
A Review of Immunocryosurgery and a Practical Guide to Its Applications


Abstract
:1. Introduction
2. Action Mechanism of Immunocryosurgery
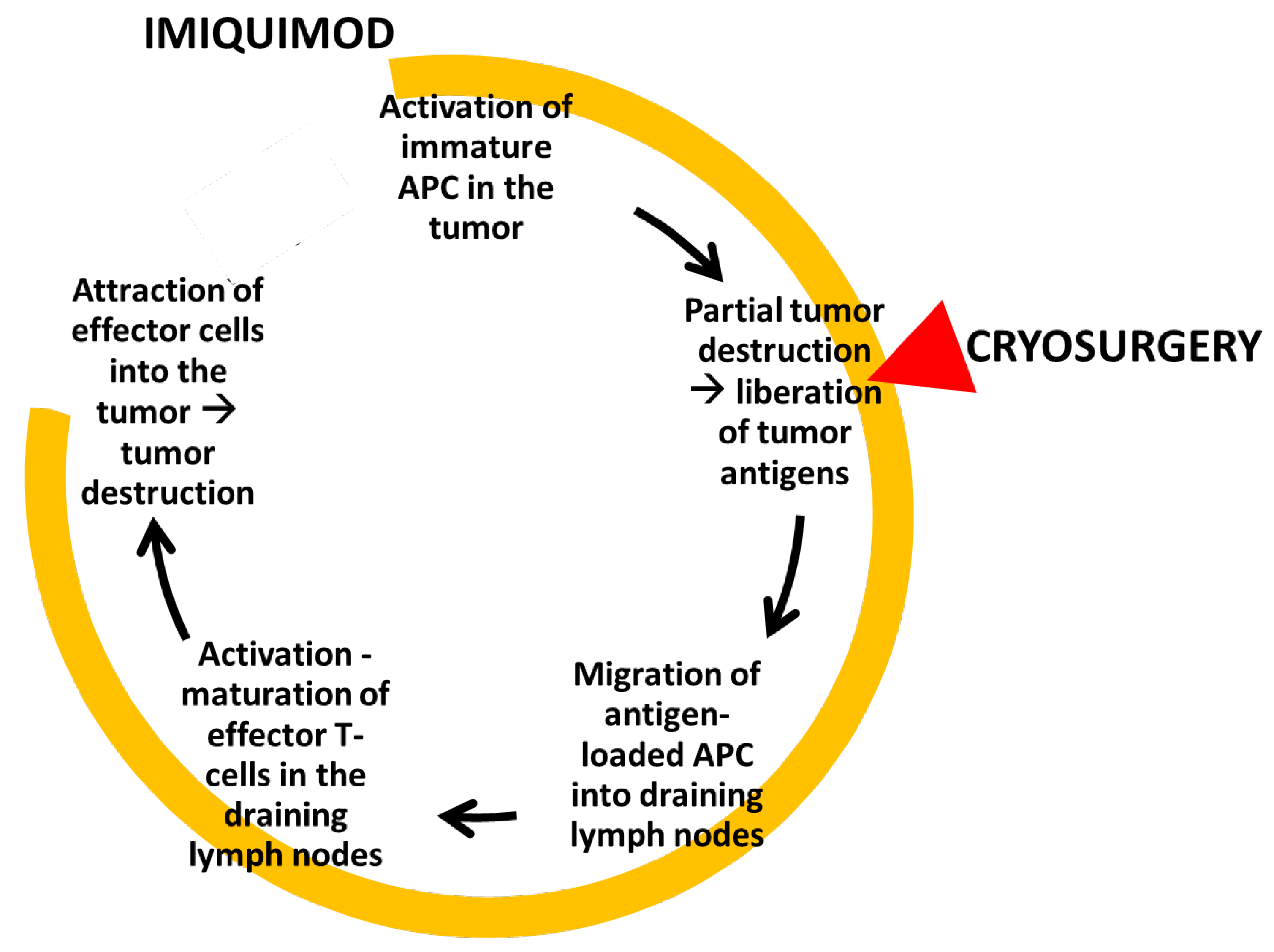
- The precryosurgery treatment of the tumor with imiquimod creates a proapoptotic environment within and around the tumor [15] that intensifies the destruction of the tumor cells during the ‘physical’ phase of the upcoming cryosurgery. This is especially important at the periphery of the treated lesion where effective freezing temperatures cannot be achieved without extensive damage to the adjacent healthy tissues.
- Finally, data originating from BCC studies suggest that a cascade of tissue events during immunocryosurgery leads to an efficient antitumor immune response (Figure 1).

3. Protocol of Immunocryosurgery
3.1. The Right “Intensity” of Inflammation
3.2. Management of Adverse Events
4. Indications of Immunocryosurgery
4.1. Keratinocytic Skin Cancers
4.1.1. Actinic Keratoses, Actinic Cheilitis, in situ Squamous Cell Carcinoma (Bowen’s Disease) and Keratoacanthoma
Actinic Keratoses
Actinic Cheilitis (Solar Cheilosis)
In Situ Squamous Cell Carcinoma (Bowen’s Disease)
Keratoacanthoma
4.1.2. Cutaneous Squamous Cell Carcinoma
4.1.3. Basal Cell Carcinoma
Locally confined BCC
Locally Advanced Basal Cell Carcinoma
Multiple Locally Confined Basal Cell Carcinoma
Palliative Therapy for Locally Advanced Basal Cell Carcinoma
4.2. Non Keratinocytic Skin Cancers
4.2.1. Lentigo Maligna and Malignant Melanoma
4.2.2. Sarcoma Kaposi
4.2.3. Merkel Cell Carcinoma
4.3. Non-Malignant Skin Lesions
4.3.1. Cutaneous and Genital Warts
4.3.2. Pyogenic Granuloma
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bassukas, I.D.; Gamvroulia, C.; Zioga, A.; Nomikos, K.; Fotika, C. Cryosurgery during topical imiquimod: A successful combination modality for lentigo maligna. Int. J. Dermatol. 2008, 47, 519–521. [Google Scholar] [CrossRef]
- Bassukas, I.D.; Gaitanis, G. Combination of cryosurgery and topical imiquimod: Does timing matter for successful immunocryosurgery? Cryobiology 2009, 59, 116–117. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Alexopoulos, E.C.; Bassukas, I.D. Cryosurgery is more effective in the treatment of primary, non-superficial basal cell carcinomas when applied during and not prior to a five week imiquimod course: A randomized, prospective, open-label study. Eur. J. Dermatol. 2011, 21, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Bassukas, I.D. Immunocryosurgery for non-superficial basal cell carcinoma: A prospective, open-label phase III study for tumours ≤ 2 cm in diameter. Acta Derm. Venereol. 2014, 94, 38–44. [Google Scholar] [CrossRef]
- Gaitanis, G.; Bassukas, I.D. Immunocryosurgery for non-superficial basal cell carcinomas ≤ 20 mm in maximal diameter: Five-year follow-up. J. Geriatr. Oncol. 2019, 10, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Bassukas, I.D. Immunocryosurgery—An effective combinational modality for Bowen’s disease. Dermatol. Ther. 2016. [Google Scholar] [CrossRef]
- Gaitanis, G.; Bassukas, I.D. Cryosurgery, Intralesional Methotrexate and Imiquimod for Keratoacanthoma: Tuning the Combination. Case Rep. Dermatol. Med. 2019, 2019, 3489748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voulgari, P.V.; Gaitanis, G.; Markatseli, T.E.; Kempf, W.; Bassukas, I.D. In transit recurrence of merkel cell carcinoma associated with polyarthritis effectively treated with immunocryosurgery. Acta Derm. Venereol. 2014, 94, 739–740. [Google Scholar] [CrossRef] [Green Version]
- Matas-Nadal, C.; Sòria, X.; García-de-la-Fuente, M.R.; Huerva, V.; Ortega, E.; Vilardell, F.; Gatius, S.; Casanova, J.M.; Martí, R.M. Immunocryosurgery as monotherapy for lentigo maligna or combined with surgical excision for lentigo maligna melanoma. J. Dermatol. 2018, 45, 564–570. [Google Scholar] [CrossRef]
- Gaitanis, G.; Vlachos, C.C.; Bassukas, I.D. Individualized, adjuvant-intensified immunocryosurgery for the treatment of squamous cell carcinoma in the oldest old: An exploratory case series. Actas Dermosifiliogr. 2021. in print. [Google Scholar]
- Gaitanis, G.; Ganiatsa, A.; Vartholomatos, G.; Karamoutsios, A.; Pappas, P.; Bassukas, I.D. Immunocryosurgery for basal cell carcinoma: Impact on circulating CD4+ CD25high T regulatory cells and serum cytokines. Eur. J. Dermatol. 2020, 605–606, in print. [Google Scholar] [CrossRef]
- Nomikos, K.; Lampri, E.; Spyridonos, P.; Bassukas, I.D. Alterations in the inflammatory cells infiltrating basal cell carcinomas during immunocryosurgery. Arch. Dermatol. Res. 2019, 311, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Redondo, P.; Del Olmo, J.; López-Diaz De Cerio, A.; Inoges, S.; Marquina, M.; Melero, I.; Bendandi, M. Imiquimod enhances the systemic immunity attained by local cryosurgery destruction of melanoma lesions. J. Investig. Dermatol. 2007, 127, 1673–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Den Brok, M.H.M.G.M.; Sutmuller, R.P.M.; Nierkens, S.; Bennink, E.J.; Frielink, C.; Toonen, L.W.J.; Boerman, O.C.; Figdor, C.G.; Ruers, T.J.M.; Adema, G.J. Efficient loading of dendritic cells following cryo and radiofrequency ablation in combination with immune modulation induces anti-tumour immunity. Br. J. Cancer 2006, 95, 896–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schön, M.P.; Schön, M. TLR7 and TLR8 as targets in cancer therapy. Oncogene 2008, 27, 190–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidbury, R.; Neuschler, N.; Neuschler, E.; Sun, P.; Wang, X.; Miller, R.; Tomai, Ã.M.; Puscasiu, E.; Gugneja, S.; Paller, A. Topically Applied Imiquimod Inhibits Vascular Tumor Growth In Vivo. J. Investig. Dermatol. 2003, 121, 1205–1209. [Google Scholar] [CrossRef] [Green Version]
- Wolf, I.H.; Kodama, K.; Cerroni, L.; Kerl, H. Nature of Inflammatory Infiltrate in Superficial Cutaneous Malignancies During Topical Imiquimod Treatment. Am. J. Dermatopathol. 2007, 29, 237–241. [Google Scholar] [CrossRef]
- Beatty, G.L.; Gladney, W.L. Immune escape mechanisms as a guide for cancer immunotherapy. Clin. Cancer Res. 2015, 21, 687–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaporis, H.G.; Guttman-Yassky, E.; Lowes, M.A.; Haider, A.S.; Fuentes-Duculan, J.; Darabi, K.; Whynot-Ertelt, J.; Khatcherian, A.; Cardinale, I.; Novitskaya, I.; et al. Human basal cell carcinoma is associated with Foxp3+ T cells in a Th2 dominant microenvironment. J. Investig. Dermatol. 2007, 127, 2391–2398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crittenden, M.R.; Thanarajasingam, U.; Vile, R.G.; Gough, M.J. Intratumoral immunotherapy: Using the tumour against itself. Immunology 2005, 114, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.R.; Shin, J.H.; Park, J.H.; Song, S.U.; Choi, G.S. Combined treatment with intratumoral injection of dendritic cells and topical application of imiquimod for murine melanoma. Clin. Exp. Dermatol. 2007, 32, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Urosevic, M.; Dummer, R.; Conrad, C.; Beyeler, M.; Laine, E.; Burg, G.; Gilliet, M. Disease-independent skin recruitment and activation of plasmacytoid predendritic cells following imiquimod treatment. J. Natl. Cancer Inst. 2005, 97, 1143–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Den Brok, M.H.M.G.M.; Sutmuller, R.P.M.; Nierkens, S.; Bennink, E.J.; Toonen, L.W.J.; Figdor, C.G.; Ruers, T.J.M.; Adema, G.J. Synergy between in situ cryoablation and TLR9 stimulation results in a highly effective in vivo dendritic cell vaccine. Cancer Res. 2006, 66, 7285–7292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urosevic, M.; Maier, T.; Benninghoff, B.; Slade, H.; Burg, G.; Dummer, R. Mechanisms underlying imiquimod-induced regression of basal cell carcinoma in vivo. Arch. Dermatol. 2003, 139, 1325–1332. [Google Scholar] [CrossRef] [Green Version]
- Machlenkin, A.; Goldberger, O.; Tirosh, B.; Paz, A.; Bar-haim, E.; Lee, S.; Tzehoval, E.; Eisenbach, L. Cancer Therapy: Preclinical Combined Dendritic Cell Cryotherapy of Tumor Induces Systemic Antimetastatic Immunity. Clin. Cancer Res. 2005, 11, 4955–4962. [Google Scholar] [PubMed] [Green Version]
- Gaitanis, G.; Bassukas, I.D. Intralesional bevacizumab as in-add adjuvant to immunocryosurgery for locally advanced basal cell carcinoma. J. Eur. Acad. Dermatol. Venereol. 2014, 28. [Google Scholar] [CrossRef] [PubMed]
- Knabel, P.; Cleaver, L. Arbor cutis: Hyperkeratotic plaque secondary to the use of imiquimod for the treatment of squamous cell carcinoma in situ. Dermatol. Surg. 2013, 39, 655–657. [Google Scholar] [CrossRef]
- Gaitanis, G.; Kalogeropoulos, C.; Bassukas, I.D. Imiquimod can be combined with cryosurgery (immunocryosurgery) for locally advanced periocular basal cell carcinomas. Br. J. Ophthalmol. 2011, 95, 890–892. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Kalogeropoulos, C.D.; Bassukas, I.D. Cryosurgery during Imiquimod (Immunocryosurgery) for Periocular Basal Cell Carcinomas: An Efficacious Minimally Invasive Treatment Alternative. Dermatology 2016, 232, 17–21. [Google Scholar] [CrossRef]
- Bassukas, I.D.; Ganiatsa, A.; Gaitanis, G. Health-related quality of life associated with immunocryosurgery, a minimally invasive modality, for cervicofacial basal cell carcinoma. Eur. J. Dermatol. 2019, 29, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Nakuçi, M.; Bassukas, I.D. Office-based treatment of basal cell carcinoma with immunocryosurgery: Feasibility and efficacy. Acta Dermatovenerol. Alp. Pannonica Adriat. 2013, 22, 35–38. [Google Scholar] [PubMed]
- Nakuci; Mikel Hôpital Valida, B. Récidive de Carcinome Basocellulaire, Traitée par Immunocryochirurgie-Skin. Available online: https://www.skin.be/fr/actualites/medical/recidive-de-carcinome-basocellulaire-traitee-par-immunocryochirurgie.html (accessed on 25 September 2021).
- Gaitanis, G.; Tronnier, M.; Zioga, A.; Spyridonos, P.; Bassukas, I.D. A neglected basal cell carcinoma in a young patient: Successful treatment with immunocryosurgery. Int. J. Adv. Med. 2015, 2, 406–410. [Google Scholar] [CrossRef] [Green Version]
- Manoli, S.M.; Moutsoudis, A.; Papageorgiou, C.; Lallas, K.; Rigas, H.M.; Kyrmanidou, E.; Papadimitriou, I.; Paschou, E.; Spyridis, I.; Gkentsidi, T.; et al. Real-life data on basal cell carcinoma treatment: Insights on clinicians’ therapeutic choices from an institutional hospital registry. Dermatol. Ther. 2020, 33, e14414. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Nomikos, K.; Vava, E.; Alexopoulos, E.C.; Bassukas, I.D. Immunocryosurgery for basal cell carcinoma: Results of a pilot, prospective, open-label study of cryosurgery during continued imiquimod application. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 1427–1431. [Google Scholar] [CrossRef] [PubMed]
- Apalla, Z.; Karteridou, A.; Lallas, A.; Tzellos, T.; Lefaki, I.; Sotiriou, E.; Varytimiadis, D. Letter: Immunocryotherapy for difficult-to-treat basal cell carcinoma of the eyelid. Dermatol. Surg. 2013, 39, 146–147. [Google Scholar] [CrossRef]
- Gaitanis, G.; Nomikos, K.; Vlachos, C.; Bassukas, I.D. Immunocryosurgery for patients with therapeutically challenging basal cell carcinomas: Report of two representative cases. J. Dermatol. Treat. 2012, 23, 70–71. [Google Scholar] [CrossRef]
- Gaitanis, G.; Mitsou, G.; Tsiouri, G.; Alexis, I.; Bassukas, I.D. Cryosurgery during imiquimod cream treatment (“immunocryosurgery” ) for Bowen’s disease of the skin: A case series. Acta Derm. Venereol. 2010, 90, 533–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benmously-Mlika, R.; Hammami-Ghorbel, H.; Koubaa, W.; Debbiche, A.; Mokhtar, I. Bowen’s disease of the digit successfully treated with immunocryosurgery. Int. J. Dermatol. 2013, 52, 514–516. [Google Scholar] [CrossRef]
- Oro-Ayude, M.; Gonzalez-Sixto, B.; Faraldo-Lorenzo, J.M.; Feal, C.; Flórez, A. Periocular lentigo maligna successfully treated with immunocryosurgery. Dermatol. Ther. 2021, 34, e14561. [Google Scholar] [CrossRef] [PubMed]
- Gaitanis, G.; Bassukas, I.M. Long-term outcomes of imiquimod-treated lentigo maligna: Add on cryosurgery to induce inflammation and increase efficacy? Clin. Exp. Dermatol. 2020, 45, 272. [Google Scholar] [CrossRef]
- Bratton, E.M.; Knutsen-Larson, S.; Durairaj, V.D.; Gregory, D.G.; Mellette, J.R. Combination topical therapy for conjunctival primary acquired melanosis with atypia and periocular lentigo maligna. Cornea 2015, 34, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.; Stockfleth, E.; Peris, K.; Aractingi, S.; Alomar, A.; Dakovic, R.; Dirschka, T. Long-term sustained lesion clearance from Lmax with imiquimod 3.75%, a new field-directed treatment for actinic keratosis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1840–1842. [Google Scholar] [CrossRef]
- Jadotte, Y.T.; Schwartz, R.A. Solar cheilosis: An ominous precursor: Part I. Diagnostic insights. J. Am. Acad. Dermatol. 2012, 66, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Spyridonos, P.; Gaitanis, G.; Tzaphlidou, M.; Bassukas, I.D. Spatial fuzzy c-means algorithm with adaptive fuzzy exponent selection for robust vermilion border detection in healthy and diseased lower lips. Comput. Methods Programs Biomed. 2014, 114, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, I.; Cruz, A.; Chang, K.H.; Dufresne, R.G. Treatment of squamous cell carcinoma in situ: A review. Dermatol. Surg. 2011, 37, 1394–1411. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.S.; Cho, J.H.; Roh, Y.H.; Chung, M.S.; Baek, G.H. Bone Invasion by Squamous Cell Carcinoma In Situ (Bowen’s Disease) of the Finger During Treatment With Imiquimod 5% Cream: Case Report. J. Hand Surg. Am. 2010, 35, 999–1002. [Google Scholar] [CrossRef]
- Kwiek, B.; Schwartz, R.A. Keratoacanthoma (KA): An update and review. J. Am. Acad. Dermatol. 2016, 74, 1220–1233. [Google Scholar] [CrossRef] [PubMed]
- Carr, R.A.; Houghton, J.P. Histopathologists’ approach to keratoacanthoma: A multisite survey of regional variation in Great Britain and Ireland. J. Clin. Pathol. 2014, 67, 637–638. [Google Scholar] [CrossRef]
- Takai, T. Advances in histopathological diagnosis of keratoacanthoma. J. Dermatol. 2017, 44, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Gleich, T.; Chiticariu, E.; Huber, M.; Hohl, D. Keratoacanthoma: A distinct entity? Exp. Dermatol. 2016, 25, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dika, E.; Fanti, P.A.; Lambertini, M.; Scarfì, F.; Maria Ravaioli, G.; Veronesi, G.; Baraldi, C.; Guglielmo, A.; Patrizi, A. Cutaneous squamous cell carcinoma progression during imiquimod treatment. J. Am. Acad. Dermatol. 2018, 79, e11–e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hengge, U.R.; Schaller, J. Successful Treatment of Invasive Squamous Cell Carcinoma Using Topical Imiquimod. Arch. Dermatol. 2004, 140, 404–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oster-Schmidt, C. Two cases of squamous cell carcinoma treated with topical imiquimod 5%. J. Eur. Acad. Dermatol. Venereol. 2004, 18, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Tiodorovic-Zivkovic, D.; Zalaudek, I.; Longo, C.; De Pace, B.; Albertini, G.; Argenziano, G. Successful treatment of two invasive squamous cell carcinomas with topical 5% imiquimod cream in elderly patients. Eur. J. Dermatol. 2012, 22, 579–580. [Google Scholar] [CrossRef] [PubMed]
- Dirschka, T.; Schmitz, L.; Bartha, Á. Clinical and histological resolution of invasive squamous cell carcinoma by topical imiquimod 3.75%: A case report. Eur. J. Dermatol. 2016, 26, 408–409. [Google Scholar] [CrossRef]
- Konstantopoulou, M.; Lord, M.G.; Macfarlane, A.W. Treatment of invasive squamous cell carcinoma with 5-percent imiquimod cream. Dermatol. Online J. 2006, 12, 10. [Google Scholar] [CrossRef]
- Leibovitch, I.; Huilgol, S.C.; Selva, D.; Richards, S.; Paver, R. Basal cell carcinoma treated with Mohs surgery in Australia II. Outcome at 5-year follow-up. J. Am. Acad. Dermatol. 2005, 53, 452–457. [Google Scholar] [CrossRef]
- Gulleth, Y.; Goldberg, N.; Silverman, R.P.; Gastman, B.R. What is the best surgical margin for a basal cell carcinoma: A meta-analysis of the literature. Plast. Reconstr. Surg. 2010, 126, 1222–1231. [Google Scholar] [CrossRef]
- Bichakjian, C.K.; Olencki, T.; Aasi, S.Z.; Alam, M.; Andersen, J.S.; Berg, D.; Bowen, G.M.; Cheney, R.T.; Daniels, G.A.; Glass, L.F.; et al. Basal Cell Skin Cancer, Version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2016, 14, 574–597. [Google Scholar] [CrossRef]
- Peris, K.; Fargnoli, M.C.; Garbe, C.; Kaufmann, R.; Bastholt, L.; Seguin, N.B.; Bataille, V.; del Marmol, V.; Dummer, R.; Harwood, C.A.; et al. Diagnosis and treatment of basal cell carcinoma: European consensus–based interdisciplinary guidelines. Eur. J. Cancer 2019, 118, 10–34. [Google Scholar] [CrossRef] [Green Version]
- van der Geer, S.; Ostertag, J.U.; Krekels, G.A.M. Treatment of basal cell carcinomas in patients with nevoid basal cell carcinoma syndrome. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Mitropoulos, P.; Norman, R. Nevoid basal cell carcinoma syndrome (Gorlin syndrome): Updated review of minimally invasive treatments. Cutis 2008, 81, 53–60. [Google Scholar]
- McLeod, M.; Choudhary, S.; Giannakakis, G.; Nouri, K. Surgical treatments for lentigo maligna: A review. Dermatol. Surg. 2011, 37, 1210–1228. [Google Scholar] [CrossRef]
- Ellis, L.Z.; Cohen, J.L.; High, W.; Stewart, L. Melanoma in situ treated successfully using imiquimod after nonclearance with surgery: Review of the literature. Dermatol. Surg. 2012, 38, 937–946. [Google Scholar] [CrossRef]
- Hyde, M.A.; Hadley, M.L.; Tristani-Firouzi, P.; Goldgar, D.; Bowen, G.M. A randomized trial of the off-label use of imiquimod, 5%, cream with vs. without tazarotene, 0.1%, gel for the treatment of lentigo maligna, followed by conservative staged excisions. Arch. Dermatol. 2012, 148, 592–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotter, M.A.; McKenna, J.K.; Bowen, G.M. Treatment of lentigo maligna with imiquimod before staged excision. Dermatol. Surg. 2008, 34, 147–151. [Google Scholar] [CrossRef]
- Gilsono, R.; Nugento, D.; Bennetto, K.; Doréo, C.J.; Murrayo, M.L.; Meadowso, J.; Haddowo, L.J.; Laceyo, C.; Sandmanno, F.; Jito, M.; et al. Imiquimod versus podophyllotoxin, with and without human papillomavirus vaccine, for anogenital warts: The hipvac factorial RCT. Health Technol. Assess. (Rockv) 2020, 24, 1–116. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, S.; Monastirli, A.; Pasmatzi, E.; Tsambaos, D. Pyogenic granuloma: Complete remission under occlusive imiquimod 5% cream. Clin. Exp. Dermatol. 2008, 33, 454–456. [Google Scholar] [CrossRef] [PubMed]
- Ghodsi, S.Z.; Raziei, M.; Taheri, A.; Karami, M.; Mansoori, P.; Farnaghi, F. Comparison of cryotherapy and curettage for the treatment of pyogenic granuloma: A randomized trial. Br. J. Dermatol. 2006, 154, 671–675. [Google Scholar] [CrossRef]
- Bassukas, I.D.; Kuhnert, A.; Diepgen, T.L.; Hornstein, O.P. Clinically relevant differences between amelanotic malignant melanoma and granuloma pyogenicum. Dermatologica 1991, 182, 81–84. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor | Type of Study | Number of Patients/ Tumors | Concluded Therapy | Efficacy (Clearance %) | Follow Up (Months) | Reference |
|---|---|---|---|---|---|---|
| Basal cell carcinoma | Retrospective, observational cohort study | 41 | 41 | N/A | [34] | |
| Basal cell carcinoma | Retrospective, case series | 13/21 | 13 | 20/21 (95%) | 18–24 | [35] |
| Basal cell carcinoma | Prospective, randomized, open-label, two arm study comparing 5 weeks daily imiquimod with cryosurgery at Day 0 (“cryoimmunosurgery”) vs. Day 14 (“immunocryosurgery”) (NCT01212549) | 14/17 | 12/14 | Study interrupted at interim analysis | [3] | |
| Basal cell carcinoma | Extended/repeated immunocryosurgery cycles with bevacizumab as an add-in adjuvant for large (>2 cm diameter), multifocal relapses after surgery, relapses after standard immunocryosurgery | 7/7 | 7 | 3/7 (43%) | 18–48 | [26] |
| Basal cell carcinoma | Phase III, prospective, interventional, single-arm evaluating a 5-week cycle of immunocryosurgery in non-superficial BCC with diameter ≤2 cm (NCT01212562) | 83/124 | 79 | With repeat immunocryosurgery cycles effectiveness reached 97.1 ± 1.6% per protocol or 93.2 ± 2.3% per intention to treat analysis | >5 years | [4,5] |
| Basal cell carcinoma | 24/36 | 24 | 35/36 (97.2%) tumor sites, 5 tumors required repeat cryosurgery/immunocryosurgery at one month follow-up | 3–24 | [31] | |
| Basal cell carcinoma (periocular) | Case-series | 16/16 | 16 | 13/16 (81%) | 3–60 | [28,29] |
| Basal cell carcinoma (periocular) | Case | 1 | 1 | Clearance | 12 | [36] |
| Basal cell carcinoma | Case of neglected BCC | 1 | 1 | 1/1 | 24 | [33] |
| Basal cell carcinoma | Cases | 2/17 | 2 | Clearance | 18–24 | [37] |
| Bowen’s disease | Case series | 8/11 | 8 | 11 (100%) | 6–24 | [38] |
| Bowen’s disease | Case series | 21/24 | 21 | 22/24 (91.7%) | 6–60 | [6] |
| Bowen’s disease | Case | 1/1 | 1 | 1/1 | 12 | [39] |
| Squamous cell carcinoma | Case series | 4/8 | 4 | 6/8 (75%) | 12 | [10] |
| Lentigo Maligna | Case | 1/1 | 1 | 1/1 | 26 | [1] |
| Lentigo Maligna | Cases | 2/2 | 2 | 1/2 (50%) | 15–18 | [40] |
| Lentigo Maligna | Cases | 3/3 | 3 | 3/3 (100%) | 41–48 | [9] |
| Lentigo Maligna | Case | 1/1 | 1 | 1/1 | 48 | [41] |
| Lentigo Maligna | Case | 1/1 | 1 | 1/1 | 21 | [42] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaitanis, G.; Bassukas, I.D. A Review of Immunocryosurgery and a Practical Guide to Its Applications. Diseases 2021, 9, 71. https://doi.org/10.3390/diseases9040071
Gaitanis G, Bassukas ID. A Review of Immunocryosurgery and a Practical Guide to Its Applications. Diseases. 2021; 9(4):71. https://doi.org/10.3390/diseases9040071
Chicago/Turabian StyleGaitanis, Georgios, and Ioannis D. Bassukas. 2021. "A Review of Immunocryosurgery and a Practical Guide to Its Applications" Diseases 9, no. 4: 71. https://doi.org/10.3390/diseases9040071
APA StyleGaitanis, G., & Bassukas, I. D. (2021). A Review of Immunocryosurgery and a Practical Guide to Its Applications. Diseases, 9(4), 71. https://doi.org/10.3390/diseases9040071