
Role of Ranolazine in the Prevention and Treatment of Atrial Fibrillation in Patients with Left Ventricular Systolic Dysfunction: A Meta-Analysis of Randomized Clinical Trials

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
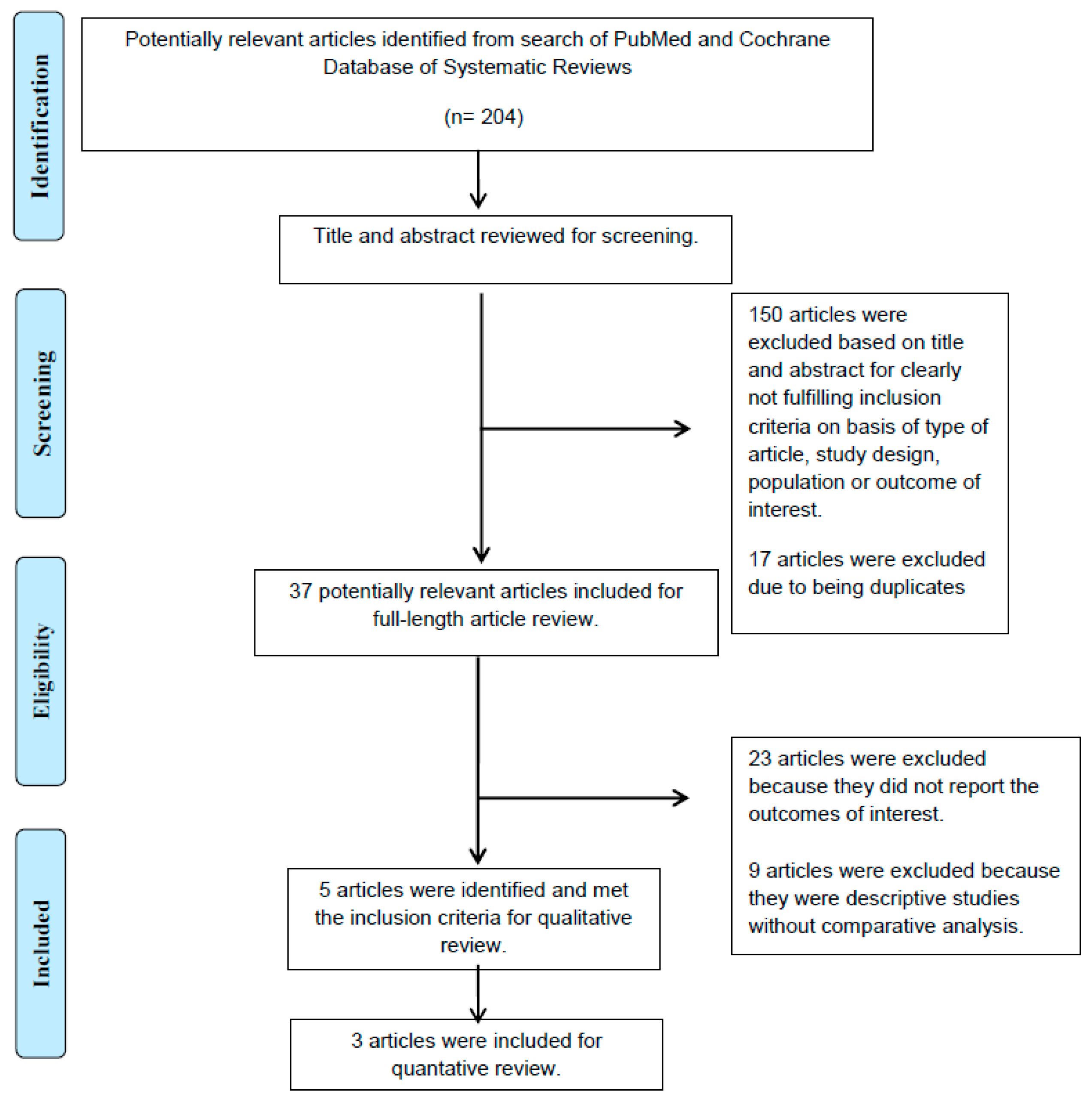
2.1. Literature Review and Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
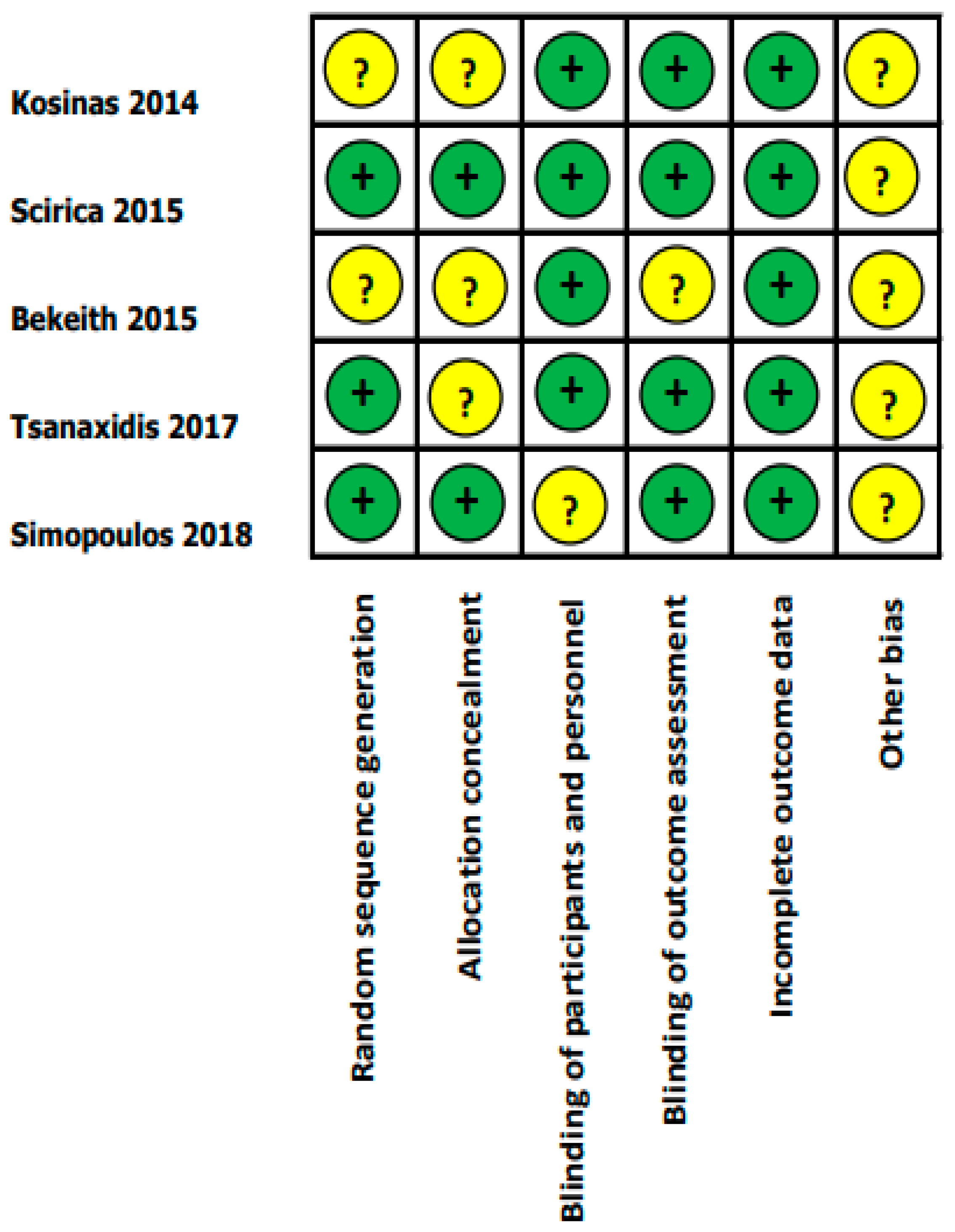
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
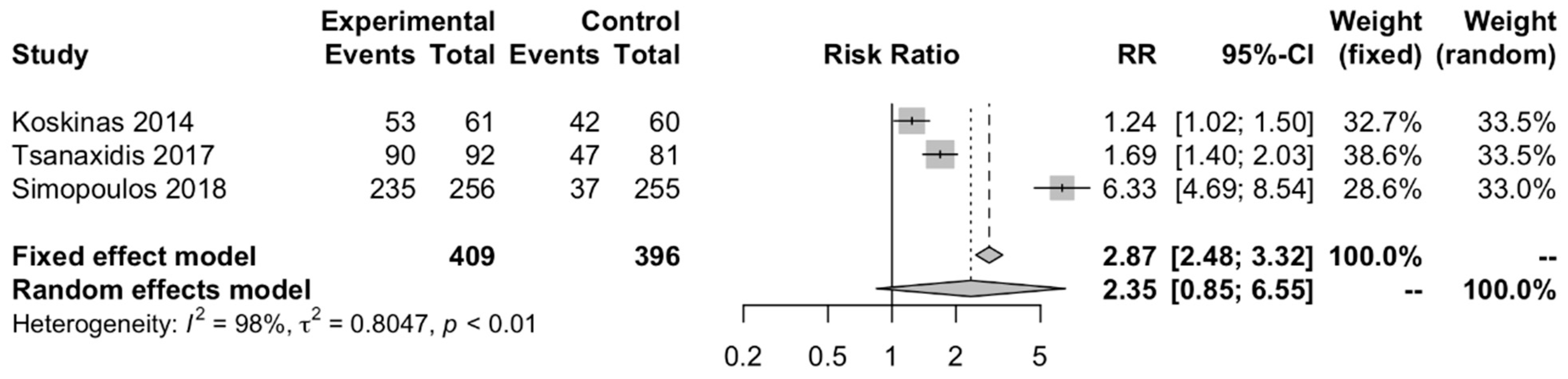
3.1. Sinus Rhythm Restoration Rate in AF Patients with LV Systolic Dysfunction
3.2. Incidence of AF in Various Clinical Settings
3.3. Safety Profile of Ranolazine
3.4. Evaluation for Publication Bias
4. Discussion
4.1. Ranolazine for Pharmacological Cardioversion of AF in LV Systolic Dysfunction
4.2. Ranolazine for Prevention of AF in LV Systolic Dysfunction
4.3. Ranolazine Safety in LV Systolic Dysfunction
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Moretz, K.; Poole, J.E.; Mascette, A.; Rosenberg, Y.; Jeffries, N.; et al. Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) Trial: Study Rationale and Design. Am. Heart J. 2018, 199, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Trulock, K.M.; Narayan, S.M.; Piccini, J.P. Rhythm Control in Heart Failure Patients With Atrial Fibrillation. Contemp. Chall. Incl. Role Ablation 2014, 64, 710–721. [Google Scholar] [CrossRef] [Green Version]
- Cosedis Nielsen, J.; Johannessen, A.; Raatikainen, P.; Hindricks, G.; Walfridsson, H.; Kongstad, O.; Pehrson, S.; Englund, A.; Hartikainen, J.; Mortensen, L.S.; et al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N. Engl. J. Med. 2012, 367, 1587–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA 2019, 321, 1261–1274. [Google Scholar] [CrossRef] [PubMed]
- Gaztañaga, L.; Frankel, D.S.; Kohari, M.; Kondapalli, L.; Zado, E.S.; Marchlinski, F.E. Time to recurrence of atrial fibrillation influences outcome following catheter ablation. Heart Rhythm 2013, 10, 2–9. [Google Scholar] [CrossRef]
- Shah, S.; Barakat, A.F.; Saliba, W.I.; Abdur Rehman, K.; Tarakji, K.G.; Rickard, J.; Bassiouny, M.; Baranowski, B.; Tchou, P.; Bhargava, M.; et al. Recurrent Atrial Fibrillation After Initial Long-Term Ablation Success: Electrophysiological Findings and Outcomes of Repeat Ablation Procedures. Circ. Arrhythm. Electrophysiol. 2018, 11, e005785. [Google Scholar] [CrossRef]
- Sultan, A.; Lüker, J.; Andresen, D.; Kuck, K.H.; Hoffmann, E.; Brachmann, J.; Hochadel, M.; Willems, S.; Eckardt, L.; Lewalter, T.; et al. Predictors of Atrial Fibrillation Recurrence after Catheter Ablation: Data from the German Ablation Registry. Sci. Rep. 2017, 7, 16678. [Google Scholar] [CrossRef] [Green Version]
- Darby, A.E. Recurrent Atrial Fibrillation After Catheter Ablation: Considerations For Repeat Ablation And Strategies To Optimize Success. J. Atr. Fibrillation 2016, 9, 1427. [Google Scholar] [CrossRef]
- Chaitman, B.R. Ranolazine for the treatment of chronic angina and potential use in other cardiovascular conditions. Circulation 2006, 113, 2462–2472. [Google Scholar] [CrossRef] [Green Version]
- Burashnikov, A.; Antzelevitch, C. Role of late sodium channel current block in the management of atrial fibrillation. Cardiovasc. Drugs Ther. 2013, 27, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Gong, M.; Zhang, Z.; Fragakis, N.; Korantzopoulos, P.; Letsas, K.P.; Li, G.; Yan, G.X.; Liu, T. Role of ranolazine in the prevention and treatment of atrial fibrillation: A meta-analysis of randomized clinical trials. Heart Rhythm 2017, 14, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Rosa, G.M.; Dorighi, U.; Ferrero, S.; Brunacci, M.; Bertero, G.; Brunelli, C. Ranolazine for the treatment of atrial fibrillation. Expert Opin. Investig. Drugs 2015, 24, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Romandini, A.; Barbarossa, A.; Belardinelli, L.; Capucci, A. Ranolazine for rhythm control in atrial fibrillation: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 227, 284–291. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Bekeith, S.; Meghani, M.; Shariff, M.A.; Asti, D.; Nalluri, N.; Agarwal, V.; Shah, N.; Soomro, A.; Khan, M.; Spagnola, J.; et al. Abstract 13387: Effect of Ranolazine on the Incidence of Atrial Fibrillation Following Cardiac Surgery. Circulation 2015, 132, A13387. [Google Scholar] [CrossRef]
- Koskinas, K.C.; Fragakis, N.; Katritsis, D.; Skeberis, V.; Vassilikos, V. Ranolazine enhances the efficacy of amiodarone for conversion of recent-onset atrial fibrillation. Europace 2014, 16, 973–979. [Google Scholar] [CrossRef] [Green Version]
- Scirica, B.M.; Belardinelli, L.; Chaitman, B.R.; Waks, J.W.; Volo, S.; Karwatowska-Prokopczuk, E.; Murphy, S.A.; Cheng, M.L.; Braunwald, E.; Morrow, D.A. Effect of ranolazine on atrial fibrillation in patients with non-ST elevation acute coronary syndromes: Observations from the MERLIN-TIMI 36 trial. Europace 2015, 17, 32–37. [Google Scholar] [CrossRef] [Green Version]
- Simopoulos, V.; Hevas, A.; Hatziefthimiou, A.; Dipla, K.; Skoularigis, I.; Tsilimingas, N.; Aidonidis, I. Amiodarone plus Ranolazine for Conversion of Post-Cardiac Surgery Atrial Fibrillation: Enhanced Effectiveness in Reduced Versus Preserved Ejection Fraction Patients. Cardiovasc. Drugs Ther. 2018, 32, 559–565. [Google Scholar] [CrossRef]
- Tsanaxidis, N.; Aidonidis, I.; Hatziefthimiou, A.; Daskalopoulou, S.S.; Giamouzis, G.; Triposkiadis, F.; Skoularigis, I. Ranolazine Added to Amiodarone Facilitates Earlier Conversion of Atrial Fibrillation Compared to Amiodarone-Only Therapy. Pacing Clin. Electrophysiol. 2017, 40, 372–378. [Google Scholar] [CrossRef]
- Fragakis, N.; Koskinas, K.C.; Katritsis, D.G.; Pagourelias, E.D.; Zografos, T.; Geleris, P. Comparison of effectiveness of ranolazine plus amiodarone versus amiodarone alone for conversion of recent-onset atrial fibrillation. Am. J. Cardiol. 2012, 110, 673–677. [Google Scholar] [CrossRef]
- Trivedi, C.; Upadhyay, A.; Solanki, K. Efficacy of ranolazine in preventing atrial fibrillation following cardiac surgery: Results from a meta-analysis. J. Arrhythm. 2017, 33, 161–166. [Google Scholar] [CrossRef]
- Antzelevitch, C.; Burashnikov, A.; Sicouri, S.; Belardinelli, L. Electrophysiologic basis for the antiarrhythmic actions of ranolazine. Heart Rhythm 2011, 8, 1281–1290. [Google Scholar] [CrossRef] [Green Version]
- Verrier, R.L.; Kumar, K.; Nieminen, T.; Belardinelli, L. Mechanisms of ranolazine’s dual protection against atrial and ventricular fibrillation. Europace 2013, 15, 317–324. [Google Scholar] [CrossRef]
- Burashnikov, A.; Di Diego, J.M.; Zygmunt, A.C.; Belardinelli, L.; Antzelevitch, C. Atrium-selective sodium channel block as a strategy for suppression of atrial fibrillation: Differences in sodium channel inactivation between atria and ventricles and the role of ranolazine. Circulation 2007, 116, 1449–1457. [Google Scholar] [CrossRef] [Green Version]
- Tsiachris, D.; Doundoulakis, I.; Pagkalidou, E.; Kordalis, A.; Deftereos, S.; Gatzoulis, K.A.; Tsioufis, K.; Stefanadis, C. Pharmacologic Cardioversion in Patients with Paroxysmal Atrial Fibrillation: A Network Meta-Analysis. Cardiovasc. Drugs Ther. 2021, 35, 293–308. [Google Scholar] [CrossRef]
- Sicouri, S.; Burashnikov, A.; Belardinelli, L.; Antzelevitch, C. Synergistic electrophysiologic and antiarrhythmic effects of the combination of ranolazine and chronic amiodarone in canine atria. Circ. Arrhythm. Electrophysiol. 2010, 3, 88–95. [Google Scholar] [CrossRef] [Green Version]
- De Vecchis, R.; Ariano, C.; Giasi, A.; Cioppa, C. Antiarrhythmic effects of ranolazine used both alone for prevention of atrial fibrillation and as an add-on to intravenous amiodarone for its pharmacological cardioversion: A meta-analysis. Minerva Cardioangiol. 2018, 66, 349–359. [Google Scholar] [CrossRef]
- Burashnikov, A.; Di Diego, J.M.; Barajas-Martínez, H.; Hu, D.; Cordeiro, J.M.; Moise, N.S.; Kornreich, B.G.; Belardinelli, L.; Antzelevitch, C. Ranolazine effectively suppresses atrial fibrillation in the setting of heart failure. Circ. Heart Fail. 2014, 7, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Sossalla, S.; Kallmeyer, B.; Wagner, S.; Mazur, M.; Maurer, U.; Toischer, K.; Schmitto, J.D.; Seipelt, R.; Schöndube, F.A.; Hasenfuss, G.; et al. Altered Na(+) currents in atrial fibrillation effects of ranolazine on arrhythmias and contractility in human atrial myocardium. J. Am. Coll Cardiol. 2010, 55, 2330–2342. [Google Scholar] [CrossRef] [Green Version]
- Verheule, S.; Wilson, E.; Everett, T.t.; Shanbhag, S.; Golden, C.; Olgin, J. Alterations in atrial electrophysiology and tissue structure in a canine model of chronic atrial dilatation due to mitral regurgitation. Circulation 2003, 107, 2615–2622. [Google Scholar] [CrossRef] [Green Version]
- Georgios, I.T.; Isaac, A.; Stella, S.D.; Vassilios, S.; Vassilios, L.; Marios, E.D.; Charalampos, P.; Kiriaki, P.; Ioannis, S.; Filippos, T.; et al. Effect of Ranolazine in Preventing Postoperative Atrial Fibrillation in Patients Undergoing Coronary Revascularization Surgery. Curr. Vasc. Pharmacol. 2013, 11, 988–991. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Koskinas 2014 [20] | Scirica 2015 [21] | Bekeith 2015 [19] | Tsanaxidis 2017 [23] | Simopoulos 2018 [22] | |
|---|---|---|---|---|---|
| Characteristics of RCT | |||||
| Design | Single center, RCT, SB | RCT, DB | Single center, RCT, DB | Single center, RCT, PROBE | Single center, RCT, SB |
| Intervention group | Ranolazine 1500 mg once plus IV amiodarone | IV ranolazine with a 200 mg bolus, then 80 mg/h for 12–96 h, then oral ranolazine 1000 mg bid | Oral ranolazine 1000 mg bid 48 h prior to surgery to 14th postoperative day | Oral ranolazine 1000 mg once plus IV amiodarone | Ranolazine 55 mg once, then 375 mg 6 h later, then 375 mg bid plus IV amiodarone |
| Control group | IV amiodarone loading dose 5 mg/kg then 50 mg/h for 24 h | Placebo | Placebo | IV amiodarone loading dose 5 mg/kg in 1 h then 50 mg/h | IV amiodarone 300 mg then 1125 mg/36 h |
| Primary endpoint, Number of events | Conversion of AF to SR within 24 h | Cardiovascular death, MI, recurrent ischemia | POAF | Time to conversion of AF | Time to conversion of POAF |
| Method of AF detection | Continuous ECG monitoring for 24 h | Continuous ECG monitoring for the first 7 days | Holter monitoring for 2 weeks | Continuous ECG monitoring | 12-lead ECG every 4 h, if not, convert within 12 h, then Holter monitoring for 24 h |
| Follow-up period | 24 h | 12 months | 2 weeks | 24 h | 36 h |
| Characteristics of patients in RCT | |||||
| Country | Greece | US | US | Greece | Greece |
| Study population | Recent-onset AF (<48 h) | NSTEMI, SR | Postoperative cardiac surgery, SR | Recent-onset AF (<48 h) | Postoperative CABG, POAF |
| No. of patients | 61/60 | 3162/3189 | 27/27 | 92/81 | 256/255 |
| Mean age (years) | 66 ± 11/64 ± 9 | 63 ± 11/63 ± 11 | 64.3 ± 11.4 | 70 ± 10/67 ± 11 | 65.3 ± 9.5/65.5 ± 9.6 |
| Male (%) | 41/48 | 66.2/63.7 | 81 | 38/41 | 86.3/87.8 |
| LA diameter (mm) | 49 ± 8/46 ± 6 | NA | NA | 4.1 ± 0.4/4.2 ± 0.5 | 48.1 ± 2.7/48.3 ± 2.6 |
| LVEF (%) | 58 ± 7/54 ± 10 (LVEF < 50%, 25%/20%) | LVEF < 40%, 13.9%/13.4%) | 45.4 ± 14.6 | 52 ± 10/53 ± 8 (LVEF < 50%, 14%/8%) | 36.6 ± 4.8/36.5 ± 4.7 |
| Study results | |||||
| Incidence of AF | NA | 55/75 | 5/8 | NA | NA |
| Conversion of AF to SR within 24 h | 53/42 | NA | NA | 90/47 | 235/37 |
| Time to AF conversion | 10.2 + 3.3/13.3 + 4.1 | NA | NA | 8.6 ± 2.8/19.4 ± 4.4 | 10.4 ± 4.5/24.3 ± 4.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leelapatana, P.; Thongprayoon, C.; Prasitlumkum, N.; Vallabhajosyula, S.; Cheungpasitporn, W.; Chokesuwattanaskul, R. Role of Ranolazine in the Prevention and Treatment of Atrial Fibrillation in Patients with Left Ventricular Systolic Dysfunction: A Meta-Analysis of Randomized Clinical Trials. Diseases 2021, 9, 31. https://doi.org/10.3390/diseases9020031
Leelapatana P, Thongprayoon C, Prasitlumkum N, Vallabhajosyula S, Cheungpasitporn W, Chokesuwattanaskul R. Role of Ranolazine in the Prevention and Treatment of Atrial Fibrillation in Patients with Left Ventricular Systolic Dysfunction: A Meta-Analysis of Randomized Clinical Trials. Diseases. 2021; 9(2):31. https://doi.org/10.3390/diseases9020031
Chicago/Turabian StyleLeelapatana, Pattranee, Charat Thongprayoon, Narut Prasitlumkum, Saraschandra Vallabhajosyula, Wisit Cheungpasitporn, and Ronpichai Chokesuwattanaskul. 2021. "Role of Ranolazine in the Prevention and Treatment of Atrial Fibrillation in Patients with Left Ventricular Systolic Dysfunction: A Meta-Analysis of Randomized Clinical Trials" Diseases 9, no. 2: 31. https://doi.org/10.3390/diseases9020031
APA StyleLeelapatana, P., Thongprayoon, C., Prasitlumkum, N., Vallabhajosyula, S., Cheungpasitporn, W., & Chokesuwattanaskul, R. (2021). Role of Ranolazine in the Prevention and Treatment of Atrial Fibrillation in Patients with Left Ventricular Systolic Dysfunction: A Meta-Analysis of Randomized Clinical Trials. Diseases, 9(2), 31. https://doi.org/10.3390/diseases9020031