
Evaluation of Rational Drug Use for Acute Pharyngitis Associated with the Incidence and Prevalence of the Disease at Two Community Health Centers in Indonesia

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1 Causes of Acute Pharyngitis Based on the Centor Criteria
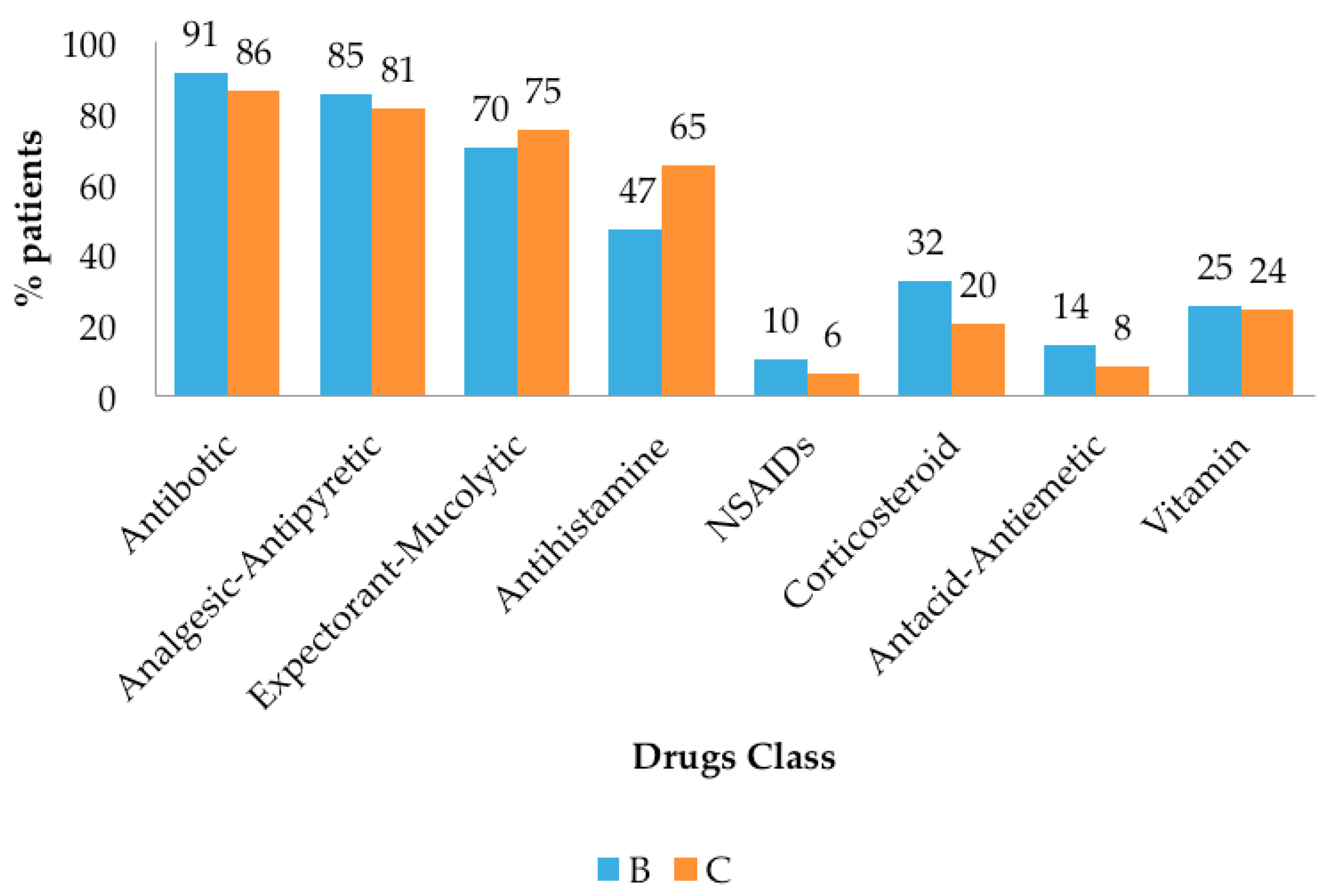
3.2 Drug Use Evaluation
3.3 Incidence and Prevalence Calculation
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pedoman Pengendalian Infeksi Saluran Nafas Akut: Direktorat Jenderal Pengendalian Penyakit dan Penyehatan Lingkungan; Kementrian Kesehatan Republik Indonesia: Jakarta, Indonesia, 2012.
- Riset Kesehatan Dasar 2013; Badan Penelitian dan Pengembangan Kesehatan; Kementrian Kesehatan Republik Indonesia: Jakarta, Indonesia, 2013.
- Shaikh, N.; Leonard, E.; Martin, J.M. Prevalence of streptococcal pharyngitis and streptococcal carriage in children: A meta-analysis. Pediatrics 2010, 126, e557–e564. [Google Scholar] [CrossRef] [PubMed]
- Vincent, M.T.; Celestin, N.; Hussain, A.N. Pharyngitis. Am. Fam. Physician 2004, 69, 1465–1470. [Google Scholar] [PubMed]
- Snow, V.; Mottur-Pilson, C.; Cooper, R.J.; Hoffman, J.R. Principles of appropriate antibiotic use for acute pharyngitis in adults. Ann. Intern. Med. 2001, 134, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Profil Kesehatan Indonesia 2004: Menuju Indonesia Sehat 2010; Departemen Kesehatan Republik Indonesia; Kementrian Kesehatan Republik Indonesia: Jakarta, Indonesia, 2006.
- Peraturan Menteri Kesehatan RI, No.5 Tahun 2014 Tentang Panduan Praktik Klinik Bagi Dokter di Fasilitas Pelayanan Kesehatan Primer; Departemen Kesehatan Republik Indonesia: Jakarta, Indonesia, 2014.
- The Pursuit of Responsible Use of Medicines: Sharing and Learning from Country Experiences. Available online: http://www.who.int/medicines/areas/rational_use/en/ (accessed on 26 November 2015).
- Laporan Kegiatan Subdit Penggunaan Obat Rasional Tahun 2014; Direktorat Jenderal Bina Kefarmasian dan Alat Kesehatan: Jakarta, Indonesia, 2014.
- Modul Penggunaan Obat Rasional di Indonesia; Kementrian Kesehatan Republik Indonesia: Jakarta, Indonesia, 2011.
- Strom, B.L.; Kimmel, S.H. Textbook of Pharmacoepidemiology, 5th ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2006; pp. 71–74. [Google Scholar]
- Epidemiology: A Tool for The Assessment Risk. Available online: http://www.who.int/water_sanitation_health/dwq/iwachap7.pdf (accessed on 26 November 2016).
- Orofino, D.H.; Passos, S.R.; Andrade, C.A.; Nigri, D.; dos Santos Werneck, L.; de Oliveira, R.C.; Hökerberg, Y.H. Accuracy and interobserver variation of three clinical decision rules for the diagnosis of streptococcal pharyngitis. Pediatr. Infect. Dis. J. 2013, 32, 686–687. [Google Scholar] [CrossRef] [PubMed]
- Pelluchi, C.; Grigoryan, L.; Galeone, C.; Esposito, S.; Huovinen, P.; Little, P. Guideline for the management of acute sore throat; ESCMID Sore Throat Guideline Group. Clin. Microbiol. Infect. 2012, 18 (Suppl. 1), 1–28. [Google Scholar] [CrossRef] [PubMed]
- Centor, R.M.; Witherspoon, J.M.; Dalton, H.P.; Brody, C.E.; Link, K. The diagnosis of strep throat in adults in the emergency room. Med. Decis. Mak. 1981, 1, 239–246. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, W.J.; McIsaac, W.; Goel, V.; To, T.; Low, D.E. The validity of a sore throat score in family practice. CMAJ 2000, 163, 811–815. [Google Scholar] [PubMed]
- Fine, A.M.; Nizet, V.; Mandl, K.D. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch. Intern. Med. 2012, 172, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.J.; Hoffman, J.R.; Bartlett, J.G.; for the American Academy of Family Physicians; American College of Physicians; American Society of Internal Medicine; Centers for Disease Control and Prevention. Principles of appropriate antibiotic use for acute pharyngitis in adults: Background. Ann. Intern. Med. 2001, 134, 509–517. [Google Scholar] [PubMed]
- American Academy of Pediatrics; Committee on Infectious Diseases. Red Book, 26th ed.; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2003; pp. 578–580. [Google Scholar]
- Dajani, A.; Taubert, K.; Ferrieri, P.; Peter, G.; Shulman, S. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: A statement for health professionals. Committee on Rheumatic Fever; Endocarditis; and Kawasaki Disease of the Council on Cardiovascular Disease in the Young; the American Heart Association. Pediatrics 1995, 96, 758–764. [Google Scholar] [PubMed]
- Bisno, A.L.; Gerber, M.A.; Gwaltney, J.M, Jr.; Kaplan, E.L.; Schwartz, R.H.; for the Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Clin. Infect. Dis. 2002, 35, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Rimoin, A.W.; Hamza, H.S.; Vince, A. Evaluation of the WHO clinical decision rule for streptococcal pharyngitis. Arch. Dis. Child. 2005, 90, 1066–1070. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.A.; Baltimor, R.S.; Eaton, C.B.; Gewitz, M.; Rowley, A.H.; Shulman, S.T.; Taubert, K.A. Prevention of rheumatic fever and diagnosis and treatment of acute streptococcal pharyngitis: A scientific statement from the American Heart Association Rheumatic Fever; Endocarditis; and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young; the Interdisciplinary Council on Functional Genomics and Translational Biology; and the Interdisciplinary Council on Quality of Care and Outcomes Research: Endorsed by the American Academy of Pediatrics. Circulation 2009, 119, 1541–1551. [Google Scholar] [PubMed]
- Hickerson, A.D.; Carson, C.C. The treatment of urinary tract infections and use of ciprofloxacin extended release. Expert Opin. Investig. Drugs 2006, 15, 519–532. [Google Scholar] [CrossRef] [PubMed]
- Gleadhill, I.C.; Ferguson, W.P.; Lowry, R.C. Efficacy and safety of ciprofloxacin in patients with respiratory infections in comparison with amoxycillin. J. Antimicrob. Chemother 1986, Suppl D, 133–138. [Google Scholar] [CrossRef]
- Duerink, D.O.; Lestari, E.S.; Hadi, U.; Nagelkerke, N.J.; Severin, J.A.; Verbrugh, H.A.; Keuter, M.; Gyssens, I.C.; van den Broek, P.J. Determinants of carriage of resistant Escherichia coli in the Indonesian population inside and outside hospitals. J. Antimicrob. Chemother. 2007, 60, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Anjos, L.M.M.; Marcondes, M.B.; Lima, M.F. Review article: Streptococcal acute pharyngitis. Rev. Soc. Bras. Med. Trop. 2014, 47, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Altamimi, S.; Khalil, A.; Khalaiwi, K.A. Short versus standard duration antibiotic therapy for acute streptococcal pharyngitis in children. Cochrane Database Syst. Rev. 2009, 1, CD004872. [Google Scholar]
- Falagas, M.E.; Vouloumanou, E.K.; Matthaiou, D.K. Effectiveness and safety of short-course vs long-course antibiotic therapy for group A β-hemolytic streptococcal tonsillopharyngitis: A meta-analysis of randomized trials. Mayo Clin. Proc. 2008, 83, 880–889. [Google Scholar] [CrossRef]
- Casey, J.R.; Pichichero, M.E. Metaanalysis of short course antibiotic treatment for group A streptococcal tonsillopharyngitis. Pediatr. Infect. Dis. J. 2005, 24, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Bergeso, K.; Rogers, N.; Shailendra, P. Corticosteroids for a sore throat? J. Fam. Pract. 2013, 62, 372–374. [Google Scholar]
- Shulman, S.T.; Bisno, A.L.; Clegg, H.W. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by The Infectious Diseases Aociety of America. Clin. Infect. Dis. 2012, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Peraturan Menteri Kesehatan RI, No. 35 Tahun 2014: Standar Pelayanan Kefarmasian di Apotek; Departemen Kesehatan Republik Indonesia: Jakarta, Indonesia, 2014.



{kind=link}
{kind=link}
| Centor | Risk of Streptococcus Infection | Health Center in Bandung | Health Center in Cimahi |
|---|---|---|---|
| ∑ Patients (%) | ∑ Patients (%) | ||
| ≤0 | 1–2.5% | 209 (25.30) | 161 (19.68) |
| 1 | 5–10% | 202 (24.46) | 268 (32.76) |
| 2 | 11–17% | 437 (52.91) | 424 (51.83) |
| 3 | 28–35% | 213 (25.79) | 121 (14.79) |
| ≥4 | 51–53% | 19 (2.30) | 3 (4.03) |
| Total patients | 826 | 818 |
| Etiology | One Health Center in Bandung | One Health Center in Cimahi |
|---|---|---|
| ∑ Patients (%) | ∑ Patients (%) | |
| Bacteria | 136 (16.52) | 90 (11.00) |
| Virus | 564 (68.53) | 615 (75.18) |
| Cannot be determined | 123 (14.95) | 113 (13.81) |
| Total patients | 826 | 818 |
| Criteria | Antibiotic Therapy (∑ Patients, %) | Corticosteroid Therapy * ∑ Patients (%) | |
|---|---|---|---|
| Health Center in Bandung | Health Center in Cimahi | ||
| Inappropriate indication | 627 (83.82) | 639 (91.29) | x |
| Inappropriate drug selection | 10 (1.34) | 3 (0.43) | x |
| Inappropriate dosage | x | x | 55 (15.19) |
| Inappropriate route of administration | x | x | x |
| Inappropriate intervals of administration | x | x | 134 (37.02) |
| Inappropriate duration of administration | 109 (90.08) | 54 (88.52) | 37 (10.22) |
| Inappropriate assessment of the patient’s condition | x | x | x |
| Score Centor | Outcome Therapy | ||||
|---|---|---|---|---|---|
| Improved | Unimproved | ||||
| ≤3 days | 4–6 days | ≥7 days | Persistent | Worsen | |
| Antibiotic | 29 | 10 | 2 | 28 | 3 |
| Without Antibiotic | 1 | 1 | 0 | 2 | 1 |
| Total | 30 | 11 | 2 | 30 | 4 |
| Adverse Effect | Incidence (%) |
|---|---|
| Dizziness | 1 (12.5) |
| Headache | 3 (37.5) |
| Weakness | 1 (12.5) |
| Stiffness | 1 (12.5) |
| Shoulder pain | 1 (12.5) |
| Heartburn | 1 (12.5) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuniar, C.T.; Anggadiredja, K.; Islamiyah, A.N. Evaluation of Rational Drug Use for Acute Pharyngitis Associated with the Incidence and Prevalence of the Disease at Two Community Health Centers in Indonesia. Sci. Pharm. 2017, 85, 22. https://doi.org/10.3390/scipharm85020022
Yuniar CT, Anggadiredja K, Islamiyah AN. Evaluation of Rational Drug Use for Acute Pharyngitis Associated with the Incidence and Prevalence of the Disease at Two Community Health Centers in Indonesia. Scientia Pharmaceutica. 2017; 85(2):22. https://doi.org/10.3390/scipharm85020022
Chicago/Turabian StyleYuniar, Cindra T., Kusnandar Anggadiredja, and Alfi N. Islamiyah. 2017. "Evaluation of Rational Drug Use for Acute Pharyngitis Associated with the Incidence and Prevalence of the Disease at Two Community Health Centers in Indonesia" Scientia Pharmaceutica 85, no. 2: 22. https://doi.org/10.3390/scipharm85020022
APA StyleYuniar, C. T., Anggadiredja, K., & Islamiyah, A. N. (2017). Evaluation of Rational Drug Use for Acute Pharyngitis Associated with the Incidence and Prevalence of the Disease at Two Community Health Centers in Indonesia. Scientia Pharmaceutica, 85(2), 22. https://doi.org/10.3390/scipharm85020022