
CD3+, CD8+, CD4+ and FOXP3+ T Cells in the Immune Microenvironment of Small Bowel Neuroendocrine Tumors


Abstract
:1. Introduction
2. Materials and Methods
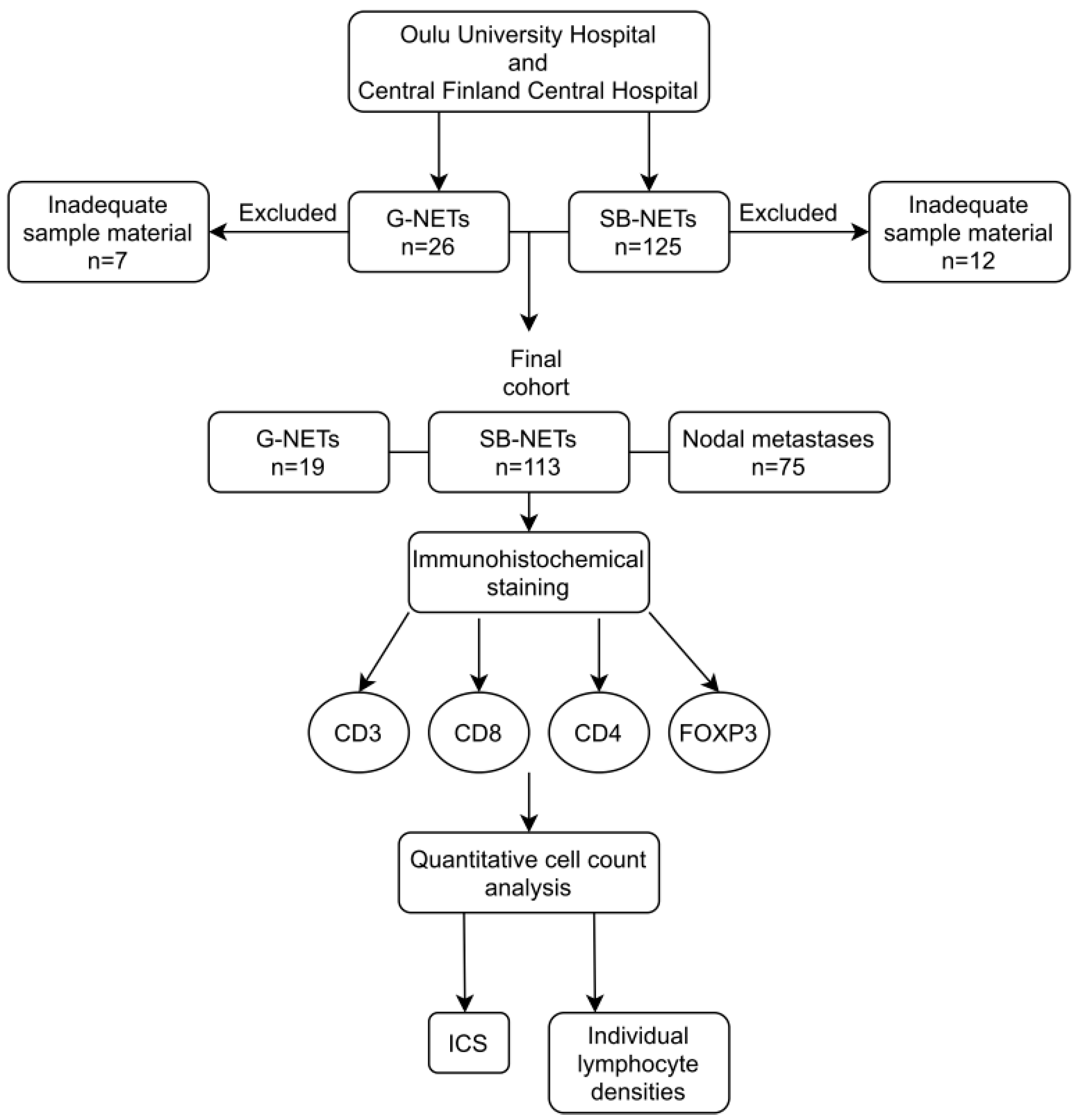
2.1. Patients
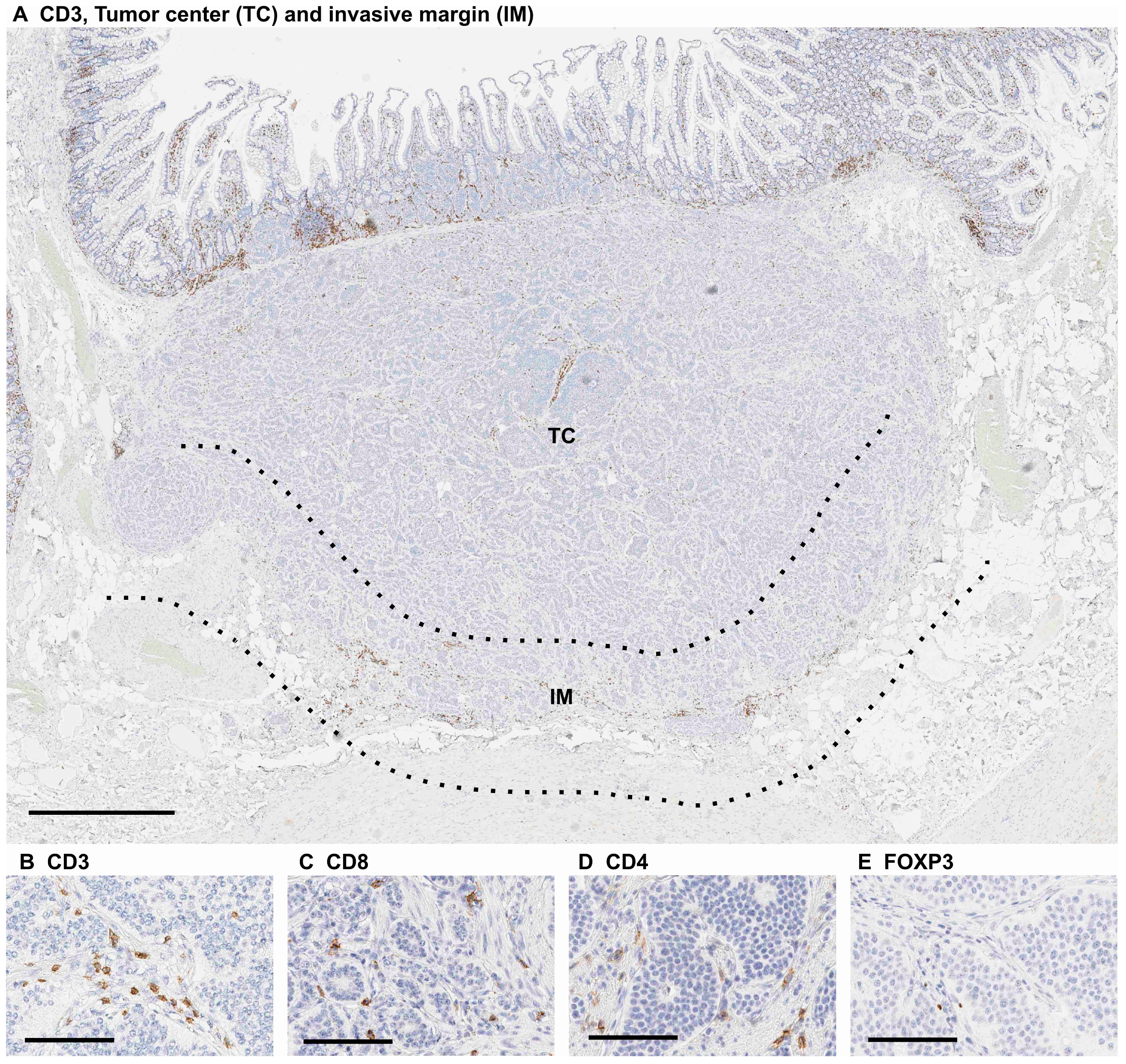
2.2. Immunohistochemical Staining
2.3. Scoring
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
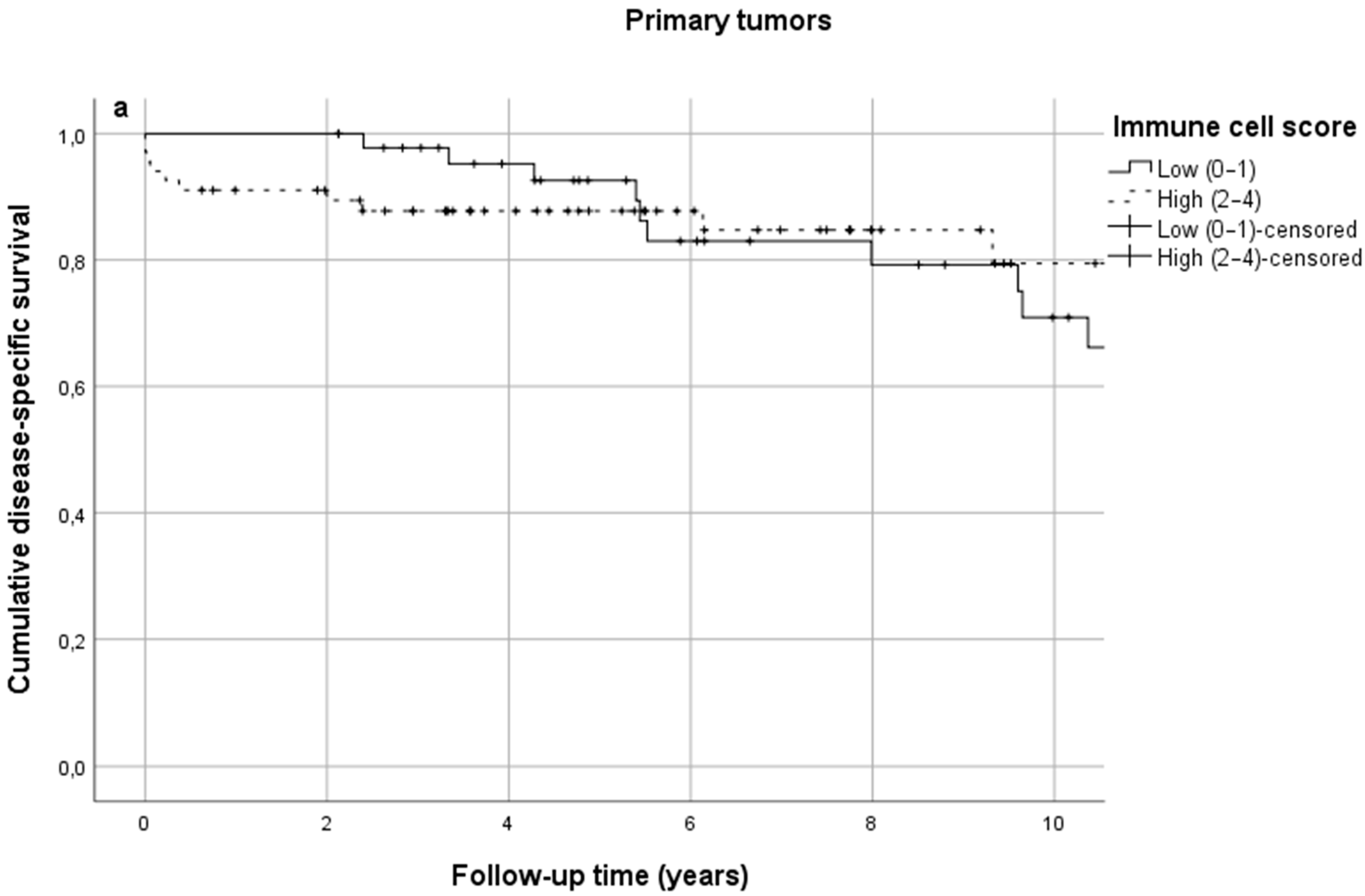
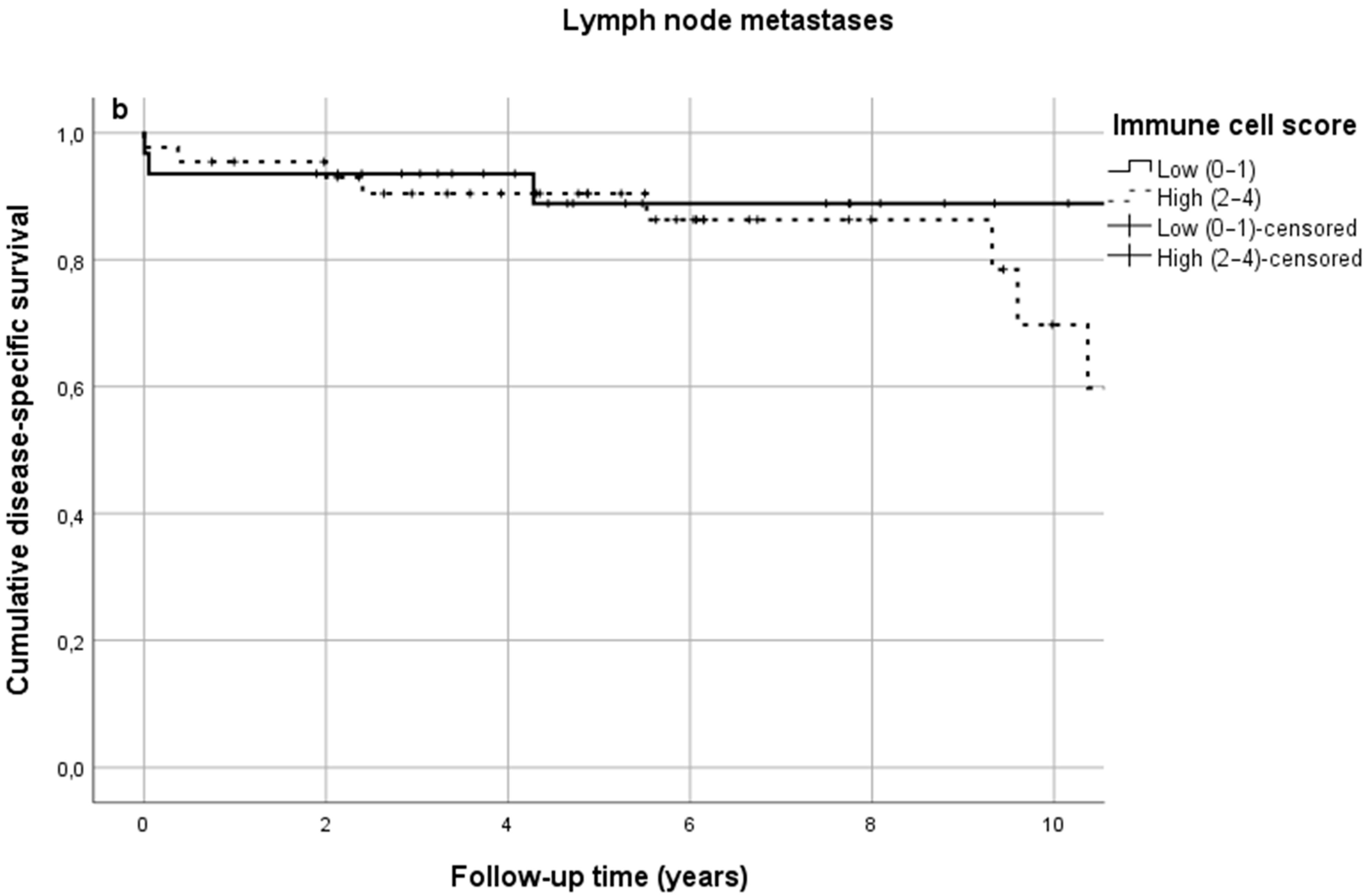
3.2. Immune Cell Score—No Prognostic Value in Primary Tumors or Lymph Node Metastases
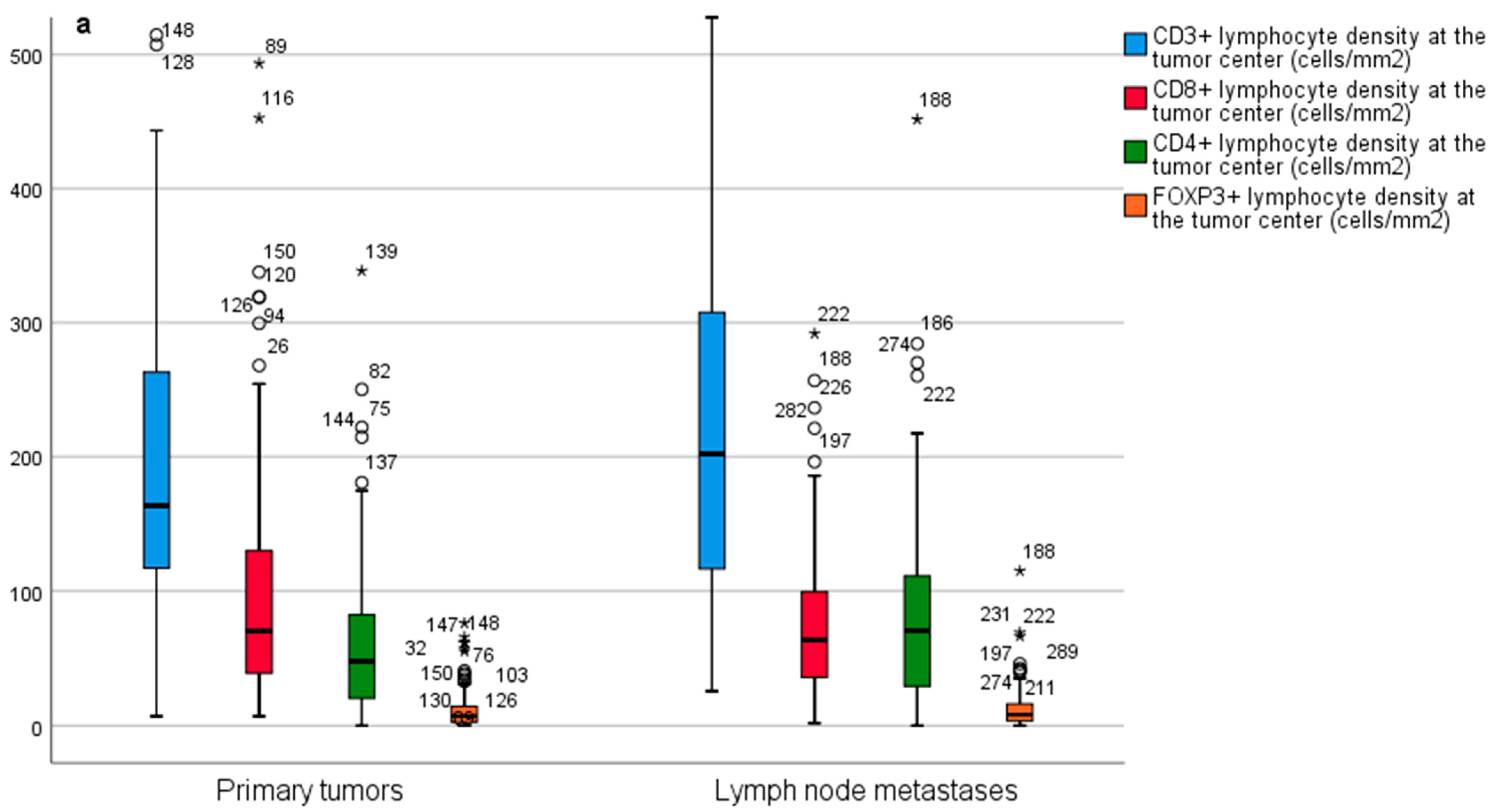
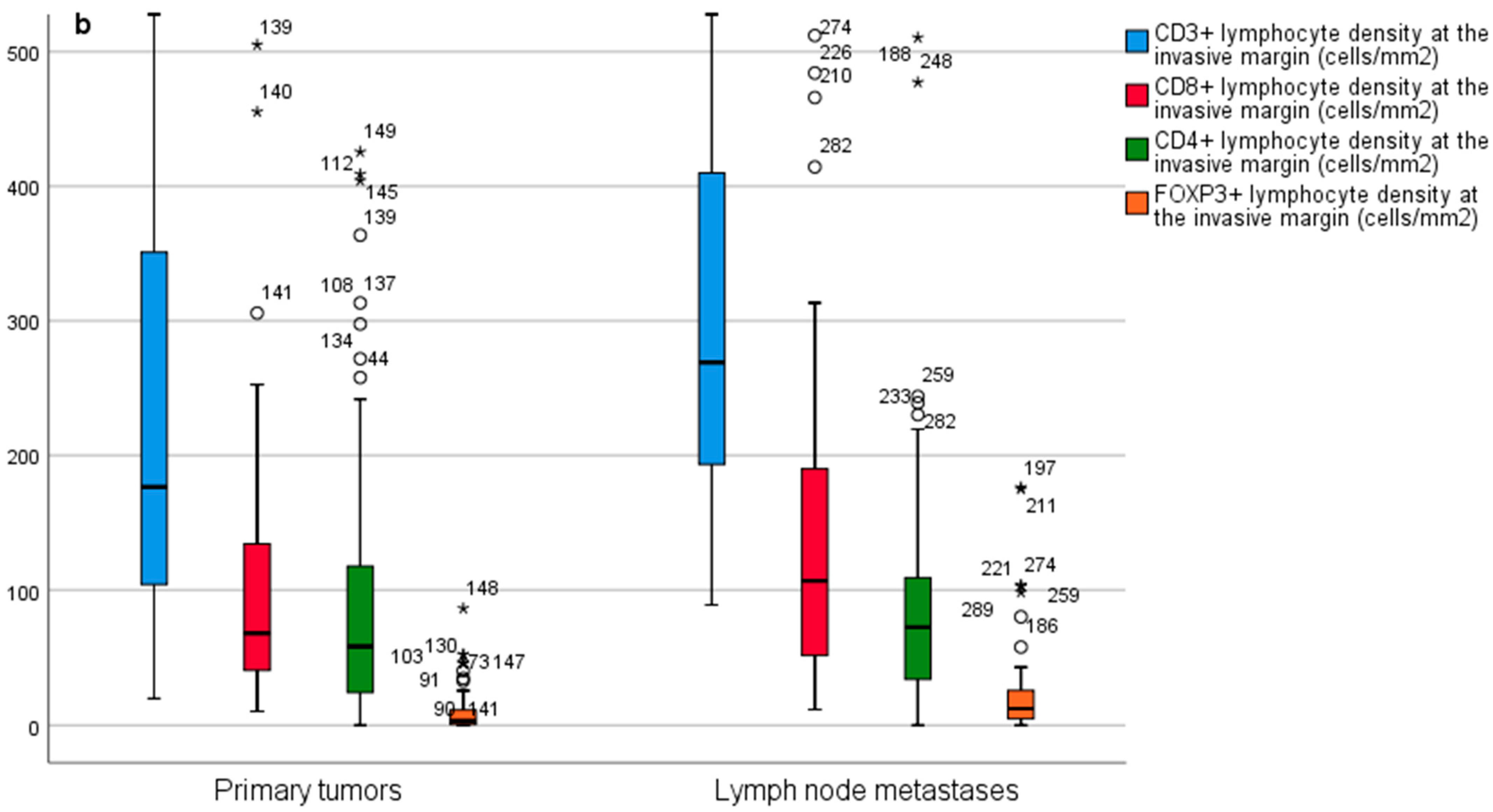
3.3. Individual Lymphocyte Densities in Primary Tumors Have No Prognostic Value
3.4. Individual Lymphocyte Densities in Lymph Node Metastases Have No Prognostic Value
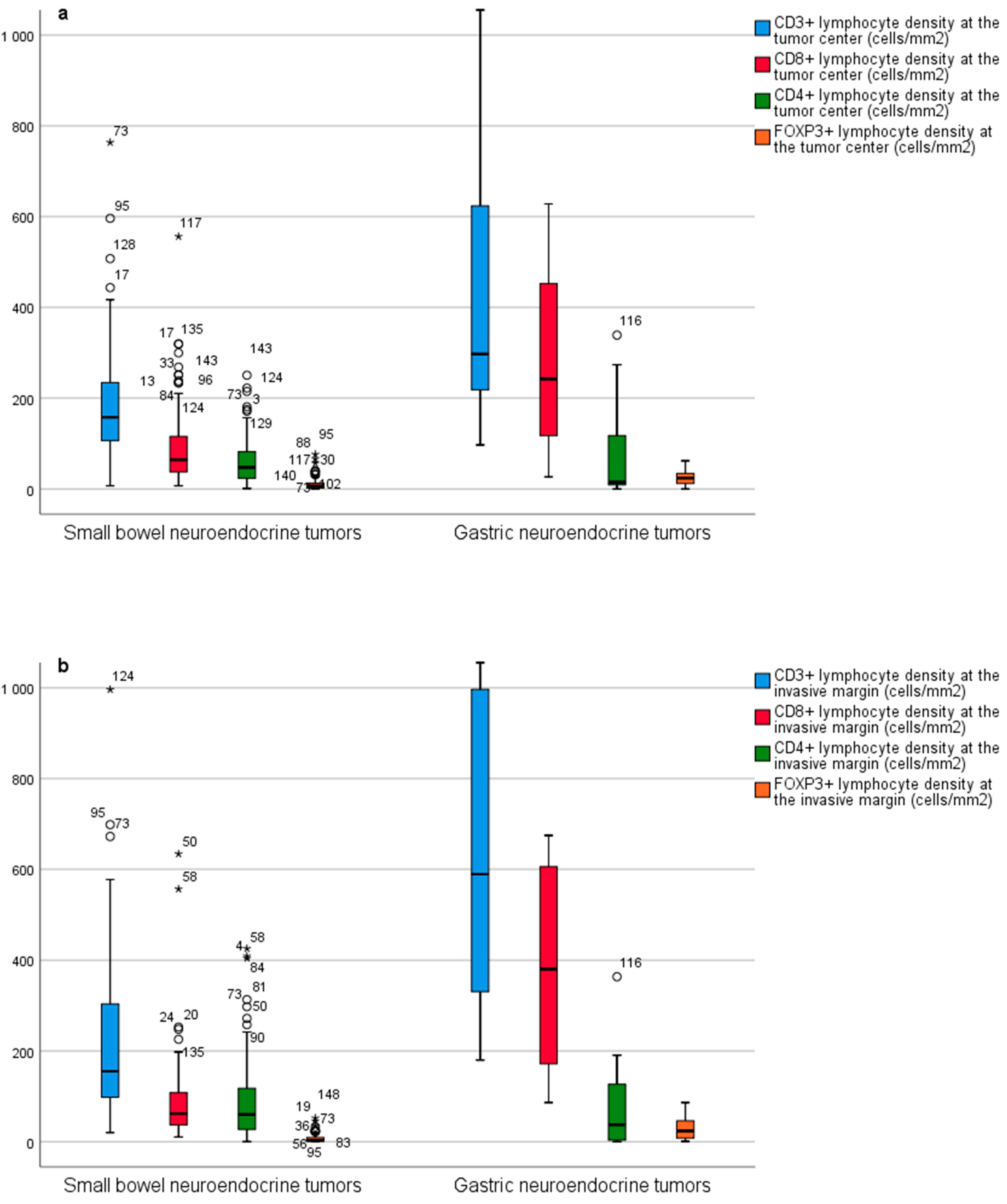
3.5. Immune Microenvironment in SB-NETs and G-NETs—Lower T Cell Densities in SB-NETs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fernandez, C.J.; Agarwal, M.; Pottakkat, B.; Haroon, N.N.; George, A.S.; Pappachan, J.M. Gastroenteropancreatic neuroendocrine neoplasms: A clinical snapshot. World J. Gastrointest. Surg. 2021, 13, 231–255. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Hassan, M.M.; Phan, A.T.; Dagohoy, C.G.; Leary, C.C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.-N.; Rashid, A.; et al. One Hundred Years After “Carcinoid”: Epidemiology of and Prognostic Factors for Neuroendocrine Tumors in 35,825 Cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasari, A.; Shen, C.; Halperin, D.M.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Niederle, M.B.; Hackl, M.; Kaserer, K.; Niederle, B. Gastroenteropancreatic neuroendocrine tumours: The current incidence and staging based on the WHO and European Neuroendocrine Tumour Society classification: An analysis based on prospectively collected parameters. Endocrine-Relat. Cancer 2010, 17, 909–918. [Google Scholar] [CrossRef]
- Fridman, W.H.; Zitvogel, L.; Sautès-Fridman, C.; Kroemer, G. The immune contexture in cancer prognosis and treatment. Nat. Rev. Clin. Oncol. 2017, 14, 717–734. [Google Scholar] [CrossRef]
- Şenbabaoğlu, Y.; Gejman, R.S.; Winer, A.G.; Liu, M.; Van Allen, E.M.; De Velasco, G.; Miao, D.; Ostrovnaya, I.; Drill, E.; Luna, A.; et al. Tumor immune microenvironment characterization in clear cell renal cell carcinoma identifies prognostic and immunotherapeutically relevant messenger RNA signatures. Genome Biol. 2016, 17, 231. [Google Scholar] [CrossRef] [Green Version]
- Galon, J.; Costes, A.; Sanchez-Cabo, F.; Kirilovsky, A.; Mlecnik, B.; Lagorce-Pagès, C.; Tosolini, M.; Camus, M.; Berger, A.; Wind, P.; et al. Type, Density, and Location of Immune Cells Within Human Colorectal Tumors Predict Clinical Outcome. Science 2006, 313, 1960–1964. [Google Scholar] [CrossRef] [Green Version]
- Pagès, F.; Mlecnik, B.; Marliot, F.; Bindea, G.; Ou, F.-S.; Bifulco, C.; Lugli, A.; Zlobec, I.; Rau, T.T.; Berger, M.D.; et al. International validation of the consensus Immunoscore for the classification of colon cancer: A prognostic and accuracy study. Lancet 2018, 391, 2128–2139. [Google Scholar] [CrossRef]
- Galon, J.; Mlecnik, B.; Bindea, G.; Angell, H.K.; Berger, A.; Lagorce, C.; Lugli, A.; Zlobec, I.; Hartmann, A.; Bifulco, C.; et al. Towards the introduction of the ‘Immunoscore’ in the classification of malignant tumours. J. Pathol. 2014, 232, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Yang, J.; Du, L.; Zhou, Y.; Li, K. The prognostic value of Immunoscore in patients with cancer: A pooled analysis of 10,328 patients. Int. J. Biol. Mark. 2020, 35, 3–13. [Google Scholar] [CrossRef]
- Wei, M.; Xu, J.; Hua, J.; Meng, Q.; Liang, C.; Liu, J.; Zhang, B.; Wang, W.; Yu, X.; Shi, S. From the Immune Profile to the Immunoscore: Signatures for Improving Postsurgical Prognostic Prediction of Pancreatic Neuroendocrine Tumors. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef]
- Tay, R.E.; Richardson, E.K.; Toh, H.C. Revisiting the role of CD4+ T cells in cancer immunotherapy—New insights into old paradigms. Cancer Gene Ther. 2021, 28, 5–17. [Google Scholar] [CrossRef]
- Goto-Silva, L.; Junqueira, M. Single-cell proteomics: A treasure trove in neurobiology. Biochim. Biophys. Acta Proteins Proteom. 2021, 1869, 140658. [Google Scholar] [CrossRef]
- Alexovič, M.; Sabo, J.; Longuespée, R. Microproteomic sample preparation. Proteomics 2021, 21, 2000318. [Google Scholar] [CrossRef]
- Woltering, E.A.; Bergsland, E.K.; Beyer, D.T.; O’Dorisio, T.M.; Rindi, G.; Klimstra, D.S.; Tang, L.H.; Reidy-Lagunes, D.; Strosberg, J.R.; Wolin, E.M.; et al. Neuroendocrine Tumors of the Jejunum and Ileum; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2016; pp. 375–387. [Google Scholar]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, M.K.; Carneiro, F.; Cree, I.A. The WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemi, N.; Hiltunen, N.; Väyrynen, J.P.; Pohjanen, V.-M.; Helminen, O.; Junttila, A.; Mrena, J.; Böhm, J.; Huhta, H.; Leppänen, J.; et al. Immune Cell Infiltrate and Prognosis in Gastric Cancer. Cancers 2020, 12, 3604. [Google Scholar] [CrossRef]
- da Silva, A.; Bowden, M.; Zhang, S.; Masugi, Y.; Thorner, A.R.; Herbert, Z.T.; Zhou, C.W.; Brais, L.; Chan, J.A.; Hodi, F.S.; et al. Characterization of the Neuroendocrine Tumor Immune Microenvironment. Pancreas 2018, 47, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.; Ying, H.; Li, J.; Gao, Y.; Sun, Z.; Li, J.; Bai, C.; Cheng, Y.; Wu, H. Immune Checkpoint Markers in Neuroendocrine Carcinoma of the Digestive System. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef]
- Ferrata, M.; Schad, A.; Zimmer, S.; Musholt, T.J.; Bahr, K.; Kuenzel, J.; Becker, S.; Springer, E.; Roth, W.; Weber, M.M.; et al. PD-L1 Expression and Immune Cell Infiltration in Gastroenteropancreatic (GEP) and Non-GEP Neuroendocrine Neoplasms with High Proliferative Activity. Front. Oncol. 2019, 9, 343. [Google Scholar] [CrossRef] [Green Version]
- Lamarca, A.; Nonaka, D.; Breitwieser, W.; Ashton, G.; Barriuso, J.; McNamara, M.G.; Moghadam, S.; Rogan, J.; Mansoor, W.; Hubner, R.A.; et al. PD-L1 expression and presence of TILs in small intestinal neuroendocrine tumours. Oncotarget 2018, 9, 14922–14938. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.C.; Donkor, C.; Glasgow, K.; Pillarisetty, V.G.; Gönen, M.; Espat, N.J.; Klimstra, D.S.; D’Angelica, M.I.; Allen, P.J.; Jarnagin, W.; et al. T cell infiltrate and outcome following resection of intermediate-grade primary neuroendocrine tumours and liver metastases. HPB 2010, 12, 674–683. [Google Scholar] [CrossRef] [Green Version]
- de Reuver, P.R.; Mehta, S.; Gill, P.; Andrici, J.; D’Urso, L.; Clarkson, A.; Mittal, A.; Hugh, T.J.; Samra, J.S.; Gill, A.J. Immunoregulatory Forkhead Box Protein p3-Positive Lymphocytes Are Associated with Overall Survival in Patients with Pancreatic Neuroendocrine Tumors. J. Am. Coll. Surg. 2016, 222, 281–287. [Google Scholar] [CrossRef]
- Jiao, Y.; Shi, C.; Edil, B.H.; De Wilde, R.F.; Klimstra, D.S.; Maitra, A.; Schulick, R.D.; Tang, L.H.; Wolfgang, C.L.; Choti, M.A.; et al. DAXX/ATRX, MEN1, and mTOR Pathway Genes Are Frequently Altered in Pancreatic Neuroendocrine Tumors. Science 2011, 331, 1199–1203. [Google Scholar] [CrossRef] [Green Version]
- Samsom, K.G.; Van Veenendaal, L.M.; Valk, G.D.; Vriens, M.R.; Tesselaar, M.; Berg, J.G.V.D. Molecular prognostic factors in small-intestinal neuro-endocrine tumours. Endocr. Connect. 2019, 8, 906–922. [Google Scholar] [CrossRef] [Green Version]
- Lynch, H.T.; Drescher, K.M.; de la Chapelle, A. Immunology and the Lynch Syndrome. Gastroenterology 2008, 134, 1246–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samsom, K.G.; Levy, S.; van Veenendaal, L.M.; Roepman, P.; Kodach, L.L.; Steeghs, N.; Valk, G.D.; Dercksen, M.W.; Kuhlmann, K.F.; Verbeek, W.H.; et al. Driver mutations occur frequently in metastases of well-differentiated small intestine neuroendocrine tumours. Histopathology 2021, 78, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Teng, M.W.L.; Ngiow, S.F.; Ribas, A.; Smyth, M.J. Classifying Cancers Based on T-cell Infiltration and PD-L1. Cancer Res. 2015, 75, 2139–2145. [Google Scholar] [CrossRef] [Green Version]
- Lipson, E.J.; Vincent, J.G.; Loyo, M.; Kagohara, L.T.; Luber, B.S.; Wang, H.; Xu, H.; Nayar, S.K.; Wang, T.S.; Sidransky, D.; et al. PD-L1 Expression in the Merkel Cell Carcinoma Microenvironment: Association with Inflammation, Merkel Cell Polyomavirus, and Overall Survival. Cancer Immunol. Res. 2013, 1, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.; He, Y.; Zhou, C. P47.13 Galectin-9, A Novel Prognostic Factor in Small Cell Lung Cancer. J. Thorac. Oncol. 2021, 16, S498. [Google Scholar] [CrossRef]
- Xu, Y.; Cui, G.; Jiang, Z.; Li, N.; Zhang, X. Survival analysis with regard to PD-L1 and CD155 expression in human small cell lung cancer and a comparison with associated receptors. Oncol. Lett. 2019, 17, 2960–2968. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.P.; Othus, M.; Chae, Y.K.; Giles, F.J.; Hansel, D.E.; Singh, P.P.; Fontaine, A.; Shah, M.H.; Kasi, A.; Al Baghdadi, T.; et al. A Phase II Basket Trial of Dual Anti–CTLA-4 and Anti–PD-1 Blockade in Rare Tumors (DART SWOG 1609) in Patients with Nonpancreatic Neuroendocrine Tumors. Clin. Cancer Res. 2020, 26, 2290–2296. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Small Bowel NET, n = 113 | Gastric NET, n = 19 |
|---|---|---|
| Sex | ||
| Female, n (%) | 50 (44.2) | 12 (63.2) |
| Male, n (%) | 63 (55.8) | 7 (36.8) |
| Age, median (IQR) years | 65.2 (55.3–72.4) | 61.7 (52.8–68.1) |
| Immune Cell Score, Primary Tumors | ||
| 0, n (%) | 27 (23.9) | |
| 1, n (%) | 19 (16.8) | |
| 2, n (%) | 26 (23.0) | |
| 3, n (%) | 14 (12.4) | |
| 4, n (%) | 27 (23.9) | |
| Immune Cell Score, Lymph Node Metastases | ||
| 0, n (%) | 18 (24.0) | |
| 1, n (%) | 13 (17.3) | |
| 2, n (%) | 12 (16.0) | |
| 3, n (%) | 17 (22.7) | |
| 4, n (%) | 15 (20.0) | |
| T-Class | ||
| TX, n (%) | 6 (5.3) | 11 (57.9) |
| Tis, n (%) | 0 | 1 (5.3) |
| T1, n (%) | 5 (4.4) | 3 (15.8) |
| T2, n (%) | 23 (20.4) | 4 (21.1) |
| T3, n (%) | 43 (38.1) | 0 |
| T4, n (%) | 36 (31.9) | 0 |
| N-Class | ||
| N0, n (%) | 21 (18.6) | 18 (94.7) |
| N1–2, n (%) | 92 (81.4) | 1 (5.3) |
| M-Class | ||
| M0, n (%) | 73 (64.6) | 18 (94.7) |
| M1, n (%) | 40 (35.4) | 1 (5.3) |
| Stage | ||
| I-II, n (%) | 13 (11.5) | 18 (94.7) |
| III, n (%) | 60 (53.1) | 0 |
| IV, n (%) | 40 (35.4) | 1 (5.3) |
| Grade | ||
| Not available, n (%) | 2 (1.8) | 3 (15.8) |
| 1, n (%) | 87 (77.0) | 9 (47.4) |
| 2, n (%) | 24 (21.2) | 7 (36.8) |
| 3, n (%) | 0 | 0 |
| Tumor Location | ||
| Ileum, n (%) | 106 (93.8) | |
| Jejunum, n (%) | 7 (6.2) | |
| Gastric corpus, n (%) | 19 (100) | |
| Somatostatin Analog Treatment | ||
| Yes, n (%) | 62 (54.9) | 1 (5.3) |
| Chemotherapy | ||
| No, n (%) | 96 (85.0) | 19 (100) |
| Preoperative, n (%) | 5 (4.4) | 0 |
| Postoperative, n (%) | 12 (10.6) | 0 |
| Multiple Primary Tumors | ||
| Yes, n (%) | 32 (28.3) | 11 (57.9) |
| P-CgA | ||
| ≥3 nmol/L, n (%) | 87 (77.0) | 10 (52.6) |
| Median (IQR) nmol/L | 5.8 (3.4–14.0) | 9.4 (5.1–17.9) |
| dU-5-HIAA | ||
| ≥42 umol/L, n (%) | 52 (46.0) | 1 (5.3) |
| Median (IQR) umol/l | 44.0 (21.0–133) | 25.0 (17.5–47.0) |
| Atrophic Gastritis, n (%) | 0 | 15 (78.9) |
| DSS | No. of Patients | ICS Low (0–1) | ICS High (2–4) | p |
|---|---|---|---|---|
| Primary tumors | 113 | 5-year: 92.6% | 5-year: 87.8% | |
| 10-year: 53.8% | 10-year: 79.4% | 0.507 | ||
| Lymph node metastases | 75 | 5-year: 88.9% | 5-year: 90.4% | |
| 10-year: 71.1% | 10-year: 59.8% | 0.466 |
| No. of Patients | ICS Low (0–1) | ICS High (2–4) | |
|---|---|---|---|
| Primary Tumors | |||
| Crude | 113 | 1.00 (reference) | 0.75 (CI 0.32–1.75) |
| Adjusted | 113 | 1.00 (reference) | 1.37 (CI 0.56–3.38) |
| Lymph Node Metastases | |||
| Crude | 75 | 1.00 (reference) | 1.56 (CI 0.47–5.21) |
| Adjusted | 75 | 1.00 (reference) | 1.51 (CI 0.39–5.81) |
| DSS | TC Low | TC High | p-Value | IM Low | IM High | p-Value | |
|---|---|---|---|---|---|---|---|
| CD3+ | 5-year | 90.00% | 89.10% | 88.50% | 90.80% | ||
| 10-year | 54.80% | 77.60% | 0.584 | 60.50% | 68.10% | 0.612 | |
| CD8+ | 5-year | 90.40% | 90.90% | 92.40% | 88.60% | ||
| 10-year | 63.70% | 69.10% | 0.762 | 58.90% | 80.50% | 0.547 | |
| CD4+ | 5-year | 91.90% | 90.80% | 90.20% | 92.60% | ||
| 10-year | 63.50% | 71.70% | 0.913 | 64.40% | 66.70% | 0.884 | |
| FOXP3+ | 5-year | 89.80% | 91.00% | 90.30% | 90.80% | ||
| 10-year | 61.70% | 70.10% | 0.901 | 60.40% | 73.00% | 0.832 |
| DSS | TC Low | TC High | p-Value | IM Low | IM High | p-Value | |
|---|---|---|---|---|---|---|---|
| CD3+ | 5-year | 90.50% | 91.60% | 85.10% | 97.30% | ||
| 10-year | 72.40% | 57.70% | 0.366 | 70.90% | 60.90% | 0.798 | |
| CD8+ | 5-year | 91.10% | 88.40% | 90.90% | 88.90% | ||
| 10-year | 71.90% | 53.00% | 0.337 | 68.70% | 61.60% | 0.516 | |
| CD4+ | 5-year | 88.00% | 91.60% | 88.00% | 91.90% | ||
| 10-year | 51.90% | 77.20% | 0.539 | 63.40% | 65.30% | 0.737 | |
| FOXP3+ | 5-year | 87.90% | 91.70% | 85.60% | 94.40% | ||
| 10-year | 75.30% | 49.70% | 0.335 | 67.60% | 51.60% | 0.832 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiltunen, N.; Väyrynen, J.P.; Böhm, J.; Helminen, O. CD3+, CD8+, CD4+ and FOXP3+ T Cells in the Immune Microenvironment of Small Bowel Neuroendocrine Tumors. Diseases 2021, 9, 42. https://doi.org/10.3390/diseases9020042
Hiltunen N, Väyrynen JP, Böhm J, Helminen O. CD3+, CD8+, CD4+ and FOXP3+ T Cells in the Immune Microenvironment of Small Bowel Neuroendocrine Tumors. Diseases. 2021; 9(2):42. https://doi.org/10.3390/diseases9020042
Chicago/Turabian StyleHiltunen, Niko, Juha P. Väyrynen, Jan Böhm, and Olli Helminen. 2021. "CD3+, CD8+, CD4+ and FOXP3+ T Cells in the Immune Microenvironment of Small Bowel Neuroendocrine Tumors" Diseases 9, no. 2: 42. https://doi.org/10.3390/diseases9020042
APA StyleHiltunen, N., Väyrynen, J. P., Böhm, J., & Helminen, O. (2021). CD3+, CD8+, CD4+ and FOXP3+ T Cells in the Immune Microenvironment of Small Bowel Neuroendocrine Tumors. Diseases, 9(2), 42. https://doi.org/10.3390/diseases9020042