

Improving the Response of Health Systems to Female Genital Schistosomiasis in Endemic Countries through a Gender-Sensitive Human Rights-Based Framework
Abstract
:1. Introduction
1.1. FGS: Biological Manifestations
1.2. FGS: A Gender and Human Rights Issue
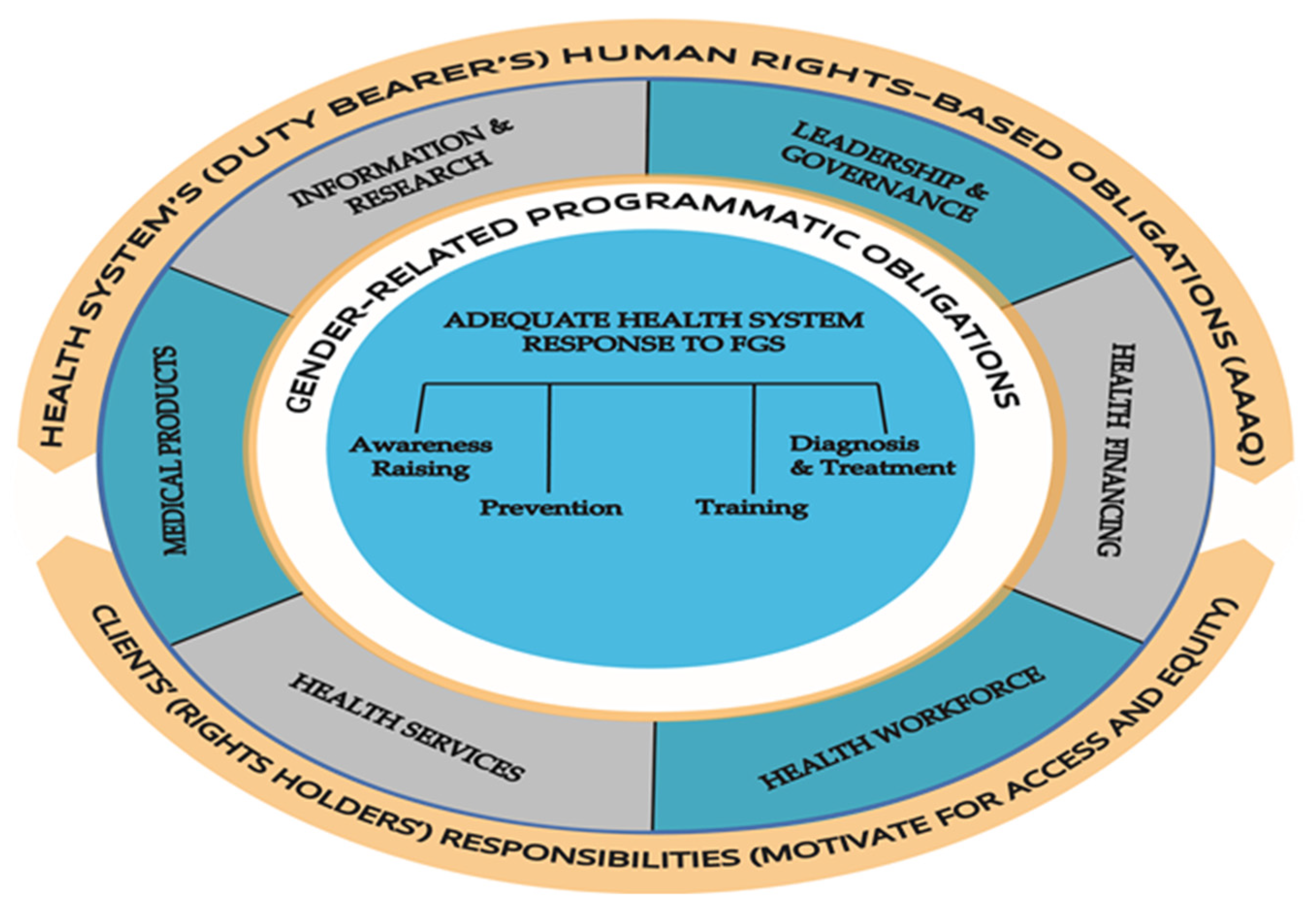
1.3. The Framework
2. Materials and Methods
3. Results
3.1. Applying the Framework
- (a)
- Health system (duty bearer) and Female Genital Schistosomiasis
3.2. Awareness Raising
3.3. Prevention of Infection
3.4. Training of Health Personnel
3.5. Diagnosis and Treatment
- (b)
- Clients (Rights Holders) and FGS
3.6. Access to Discrimination-Free Health Facilities, Goods and Services
3.7. Access to Essential Drugs
3.8. Equitable Distribution of All Health Facilities and Goods and Services
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNAIDS, World Health Organization. No More Neglect. Female Genital Schistosomiasis and HIV [Internet]; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.unaids.org/en/resources/documents/2019/female_genital_schistosomiasis_and_hiv (accessed on 30 July 2022).
- Kjetland, E.F.; Gwanzura, L.; Ndhlovu, P.D.; Mduluza, T.; Gomo, E.; Mason, P.R.; Midzi, N.; Friis, H.; Gundersen, S.G. Herpes simplex virus types 2 prevalence of epidemic proportions in rural Zimbabwean women: Association with other sexually transmitted infections. Arch. Gynecol. Obstet. 2005, 272, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Christinet, V.; Lazdins-Helds, J.K.; Stothard, J.R.; Reinhard-Rupp, J. Female genital schistosomiasis (FGS): From case reports to a call for concerted action against this neglected gynaecological disease. Int. J. Parasitol. 2016, 46, 395–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotez, P.J.; Engels, D.; Gyapong, M.; Ducker, C.; Malecela, M.N. Female genital schistosomiasis. NEJM 2019, 381, 2493–2495. [Google Scholar] [CrossRef] [PubMed]
- Ekpo, U.F.; Odeyemi, O.M.; Sam-Wobo, S.O.; Onunkwor, O.B.; Mogaji, H.O.; Oluwole, A.S.; Abdussalam, H.O.; Stothard, J.R. Female genital schistosomiasis (FGS) in Ogun State, Nigeria: A pilot survey on genital symptoms and clinical findings. Parasitol. Open 2017, 3, E10. [Google Scholar] [CrossRef] [Green Version]
- Yirenya-Tawiah, D.; Amoah, C.; Apea-Kubi, K.A.; Dade, M.; Ackumey, M.; Annang, T.; Mensah, D.Y.; Bosompem, K.M. A survey of female genital schistosomiasis of the lower reproductive tract in the volta basin of Ghana. Ghana Med. J. 2011, 45, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Downs, J.A.; Mguta, C.; Kaatano, G.M.; Mitchell, K.B.; Bang, H.; Simplice, H.; Kalluvya, S.E.; Changalucha, J.M.; Johnson, W.D., Jr.; Fitzgerald, D.W. Urogenital schistosomiasis in women of reproductive age in Tanzania’s Lake Victoria region. Am. J. Trop. Med. Hyg. 2011, 84, 364–369. [Google Scholar] [CrossRef] [Green Version]
- Kjetland, E.F.; Poggensee, G.; Helling-Giese, G.; Richter, J.; Sjaastad, A.; Chitsulo, L.; Kumwenda, N.; Gundersen, S.G.; Krantz, I.; Feldmeier, H. Female genital schistosomiasis due to Schistosoma haematobium: Clinical and parasitological findings in women in rural Malawi. Acta Trop. 1996, 62, 239–255. [Google Scholar] [CrossRef]
- Engels, D.; Hotez, P.J.; Ducker, C.; Gyapong, M.; Bustinduy, A.L.; Secor, W.E.; Harrison, W.; Theobald, S.; Thomson, R.; Gamba, V.; et al. Integration of prevention and control measures for female genital schistosomiasis, HIV and cervical cancer. Bull. World Health Organ. 2020, 98, 615–624. [Google Scholar] [CrossRef]
- Jacobson, J.; Pantelias, A.; Williamson, M.; Kjetland, E.F.; Krentel, A.; Gyapong, M.; Mbabazi, P.S.; Djirmay, A.G. Addressing a silent and neglected scourge in sexual and reproductive in Sub-Saharan Africa by development of training competencies to improve prevention, diagnosis, and treatment of female genital schistosomiasis (FGS) for health workers. Reprod. Health 2022, 19, 20. [Google Scholar] [CrossRef]
- Brodish, P.H.; Singh, K. Association between Schistosoma haematobium exposure and human immunodeficiency virus infection among females in Mozambique. Am. J. Trop. Med. Hyg. 2016, 94, 1040–1044. [Google Scholar] [CrossRef]
- Downs, J.A.; Dupnik, K.M.; van Dam, G.J.; Urassa, M.; Lutonja, P.; Kornelis, D.; de Dood, C.J.; Hoekstra, P.; Kanjala, C.; Isingo, R.; et al. Effects of schistosomiasis on susceptibility to HIV-1 infection and HIV-1 viral load at HIV-1 seroconversion: A nested case-control study. PLoS Negl. Trop. Dis. 2017, 11, 1–15. [Google Scholar] [CrossRef]
- Kjetland, E.F.; Ndhlovu, P.D.; Gomo, E.; Mduluza, T.; Midzi, N.; Gwanzura, L.; Mason, P.R.; Sandvik, L.; Friis, H.; Gundersen, S.G. Association between genital schistosomiasis and HIV in rural Zimbabwean women. Aids 2006, 20, 593–600. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Female Genital Schistosomiasis. A Pocket Atlas for Clinical Health Care Professionals. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/180863/9789241509299_eng.pdf?sequence=1 (accessed on 11 July 2022).
- Holmen, S.D.; Onsrud, M.; Vennervald, B.J.; Albregtsen, F.; Taylor, M.; Moodley, J.; Van Lieshout, L.; Pillay, P.; Lillebo, K.; Kleppa, E.; et al. Diagnosing female genital schistosomiasis. 16th ICID Abstracts. Int. J. Infect. Dis. 2014, 21S, 1–460. [Google Scholar]
- Galappaththi-Arachchige, H.N.; Holmen, S.; Koukounari, A.; Kleppa, E.; Pillay, P.; Sebitloane, M.; Ndhlovu, P.D.; van Lieshout, L.; Vennervald, B.J.; Gundersen, S.G.; et al. Evaluating diagnostic indicators of urogenital Schistosoma haematobium infection in young women: A cross sectional study in rural South Africa. PLoS ONE 2018, 13, e0191459. [Google Scholar] [CrossRef] [Green Version]
- Norseth, H.M.; Ndhlovu, P.D.; Kleppa, E.; Randrianasolo, B.S.; Jourdan, P.M.; Roald, B.; Holmen, S.D.; Gundersen, S.G.; Bagratee, J.; Onsrud, M.; et al. The colposcopic atlas of schistosomiasis in the lower female genital tract based on studies in Malawi, Zimbabwe, Madagascar and South Africa. PLoS Negl. Trop. Dis. 2014, 8, e3229. [Google Scholar] [CrossRef] [Green Version]
- Randrianasolo, B.S.; Jourdan, P.M.; Ravoniarimbinina, P.; Ramarokoto, C.E.; Rakomanana, F.; Ravaoalimalala, V.E.; Gundersen, S.G.; Feldmeier, H.; Vennervald, B.J.; van Lieshout, L.; et al. Gynecological manifestations, histopathological findings, and schistosoma-specific polymerase chain reaction results among women with schistosoma haematobium infection: A Cross-sectional study in Madagascar. J. Infect. Dis. 2015, 212, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Kjetland, E.F.; Leutscher, P.D.; Ndhlovu, P.D. A review of female genital schistosomiasis. Trends Parasitol. 2012, 28, 58–65. [Google Scholar] [CrossRef]
- Miller-Fellows, S.C.; Howard, L.; Kramer, R.; Hildebrand, V.; Furin, J.; Mutuku, F.M.; Muuoko, D.; Ivy, J.A.; King, C.H. Cross-sectional interview study of fertility, pregnancy, and urogenital schistosomiasis in coastal Kenya: Documented treatment in childhood is associated with reduced odds of subfertility among adult women. PLoS Negl. Trop. Dis. 2017, 11, e0006101. [Google Scholar] [CrossRef] [Green Version]
- Bergquist, R.; Utzinger, J.; Keiser, J. Controlling schistosomiasis with praziquantel: How much longer without a viable alternative? Infect. Dis. Poverty 2017, 6, 74. [Google Scholar] [CrossRef] [Green Version]
- Hailegebriel, T.; Nibret, E.; Munshea, A. Efficacy of praziquantel for the treatment of human schistosomiasis in Ethiopia: A systematic review and meta-analysis. J. Trop. Med. 2021, 2021, 2625255. [Google Scholar] [CrossRef]
- Kukula, V.A.; MacPherson, E.E.; Honam Tsey, I.; Russell Stothard, J.; Theobald, S.; Gyapong, M. A major hurdle in the elimination of urogenital schistosomiasis revealed: Identifying key gaps in knowledge and understanding of female genital schistosomiasis within communities and local health workers. PLoS Negl. Trop. Dis. 2019, 13, e0007207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayabina, D.V.; Clark, J.; Bayley, H.; Lamberton, P.H.L.; Toor, J.; Hollingsworth, T.D. Gender-related differences in prevalence, intensity and associated risk factors of Schistosoma infections in Africa: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2021, 15, e0009083. [Google Scholar] [CrossRef] [PubMed]
- Yirenya-Tawiah, D.R.; Ackumey, M.M.; Bosompem, K.M. Knowledge and awareness of genital involvement and reproductive health consequences of urogenital schistosomiasis in endemic communities in Ghana: A cross-sectional study. Reprod. Health 2016, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Mazigo, H.D.; Samson, A.; Lambert, V.J.; Kosia, A.L.; Ngoma, D.D.; Murphy, R.; Matungwa, D.J. “We know about schistosomiasis but we know nothing about FGS”: A qualitative assessment of knowledge gaps about female genital schistosomiasis among communities living in Schistosoma haematobium endemic districts of Zanzibar and Northwestern Tanzania. PLoS Negl. Trop. Dis. 2021, 15, e0009789. [Google Scholar] [CrossRef] [PubMed]
- Odhiambo, G.O.; Musuva, R.M.; Atuncha, V.O.; Mutete, E.T.; Odiere, M.R.; Onyango, R.O.; Alaii, J.A.; Mwinzi, P.N.M. Low levels of awareness despite high prevalence of schistosomiasis among communities in Nyalenda Informal Settlement, Kisumu City, Western Kenya. PLoS Negl. Trop. Dis. 2014, 8, e2784. [Google Scholar] [CrossRef]
- Hotez, P.; Whitham, M. Helminth infections: A new global women’s health agenda. Obstet Gynecol. 2014, 123, 155–160. [Google Scholar] [CrossRef]
- Gyapong, M.; Theobald, S. The Sexual and Reproductive Health Issue You’ve Probably Never Heard of.... Why is One of the Most Common Gynaecological Conditions in Sub-Saharan Africa, Schistosomiasis, Misunderstood, under-Researched and Under-Reported? Open Democr. 2015. Available online: https://www.opendemocracy.net/en/5050/sexual-and-reproductive-health-issue-youve-probably-never-hear/ (accessed on 5 June 2022).
- Krentel, A.; Steben, M. A Call to Action: Ending the Neglect of Female Genital Schistosomiasis. J. Obstet. Gynaecol. Can. 2021, 43, 3–4. [Google Scholar] [CrossRef]
- Williams, C.R.; Seunik, M.; Meier, B.M. Human rights as a framework for eliminating female genital schistosomiasis. PLoS Negl. Trop. Dis. 2022, 16, e0010165. [Google Scholar] [CrossRef]
- Global Schistosomiasis Alliance. WHO and UNAIDS Launch Call to Integrate Female Genital Schistosomiasis (FGS) in Women’s Health Services. 16 December 2019. Available online: https://www.eliminateschisto.org/news-events/news/who-and-unaids-launch-call-to-integrate-female-genital-schistosomiasis-fgs-in (accessed on 10 June 2022).
- Vlassoff, C.; St John, R. A human rights-based framework to assess gender equality in health systems: The example of Zika virus in the Americas. Glob. Health Action. 2019, 11 (Suppl. S3). [Google Scholar] [CrossRef]
- FGS Accelerated Package Scale Together (FAST) Package Project. Available online: https://schistosomiasiscontrolinitiative.org/projects/fast-research-project (accessed on 13 June 2022).
- United Nations Sustainable Development Group. The Human Rights Based Approach to Development Cooperation towards a Common Understanding among UN Agencies. 2003. Available online: https://unsdg.un.org/resources/human-rights-based-approach-development-cooperation-towards-common-understanding-among-un (accessed on 15 May 2022).
- Pan American Health Organization. Women’s Health Needs Still Not Adequately Met, According to New Articles in the Pan American Journal of Public Health. 2015. Available online: http://www.paho.org/hq/index.php?option=com_content&view=article&id=11074&Itemid=1926&lang=en (accessed on 1 July 2022).
- Starrs, A.M.; Ezeh, A.C.; Barker, G.; Basu, A.; Bertrand, J.T.; Blum, R.; Coll-Seck, A.M.; Grover, A.; Laski, L.; Roa, M.; et al. Accelerate progress—Sexual and reproductive health and rights for all: Report of the Guttmacher–Lancet Commission. Lancet 2018, 391, 2642–2692. [Google Scholar] [CrossRef]
- Office of the High Commissioner for Human Rights. CESCR General Comment no. 14: The Right to the Highest Attainable Standard of Health (Art. 12) Adopted at the Twenty-Second Session of the Committee on Economic, Social and Cultural Rights, on 11 August 2000. (Contained in Document E/C.12/2000/4). Available online: http://www.refworld.org/pdfid/4538838d0.pdf (accessed on 12 June 2022).
- Hofbauer, H. Budgeting for Human Rights: Progressive Realization. 2017. Available online: https://www.globalpolicy.org/component/content/article/218-injustice-and-inequality/52692-budgeting-for-human-rights-progressive-realization.html (accessed on 30 June 2022).
- World Health Organization. World Health Report 2007. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes. WHO’s Framework for Action; WHO Press: Geneva, Switzerland, 2008; Available online: http://www.who.int/healthsystems/strategy/everybodys_business.pdf (accessed on 10 June 2022).
- World Health Organization. Deworming Adolescent Girls and Women of Reproductive Age. Policy Brief. Available online: https://www.who.int/publications/i/item/9789240037670 (accessed on 28 July 2022).
- World Health Organization. Ending the Neglected to Attain the Sustainable Development Goals: A Roadmap for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Chimbatata, N.B.; Malimba, C. Infertility in sub-Saharan Africa: A Woman’s issue for how long? A qualitative review of literature. JSS 2016, 4, 96–102. [Google Scholar] [CrossRef]
- Torres-Vitolas, C.A.; Dhanani, N.; Fleming, F.M. Factors affecting the uptake of preventive chemotherapy treatment for schistosomiasis in Sub-Saharan Africa: A systematic review. PLoS Negl. Trop. Dis. 2021, 15, e0009017. [Google Scholar] [CrossRef]
- Palanisamy, B.; Gopichandran, V.; Kosalram, K. Social capital, trust in health information, and acceptance of Measles–Rubella vaccination campaign in Tamil Nadu: A case–control study. JGPM 2018, 64, 212–219. [Google Scholar]
- de Carvalho, A.R.; Mello Silva, C.C. Phytochemical molluscicides and schistosomiasis: What we know and what we still need to learn. Vet Sci. 2018, 5, 94. [Google Scholar] [CrossRef] [Green Version]
- Secor, W.E. Early lessons from schistosomiasis mass drug administration programs. F1000Research 2015, 4. Faculty Rev-1157. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Schistosomiasis. Available online: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 14 June 2022).
- Stauffe, J.R.; Madsen, H. A one health approach to reducing schistosomiasis transmission in Lake Malawi. Prev. Med. Commun. Health 2018, 1, 1–4. [Google Scholar] [CrossRef]
- Patel, P.; Rose, C.E.; Kjetland, E.F.; Downs, J.A.; Mbabazi, P.S.; Sabin, K.; Chege, W.; Watts, D.H.; Secor, W.E. Association of schistosomiasis and HIV infections: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 102, 544–553. [Google Scholar] [CrossRef]


{kind=link}
| Health System (Duty Bearer) Perspective | Gender-Related Programmatic Obligations | |||
|---|---|---|---|---|
| Awareness Raising | Prevention of Infection | Training of Health Personnel | Diagnosis and Treatment | |
| 1. Leadership and Governance (Building Block 1) |
|
|
|
|
| Are Obligation Met (Yes/No, Comment) | ||||
| 2. Health Financing (Building Block 2) |
|
|
|
|
| Obligation Met (Yes/No, Comment) | ||||
| 3. Health Workforce (Building Block 3) |
|
|
|
|
| Obligation Met (Yes/No, Comment) | ||||
| 4. Health Services (Building Block 4) |
|
|
|
|
| Obligation Met (Yes/No, Comment) | ||||
| 5. Medical Products (Building Block 5) |
|
|
|
|
| Obligation Met (Yes/No, Comment) | ||||
| 6. Health Information and Research (Building Blcok 6) |
|
|
|
|
| Obligation Met (Yes/No, Comment) | ||||
| Client Perspective (Right Held) | Benchmarks (Yes/No, Comment) | |||
|---|---|---|---|---|
| Obligations | Available | Accessible | Acceptable | Quality |
| Access to discrimination-free health facilities, goods, and services |
|
|
|
|
| Access to essential drugs |
|
|
|
|
| Equitable distribution of health facilities, goods, and services |
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlassoff, C.; Arogundade, K.; Patel, K.; Jacobson, J.; Gyapong, M.; Krentel, A. Improving the Response of Health Systems to Female Genital Schistosomiasis in Endemic Countries through a Gender-Sensitive Human Rights-Based Framework. Diseases 2022, 10, 125. https://doi.org/10.3390/diseases10040125
Vlassoff C, Arogundade K, Patel K, Jacobson J, Gyapong M, Krentel A. Improving the Response of Health Systems to Female Genital Schistosomiasis in Endemic Countries through a Gender-Sensitive Human Rights-Based Framework. Diseases. 2022; 10(4):125. https://doi.org/10.3390/diseases10040125
Chicago/Turabian StyleVlassoff, Carol, Kazeem Arogundade, Kruti Patel, Julie Jacobson, Margaret Gyapong, and Alison Krentel. 2022. "Improving the Response of Health Systems to Female Genital Schistosomiasis in Endemic Countries through a Gender-Sensitive Human Rights-Based Framework" Diseases 10, no. 4: 125. https://doi.org/10.3390/diseases10040125
APA StyleVlassoff, C., Arogundade, K., Patel, K., Jacobson, J., Gyapong, M., & Krentel, A. (2022). Improving the Response of Health Systems to Female Genital Schistosomiasis in Endemic Countries through a Gender-Sensitive Human Rights-Based Framework. Diseases, 10(4), 125. https://doi.org/10.3390/diseases10040125