
Forecasting the Endemic/Epidemic Transition in COVID-19 in Some Countries: Influence of the Vaccination




Abstract
:1. Introduction
1.1. Problem Statement
1.2. Significance of the Research
1.3. Prediction Approaches in the Literature
1.4. Methodology and Approach

1.5. Overview of Epidemic/Endemic Transition: Example of Influenza
1.6. Organization of the Article
2. Materials and Methods
2.1. Data Description
2.2. Stationarity Breakdown Criteria
2.2.1. Coefficient of Variation (CV)
2.2.2. Empirical Entropy
2.2.3. Spectral Subdominant/Dominant Ratio
2.2.4. Skewness
2.2.5. Kurtosis
2.2.6. Index of Dispersion
2.2.7. Normality Index
2.3. Principal Component Analysis
2.4. Construction of a Score
2.5. Choice of the Countries
3. Results
3.1. Indicators of Transition
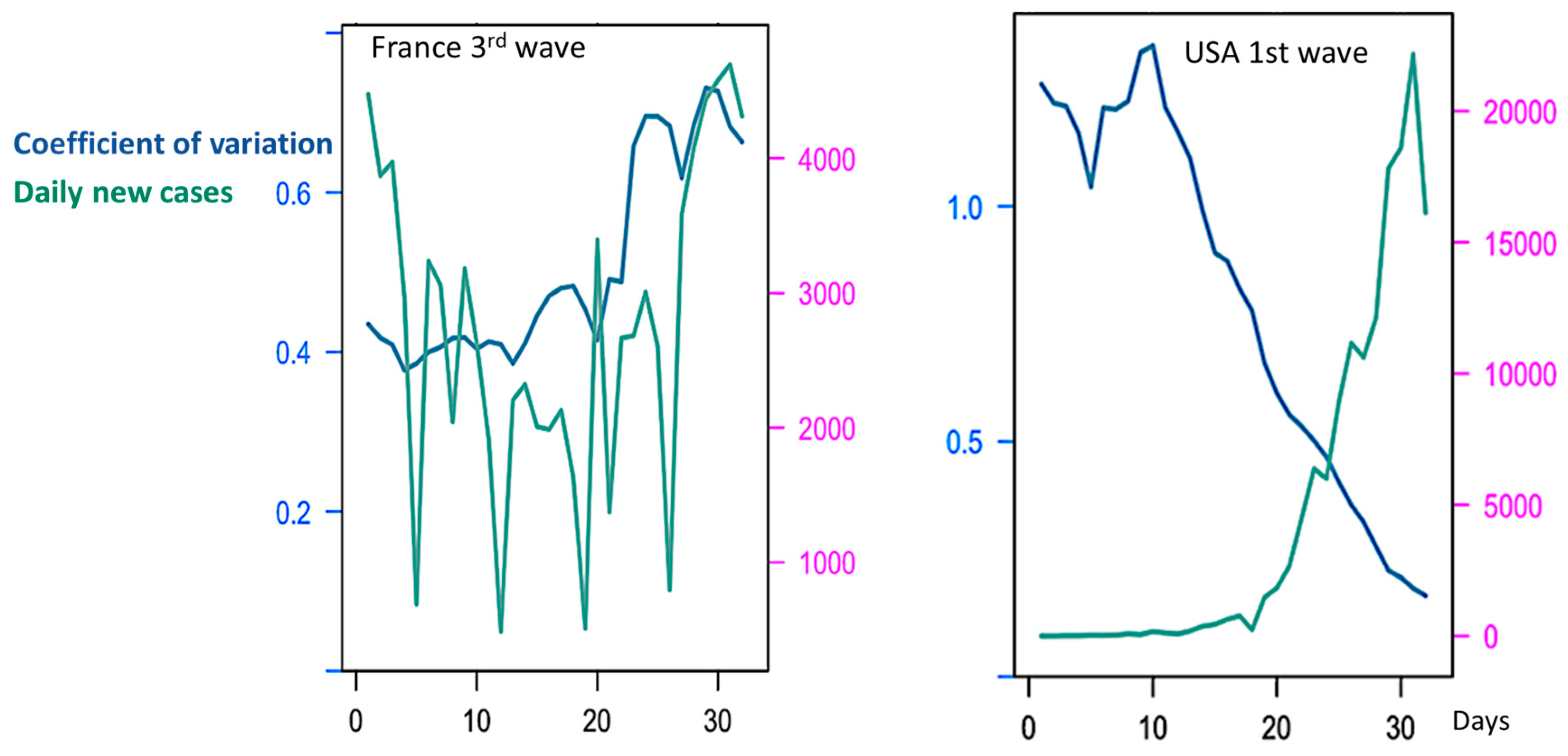
3.1.1. Coefficient of Variation (CV) during COVID-19 Outbreak
3.1.2. Empirical Entropy in COVID-19 Outbreak
3.1.3. Spectral Dominant/Subdominant Ratio in COVID-19 Outbreak
3.2. Forecasting in COVID-19 Outbreak with a Reliable Score
- Choice of the same length of moving window as for the CV calculation (14 days);
- Use of the same time step as for moving the window (1 day);
- Movement of the window from the start to the end of the COVID-19 outbreak observed between January 2020 and July 2022.
4. Discussion
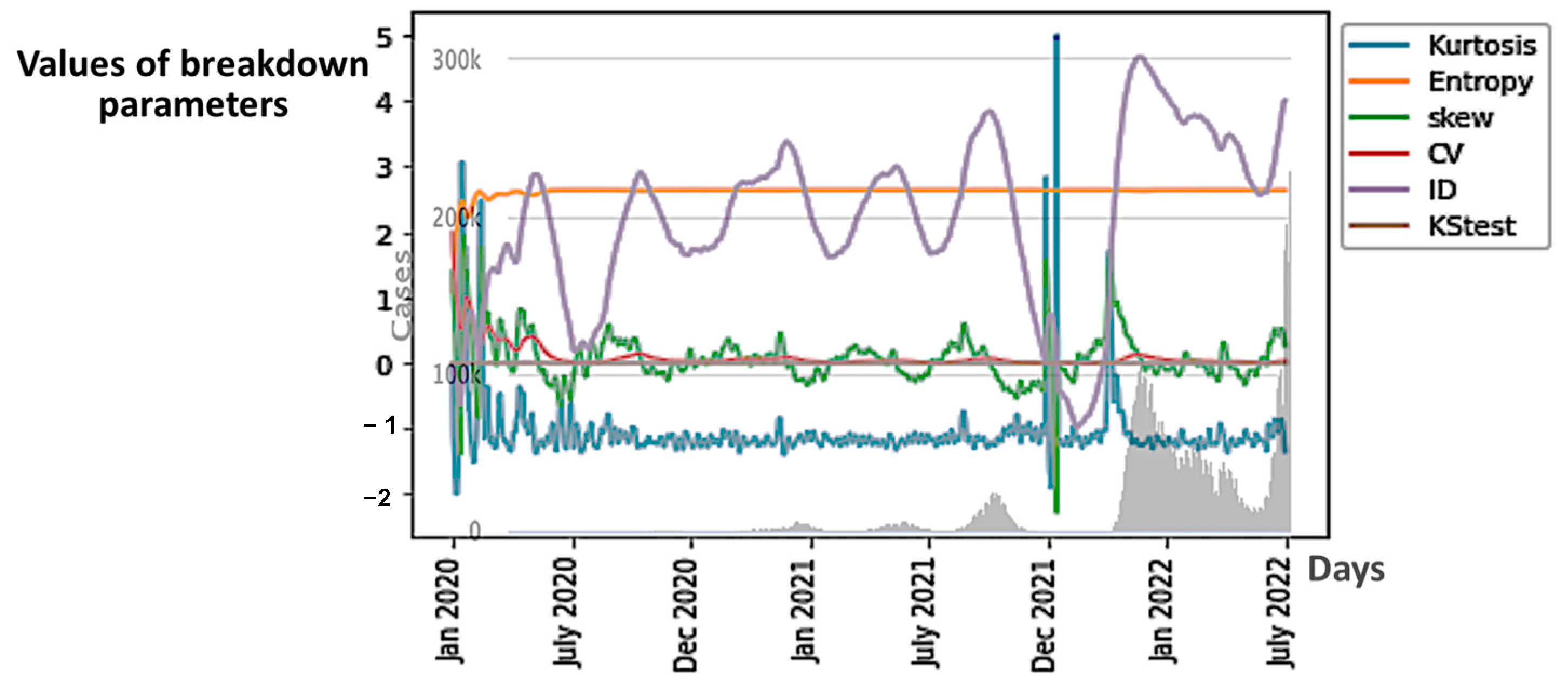
4.1. The ID Index as Predictor
4.2. The Influence of Vaccination on the Daily New Cases and Deaths Curves
- -
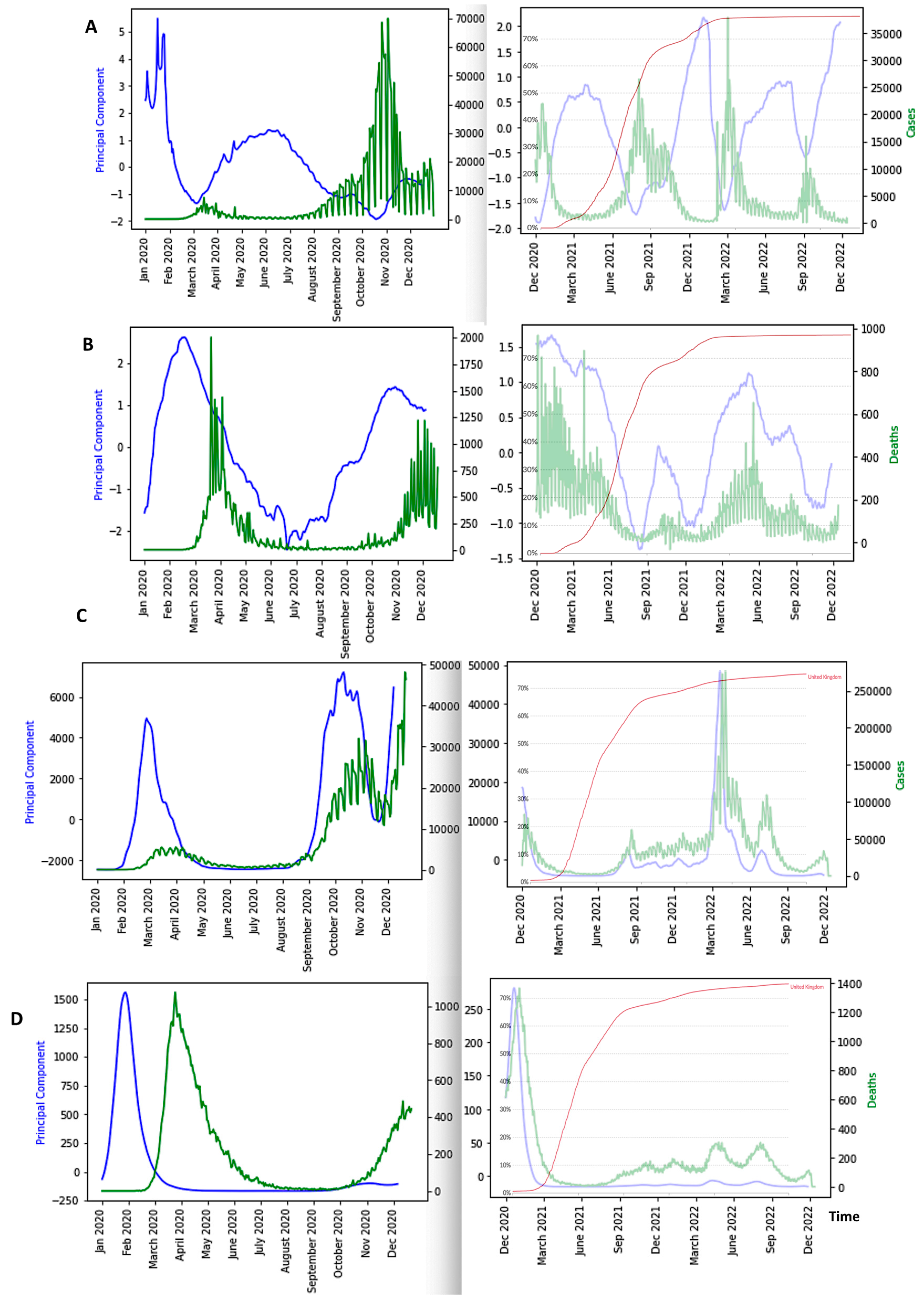
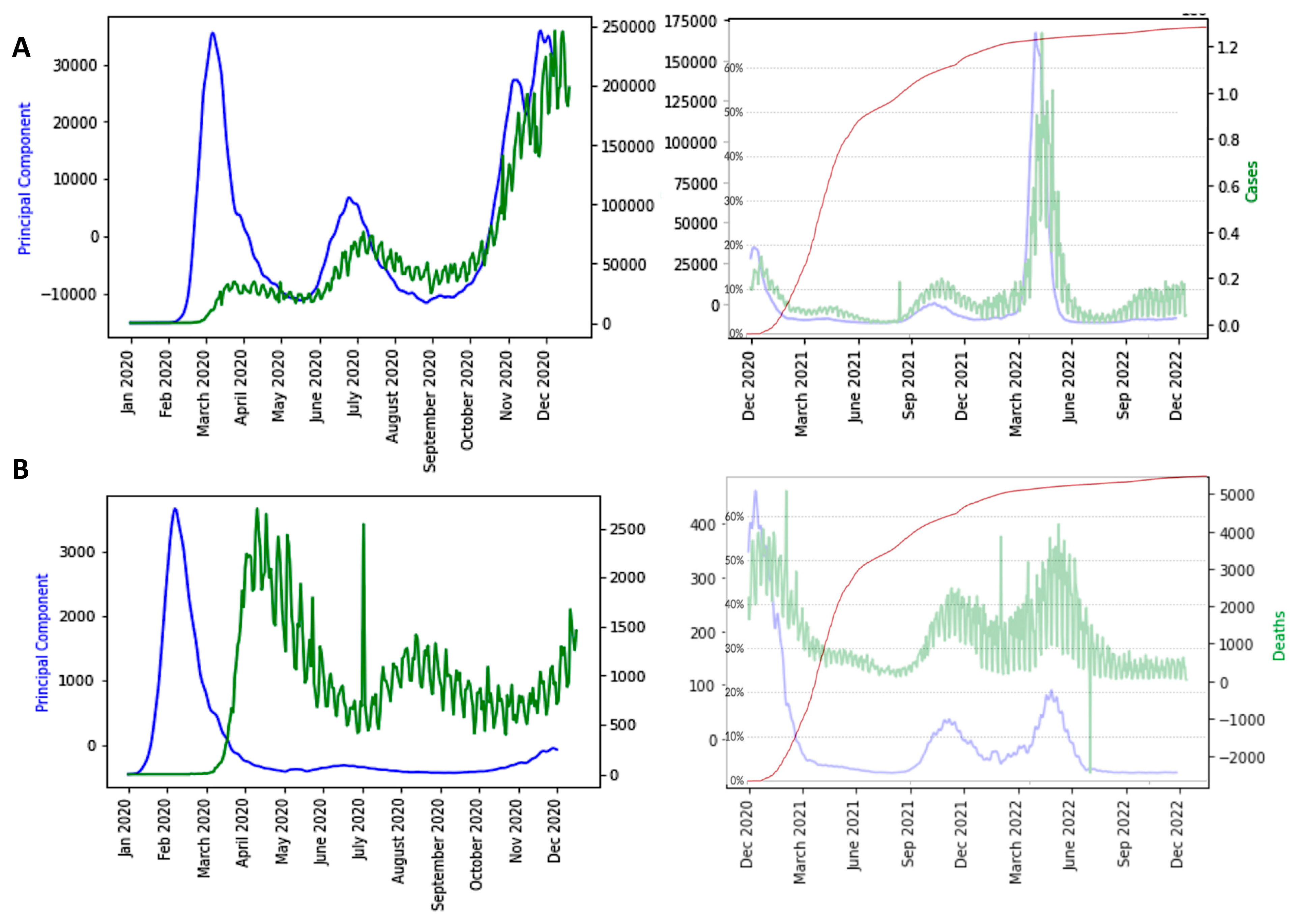
- The first PCA component (PCA1) anticipates systematically the new case and death waves, the latter ones occurring some weeks (between two and four) after the new case waves;
- -
- ID waves occur in opposition of phases with PCA1, but also predicts the new case and death waves well;
- -
- This anticipation remains true after vaccination, except for the end of the vaccination campaign which shows the beginning of a decorrelation between PCA1 and new case last waves.
- (i)
- to develop a parametric model that considers all the variables and parameters necessary for modeling the endemic/epidemic transition;
- (ii)
- to test the predictive power of the breakdown parameters used in the present article on other variables linked to the COVID-19 outbreak as the number of deaths, hospitalizations and ICU sojourns;
- (iii)
- to examine past outbreaks concerning other infectious diseases like Influenza H1N1 in 1977 or Ebola in Sierra Leone during the years of 2014 and 2015 and in Democratic Republic of Congo in 1995, and test for these infectious diseases the retro-predictive power of PCA1.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | T (°C) | E (m) | D (h/km2) | AM (years) | 1st wave R0 /Date start | 1st Wave Exponential Slope | 2nd Wave R0/Date Start | 2nd Wave Exponential Slope | GDP % Health 2020 |
|---|---|---|---|---|---|---|---|---|---|
| Africa | |||||||||
| Algeria | 22.5 | 800 | 18 | 28.1 | 2.19/20–03 | 0.1594 | 0.86/07–04 | 0.0316 | 6.32 |
| Cameroon | 31 | 667 | 56 | 17.7 | 2.56/03–04 | 0.0338 | 1.64/07–07 | 0.0085 | 3.77 |
| Djibouti | 28.0 | 430 | 47 | 23.9 | 2.31/07–04 | 0.489 | 2.47/07–05 | 0.5 | 2.01 |
| Guinea | 25.7 | 472 | 50 | 18.9 | 1.5/04–04 | 0.0744 | 1.36/28–06 | 0.01 | 4.04 |
| Mauritius | 22.4 | 209 | 620 | 35.3 | 5.4/25–03 | 0.02 | 9.32/02–06 | 0.03 | 5.83 |
| Morocco | 17.1 | 909 | 80 | 29.3 | 2.05/21–03 | 0.1161 | 0.84/21–05 | 0.0687 | 5.31 |
| Nigeria | 26.8 | 30 | 229 | 18.4 | 1.96/29–03 | 0.0672 | 1.25/02–05 | 0.0258 | 3.38 |
| Senegal | 27.85 | 69 | 82 | 18.8 | 2.02/12–04 | 0.1003 | 1.24/17–05 | 0.0238 | 3.98 |
| South Africa | 22.5 | 1034 | 49.1 | 27.6 | 2.48/07–03 | 0.257 | 1.15/06–05 | 0.0303 | 6.25 |
| Sudan | 26.9 | 568 | 22 | 19.9 | 1.97/20–04 | 0.0193 | 1.19/09–06 | 0.0407 | 4.51 |
| Tunisia | 19.2 | 246 | 186 | 31.6 | 1.34/15–03 | 0.01 | 2.64/24–06 | 0.142 | 7.29 |
| Asia | |||||||||
| Bangladesh | 25.0 | 85 | 1175 | 26.7 | 3.67/05–04 | 0.0399 | 0.92/01–08 | 0.01 | 2.34 |
| India | 27.4 | 160 | 470 | 32.4 | 2.43/22–04 | 0.0331 | 0.91/15–11 | 0.01 | 3.54 |
| Iran | 24 | 1305 | 51 | 30.3 | 3.61/04–03 | 0.2641 | 1/01–05 | 0.0438 | 8.66 |
| Iraq | 14.03 | 312 | 90 | 20.0 | 1.81/14–03 | 0.1184 | 0.96/18–07 | 0.0410 | 5.1 |
| Israel | 19.2 | 508 | 417 | 29.9 | 2.86/05–03 | 0.005 | 1.33/19–05 | 0.0339 | 7.52 |
| Japan | 11.15 | 438 | 333 | 47.3 | 1.91/25–02 | 0.0872 | 1.21/21–06 | 0.0260 | 10.95 |
| Pakistan | 20.20 | 900 | 274 | 23.8 | 1.90/15–03 | 0.1301 | 1.02/01–09 | 0.0113 | 3.20 |
| Turkey | 11.1 | 1132 | 106 | 30.9 | 4.32/11–03 | 0.0120 | 0.81/02–06 | 0.0473 | 4.12 |
| Europa | |||||||||
| Albania | 11.4 | 708 | 100 | 32.9 | 1.61/23–03 | 0.0309 | 0.99/18–05 | 0.0825 | 5.26 |
| Austria | 6.35 | 910 | 106 | 44.0 | 2.93/08–03 | 0.2825 | 1.05/07–06 | 0.0545 | 10.33 |
| Belgium | 9.55 | 181 | 378 | 41.4 | 8.28/06–03 | 0.1963 | 0.88/16–06 | 0.0257 | 10.32 |
| Bosnia/Her. | 9.85 | 500 | 69 | 42.1 | 1.70/21–03 | 0.1671 | 0.97/05–06 | 0.0667 | 8.90 |
| Bulgaria | 10.55 | 472 | 64 | 42.7 | 1.97/19–03 | 0.0927 | 0.78/13–04 | 0.0049 | 7.35 |
| Croatia | 10.9 | 331 | 187 | 43 | 3.95/18–03 | 0.093 | 0.72/12–06 | 0.01 | 6.83 |
| Denmark | 7.5 | 34 | 349 | 42.2 | 1.60/05–03 | 0.01 | 0.90/07–07 | 0.0539 | 10.07 |
| France | 10.7 | 375 | 123 | 41.4 | 2.68/29–02 | 0.2898 | 1/24–06 | 0.01 | 11.26 |
| Finland | 1.7 | 134 | 16 | 42.5 | 1.66/12–03 | 0.0711 | 1.04/26–07 | 0.0891 | 9.02 |
| Greece | 15.4 | 498 | 210 | 44.5 | 1.72/11–03 | 0.0759 | 1.05/24–06 | 0.01 | 7.72 |
| Georgia | 5.8 | 1432 | 54 | 38.1 | 2.19/30–03 | 0.0346 | 0.76/02–06 | 0.1471 | 7.11 |
| Germany | 8.5 | 263 | 233 | 47.1 | 2.84/29–02 | 0.2624 | 0.98/10–06 | 0.005 | 11.43 |
| Hungary | 9.75 | 143 | 272 | 42.3 | 2.25/21–03 | 0.0586 | 0.77/01–07 | 0.01 | 6.7 |
| Luxemburg | 8.65 | 325 | 237 | 39.3 | 1.99/16–03 | 0.4841 | 0.83/01–06 | 0.0271 | 5.29 |
| Malta | 19.2 | 1 | 1567 | 41.8 | 4.46/23–03 | 0.0712 | 1.29/19–04 | 0.0536 | 8.96 |
| Moldova | 9.45 | 139 | 79 | 36.7 | 2.03/22–03 | 0.1716 | 0.83/31–04 | 0.0217 | 6.6 |
| N Macedonia | 9.8 | 741 | 81 | 37.9 | 1.84/21–03 | 0.0858 | 0.87/03–05 | 0.028 | 6.58 |
| Netherlands | 9.25 | 30 | 421 | 42.6 | 2.4/05–03 | 0.2485 | 0.92/07–07 | 0.0002 | 9.97 |
| Norway | 1.5 | 460 | 17 | 39.2 | 2.4/09–03 | 0.2716 | 1.14/19–07 | 0.1725 | 10.05 |
| Poland | 7.85 | 173 | 123 | 40.7 | 2.17/14–03 | 0.1562 | 0.99/05–04 | 0.0094 | 6.33 |
| Romania | 8.8 | 414 | 81 | 41.1 | 2.26/14–03 | 0.1596 | 0.91/31–05 | 0.0498 | 5.56 |
| Serbia | 10.55 | 473 | 89 | 42.6 | 2.13/19–03 | 0.1919 | 0.79/01–06 | 0.0123 | 8.54 |
| Slovenia | 8.9 | 492 | 266 | 44.5 | 1.78/17–03 | 0.1301 | 1.08/12–06 | 0.01 | 8.3 |
| Spain | 13.3 | 660 | 93 | 42.7 | 3.85/25–02 | 0.335 | 1.16/29–06 | 0.0846 | 8.98 |
| Sweden | 2.1 | 320 | 23 | 41.2 | 2.10/05–03 | 0.2572 | 1.05/24–05 | 0.0768 | 10.9 |
| Switzerland | 5.5 | 1350 | 208 | 42.4 | 2.86/04–03 | 0.2388 | 0.95/08–06 | 0.0664 | 11.88 |
| UK | 8.45 | 162 | 280 | 40.5 | 2.89/04–03 | 0.2223 | 1.25/02–07 | 0.0416 | 10 |
| Ukraine | 8.3 | 175 | 70 | 40.6 | 2.16/24–03 | 0.1615 | 0.89/25–05 | 0.048 | 7.72 |
| North America | |||||||||
| Canada | −5.35 | 487 | 4 | 42.2 | 2.95/10–03 | 0.2432 | 1.05/01–07 | 0.0153 | 10.79 |
| Cuba | 25.2 | 108 | 102 | 41.5 | 2.23/27–03 | 0.0706 | 1.30/17–05 | 0.0517 | 11.19 |
| Dominican Republic | 24.55 | 424 | 34 | 38.1 | 2.09/20–03 | 0.1403 | 1.10/01–06 | 0.0151 | 5.73 |
| USA | 8.55 | 760 | 34 | 38.1 | 3.85/02–03 | 0.2882 | 0.99/07–06 | 0.0119 | 16.89 |
References
- Bernoulli, D.; Chapelle, D. Essai D’une Nouvelle Analyse de la Mortalité Causée par la Petite Vérole, et des Avantages de L’inoculation pour la Prévenir; Mémoire Académie Royale des Sciences: Paris, France, 2023. [Google Scholar]
- Xu, Z.; Yang, D.; Zhang, H.; Demongeot, J. A Novel Mathematical Model that Predicts the Protection Time of SARS-CoV-2 Antibodies. Viruses 2023, 15, 586. [Google Scholar] [CrossRef] [PubMed]
- Picard, D. Application aux tests de rupture de régression. Astérisque 1979, 68, 73–98. [Google Scholar]
- Deshayes, J.; Picard, D. Lois asymptotiques des tests et estimateurs de rupture dans un modèle statistique classique. Ann. De L’i.H.P. Probab. Et Stat. 1984, 20, 309–327. [Google Scholar]
- Vogt, M.; Dette, H. Detecting gradual changes in locally stationary processes. Ann. Stat. 2015, 43, 713–740. [Google Scholar] [CrossRef]
- van Delft, A.; Eichler, M. Locally stationary functional time series. Electron. J. Stat. 2018, 12, 107–170. [Google Scholar] [CrossRef]
- Palachy, S. Detecting stationarity in time series data. Medium Towards Data Sci. 2019, 9, 53. [Google Scholar]
- Ting, K.M.; Liu, Z.; Zhang, H.; Zhu, Y. A new distributional treatment for time series and an anomaly detection investigation. Proc. VLDB Endow. 2022, 15, 2321–2333. [Google Scholar] [CrossRef]
- Hauber, A.L.; Sigloch, C.; Timmer, J. Detecting frequency modulation in stochastic time-series data. Phys. Rev. 2022, 106, 024204. [Google Scholar] [CrossRef]
- Bawdekar, A.A.; Prusty, B.R.; Bingi, K. Sensitivity Analysis of Stationarity Tests’ Outcome to Time Series Facets and Test Parameters. Math. Probl. Eng. 2022, 2022, 2402989. [Google Scholar] [CrossRef]
- Demongeot, J.; Laksaci, A.; Madani, F.; Rachdi, M. Functional data: Local linear estimation of the conditional density and its application. Statistics 2013, 47, 26–44. [Google Scholar] [CrossRef]
- Rachdi, M.; Laksaci, A.; Demongeot, J.; Abdali, A.; Madani, F. Theoretical and practical aspects on the quadratic error in the local linear estimation of the conditional density for functional data. Comp. Stat. Data Anal. 2014, 73, 53–68. [Google Scholar] [CrossRef]
- Demongeot, J.; Laksaci, A.; Rachdi, M.; Rahmani, S. On the local linear modelization of the conditional distribution for functional data. Sankhya A 2014, 76, 328–355. [Google Scholar] [CrossRef]
- Demongeot, J.; Hamie, A.; Laksaci, A.; Rachdi, M. Relative-Error Prediction in Nonparametric Functional Statistics: Theory and Practice. J. Multivar. Anal. 2016, 146, 261–268. [Google Scholar] [CrossRef]
- Belkis, A.; Demongeot, J.; Laksaci, A.; Rachdi, M. Functional data analysis: Estimation of the relative error in functional regression under random left-truncation. J. Nonparametric Stat. 2018, 30, 472–490. [Google Scholar]
- Oshinubi, K.; Ibrahim, F.; Rachdi, M.; Demongeot, J. Functional Data Analysis: Application to Daily Observation of COVID-19 Prevalence in France. AIMS Math. 2022, 7, 5347–5385. [Google Scholar] [CrossRef]
- Jelassi, M.; Oshinubi, K.; Rachdi, M.; Demongeot, J. Epidemic Dynamics on Social Interaction Networks. AIMS Bioeng. 2022, 9, 348–361. [Google Scholar] [CrossRef]
- Agrawal, K.; Broad, A. Can we predict the future? Modelling SARS-CoV-2 epidemic to endemic transition. J. Stud. Res. 2022, 11, 2898. [Google Scholar] [CrossRef]
- Biancolella, M.; Colona, V.L.; Mehrian-Shai, R.; Watt, J.L.; Luzzatto, L.; Novelli, G.; Reichardt, J.K.V. COVID-19 2022 update: Transition of the pandemic to the endemic phase. Hum. Genom. 2022, 16, 19. [Google Scholar] [CrossRef]
- Cohen, L.E.; Spiro, D.J.; Viboud, C. Projecting the SARS-CoV-2 transition from pandemicity to endemicity: Epidemiological and immunological considerations. PLoS Pathog. 2022, 18, e1010591. [Google Scholar] [CrossRef]
- Roda, W.C.; Varughese, M.B.; Han, D.; Li, M.Y. Why is it difficult to accurately predict the COVID-19 epidemic? Infect. Dis. Model. 2020, 5, 271–281. [Google Scholar] [CrossRef]
- Smirnova, A.; deCamp, L.; Chowell, G. Forecasting epidemics through nonparametric estimation of time-dependent transmission rates using the SEIR model. Bull. Math. Biol. 2019, 81, 4343–4365. [Google Scholar] [CrossRef] [PubMed]
- Bakhta, A.; Boiveau, T.; Maday, Y.; Mula, O. Epidemiological forecasting with model reduction of compartmental models. application to the COVID-19 pandemic. Biology 2021, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Magal, P.; Webb, G. Predicting the number of reported and unreported cases for the COVID-19 epidemics in China, South Korea, Italy, France, Germany and United Kingdom. J. Theor. Biol. 2021, 509, 110501. [Google Scholar] [CrossRef] [PubMed]
- Morel, J.D.; Morel, J.M.; Alvarez, L. Learning from the past: A short-term forecast method for the COVID-19 incidence curve. PLoS Comput. Biol. 2023, 19, e1010790. [Google Scholar] [CrossRef]
- Roosa, K.; Lee, Y.; Luo, R.; Kirpich, A.; Rothenberg, R.; Hyman, J.M.; Yan, P.; Chowell, G. Real-time forecasts of the COVID-19 epidemic in China from February 5th to February 24th, 2020. Infect. Dis. Model. 2020, 5, 256–263. [Google Scholar] [CrossRef]
- Miller, J.K.; Elenberg, K.; Dubrawski, A. Forecasting emergence of COVID-19 variants of concern. PLoS ONE 2022, 17, e0264198. [Google Scholar] [CrossRef]
- Hussein, T.; Hammad, M.H.; Surakhi, O.; AlKhanafseh, M.; Fung, P.L.; Zaidan, M.A.; Wraith, D.; Ershaidat, N. Short-Term and long-term COVID-19 pandemic forecasting revisited with the emergence of Omicron variant in Jordan. Vaccines 2022, 10, 569. [Google Scholar] [CrossRef]
- Hatami, F.; Chen, S.; Paul, R.; Thill, J.C. Simulating and forecasting the COVID-19 spread in a US Metropolitan region with a spatial SEIR model. Int. J. Env. Res. Public Health 2022, 19, 15771. [Google Scholar] [CrossRef]
- Rashed, E.A.; Kodera, S.; Hirata, A. COVID-19 forecasting using new viral variants and vaccination effectiveness models. Comput. Biol. Med. 2022, 149, 105986. [Google Scholar] [CrossRef]
- Du, H.; Dong, E.; Badr, H.S.; Petrone, M.E.; Grubaugh, N.D.; Gardner, L.M. Incorporating variant frequencies data into short-term forecasting for COVID-19 cases and deaths in the USA: A deep learning approach. Ebiomedicine 2023, 89, 104482. [Google Scholar] [CrossRef]
- Ioannidis, J.P.; Cripps, S.; Tanner, M.A. Forecasting for COVID-19 has failed. Int. J. Forecast. 2022, 38, 423–438. [Google Scholar] [CrossRef] [PubMed]
- James, P.T.; Leach, R.; Kalamara, E.; Shayeghi, M. The worldwide obesity epidemic. Obes. Res. 2001, 9, 228S–233S. [Google Scholar] [CrossRef] [PubMed]
- WHO. Available online: https://www.who.int/ (accessed on 6 July 2023).
- Worldometer. Available online: https://www.worldometers.info/coronavirus/country/china/ (accessed on 6 July 2023).
- Our World in Data. Available online: Ourworldindata.org/explorers/coronavirus-data-explorer (accessed on 8 August 2023).
- Johnson, N.P.; Mueller, J. Updating the accounts: Global mortality of the 1918–1920 "Spanish" influenza pandemic. Bull. Hist. Med. 2002, 76, 105–115. [Google Scholar] [CrossRef]
- Yang, W.; Petkova, E.; Shaman, J. The 1918 influenza pandemic in New York City: Age-specific timing, mortality, and transmission dynamics. Influenza Other Respir. Viruses 2014, 8, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Knobler, S.L.; Mack, A.; Mahmoud, A.; Lemon, S.M. The Threat of Pandemic Influenza: Are We Ready? National Academies Press: Washington, DC, USA, 2005. [Google Scholar]
- Paget, J.; Spreeuwenberg, P.; Charu, V.; Taylor, R.J.; Iuliano, A.D.; Bresee, J.; Simonsen, L.; Viboud, C.; Global Seasonal Influenza-associated Mortality Collaborator Network and GLaMOR Collaborating Teams. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J. Glob. Health 2019, 9, 020421. [Google Scholar] [CrossRef] [PubMed]
- Yewdell, J.W. Antigenic drift: Understanding COVID-19. Immunity 2021, 54, 2681–2687. [Google Scholar] [CrossRef]
- Demongeot, J.; Magal, P. Spectral method in epidemic time series. Biology 2022, 11, 1825. [Google Scholar] [CrossRef]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Oshinubi, K. Mathematical and Statistical Modeling of Epidemic Data: Application to the Novel COVID-19 Outbreak. Modeling and Simulation. Ph.D Thesis, Université Grenoble Alpes, Grenoble, France, 2022. [Google Scholar]
- Gaudart, J.; Landier, J.; Huiart, L.; Legendre, E.; Lehot, L.; Bendiane, M.K.; Chiche, L.; Petitjean, A.; Mosnier, E.; Kirakoya-Samadoulougou, F.; et al. Factors associated with spatial heterogeneity of Covid-19 in France: A nationwide ecological study. Lancet Public Health 2021, 6, e222–e231. [Google Scholar] [CrossRef]
- Waku, J.; Oshinubi, K.; Demongeot, J. Maximal reproduction number estimation and identification of transmission rate from the first inflection point of new infectious cases waves: COVID-19 outbreak example. Maths Comp. Simul. 2022, 198, 47–64. [Google Scholar] [CrossRef]
- Demongeot, J.; Griette, Q.; Maday, Y.; Magal, P. A Kermack-McKendrick model with age of infection starting from a single or multiple cohorts of infected patients. Proc. R. Soc. A 2023, 479, 20220381. [Google Scholar] [CrossRef]
- Demongeot, J.; Fougère, C. mRNA vaccines—Facts and hypotheses on fragmentation and encapsulation. Vaccines 2022, 11, 40. [Google Scholar] [CrossRef] [PubMed]












| United states CV values start of the pandemic 27/02/2020 - 1.259872 12/03/2020 - 0.9012443 26/03/2020 - 0.2257 fourth wave 01/06/2021 - 0.373792 15/06/2021 - 0.4426645 01/07/2021 - 0.5956981 India CV values start of the pandemic 02/03/2020 - 0.9011401 16/03/2020 - 0.6828228 01/04/2020 - 0.4409121 Second wave 23/01/2021 - 0.1967528 06/02/2021 - 0.1313073 20/02/2021 - 0.1390496 Third wave 01/11/2021 - 0.0856899 15/11/2021 - 0.1311902 01/12/2021 - 0.4360979 Fourth wave 01/05/2022 - 0.1407748 15/05/2022 - 0.1719229 02/06/2022 - 0.3735433 | United states CV values start of the pandemic 28/02/2020 - 1.219726 13/03/2020 - 0.8833425 27/03/2020 - 0.2107585 fourth wave 02/06/2021 - 0.3787229 16/06/2021 - 0.462615 02/07/2021 - 0.5756484 India CV values start of the pandemic 03/03/2020 - 0.8479051 17/03/2020 - 0.7268929 02/04/2020 - 0.4300673 Second wave 24/01/2021 - 0.1920922 07/02/2021 - 0.1423886 21/02/2021 - 0.1463374 Third wave 02/11/2021 - 0.1042972 16/11/2021 - 0.1506754 02/12/2021 - 0.4391623 Fourth wave 02/05/2022 - 0.1613438 16/05/2022 - 0.1773734 03/06/2022 - 0.3925422 |  |
| France | |||
|---|---|---|---|
| Period 1: Epidemic phase 27 February–17 May 2020 | 1.028886 | 1.015612 | 0.987106 |
| Period 2: Endemic phase 17 May–17 July 2020 | 1.002432 | 1.002580 | 1.00015 |
| Period 3: Epidemic phase 15 September–26 November 2020 | 1.003880 | 0.981878 | 0.978083 |
| Period 4: Endemic phase 26 November–20 December 2020 | 1.019847 | 1.021709 | 1.00183 |
| Period 5: Epidemic phase 20 December–25 February 2021 | 1.005828 | 0.991934 | 0.986186 |
| Japan | |||
| Period 1: Epidemic phase 20 February–27 May 2020 | 1.028575 | 1.022287 | 0.993887 |
| Period 2: Endemic phase 27 May–13 June 2020 | 1.002512 | 0.773729 | 0.771790 |
| Period 3: Epidemic phase 13 June–10 September 2020 | 1.020337 | 1.014091 | 0.993879 |
| Period 4: Endemic phase 10 September–18 October 2020 | 1.005970 | 0.989558 | 0.983686 |
| Period 5: Epidemic phase 18 October–5 December 2020 | 1.039391 | 1.040991 | 1.001539 |
| i | Kurtosis | Entropy | Skew | CV | ID | KStest | ∆ID |
|---|---|---|---|---|---|---|---|
| 0 | −0.06 | 1.1 | 1.39 | 1.99 | −0.07 | 0.00092 | 0.57 |
| 1 | −1.1 | 1.39 | 0.95 | 1.64 | −0.11 | 0.00092 | 0.40 |
| 2 | −1.64 | 1.61 | 0.60 | 1.39 | −0.16 | 0.00092 | 0.32 |
| 3 | −1.92 | 1.79 | 0.29 | 1.20 | −0.21 | 0.00092 | 0.28 |
| 4 | −2.0 | 1.95 | 0 | 1.04 | −0.27 | 0.00092 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waku, J.; Oshinubi, K.; Adam, U.M.; Demongeot, J. Forecasting the Endemic/Epidemic Transition in COVID-19 in Some Countries: Influence of the Vaccination. Diseases 2023, 11, 135. https://doi.org/10.3390/diseases11040135
Waku J, Oshinubi K, Adam UM, Demongeot J. Forecasting the Endemic/Epidemic Transition in COVID-19 in Some Countries: Influence of the Vaccination. Diseases. 2023; 11(4):135. https://doi.org/10.3390/diseases11040135
Chicago/Turabian StyleWaku, Jules, Kayode Oshinubi, Umar Muhammad Adam, and Jacques Demongeot. 2023. "Forecasting the Endemic/Epidemic Transition in COVID-19 in Some Countries: Influence of the Vaccination" Diseases 11, no. 4: 135. https://doi.org/10.3390/diseases11040135
APA StyleWaku, J., Oshinubi, K., Adam, U. M., & Demongeot, J. (2023). Forecasting the Endemic/Epidemic Transition in COVID-19 in Some Countries: Influence of the Vaccination. Diseases, 11(4), 135. https://doi.org/10.3390/diseases11040135