Rosuvastatin Improves Vaspin Serum Levels in Obese Patients with Acute Coronary Syndrome


Abstract
:1. Introduction
2. Patient and Methods
3. Sample Collections and Anthropometric Profiles
4. Statistical Analysis
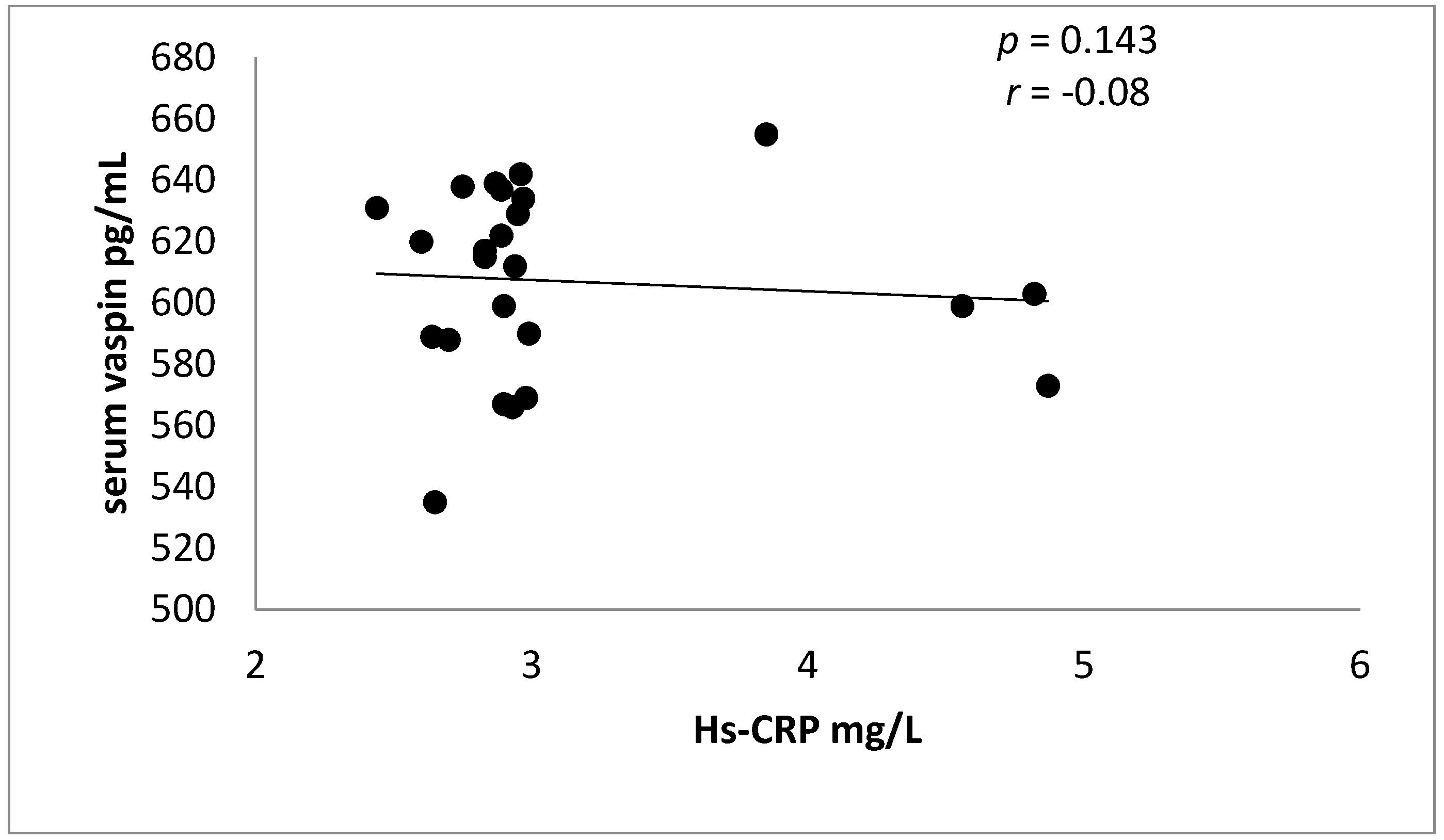
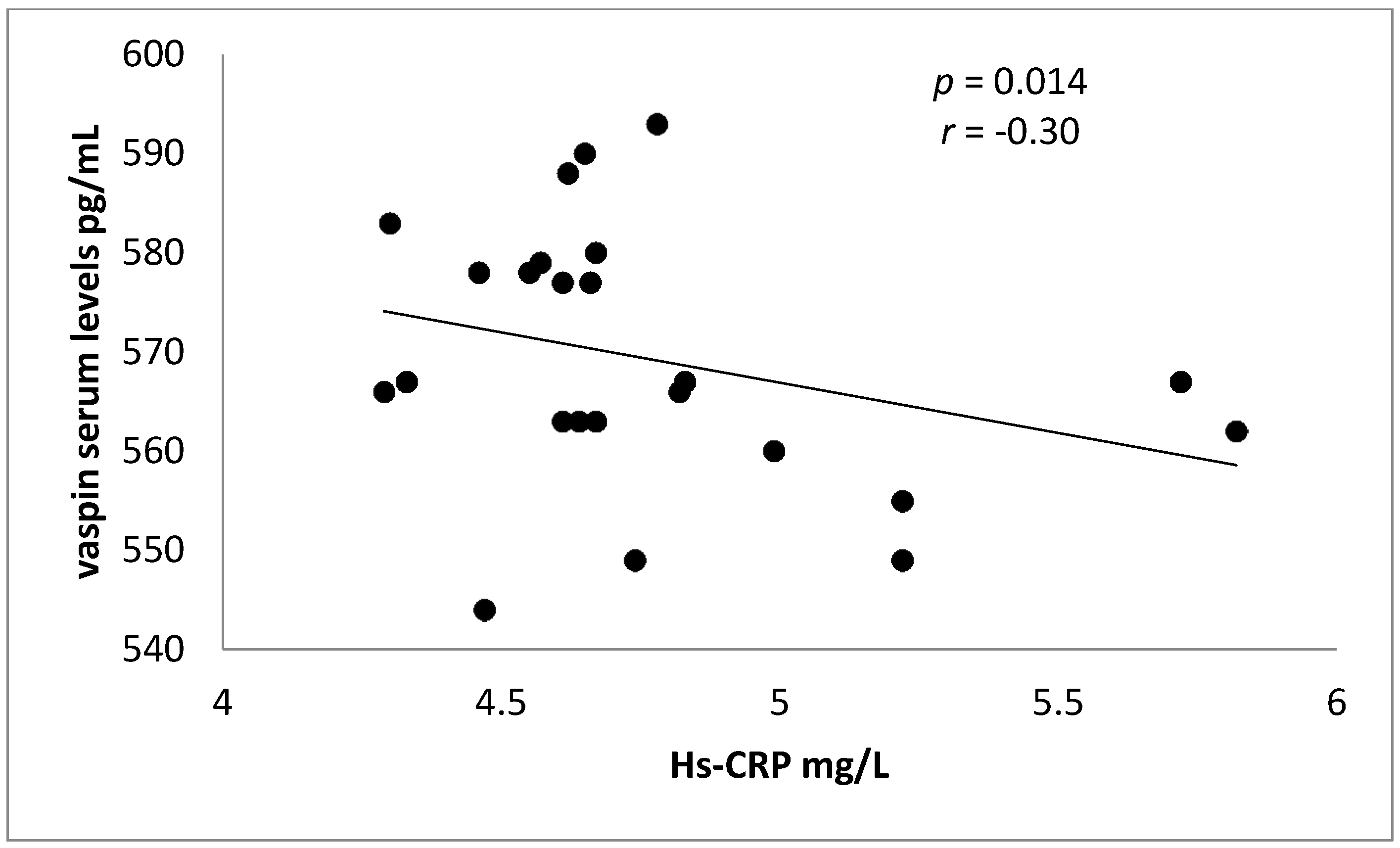
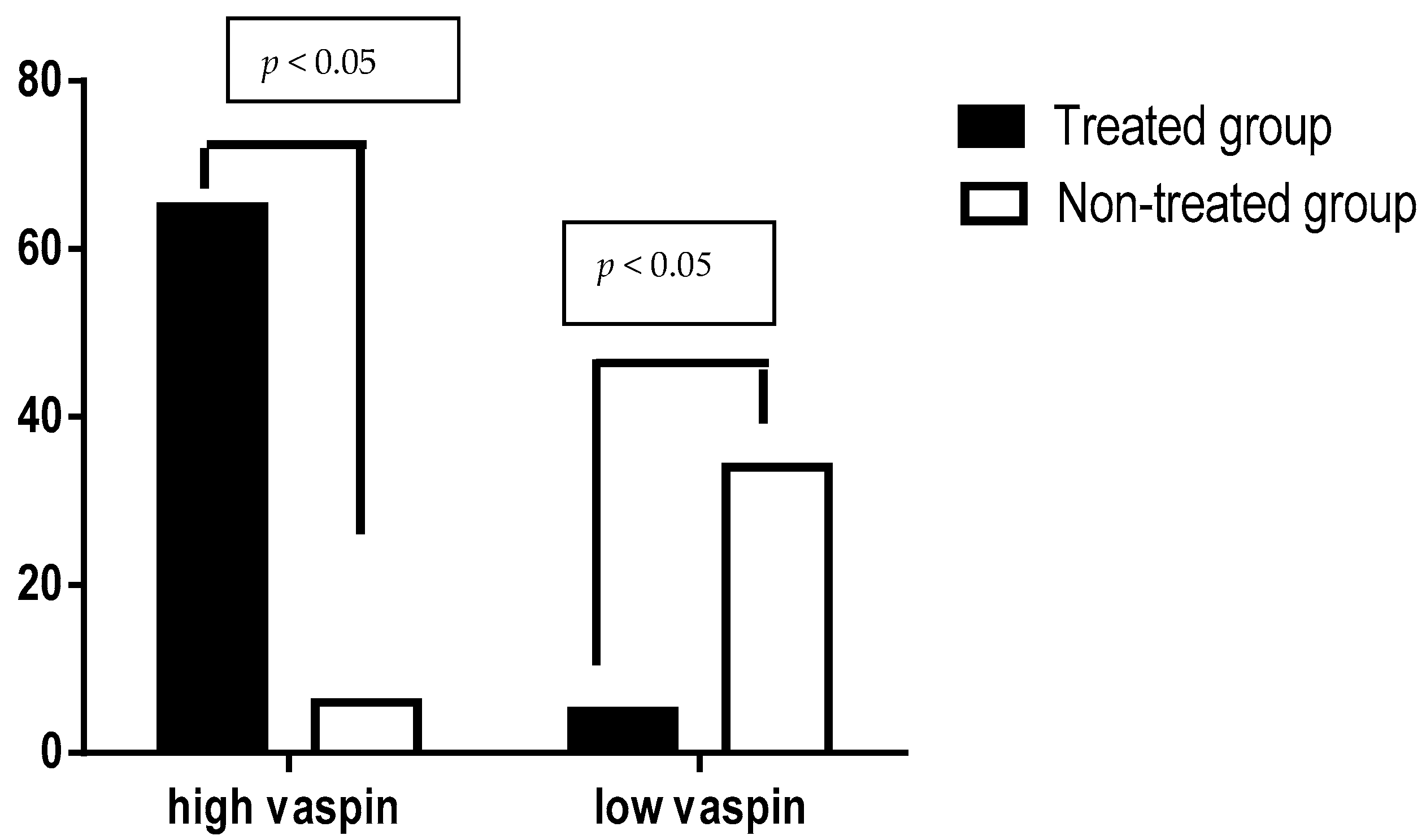
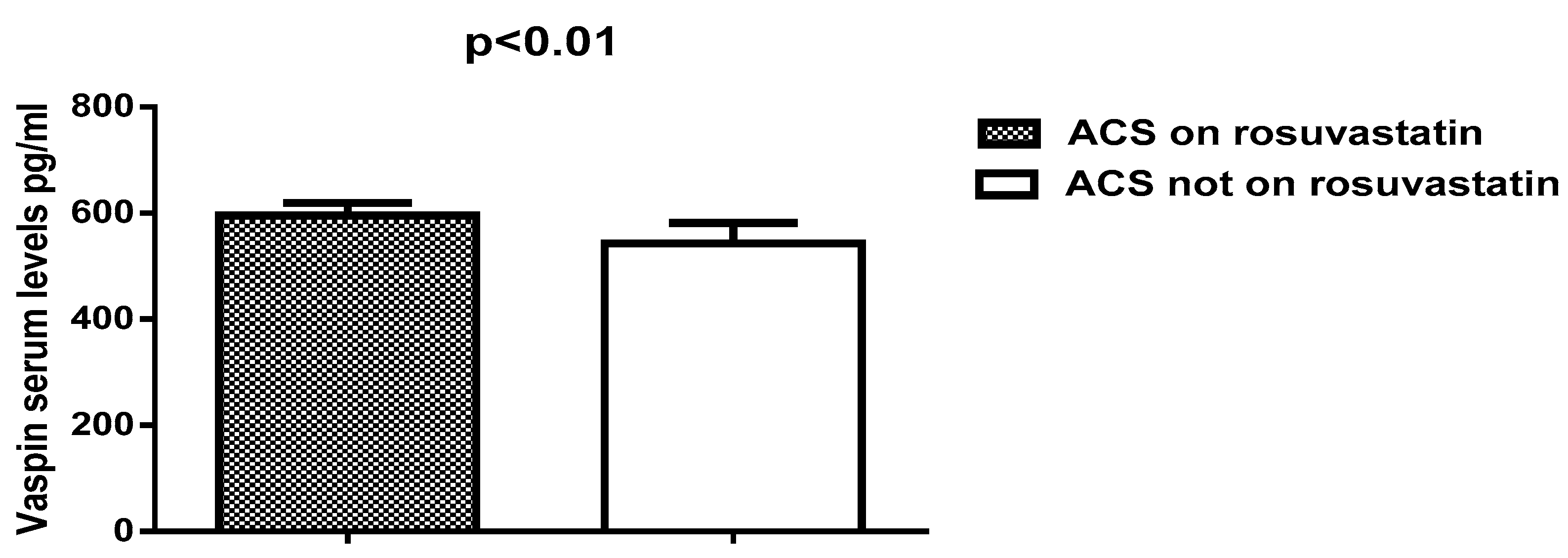
5. Results
6. Discussion
7. Conclusions
Author Contributions
Conflicts of Interest
References
- Tsaousi, G.; Pitsis, A.A.; Ioannidis, G.D.; Vasilakos, D.G. A multidisciplinary approach to unplanned conversion from off-pump to on-pump beating heart coronary artery revascularization in patients with compromised left ventricular function. Crit. Care Res. Pract. 2014, 2014, 348021. [Google Scholar] [CrossRef] [PubMed]
- Erne, P.; Radovanovic, D.; Seifert, B.; Bertel, O.; Urban, P.; AMIS Plus Investigators. The outcome of patients admitted with acute coronary syndrome on palliative treatment: Insights from the nationwide AMIS Plus Registry 1997–2014. BMJ Open 2015, 5, e006218. [Google Scholar] [CrossRef] [PubMed]
- Hicks, K.; Cocks, K.; Corbacho Martin, B.; Elton, P.; MacNab, A.; Colecliffe, W.; Furze, G. An intervention to reassure patients about test results in rapid access chest pain clinic: A pilot randomised controlled trial. BMC Cardiovasc. Disord. 2014, 14, 138. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Awad, M.S.; Alrifai, S.B. Assessment of serum prolactin levels in acute myocardial infarction: The role of pharmacotherapy. Indian J. Endocrinol. Metab. 2016, 20, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I. New Insights into the Role of Metformin Effects on Serum Omentin1 Levels in Acute MyocardialInfarction: Cross-Sectional Study. Emerg. Med. Int. 2015, 2015, 283021. [Google Scholar]
- Meyer-Saraei, R.; de Waha, S.; Eitel, I.; Desch, S.; Scheller, B.; Böhm, M.; Lauer, B.; Gawaz, M.; Geisler, T.; Gunkel, O.; et al. Thrombus aspiration in non-ST-elevation myocardial infarction—The 12-month clinical outcome of the randomised TATORT-NSTEMI trial. Eur. Heart J. Acute Cardiovasc. Care 2015, 18, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Ndrepepa, G.; Braun, S.; Tada, T.; Guerra, E.; Schunkert, H.; Laugwitz, K.L.; Kastrati, A. Comparative prognostic value of low-density lipoprotein cholesterol and C-reactive protein in patients with stable coronary artery disease treated with percutaneous coronary intervention and chronic statin therapy. Cardiovasc. Revasc. Med. 2014, 15, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Ndrepepa, G.; Braun, S.; Tada, T.; King, L.; Cassese, S.; Fusaro, M.; Keta, D.; Kastrati, A.; Schmidt, R. Comparative prognostic value of C-reactive protein & fibrinogen in patients with coronary artery disease. Indian J. Med. Res. 2014, 140, 392–400. [Google Scholar] [PubMed]
- Xia, J.; Qu, Y.; Yin, C.; Xu, D. Preoperative rosuvastatin protects patients with coronary artery disease undergoing noncardiac surgery. Cardiology 2015, 131, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Esaki, E.; Adachi, H.; Hirai, Y.; Yamagishi, S.; Kakuma, T.; Enomoto, M.; Fukami, A.; Kumagai, E.; Ohbu, K.; Obuchi, A.; et al. Serum vaspin levels are positively associated with carotid atherosclerosis in a general population. Atherosclerosis 2014, 233, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Shaker, O.G.; Sadik, N.A. Vaspin gene in rat adipose tissue: Relation to obesity-induced insulin resistance. Mol. Cell. Biochem. 2013, 373, 229–239. [Google Scholar] [CrossRef] [PubMed]
- DeClercq, V.; Enns, J.E.; Yeganeh, A.; Taylor, C.G.; Zahradka, P. Modulation of cardiovascular function by adipokines. Cardiovasc. Hematol. Disord. Drug Targets 2013, 13, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.J.; Matsuo, Y.; Aoki, T.; Kwon, T.G.; Prasad, A.; Gulati, R.; Lennon, R.J.; Lerman, L.O.; Lerman, A. Coronary endothelial dysfunction is associated with inflammation and vasa vasorum proliferation in patients with early atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2473–2477. [Google Scholar] [CrossRef] [PubMed]
- Moradi, S.; Mirzaei, K.; Abdurahman, A.A.; Keshavarz, S.A.; Hossein-Nezhad, A. Mediatory effect of circulating vaspin on resting metabolic rate in obese individuals. Eur. J. Nutr. 2015, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kêkê, L.M.; Samouda, H.; Jacobs, J.; Di Pompeo, C.; Lemdani, M.; Hubert, H.; Zitouni, D.; Guinhouya, B.C. Body mass index and childhood obesity classification systems: A comparison of the French, International Obesity Task Force (IOTF) and World Health Organization (WHO) references. Rev. Epidemiol. Sante Publique 2015, 63, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Abeles, A.M.; Pillinger, M.H. Statins as antiinflammatory and immunomodulatory agents: A future in rheumatologic therapy? Arthritis Rheumatol. 2006, 54, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I. Effects of Rosuvastatin Alone or in Combination withOmega3 FattyAcid on Adiponectin Levelsand Cardiometabolic Profile. J. Basic Clin. Pharm. 2016, 8, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Abudukeremu, N.; Pan, S.; Ma, Y.; Yang, Y.; Ma, X.; Li, X.; Fu, Z.; Huang, Y.; Xie, X.; Liu, F.; et al. The optimal cutoff point of the waist-to-hip ratio for screening Uyghur population aged 35 years and over at high-risk of cardiovascular diseases in Xinjiang. Zhonghua Xin Xue Guan Bing Za Zhi 2015, 43, 173–178. [Google Scholar] [PubMed]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I. Acylation-stimulating protein is a surrogate biomarker for acute myocardial infarction: Role of statins. J. Lab. Physicians 2017, 9, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Vaspin in obesity and diabetes: Pathophysiological and clinical significance. Endocrine 2012, 41, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Heiker, J.T.; Klöting, N.; Kovacs, P.; Kuettner, E.B.; Sträter, N.; Schultz, S.; Kern, M.; Stumvoll, M.; Blüher, M.; Beck-Sickinger, A.G.; et al. Vaspin inhibits kallikrein 7 by serpin mechanism. Cell. Mol. Life Sci. 2013, 70, 2569–2583. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, S.E.; Gee, L.L.; Wachtel, M.S.; Frezza, E.E. Adipose tissue: The new endocrine organ? A review article. Dig. Dis. Sci. 2009, 54, 1847–1856. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.K.; Han, T.K.; Kang, H.S. Combined effects of body mass index and cardio/respiratory fitness on serum vaspin concentrations in Korean young men. Eur. J. Appl. Physiol. 2010, 108, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Mahdirejei, H.A.; Abadei, S.F.R.; Seidi, A.A.; Gorji, N.E.; Kafshgari, H.R.; Pour, M.E.; Khalili, H.B.; Hajeizad, F.; Khayeri, M. Effects of an eight-week resistance training on plasma vaspin concentrations, metabolic parameters levels and physical fitness in patients with type 2 diabetes. Cell J. 2014, 16, 367–374. [Google Scholar]
- Kim, J.M.; Kim, T.N.; Won, J.C. Association between serum vaspin level and metabolic syndrome in healthy Korean subjects. Metab. Syndr. Relat. Disord. 2013, 11, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Kobat, M.A.; Celik, A.; Balin, M.; Altas, Y.; Baydas, A.; Bulut, M.; Aydin, S.; Dagli, N.; Yavuzkir, M.F.; Ilhan, S. The investigation of serum vaspin level in atherosclerotic coronary artery disease. J. Clin. Med. Res. 2012, 4, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.; Vrabas, I.S.; Kapelouzou, A.; Lampropoulos, S.; Sailer, N.; Kostakis, A.; Liapis, C.D. Impact of atorvastatin on serum vaspin levels in hypercholesterolemic patients with moderate cardiovascular risk. Regul. Pept. 2011, 170, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Satoh, M.; Takahashi, Y.; Tabuchi, T.; Minami, Y.; Tamada, M.; Takahashi, K.; Itoh, T.; Morino, Y.; Nakamura, M. Cellular and molecular mechanisms of statins: An update on pleiotropic effects. Clin. Sci. 2015, 129, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Vidyarthi, M.; Jacob, P.; Chowdhury, T.A. Oral use of “Low and Slow” Rosuvastatin with Co-Enzyme Q10 in patients with Statin-Induced Myalgia: Retrospective case review. Indian J. Endocrinol. Metab. 2012, 16 (Suppl. S2), S498–S500. [Google Scholar] [PubMed]
- Kavalipati, N.; Shah, J.; Ramakrishan, A.; Vasnawala, H. Pleiotropic effects of statins. Indian J. Endocrinol. Metab. 2015, 19, 554–562. [Google Scholar] [PubMed]
- Kadoglou, N.P.; Gkontopoulos, A.; Kapelouzou, A.; Fotiadis, G.; Theofilogiannakos, E.K.; Kottas, G.; Lampropoulos, S. Serum levels of vaspin and visfatin in patients with the coronary artery disease-Kozani study. Clin. Chim. Acta 2011, 412, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Phalitakul, S.; Okada, M.; Hara, Y.; Yamawaki, H. Vaspin prevents TNF-α-induced intracellular adhesion molecule-1 via inhibiting reactive oxygen species-dependent NF-κB and PKC activation in cultured rat vascular smooth muscle cells. Pharmacol. Res. 2011, 64, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Phalitakul, S.; Okada, M.; Hara, Y.; Yamawaki, H. A novel adipocytokine, vaspin inhibits platelet-derived growth factor-BB-induced migration of vascular smooth muscle cells. Biochem. Biophys. Res. Commun. 2012, 423, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Al-Azzam, S.I.; Alzoubi, K.H.; Abeeleh, J.A.; Mhaidat, N.M.; Abu-Abeeleh, M. Effect of statin therapy on vaspin levels in type 2 diabetic patients. Clin. Pharmacol. 2013, 5, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Teshigawara, S.; Wada, J.; Hida, K.; Nakatsuka, A.; Eguchi, J.; Murakami, K.; Kanzaki, M.; Inoue, K.; Terami, T.; Katayama, A.; et al. Serum vaspin concentrations are closely related to insulin resistance, with higher serum levels in Japanese population. J. Clin. Endocrinol. Metab. 2012, 97, E1202–E1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyashita, H.; Honda, T.; Maekawa, T.; Takahashi, N.; Aoki, Y.; Nakajima, T.; Tabeta, K.; Yamazaki, K. Relationship between serum antibody titers to Porphyromonas gingivalis and hs-CRP levels as inflammatory markers of periodontitis. Arch. Oral Biol. 2012, 57, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Motawi, T.M.K.; Mahdy, S.G.; El-Sawalhi, M.M.; Ali, E.N.; El-Telbany, R.F.A. Serum levels of chemerin, apelin, vaspin, and omentin-1 in obese type 2 diabetic Egyptian patients with coronary artery stenosis. Can. J. Physiol. Pharmacol. 2017, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sathyaseelan, A.J.; Adole, P.S.; Wyawahare, M.; Saya, R.P. Assessment of Serum VASPIN Levels among Type 2 Diabetes Mellitus Patients with or without Acute Coronary Syndrome. J. Clin. Diagn. Res. 2016, 10, BC07–BC10. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Rosuvastatin Group | Control Group | p Value |
|---|---|---|---|
| (n = 70) | (n = 40) | ||
| Age | 47.87 ± 12.72 | 49.85 ± 11.83 | 0.52 |
| Gender | |||
| M:F ratio | (71.42:28.57)% | (22:18) % | - |
| BMI | 31.44 ± 7.81 | 32.39 ± 6.77 | 0.59 |
| W-H ratio | |||
| Men | 1.32 ± 0.67 | 1.39 ± 0.77 | 0.71 |
| Women | 0.88 ± 0.31 | 0.91 ± 0.11 | 0.67 |
| Hypertension | 70 (100%) | 20 (100%) | <0.0001 ** |
| ACS | |||
| STEMI | 25 (35.71%) | 8 (40%) | 0.72 |
| NSTEMI | 25 (35.71%) | 10 (50%) | 0.24 |
| UA | 20 (28.57%) | 2 (10%) | 0.08 |
| Troponin positive | 67 (95.71%) | 18 (90%) | 0.32 |
| Troponin negative | 3 (4.28%) | 2 (10%) | 0.32 |
| Dyslipidemia | 64 (44.8%) | 18 (90%) | 0.84 |
| Duration of IHD (years) | 8.42 ± 2.28 | 7.44 ± 2.39 | 0.11 |
| Diabetes mellitus | 3 (4.28%) | 2 (10%) | 0.32 |
| Pharmacotherapy | |||
| Anticoagulant | 44 (62.58%) | 17 (85%) | 0.06 |
| Antiplatelet | 70 (100%) | 18 (90%) | 0.0072 |
| ACEIs | 44 (62.58%) | 18 (90%) | 0.02 * |
| Statins | 70 (100%) | - | <0.0001 ** |
| CCB | 22 (31.42%) | 12 (60%) | 0.02 * |
| β-blockers | 6 (8.57%) | 5 (25%) | 0.04 * |
| Insulin | 3 (4.28%) | 2 (10%) | 0.32 |
| Complications | 10 (15.71%) | 4 (20%) | 0.53 |
| Shock | 2 (2.85%) | 1 (5%) | 0.63 |
| Heart failure | 5 (3.5%) | 2 (10%) | 0.67 |
| Cardiac aneurysm | 1 (1.42%) | 1 (5%) | 0.33 |
| Death | 2 (2.85%) | 1 (5%) | 0.33 |
| Cardio-Metabolic Variables | Study Group (n = 70) | Control Group (n = 40) | t Value | 95% CI Upper-Lower Limits | p Value |
|---|---|---|---|---|---|
| Serum cTn-I pg/mL) | 74.54 ± 13.32 | 77.64 ± 12.22 | −0.98 | 3.33–9.53 | 0.33 |
| Serum vaspin(pg/mL) | 603.83 ± 18.13 | 542.75 ± 38.95 | 6.8 | 79.72–42.33 | <0.0001 ** |
| TC (mg/dL) | 199.28 ± 20.49 | 266.43 ± 16.59 | −15.1 | −134.29 | <0.0001 ** |
| TG (mg/dL) | 166.83 ± 17.34 | 254.73 ± 22.82 | −15.95 | −175.78 | <0.0001 ** |
| LDL (mg/dL) | 118.80 ± 8.75 | 164.71 ± 13.59 | −14.28 | −81.81 | <0.0001 ** |
| HDL(mg/dL) | 47.11 ± 9.86 | 50.76 ± 7.34 | −1.8 | 0.43–7.73 | 0.078 |
| VLDL (mg/dL) | 33.36 ± 5.83 | 50.94 ± 6.42 | −11.01 | −35.15 | <0.0001 ** |
| AI | 0.189 ± 0.012 | 0.341 ± 0.021 | −30.95 | −0.3 | <0.0001 ** |
| CRR | 4.23 ± 1.44 | 5.24 ± 1.98 | −2.12 | −2.01 | 0.04 * |
| SBP (mmHg) | 166.54 ± 21.54 | 155.87 ± 19.63 | 2.09 | 21.02–0.31 | 0.043 * |
| DBP (mmHg) | 92.23 ± 22.69 | 87.67 ± 13.75 | 1.11 | 12.78–3.66 | 0.27 |
| FBG (mg/dL) | 101.65 ± 11.93 | 97.87 ± 8.97 | 1.53 | 8.75–1.19 | 0.132 |
| PPG(mg/dL) | 128.64 ± 11.83 | 132.64 ± 12.74 | −1.25 | 2.50–10.50 | 0.21 |
| Hs-CRP (mg/L) | 2.95 ± 0.45 | 4.65 ± 1.84 | −4.09 | −3.39 | 0.0006 ** |
| Cardio-Metabolic Variables | STEMI (n = 25) | NSTEMI (n = 25) | Unstable Angina (n = 20) | Control (n = 40) |
|---|---|---|---|---|
| Serum cTn-I (pg/mL) | 74.12 ± 12.45 | 72.65 ± 22.49 | 54.45 ± 23.53 ** | 77.64 ± 12.22 |
| Serum vaspin (pg/mL) | 611.32 ± 33.64 ** | 588.67 ± 22.29 ** | 586.87 ± 33.72 ** | 542.75 ± 38.95 |
| TC (mg/dL) | 197.28 ± 21.77 ** | 192.99 ± 19.64 ** | 193.64 ± 20.65 ** | 266.43 ± 16.59 |
| TG (mg/dL) | 160.83 ± 19.42 ** | 167.54 ± 18.74 ** | 166.83 ± 16.84 ** | 254.73 ± 22.82 |
| LDL (mg/dL) | 117.78 ± 8.75 ** | 113.85 ± 9.98 ** | 112.63 ± 13.83 ** | 164.71 ± 13.59 |
| HDL (mg/dL) | 47.33 ± 9.77 | 45.63 ± 8.99 | 45.55 ± 8.33 * | 31.76 ± 7.34 |
| VLDL (mg/dL) | 32.16 ± 5.88 ** | 33.50 ± 4.34 ** | 33.57 ± 4.22 ** | 50.94 ± 6.42 |
| AI | 0.171 ± 0.011 ** | 0.205 ± 0.014 ** | 0.204 ± 0.012 ** | 0.341 ± 0.021 |
| CRR | 4.16 ± 1.65 | 4.22 ± 1.99 | 4.25 ± 1.86 | 5.24 ± 1.98 |
| SBP (mmHg) | 162.66 ± 20.33 | 165.62 ± 19.82 | 164.76 ± 18.93 | 155.87 ± 19.63 |
| DBP (mmHg) | 91.20 ± 20.39 | 93.53 ± 20.37 | 93.77 ± 20.53 | 87.67 ± 13.75 |
| Pulse pressure (mmHg) | 71.46 ± 11.76 | 72.09 ± 10.74 | 70.99 ± 11.55 | 68.20 ± 9.33 |
| FBG (mg/dL) | 101.44 ± 10.98 | 100.54 ± 10.71 | 104.61 ± 9.88 | 97.87 ± 8.97 |
| PPG (mg/dL) | 129.60 ± 10.82 | 127.55 ± 9.76 | 126.83 ± 9.38 | 132.64 ± 12.74 |
| Hs-CRP (mg/L) | 2.93 ± 0.44 ** | 2.89 ± 0.45 ** | 1.44 ± 0.11 ** | 4.65 ± 1.84 |
| Variables | STEMI (n = 25) | NSTEMI (n = 25) | UA (n = 20) | Control (n = 40) | ||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| Serum cTn-I (pg/mL) | 0.87 | 0.001 * | 0.77 | 0.0001 * | 0.44 | NS | 0.94 | 0.0001 * |
| TC (mg/dL) | −0.52 | 0.007 * | −0.67 | 0.0002 * | −0.67 | 0.001 * | −0.56 | 0.007 * |
| TG (mg/dL) | −0.41 | 0.04 ! | −0.32 | NS | −0.36 | NS | −0.75 | 0.001 * |
| LDL (mg/dL) | −0.33 | NS | −0.32 | NS | 0.38 | NS | −0.63 | 0.0002 * |
| HDL (mg/dL) | 0.66 | 0.0003 * | 0.69 | 0.0002 * | 0.71 | 0.0004 * | 0.51 | 0.008 * |
| VLDL (mg/dL) | −0.31 | NS | −0.34 | NS | −0.38 | NS | −0.42 | 0.006 * |
| AI | −0.41 | 0.04 ! | −0.35 | NS | −0.41 | NS | −0.51 | 0.0007 * |
| CRR | −0.34 | NS | −0.31 | NS | −0.37 | NS | −0.41 | 0.008 * |
| SBP (mmHg) | −0.33 | NS | −0.36 | NS | −0.32 | NS | −0.42 | 0.006 * |
| DBP (mmHg) | −0.37 | NS | −0.30 | NS | −0.22 | NS | −0.41 | 0.008 * |
| FBG (mg/dL) | −0.28 | NS | −0.32 | NS | −0.30 | NS | −0.33 | 0.03 ! |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-kuraishy, H.M.; Al-Gareeb, A.I.; Al-Buhadilly, A.K. Rosuvastatin Improves Vaspin Serum Levels in Obese Patients with Acute Coronary Syndrome. Diseases 2018, 6, 9. https://doi.org/10.3390/diseases6010009
Al-kuraishy HM, Al-Gareeb AI, Al-Buhadilly AK. Rosuvastatin Improves Vaspin Serum Levels in Obese Patients with Acute Coronary Syndrome. Diseases. 2018; 6(1):9. https://doi.org/10.3390/diseases6010009
Chicago/Turabian StyleAl-kuraishy, Hayder M., Ali I. Al-Gareeb, and Ali K. Al-Buhadilly. 2018. "Rosuvastatin Improves Vaspin Serum Levels in Obese Patients with Acute Coronary Syndrome" Diseases 6, no. 1: 9. https://doi.org/10.3390/diseases6010009
APA StyleAl-kuraishy, H. M., Al-Gareeb, A. I., & Al-Buhadilly, A. K. (2018). Rosuvastatin Improves Vaspin Serum Levels in Obese Patients with Acute Coronary Syndrome. Diseases, 6(1), 9. https://doi.org/10.3390/diseases6010009