Fatal Human Case of Zika and Chikungunya Virus Co-Infection with Prolonged Viremia and Viruria

 , ,
, , 
Abstract
:1. Introduction
2. Case Presentation
3. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Azevedo, R.S.; Araujo, M.T.; Martins Filho, A.J.; Oliveira, C.S.; Nunes, B.T.; Cruz, A.C.; Nascimento, A.G.; Medeiros, R.C.; Caldas, C.A.; Araujo, F.C.; et al. Zika vírus epidemic in Brazil. I. Fatal disease in adults: Clinical and laboratorial aspects. J. Clin. Virol. 2016, 85, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Zonneveld, R.; Roosblad, J.; Staveren, J.W.; Wilschut, J.C.; Vreden, S.G.; Codrington, J. Three atypical lethal cases associated with acute Zika virus infection in Suriname. IDCases 2016, 5, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, I.R.F.; Frontera, J.A.; Bispo de Filippis, A.M.; Nascimento, O.J.M.D.; RIO-GBS-ZIKV Research Group. Neurologic complications associated with the Zika Virus in Brazilian adults. JAMA Neurol. 2017, 74, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Roimicher, L.; Ferreira, O.C., Jr.; Arruda, M.B.; Tanuri, A. Zika Virus in the joint of a patient with rheumatoid arthritis. J. Rheumatol. 2017, 44, 535. [Google Scholar] [CrossRef] [PubMed]
- Villamil-Gómez, W.E.; Rodriguez-Moeales, A.J.; Uribe-Garcia, A.M.; González-Arismendy, E.; Castellanos, J.E.; Calvo, E.P.; Álvares-mon, M.; Musso, D. Zika, Dengue and Chikungunya co-infection in a pregnant woman from Colombia. Int. J. Infect. Dis. 2016, 51, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.R.T.; Faria, N.R.; de Vasconcelos, J.M.; Golding, N.; Kraemer, M.U.; de Oliveira, L.F.; da Silva Azevedo, R.d.S.; Andrade da Silva, D.E.; Pinto da Silva, E.V.; da Silva, S.P.; et al. Emergence and potential for spread of Chikungunya virus in Brazil. BMC Med. 2015, 13, 102. [Google Scholar] [CrossRef] [PubMed]
- Campos, G.S.; Bandeira, A.C.; Sardi, S.I. Zika Virus Outbreak, Bahia, Brazil. Emerg. Infect. Dis. 2015, 21, 1885–1886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelser, E.A. Meet dengue’s cousin, Zika. Microbes Infect. 2016, 18, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Panella, A.J.; Velez, J.O.; Lambert, A.J.; Campbell, G.L. Chikungunya virus in US travelers returning from India, 2006. Emerg. Infect. Dis. 2007, 13, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Waggoner, J.J.; Pinsky, B.A. Zika virus: Diagnostics for an emerging pandemic threat. J. Clin. Microbiol. 2016, 54, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Dupont-Rouzeyrol, M.; O’Connor, O.; Calvez, E.; Daurès, M.; John, M.; Grangeon, J.P.; Gourinat, A.C. Co-infection with Zika and Dengue Viruses in 2 Patients, New Caledonia, 2014. Emerg. Infect. Dis. 2015, 21, 381–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambrano, H.; Waggoner, J.J.; Almeida, C.; Rivera, L.; Benjamin, J.Q.; Pinsky, B.A. Case Report: Zika Virus and Chikungunya Virus CoInfections: A Series of Three Cases from a Single Center in Ecuador. Am. J. Trop. Med. Hyg. 2016, 95, 894–896. [Google Scholar] [CrossRef] [PubMed]
- Kutsuna, S.; Kato, Y.; Nakayama, E.; Taniguchi, S.; Takasaki, T.; Yamamoto, K.; Takeshita, N.; Hayakawa, K.; Kanagawa, S.; Ohmagari, N. A case of consecutive infection with Zika virus and Chikungunya virus in Bora Bora, French Polynesia. J. Infect. Chemother. 2017, 23, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Villamil-Gómez, W.E.; González-Camargo, O.; Rodriguez-Ayubi, J.; Zapata-Serpa, D.; Rodriguez-Morales, A.J. Dengue, chikungunya and Zika co-infection in a patient from Colombia. J. Infect. Public Health 2016, 9, 684–686. [Google Scholar] [CrossRef] [PubMed]
- Sardi, S.I.; Somasekar, S.; Naccache, S.N.; Bandeira, A.C.; Tauro, L.B.; Campos, G.S.; Chiu, C.Y. Coinfections of Zika and Chikungunya viruses in Bahia, Brazil, identified by metagenomic next-generation sequencing. J. Clin. Microbiol. 2016, 54, 2348–2353. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento-Ospina, A.; Vasquez-Serna, H.; Jimenez-Canizales, C.E.; Villamil-Gomez, W.E.; Rodriguez-Morales, A.J. Zika virus associated deaths in Colombia. Lancet Infect. Dis. 2016, 16, 523–524. [Google Scholar] [CrossRef]
- Paz-Bailey, G.; Rosenberg, E.S.; Doyle, K.; Munoz-Jordan, J.; Santiago, G.A.; Klein, L.; Perez-Padilla, J.; Medina, F.A.; Waterman, S.H.; Gubern, C.G.; et al. Persistence of Zika Virus in Body Fluids-Preliminary Report. N. Engl. J. Med. 2017. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Laboratory Findings | Pre Hospital Admission | Hospital Admission | Follow Up | ||||
|---|---|---|---|---|---|---|---|
| 1–52 dpo | ≥Day 53 dpo | >80 dpo | ≥89 dpo | 114–140 dpo | 141–266 dpo | 267–315 dpo | |
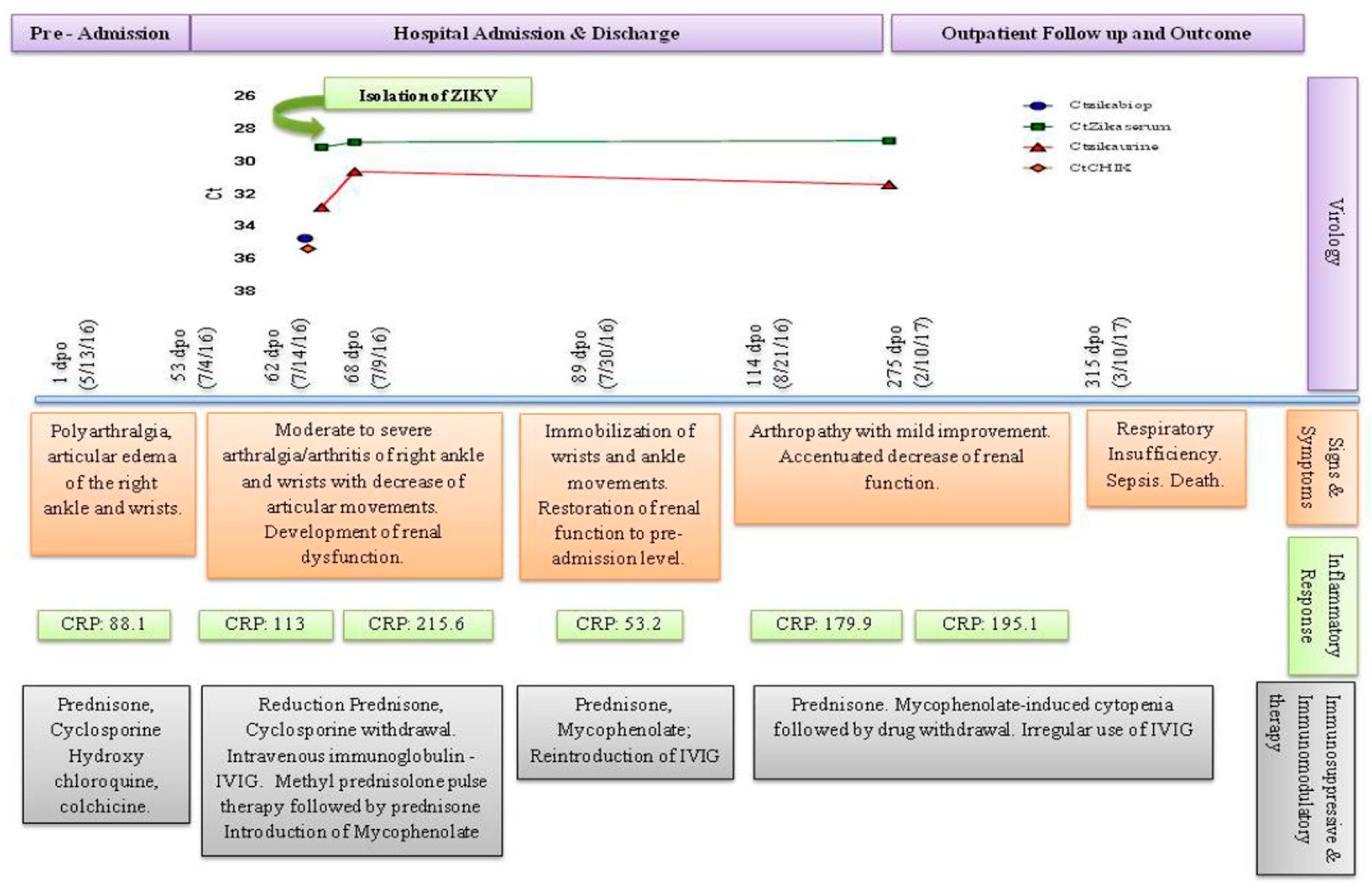
| ZIKV RNA tissue | Ct 34.7 | ||||||
| ZIKV RNA serum | Ct 29.1 | Ct 30.6 | Ct 30.4 | ||||
| ZIKV RNA urine | Ct 32.8 | Ct 28.8 | Ct 28.7 | ||||
| CHIKV RNA serum | Ct 35.3 | ||||||
| ZIKV isolation | Positive | ||||||
| CHIKV isolation | Negative | ||||||
| DENV NS1 | 0.541 | 0.456 | |||||
| Anti-DENV IgM | 0.011 | 0.012 | |||||
| Anti-DENV IgG | 0.337 | 2.116 | |||||
| Anti-CHIKV IgM | 0.0 * | 0.08 | |||||
| Anti-CHIKV IgG | 0.0 * | 0.08 | |||||
| BUN | 100 | 88 | 118 | 89 | 69 | 73 | 119 |
| Creatinine | 3.40 | 2.50 | 3.50 | 2.20 | 2.40 | 2.80 | 2.60 |
| Urinary Protein | 254 | 137 | 115 | ||||
| Proteinuria | 3+ | 3+ | 3+ | 3+ | 3+ | 3+ | |
| RBC (× 106/mm3) | 4.21 | 3.30 | 3.26 | 4.06 | 3.65 | 2.78 | 2.41 |
| Hematocrit (%) | 36 | 8.80 | 8.90 | 11.20 | 9.50 | 7.70 | 6.10 |
| Hemoglobin (g/dL) | 11.8 | 26.40 | 27.60 | 34.00 | 30.00 | 33.60 | 18.90 |
| WBC (mm3) | 10,800 | 12,600 | 9300 | 9000 | 6800 | 2300 | 3900 |
| Neutrophils (mm3, %) | 7884 (73) | 9941 (79) | 7254 (78) | 8109 (90) | 4964 (73) | 1127 (49) | 2652 (68) |
| Lymphocytes (mm3, %) | 2052 (19) | 1235 (9.8) | 1395 (15) | 594 (6.6) | 1156 (17) | 943 (41) | 975 (25) |
| Platelets | 165,000 | 380,000 | 249,000 | 252,000 | 240,000 | 211,000 | 8700 |
| IgA | <25 | ||||||
| IgE | <18 | ||||||
| IgG | 267 | ||||||
| IgM | <17 | ||||||
| ANA | Negative | ||||||
| Hospital Admission | Follow Up | |
|---|---|---|
| USG | ≥Day 53dpo (7/4/16) Wrists: Tenosynovitis with severe SP. PDIII Right Ankle: Moderate SP; PD II | Day141-266 dpo (9/29/16–2/1/17) Wrists: Moderate to severe SP. PD II to III Right Ankle: Mild to Moderate SP; PD I |
| BSc | Day 114–140 dpo ((9/2–9/28/16) Prominent localized inflammation in the right and left wrists and right ankle. | |
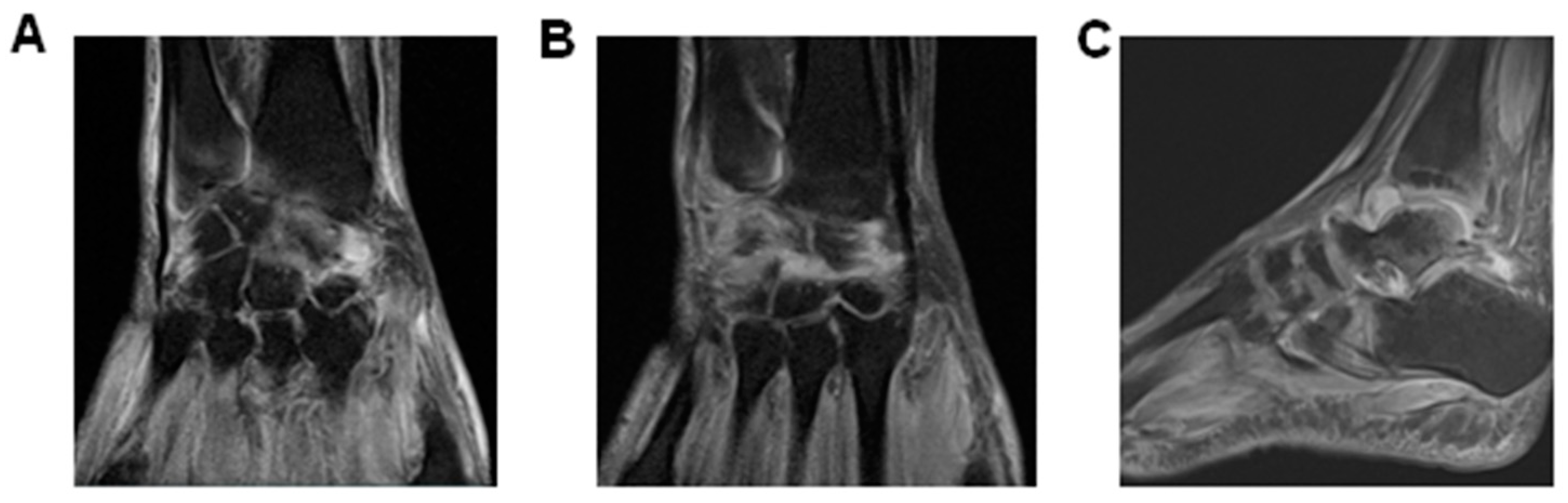
| MRI | Day 114–140 dpo (9/2–9/28/16) Right Ankle\Subchondral areas of talo-tibial, talo-calcaneus, navicular bone and Lisfranc & Chopard presented edema and inflammatory process compatible with synovitis. Liquid infiltration of foot plantar, abductors and flexor muscles. Extensive edema and inflammatory infiltration of soft tissues around the right ankle. Day 267–315dpo (2/2–3/10/17) Wrists: Test revealed synovitis and tenosynovitis. A moderate increase of intra-articular fluid. Augmented tendon thickening and intercarpal arthrosis. Marked periosteal inflammation and oedematous capitis with carpi synovitis. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, K.R.; Bica, B.E.R.G.; Pimenta, E.S.; Serafim, R.B.; Abreu, M.M.; Gonçalves, J.L.S.; Santana, L.D.S.; Cabral-Castro, M.J.; Peralta, J.M.; Cavalcanti, M.G. Fatal Human Case of Zika and Chikungunya Virus Co-Infection with Prolonged Viremia and Viruria. Diseases 2018, 6, 53. https://doi.org/10.3390/diseases6030053
Silva KR, Bica BERG, Pimenta ES, Serafim RB, Abreu MM, Gonçalves JLS, Santana LDS, Cabral-Castro MJ, Peralta JM, Cavalcanti MG. Fatal Human Case of Zika and Chikungunya Virus Co-Infection with Prolonged Viremia and Viruria. Diseases. 2018; 6(3):53. https://doi.org/10.3390/diseases6030053
Chicago/Turabian StyleSilva, Kelly R., Blanca E. R. G. Bica, Eduardo S. Pimenta, Rodrigo B. Serafim, Mirhelen M. Abreu, Jorge L. S. Gonçalves, Larissa De S. Santana, Mauro J. Cabral-Castro, José M. Peralta, and Marta G. Cavalcanti. 2018. "Fatal Human Case of Zika and Chikungunya Virus Co-Infection with Prolonged Viremia and Viruria" Diseases 6, no. 3: 53. https://doi.org/10.3390/diseases6030053
APA StyleSilva, K. R., Bica, B. E. R. G., Pimenta, E. S., Serafim, R. B., Abreu, M. M., Gonçalves, J. L. S., Santana, L. D. S., Cabral-Castro, M. J., Peralta, J. M., & Cavalcanti, M. G. (2018). Fatal Human Case of Zika and Chikungunya Virus Co-Infection with Prolonged Viremia and Viruria. Diseases, 6(3), 53. https://doi.org/10.3390/diseases6030053