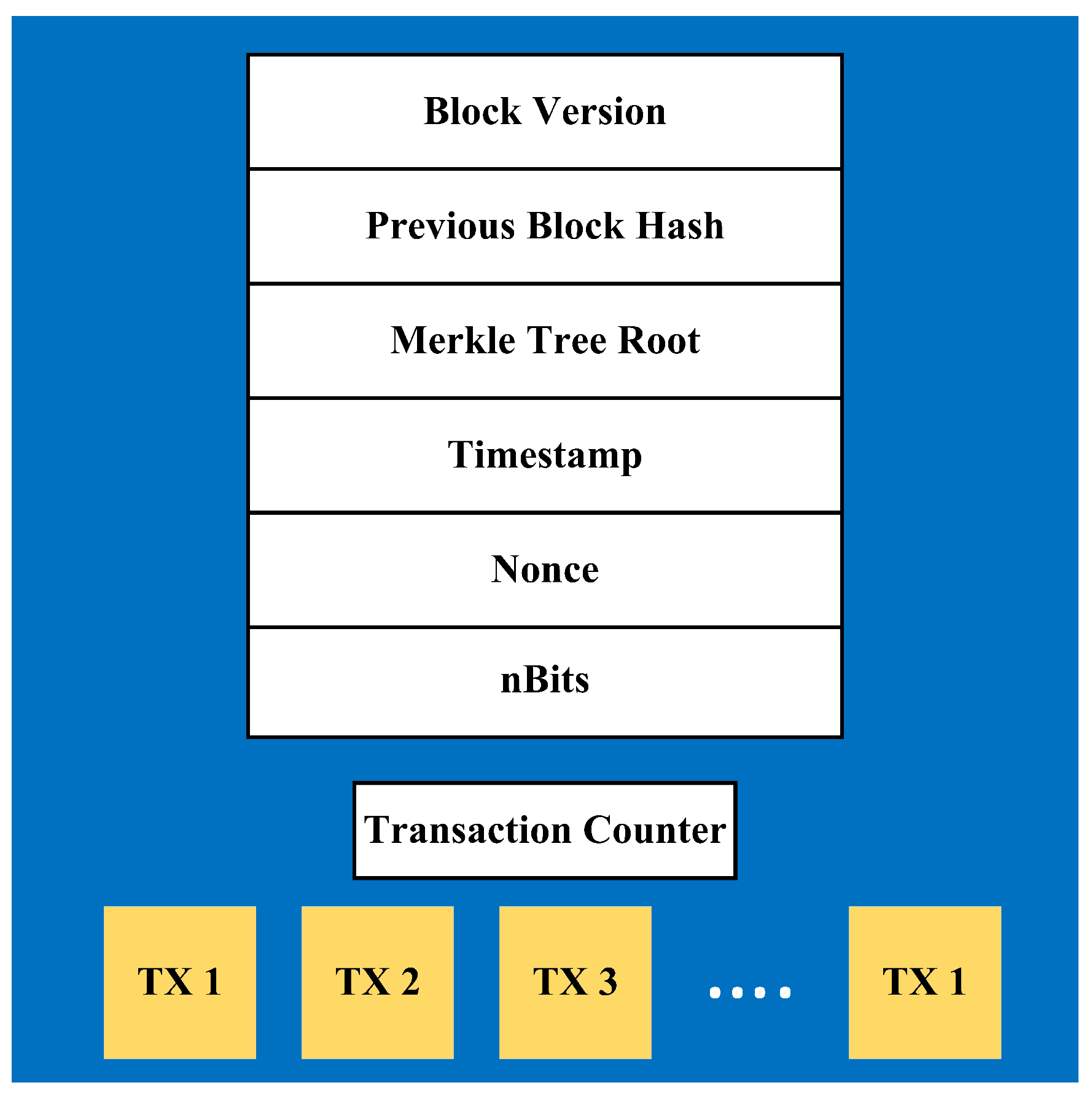
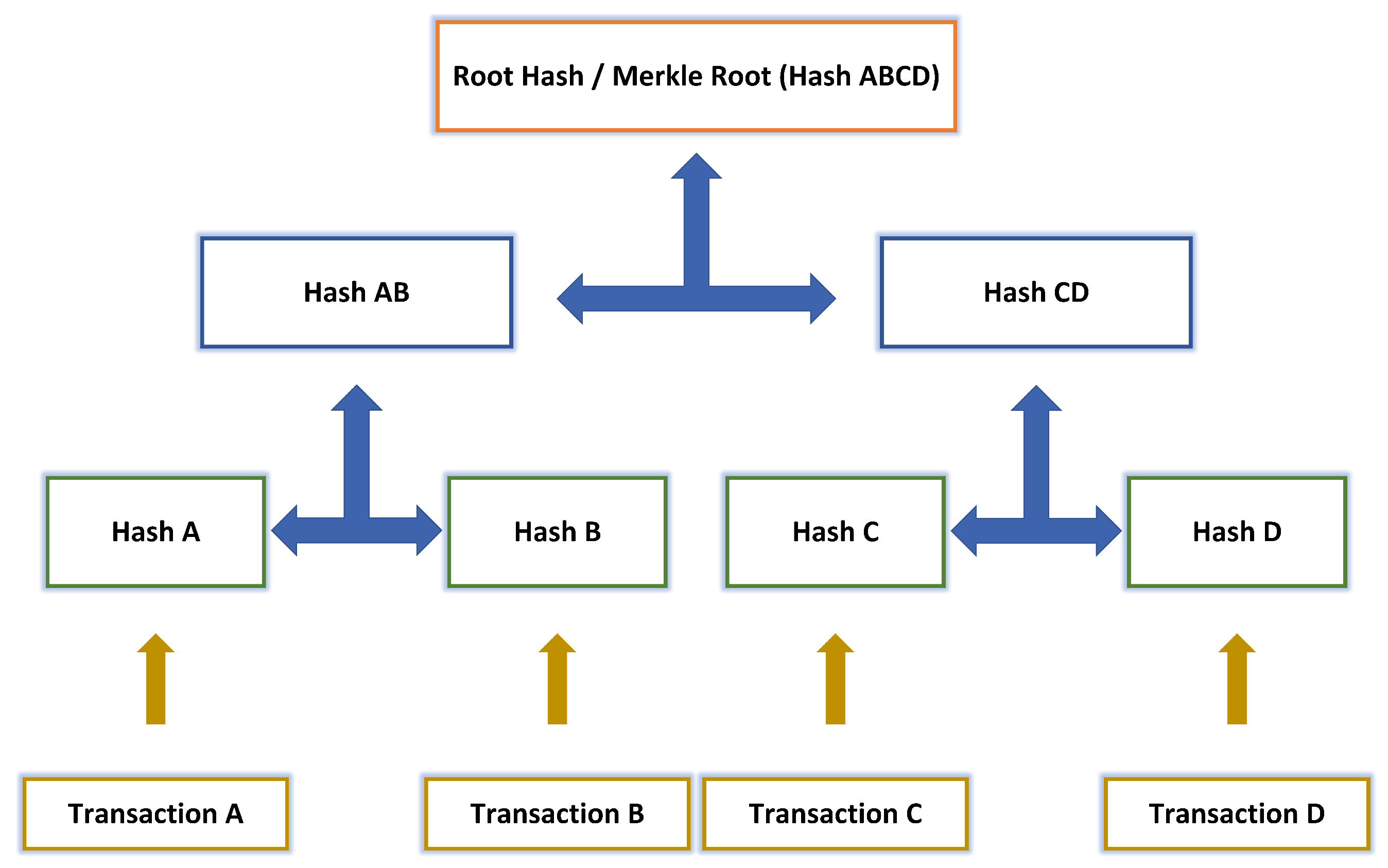
2.1. Overview
2.2. Consensus Algorithms
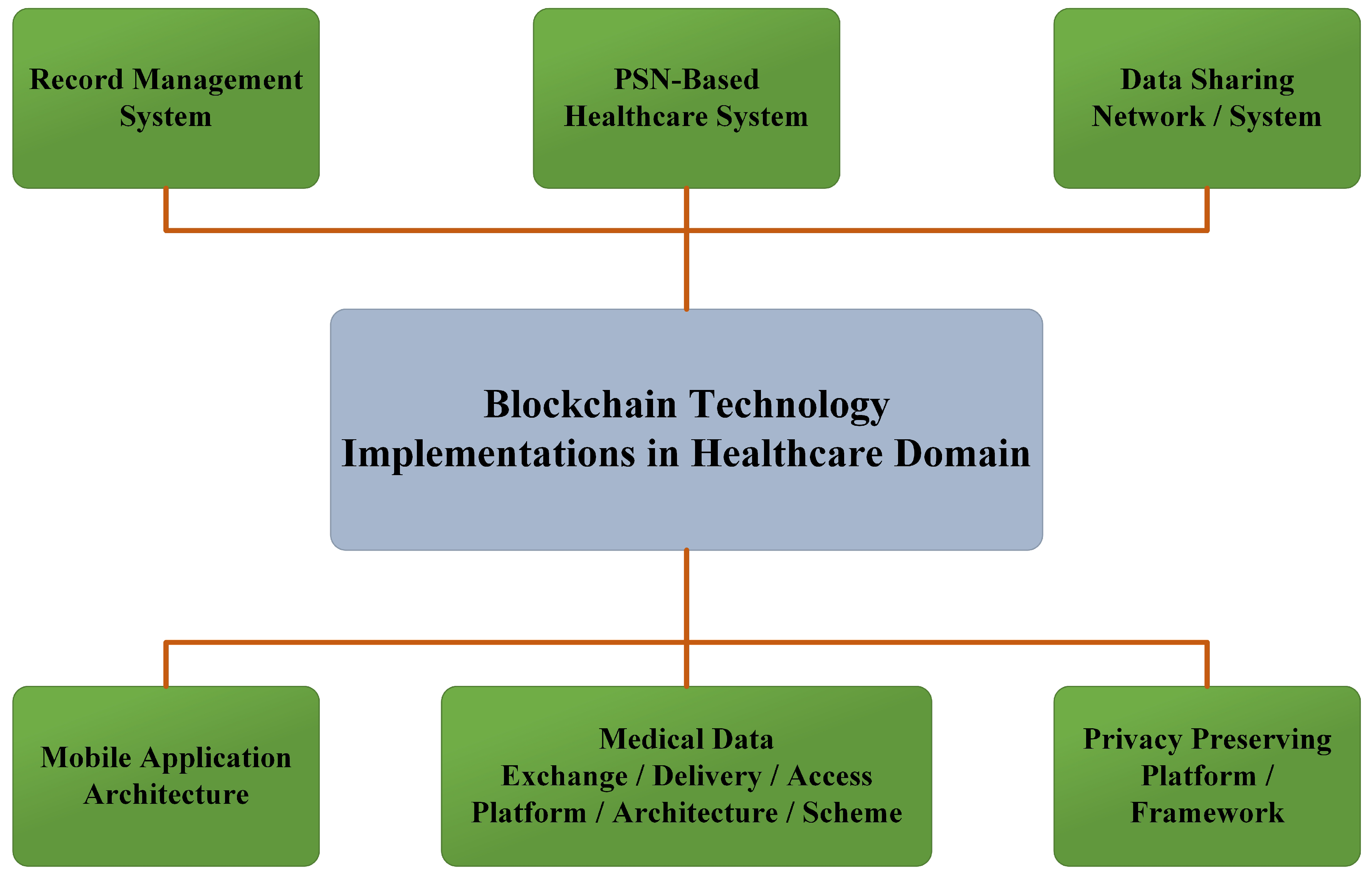
3. Blockchain in Healthcare
3.1. Research Method
3.2. Systematic Review
3.2.1. Data Sharing Network/System
3.2.2. Record Management System
3.2.3. Medical Data Exchange/Delivery/Access, Platform/Architecture/Scheme
3.2.4. Mobile Application Architecture
3.2.5. PSN-Based Healthcare System
3.2.6. Privacy Preserving Platform/Framework
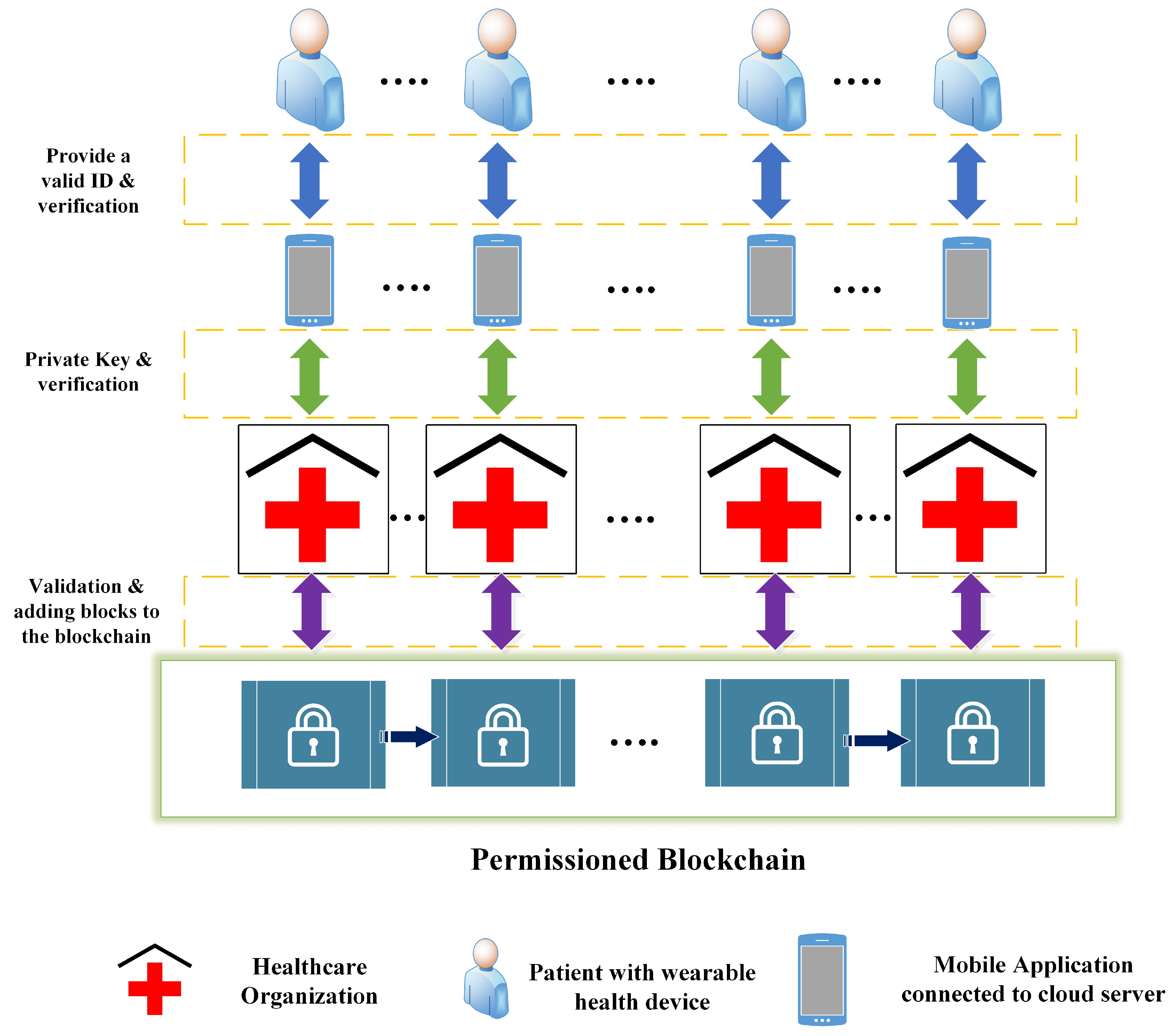
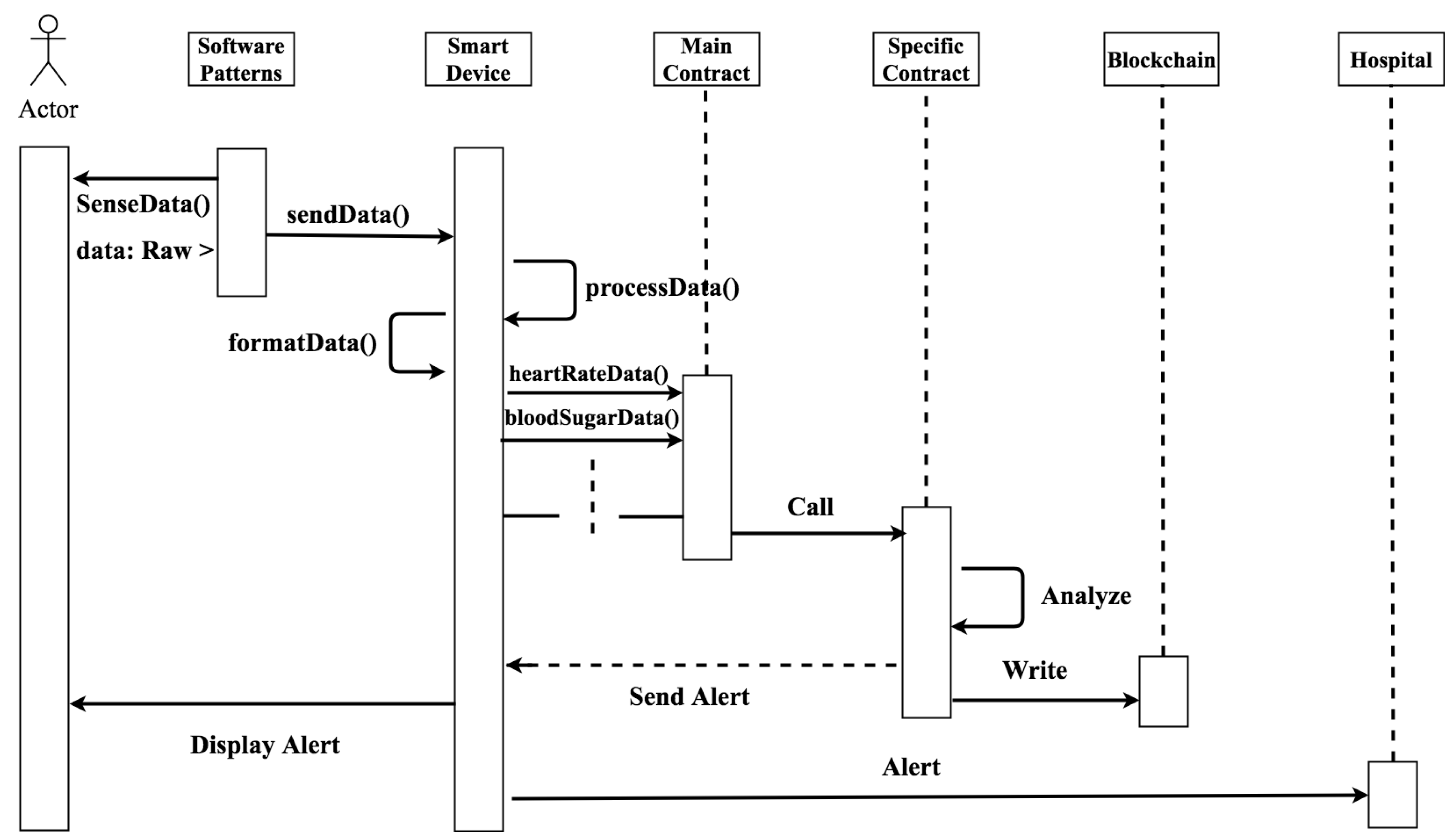
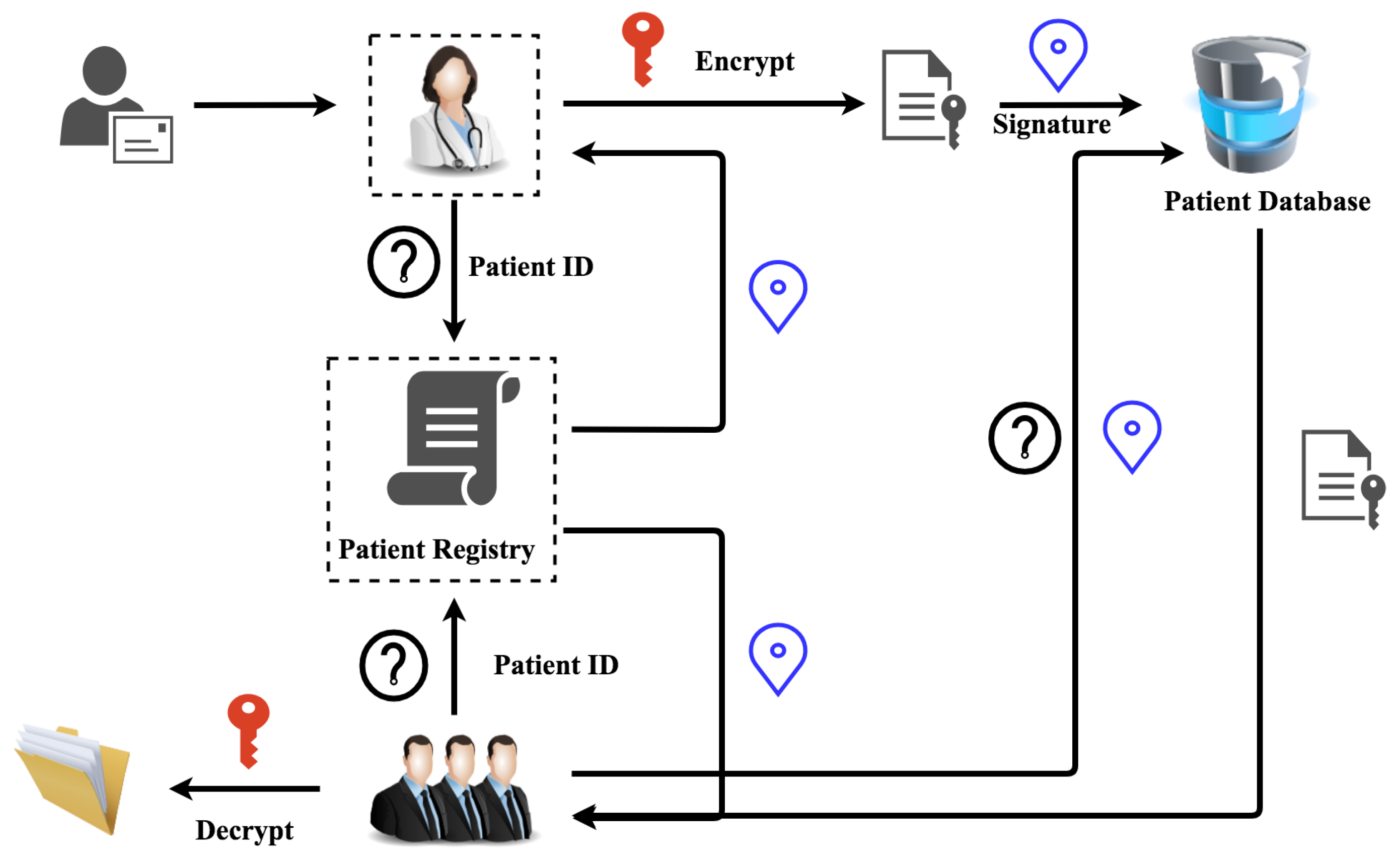
4. Case Study in Healthcare Domain
- How authenticated parties can access and retrieve healthcare data from healthcare institutions while preserving patients’ privacy
- How to ensure security of interaction between patients and the system
- How to eliminate legal and regulatory sanctions and unethical use of data when exchanging healthcare information
- How patients can access various types of data from multiple healthcare organizations using a single system.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Joshi, A.P.; Han, M.; Wang, Y. A Survey on Security and Privacy Issues of Blockchain Technology. Math. Found. Comput. 2018, 1, 121–147. [Google Scholar] [CrossRef]
- Ji, S.; Cai, Z.; Han, M.; Beyah, R. Whitespace measurement and virtual backbone construction for Cognitive Radio Networks: From the social perspective. In Proceedings of the 2015 12th Annual IEEE International Conference on Sensing, Communication and Networking, SECON 2015, Seattle, WA, USA, 22–25 June 2015; pp. 435–443. [Google Scholar]
- Han, M.; Yan, M.; Li, J.; Ji, S.; Li, Y. Generating uncertain networks based on historical network snapshots. Lect. Notes Comput. Sci. 2013, 7936, 747–758. [Google Scholar]
- Duan, Z.; Yan, M.; Cai, Z.; Wang, X.; Han, M.; Li, Y. Truthful incentive mechanisms for social cost minimization in mobile crowdsourcing systems. Sensors 2016, 16, 481. [Google Scholar] [CrossRef] [PubMed]
- Kostakis, V.; Giotitsas, C. The (A)political economy of bitcoin. TripleC 2014, 12, 431–440. [Google Scholar]
- Efanov, D.; Roschin, P. The all-pervasiveness of the blockchain technology. Procedia Comput. Sci. 2018, 123, 116–121. [Google Scholar] [CrossRef]
- Buterin, V. A Next-Generation Smart Contract and Decentralized Application Platform. Ethereum White Paper. 2014. Available online: http://blockchainlab.com/pdf/Ethereum_white_paper-a_next_generation_smart_contract_and_decentralized_application_platform-vitalik-buterin.pdf (accessed on 15 June 2018).
- Ethereum Community. A Next Generation Smart Contract and Decentralized Application Platform. Available online: https://github.com/ethereum/wiki/wiki/White-Paper (accessed on 1 April 2018).
- Underwood, S. Blockchain beyond bitcoin, Commun. ACM 2016, 59, 15–17. [Google Scholar] [CrossRef]
- Zheng, Z.; Xie, S.; Dai, H.N.; Chen, X.; Wang, H. Blockchain Challenges and Opportunities: A Survey. Int. J. Web Grid Serv. 2016. [Google Scholar] [CrossRef]
- Agbo, C.C.; Mahmoud, Q.H.; Eklund, J.M. Blockchain Technology in Healthcare: A Systematic Review. Healthcare 2019, 7, 56. [Google Scholar] [CrossRef] [PubMed]
- Akins, B.W.; Chapman, J.L.; Gordon, J.M. A Whole New World: Income Tax Considerations of the Bitcoin Economy. Pittsburgh Tax Rev. 2015, 12, 24–56. [Google Scholar] [CrossRef] [Green Version]
- Sharples, M.; Domingue, J. The Blockchain and Kudos: A Distributed System for Educational Record, Reputation and Reward. In Adaptive and Adaptable Learning; Springer: Cham, Switzerland, 2016; pp. 490–496. [Google Scholar] [Green Version]
- Zhang, Y.; Wen, J. An IoT electric business model based on the protocol of Bitcoin. In Proceedings of the 2015 18th Intternational Conference on Intelligence in Next Generation Networks, ICIN 2015, Paris, France, 17–19 February 2015; pp. 184–191. [Google Scholar]
- Noyes, C. BitAV: Fast Anti-Malware by Distributed Blockchain Consensus and Feedforward Scanning. arXiv 2016, arXiv:1601.01405. [Google Scholar]
- Kosba, A.; Miller, A.; Shi, E.; Wen, Z.; Papamanthou, C. Hawk: The Blockchain Model of Cryptography and Privacy-Preserving Smart Contracts. In Proceedings of the 37th IEEE Symposium on Security and Privacy, San Jose, CA, USA, 23–25 May 2016; pp. 839–858. [Google Scholar]
- Crosby, M.; Nachiappan; Pattanayak, P.; Verma, S.; Kalyanaraman, V. BlockChain Technology: Beyond Bitcoin. Appl. Innov. Rev. 2016, 2, 71. [Google Scholar]
- Ren, L. Proof of Stake Velocity: Building the Social Currency of the Digital Age. Self-Published White Paper. 2014. Available online: https://www.reddcoin.com/papers/PoSV.pdf (accessed on 22 July 2018).
- Kuo, T.T.; Kim, H.E.; Ohno-Machado, L. Blockchain distributed ledger technologies for biomedical and health care applications. J. Am. Med. Inf. Assoc. 2017, 24, 1211–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, T.; Ramani, V.; Ahmad, I.; Braeken, A.; Harjula, E.; Ylianttila, M. Blockchain Utilization in Healthcare: Key Requirements and Challenges. In Proceedings of the IEEE 20th International Conference on e-Health Networking, Applications and Services, Ostrava, Czech Republic, 17–20 September 2018. [Google Scholar]
- Swan, M. Blockchain: Blueprint for a New Economy; O’Reilly Media Inc: Sevastopol, CA, USA, 2015. [Google Scholar]
- McGhin, T.; Choo, R.; Liu, C.; He, D. Blockchain in healthcare applications: Research challenges and opportunities. J. Netw. Comput. Appl. 2019, 135, 62–75. [Google Scholar] [CrossRef]
- Tama, B.A.; Kweka, B.J.; Park, Y.; Rhee, K.H. A critical review of blockchain and its current applications. In Proceedings of the 2017 International Conference on Electrical Engineering and Computer Science (ICECOS), Palembang, Indonesia, 22–23 August 2017; pp. 109–113. [Google Scholar]
- Drescher, D. Blockchain Basics: A Non-Technical Introduction in 25 Steps; Apress: New York, NY, USA, 2017. [Google Scholar]
- Rutland, E. Blockchain Byte. Available online: https://docplayer.net/57510249-Blockchain-byte-r3-research-emily-rutland-the-blockchain-byte-features-a-question-from-the-distributed-ledger-space.html (accessed on 15 September 2018).
- Holbl, M.; Kompara, M.; Kamisali, A. A Systematic Review of the Use of Blockchain in Healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef]
- Lamport, L.; Shostak, R.; Pease, M. The Byzantine Generals Problem. ACM Trans. Program. Lang. Syst. 1982, 4, 382–401. [Google Scholar] [CrossRef] [Green Version]
- Merkle, R.C. A Digital Signature Based on a Conventional Encryption Function. In Advances in Cryptology—CRYPTO 1987; Lecture Notes in Computer Science 293; Springer: Berlin/Heidelberg, German, 1988; pp. 369–378. [Google Scholar] [Green Version]
- Nakamoto, S. Bitcoin: A Peer-to-Peer Electronic Cash System. Available online: www.Bitcoin.Org (accessed on 30 May 2018).
- Larimer, D. Transactions as Proof of Stake. Available online: https://bravenewcoin.com/assets/Uploads/TransactionsAsProofOfStake10.pdf (accessed on 30 May 2018).
- O’Dwyer, K.J.; Malone, D. Bitcoin Mining and its Energy Footprint. In Proceedings of the 25th IET Irish Signals Systems Conference 2014 and 2014 China-Ireland International Conference on Information and Communications Technologies, Limerick, Ireland, 26–27 June 2014. [Google Scholar]
- Gervais, A.; Karame, G.O.; Wüst, K.; Glykantzis, V.; Ritzdorf, H.; Capkun, S. On the security and performance of proof of work blockchains. In Proceedings of the ACM Conference on Computer and Communications Security (CCS), Vienna, Austria, 24–28 October 2016; pp. 3–16. [Google Scholar]
- Chuen, D.L.K. (Ed.) Handbook Of Digital Currency: Bitcoin, Innovation, Financial Instruments, and Big Data; Academic Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Sultan, K.; Ruhi, U.; Lakhani, R. Conceptualizing Blockchains: Characteristics and Applications. In Proceedings of the 11th IADIS International Conference on Information Systems 2018, Lisbon, Portugal, 14–16 April 2018; pp. 49–57. [Google Scholar]
- Bitcoin Project. nBits, Target Threshold. Available online: https://bitcoin.org/en/glossary/nbits (accessed on 8 September 2018).
- Norberhuis, S.D. MultiChain: A Cybercurrency for Cooperation. Master’s Thesis, Delft University of Technology, Delft, The Netherlands, 2015. [Google Scholar]
- Burgess, K.; Colangelo, J. The Promise of Bitcoin and the Blockchain; Consumers’ Research: Washington, DC, USA, 2015. [Google Scholar]
- Nomura Research Institute. Survey on Blockchain Technologies and Related Services; FY2015 Report. Available online: https://www.meti.go.jp/english/press/2016/pdf/0531_01f.pdf (accessed on 15 September 2018).
- Johnson, D.; Menezes, A.; Vanstone, S. The Elliptic Curve Digital Signatur e Algorithm (ECDSA). Int. J. Inf. Secur. 2001, 1, 36–63. [Google Scholar] [CrossRef]
- Kim, S.K.; Kim, U.M.; Huh, J.H. A Study to Improvement of Blockchain Application to Overcome Vulnerability of IoT Multiplatform Security. Energies 2019, 12, 402. [Google Scholar] [CrossRef]
- C. Team. CONIKS. Available online: https://coniks.cs.princeton.edu (accessed on 16 December 2018).
- Liu, B.; Yu, X.L.; Chen, S.; Xu, X.; Zhu, L. Blockchain Based Data Integrity Service Framework for IoT Data. In Proceedings of the 2017 IEEE 24th IEEE International Conference on Web Services ICWS 2017, Honolulu, HI, USA, 25–30 June 2017; pp. 468–475. [Google Scholar]
- Xu, J.J. Are blockchains immune to all malicious attacks? Financ. Innov. 2016, 2, 25. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; Zhu, D. Fraud detections for online businesses: a perspective from blockchain technology. Financ. Innov. 2016, 2, 20. [Google Scholar] [CrossRef] [Green Version]
- Karame, G.O.; Androulaki, E. Double-Spending Fast Payments in Bitcoin. In Proceedings of the 2012 ACM Conference on Computer and Communications Security, Raleigh, NC, USA, 16–18 October 2012; pp. 906–917. [Google Scholar]
- Zheng, Z.; Xie, S.; Dai, H.; Chen, X.; Wang, H. An Overview of Blockchain Technology: Architecture, Consensus, and Future Trends. In Proceedings of the 2017 IEEE 6th International Congress on Big Data: BigData Congress, Honolulu, HI, USA, 25–30 June 2017; pp. 557–564. [Google Scholar]
- Li, X.; Jiang, P.; Chen, T.; Luo, X.; Wen, Q. A survey on the security of blockchain systems. Future Gener. Comput. Syst. 2017. [Google Scholar] [CrossRef]
- Larimer, D. Delegated Proof of Stake. Available online: https://en.bitcoinwiki.org/wiki/DPoS (accessed on 10 January 2019).
- Bentov, I.; Lee, C.; Mizrahi, A.; Rosenfeld, M. Proof of Activity: Extending Bitcoin’s Proof of Work via Proof of Stake. In SIGMETRICS Performance Evaluation Reviews; ACM: New York, NY, USA, 2014. [Google Scholar]
- Vukolic, M. The quest for scalable blockchain fabric: Proof-of-work vs. BFT replication. Lect. Notes Comput. Sci. 2016, 9591, 112–125. [Google Scholar]
- Kotla, R.; Alvisi, L.; Dahlin, M.; Clement, A.; Wong, E. Zyzzyva: Speculative byzantine fault tolerance. ACM Trans. Comput. Syst. 2009, 27, 1–39. [Google Scholar] [CrossRef]
- Copeland, C.; Zhong, H. Tangaroa: A Byzantine Fault Tolerant Raft. Available online: http://www.scs.stanford.edu/14au-cs244b/labs/projects/copeland_zhong.pdf (accessed on 10 January 2019).
- Parity Technologies. Proof of Authority Chains (PoA). 2017. Available online: https://github.com/paritytech/parity/wiki/Proof-of-Authority-Chains (accessed on 12 January 2019).
- P4Titan. Slimcoin: A Peer-To-Peer Crypto-Currency with Proof-of-Burn. Available online: http://www.doc.ic.ac.uk/~ids/realdotdot/crypto_papers_etc_worth_reading/proof_of_burn/slimcoin_whitepaper.pdf (accessed on 21 January 2019).
- Borge, M.; Kokoris-Kogias, E.; Jovanovic, P.; Gasser, L.; Gailly, N.; Ford, B. Proof-of-personhood: Redemocratizing permissionless cryptocurrencies. In Proceedings of the 2nd IEEE European Symposium on Security and Privacy, Paris, France, 26–28 April 2017; pp. 23–26. [Google Scholar]
- Ghosh, M.; Richardson, M. A TorPath to TorCoin: Proof-of-Bandwidth Altcoins for Compensating Relays. In Proceedings of the HotPETs’14: 7th Workshop on Hot Topics in Privacy Enhancing Technologies, 2014; Available online: http://dedis.cs.yale.edu/dissent/papers/hotpets14-torpath-abs/ (accessed on 12 January 2019).
- Intel. Proof of Elapsed Time (PoET), 2017. Available online: http://intelledger.github.io/ (accessed on 18 January 2019).
- Mazieres, D. The Stellar Consensus Protocol: A Federated Model for Internet-Level Consensus. 2015. Available online: https://www.stellar.org/papers/stellar-consensus-protocol.pdf (accessed on 18 January 2019).
- Metropolitana, Z.; Le, N.; California, B.; Ju, C.; Ta, C.I. Bitcoin-NG: A Scalable Blockchain Protocol. In Proceedings of the 13th USENIX Symposium on Networked Systems Design and Implementation, Santa Clara, CA, USA, 16–18 March 2016. [Google Scholar]
- Cachin, C.; Schubert, S.; Vukolic, M. Non-determinism in Byzantine Fault-Tolerant Replication. In Proceedings of the Int. Conf. Princ. Distrib. Syst. (OPODIS 2016), Madrid, Spain, 13–16 December 2016; pp. 1–20. [Google Scholar]
- Schwartz, D.; Youngs, N.; Britto, A. The Ripple Protocol Consensus Algorithm. Ripple Labs Inc White Papper. 2014. Available online: https://ripple.com/files/ripple_consensus_whitepaper.pdf (accessed on 18 January 2019).
- Kwon, J. TenderMint: Consensus without Mining; 2014. Available online: https://www.weusecoins.com/assets/pdf/library/Tendermint%20Consensus%20without%20Mining.pdf (accessed on 18 January 2019).
- Kim, S.K.; Huh, J.H. A Study on the Improvement of Smart Grid Security Performance and Blockchain Smart Grid Perspective. Energies 2018, 11, 1973. [Google Scholar] [CrossRef]
- Ongaro, D.; Ousterhout, J. In search of an Undstandable Consensus Algorithm. In Proceedings of the 2014 USENIX Annual Technical Conference, Philadelphia, PA, USA, 19–20 June 2014; Volume 37, pp. 1–16. [Google Scholar]
- Rivest, Y.H.; Shamir, R.L.; Tauman, A. How to Leak a Secret. In Proceedings of the 7th International Conference on the Theory and Application of Cryptology and Information Security, Gold Coast, Australia, 9–13 December 2001; pp. 552–565. [Google Scholar]
- Syta, E.; Tamas, I.; Visher, D.; Wolinsky, D.I.; Jovanovic, P.; Gasser, L.; Gailly, N.; Khoffi, I.; Ford, B. Keeping Authorities ’Honest or Bust’ with Decentralized Witness Cosigning. In Proceedings of the 37th IEEE Symposium on Security and Privacy, San Jose, CA, USA, 23–25 May 2016. [Google Scholar]
- Saravanan, M.; Shubha, R.; Marks, A.M.; Iyer, V. SMEAD: A secured mobile enabled assisting device for diabetics monitoring. In Proceedings of the 11th IEEE International Conference on Advanced Networks and Telecommunications Systems 2017, Odisha, India, 17–20 December 2017; pp. 1–6. [Google Scholar]
- Xia, Q.; Sifah, E.B.; Asamoah, K.O.; Gao, J.; Du, X.; Guizani, M. MeDShare: Trust-Less Medical Data Sharing among Cloud Service Providers via Blockchain. IEEE Access 2017, 5, 14757–14767. [Google Scholar] [CrossRef]
- Angraal, S.; Krumholz, H.M.; Schulz, W.L. Blockchain technology: applications in health care, Circulation: Cardiovascular Quality and Outcomes. arXiv 2017, arXiv:1706.03700. [Google Scholar]
- Zhang, J.; Xue, N.; Huang, X. A secure system for pervasive social network-based healthcare. IEEE Access 2016, 4, 9239–9250. [Google Scholar] [CrossRef]
- Rabah, K. Challenges & opportunities for blockchain powered healthcare systems: A review. Mara Res. J. Med. Health 2017, 1, 45–52. [Google Scholar]
- Esposito, C.; Santis, A.D.; Tortora, G.; Chang, H.; Choo, K.K.R. Blockchain: A Panacea for Healthcare Cloud-Based Data Security and Privacy? IEEE Cloud Comput. 2018, 5, 31–37. [Google Scholar] [CrossRef]
- Raseena, M.; Harikrishnan, G.R. Secure Sharing Of Personal Health Records in Cloud Computing Using Attribute-Based Broadcast Encryption. Int. J. Sci. Eng. Res. 2013, 1, 323–325. [Google Scholar]
- Omar, A.A.; Rahman, M.S.; Kiyomoto, A.B. MediBchain A Blockchain Based Privacy Preserving Platform for Healthcare Data. In Proceedings of the International Conference on Security, Privacy and Anonymity in Computation, Communication and Storage, Guangzhou, China, 12–15 December 2017. [Google Scholar]
- Karame, G.O.; Roeschlin, M.; Gervais, A.; Capkun, S.; Androulaki, E.; Čapkun, S. Misbehavior in Bitcoin: A Study of Double-Spending and Accountability. ACM Trans. Inf. Syst. Secur. 2015, 18, 2. [Google Scholar] [CrossRef]
- Dwivedi, A.D.; Srivastava, G.; Dhar, S.; Singh, R. A Decentralized Privacy-Preserving Healthcare Blockchain for IoT. Sensors 2019, 19, 326. [Google Scholar] [CrossRef] [PubMed]
- Giardina, T.D.; Menon, S.; Parrish, D.E.; Sittig, D.F.; Singh, H. Patient access to medical records and healthcare outcomes: a systematic review. J. Am. Med. Inform. Assoc. 2013, 21, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Engelhardt, M.A. Hitching healthcare to the chain: An introduction to blockchain technology in the healthcare sector. Technol. Innov. Manag. Rev. 2017, 7, 22–34. [Google Scholar] [CrossRef]
- Kuo, T.T.; Rojas, H.Z.; Ohno-Machado, L. Comparison of blockchain platforms: A systematic review and healthcare examples. J. Am. Med. Inform. Assoc. 2019, 26, 462–478. [Google Scholar] [CrossRef] [PubMed]
- Peterson, K.; Deeduvanu, R.; Kanjamala, P.; Boles, K. A Blockchain-Based Approach to Health Information Exchange Networks. Proc. NIST Workshop Blockchain Healthc. 2016, 1, 1–10. [Google Scholar]
- Xia, Q.; Sifah, E.B.; Smahi, A.; Amofa, S.; Zhang, X. BBDS: Blockchain-based data sharing for electronic medical records in cloud environments. Information 2017, 8, 44. [Google Scholar] [CrossRef]
- Theodouli, A.; Arakliotis, S.; Moschou, K.; Votis, K. On the design of a Blockchain-based system to facilitate Healthcare Data Sharing. In Proceedings of the 12th IEEE International Conference On Big Data Science and Engineering (TrustCom/BigDataSE), New York, NY, USA, 1–3 August 2018. [Google Scholar]
- Mcfarlane, C.; Beer, M.; Brown, J.; Prendergast, N. Patientory: A Healthcare Peer-to-Peer EMR Storage Network v1.0; Entrust Inc.: Addison, TX, USA, 2017. [Google Scholar]
- Amofa, S.; Sifah, E.B.; Kwame, O.B.; Abla, S.; Xia, Q.; Gee, J.C.; Gao, J. A Blockchain-based Architecture Framework for Secure Sharing of Personal Health Data. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018. [Google Scholar]
- Zheng, X.; Mukkamala, R.R.; Vatrapu, R.; Ordieres-Mere, J. Blockchain-based personal health data sharing system using cloud storage. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018. [Google Scholar]
- Daemen, J.; Rijmen, V. The design of Rijndael: AES-The Advanced Encryption Standard; Springer Science and Business Media: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Desmedt, Y. Threshold cryptosystems. In Proceedings of the International Conference on the Theory and Application of Cryptology and Information Security 1992, QLD, Australia, 13–16 December 1992; pp. 1–14. [Google Scholar]
- Shen, B.; Guo, J.; Yang, Y. MedChain: Efficient Healthcare Data Sharing via Blockchain. Appl. Sci. 2019, 9, 1207. [Google Scholar] [CrossRef]
- Koblitz, N. Elliptic curve cryptosystems. Math. Comput. 1987, 48, 203–209. [Google Scholar] [CrossRef]
- Azaria, A.; Ekblaw, A.; Vieira, T.; Lippman, A. MedRec: Using blockchain for medical data access and permission management. In Proceedings of the 2016 2nd International Conference on Open Big Data, OBD 2016, Vienna, Austria, 22–24 August 2016; pp. 25–30. [Google Scholar]
- Ekblaw, A.; Azaria, A.; Halamka, J.D.; Lippman, A. A Case Study for Blockchain in Healthcare: ‘MedRec’ prototype for electronic health records and medical research data. In Proceedings of the IEEE BigData 2016: IEEE International Conference on Big Data, Washington, DC, USA, 5–8 December 2016. [Google Scholar]
- Conceiçao, A.F.; da Silva, F.S.C.; Rocha, V.; Locoro, A.; Barguil, J.M. Eletronic Health Records using Blockchain Technology. arXiv 2018, arXiv:1804.10078. [Google Scholar]
- Fan, K.; Wang, S.; Ren, Y.; Li, H.; Yang, Y. MedBlock: Efficient and Secure Medical Data Sharing Via Blockchain. J. Med. Syst. 2018, 42, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dubovitskaya, A.; Xu, Z.; Ryu, S.; Schumacher, M.; Wang, F. Secure and Trustable Electronic Medical Records Sharing using Blockchain. Am. Med. Inf. Assoc. 2018, 2017, 650–659. [Google Scholar]
- Salahuddin, M.A.; Al-Fuqaha, A.; Guizani, M.; Shuaib, K.; Sallabi, F. Softwarization of internet of things infrastructure for secure and smart healthcare. IEEE Comput. Mag. 2017, 50, 74–79. [Google Scholar] [CrossRef]
- Hussein, A.F.; ArunKumar, N.; Ramirez-Gonzalez, G.; Abdulhay, E.; Tavares, J.M.R.S.; de Albuquerque, V.H.C. A medical records managing and securing blockchain based system supported by a Genetic Algorithm and Discrete Wavelet Transform. Cogn. Syst. Res. 2018, 52, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Holland, J.H. Adaptation in Natural and Artificial Systems: An Introductory Analysis with Applications to Biology, Control, and Artificial Intelligence; MIT Press: Cambridge, MA, USA, 1992. [Google Scholar]
- Shensa, M.J. The discrete wavelet transform: Wedding the a trous and Mallat algorithms. IEEE Trans. Signal Process. 1992, 40, 2464–2482. [Google Scholar] [CrossRef]
- Kotsiuba, I.; Velvkzhanin, A.; Yanovich, Y.; Bandurova, I.S.; Dyachenko, Y.; Zhygulin, V. Decentralized e-Health Architecture for Boosting Healthcare Analytics. In Proceedings of the 2018 Second World Conference on Smart Trends in Systems, Security and Sustainability (WorldS4), Lodon, UK, 30–31 October 2018; pp. 113–118. [Google Scholar]
- What Is Exonum? Available online: https://exonum.com/doc/getstarted/what-is-exonum/ (accessed on 19 January 2019).
- Jiang, S.; Cao, J.; Wu, H.; Yang, Y.; Ma, M.; He, J. Blochie: A blockchain-based platform for healthcare information exchange. In Proceedings of the SMARTCOMP 2018: The 4th IEEE International Conference on Smart Computing, Sicily, Italy, 18–20 June 2018; pp. 49–56. [Google Scholar]
- Cichosz, S.L.; Stausholm, M.N.; Kronborg, T.; Vestergaard, P.; Hejlesen, O. How to Use Blockchain for Diabetes Health Care Data and Access Management: An Operational Concept. J. Diabetes Sci. Technol. 2018, 13, 248–253. [Google Scholar] [CrossRef]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G.; Rosenbloom, S.T. FHIRChain: Applying Blockchain to Securely and Scalably Share Clinical Data. Comput. Struct. Biotechnol. J. 2018, 16, 267–278. [Google Scholar] [CrossRef]
- Guo, R.; Shi, H.; Zhao, Q.; Zheng, D. Secure Attribute-Based Signature Scheme with Multiple Authorities for Blockchain in Electronic Health Records Systems. IEEE Access 2018, 6, 11676–11686. [Google Scholar] [CrossRef]
- Yue, X.; Wang, H.; Jin, D.; Li, M.; Jiang, W. Healthcare Data Gateways: Found Healthcare Intelligence on Blockchain with Novel Privacy Risk Control. J. Med. Syst. 2016, 40, 218. [Google Scholar] [CrossRef]
- Liang, X.; Zhao, J.; Shetty, S.; Liu, J.; Li, D. Integrating Blockchain for Data Sharing and Collaboration in Mobile Healthcare Applications. In Proceedings of the PIMRC 2017: 28th Annual IEEE International Symposium on Personal, Indoor and Mobile Radio Communications, Montreal, QC, Canada, 8–13 October 2017. [Google Scholar]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G. Design of Blockchain-Based Apps Using Familiar Software Patterns to Address Interoperability Challenges in Healthcare. 2015. Available online: https://www.dre.vanderbilt.edu/~schmidt/PDF/PLoP-2017-blockchain.pdf (accessed on 20 November 2018).
- Kuo, T.; Ohno-Nachado, L. ModelChain: Decentralized Privacy-Preserving Healthcare Predictive Modeling Framework on Private Blockchain Networks. arXiv 2018, arXiv:1802.01746. [Google Scholar]
- Dagher, G.G.; Mohler, J.; Milojkovic, M.; Marella, P.B. Ancile: Privacy-preserving framework for access control and interoperability of electronic health records using blockchain technology. Sustain. Cities Soc. 2018, 39, 283–297. [Google Scholar] [CrossRef]
- Zhang, A.; Lin, X. Towards secure and privacy-preserving data sharing in e-health systems via consortium blockchain. J. Med. Syst. 2018, 42, 140. [Google Scholar] [CrossRef] [PubMed]
- Griggs, K.N.; Ossipova, O.; Kohlios, C.P.; Baccarini, A.N.; Howson, E.A.; Hayajneh, T. Healthcare Blockchain System Using Smart Contracts for Secure Automated Remote Patient Monitoring. J. Med. Syst. 2018, 42, 130. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; White, J.; Schmidt, D.C.; Lenz, G. Applying Software Patterns to Address Interoperability in Blockchain-based Healthcare Apps. arXiv 2017, arXiv:1706.03700. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Algorithm | Advantages | Drawbacks |
|---|---|---|
| Proof of Work (PoW) | * Provides comprehensive decentralization of power and control in the network More secure network | * High processing power (expensive) High electricity consumption Small networks can be compromised |
| Proof of Stake (PoS) | * More energy efficient Better rewards with bigger stakes Provides faster processing of transactions | * Less decentralized network than PoW Less security than PoW |
| Delegated Proof of Stake (DPoS) | * Faster processing than PoW and PoS Better rewards distribution Energy efficiency Lower hardware expenses | * More susceptible to attacks Richer people control the network Less resiliency due to less decentralization |
| Transactions as Proof of Stake (TaPos) | * More security than PoS since all nodes contribute in the network Provides a simplified PoS algorithm | * Lower speed than DPoS since all nodes included Does not work well when there are short forks on the blockchain |
| Proof of Activity (PoA) | * High security Eliminates 51% attack in blockchain network Improve network topology Low transaction fees | * Requires large amount of resources in mining phase Stakeholders have the ability to double sign transactions Difficult to implement |
| Practical Byzantine Fault Tolerance (PBFT) | * Ability to make transactions without the need of confirmation like in PoW Significant energy usage reduction | * Works only in small consensus group sizes due to a high amount of communication between nodes PBFT uses MACs which is extremely inefficient compared to the communication needed Hard to prove the authenticity of a message to third parties Susceptible to Sybil attacks |
| Delegated BFT (DBFT) | * Provides perfect finality (confirmation of transactions) No forks with DBFT Fast transaction execution | * Susceptible 51% attack Still considered centralized |
| Steller Consensus Protocol (SCP) | * Efficient decentralized control with large network Low latency Flexible trust & asymptotic security | * Fits finance better than any other systems Problem with choosing quorums and propose new arguments Inefficient in terms of number of sent messages |
| Ripple | * Fast transactions Low power consumption compared to PoW Path dependent; the chain is uneditable No capacity limitation for the number of transactions | * Unique Node Lists (UNLs) must be maintained, if UNLs is broken, the network might collapse It is highly centralized |
| BFTRaft | * Can tolerate failure of up to 1/2 of the node count Design simplicity and robustness | The current implementation can only be considered to guarantee liveness for one Byzantine failure |
| Tendermint | Similar to PoS | Similar to PoS |
| Proof-of-Burn (PoB) | * Encourages long-term involvement PoB implementation can be customized The power of burnt coins “decays” or reduces partially each time a new block is mined | * Rich get richer problem Resource waste (the burnt coins are wasted) High risk protocol, no coin recovery guarantee |
| Proof-of- Personhood (PoP) | Eliminates PoW and PoS disadvantages | Fits finance better than any other systems |
| Advantages | Limitations |
|---|---|
| Data Sharing Network/System [80,81,82,83] | |
| Ref. [80] provide high network security. Ref. [81] is lightweight, scalable, and provides efficiency, identity management and distant access. | Ref. [80] does not insert actual records in the block, and searchability, discoverability, and data access control mechanisms are required. Algorithms between entities and authentication and communication protocols were not investigated in ref. [81]. |
| Record Management System [67,68,90,91,92,93,94,95,96] | |
| Ref. [90,91] provides easy access, immutable log, and comprehensive services. It also avoids single point of failure. Ref. [92] delegates data management to patients; thus, patients have full control over their, medical records. Ref. [93] provides efficient access and retrieval, eliminates network congestion, high information security. Ref. [68] ensures data provenancing, security, auditability, and user verification. It provides distant access and data access revocation. Ref. [94] reduces sharing time and overall cost while improving decision making. Ref. [95] maintains comprehensive patient records and provides a holistic perspective of patient’s condition. Ref. [96] enhances overall security and access control, allows fast verification process and further accountability. | Ref. [90,91] does not consider contract encryption, auditability, obfuscation, and scalability. The design needs to be extended for complex scenarios regarding healthcare data. In ref. [92], problem may occurs if user is not tech-savvy, or a user’s private key is lost, which might result in data loss or compromise. Ref. [93] reduces the concept of decentralization since they are stored in local databases. Ref. [68] neglected data disclosure concerns. Ref. [94] is lack of efficient storage mechanism. In ref. [96], the system can be controlled for greater expandability. This would help augment system resources and enhance the security. |
| Medical Data Exchange/Delivery/Access, Platform/Architecture/Scheme [101,102,103,104] | |
| Ref. [101] ensures off-chain storage, on-chain verification. Proved practicability and effectiveness. In ref. [102], patients have full control, allows cross-intuitional sharing. Ref. [104] provides unforgeability, high security, and perfect privacy. | In ref. [102], lack of access during emergency situation. In ref. [103], semantic interoperability is not addressed, compatibility issue with legacy systems, cannot control clinical malpractice and cost of DApp deployment. In ref. [104], when number of users increase, cost increases and the amount of medical data become large. |
| Application Architecture to Manage Health Records [105,106,107] | |
| Ref. [105] provides anonymization, efficient communication between HDGs and data backup and recovery using cloud. Ref. [106] ensure scalability and performance stability, and handle the large amount of medical data. Ref. [107] maintains system evolvability, data storage requirements, scalability, and balancing interoperability with privacy concerns. | Ref. [105] is unable to process data and performs computations without revealing the data. In ref. [106], the system can also be extended to accommodate the usage of health data for research purposes. |
| PSN-Based Healthcare System [70] | |
| It provides message authentication, secret keys confidentiality, secrecy of master key, and integrity of transactions. It eliminates computational burden and data leakage. | Does not explore the benefits of the blockchain (no smart contracts), it is not evaluated for large-scale environments and it is designed to address challenges in PSN networks only. |
| Privacy Preserving Platform/Framework [74,108,109] | |
| Ref. [108] adopts permissioned blockchain networks, malicious nodes could not arbitrarily participate in the network, and therefore the risk of a 51% attack is minimal. ModelChain framework utilizes a private blockchain to enable multiple institutions to contribute health data to train a machine-learning model without disclosing their individual health records. | In ref. [74], flaws in encryption algorithms or software implementations may expose the data contents. Ref. [108] requires further security improvement through encrypting transaction metadata and using Virtual Private Network (VPN). Ref. [109] consumes computational power due to high number of used smart contracts. Need to look for methods to effectively search smart contracts with large local databases or to eliminate the needs of 850 for global smart contracts. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zubaydi, H.D.; Chong, Y.-W.; Ko, K.; Hanshi, S.M.; Karuppayah, S. A Review on the Role of Blockchain Technology in the Healthcare Domain. Electronics 2019, 8, 679. https://doi.org/10.3390/electronics8060679
Zubaydi HD, Chong Y-W, Ko K, Hanshi SM, Karuppayah S. A Review on the Role of Blockchain Technology in the Healthcare Domain. Electronics. 2019; 8(6):679. https://doi.org/10.3390/electronics8060679
Chicago/Turabian StyleZubaydi, Haider Dhia, Yung-Wey Chong, Kwangman Ko, Sabri M. Hanshi, and Shankar Karuppayah. 2019. "A Review on the Role of Blockchain Technology in the Healthcare Domain" Electronics 8, no. 6: 679. https://doi.org/10.3390/electronics8060679
APA StyleZubaydi, H. D., Chong, Y. -W., Ko, K., Hanshi, S. M., & Karuppayah, S. (2019). A Review on the Role of Blockchain Technology in the Healthcare Domain. Electronics, 8(6), 679. https://doi.org/10.3390/electronics8060679