
Compounding in Ukraine: Assessment of the Risks for the Ointment’s Quality by the FMECA Method


 , ,
, ,
Abstract
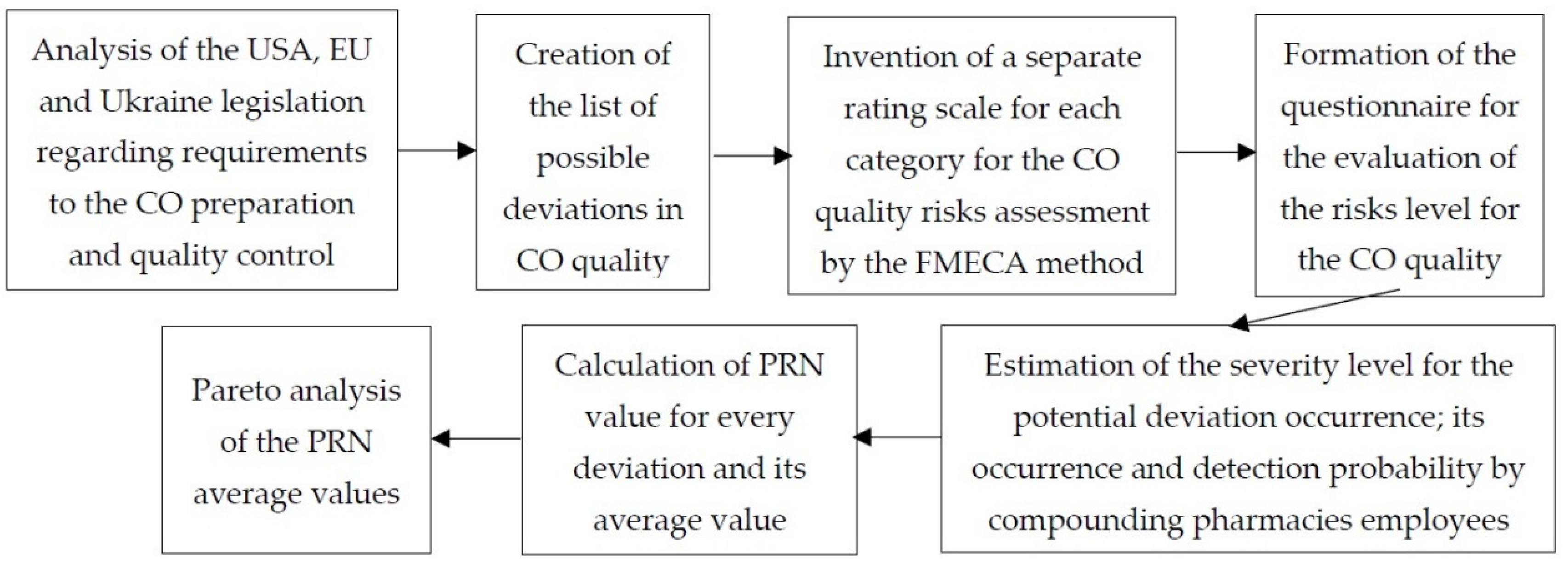
:1. Introduction
2. Results
- ✓
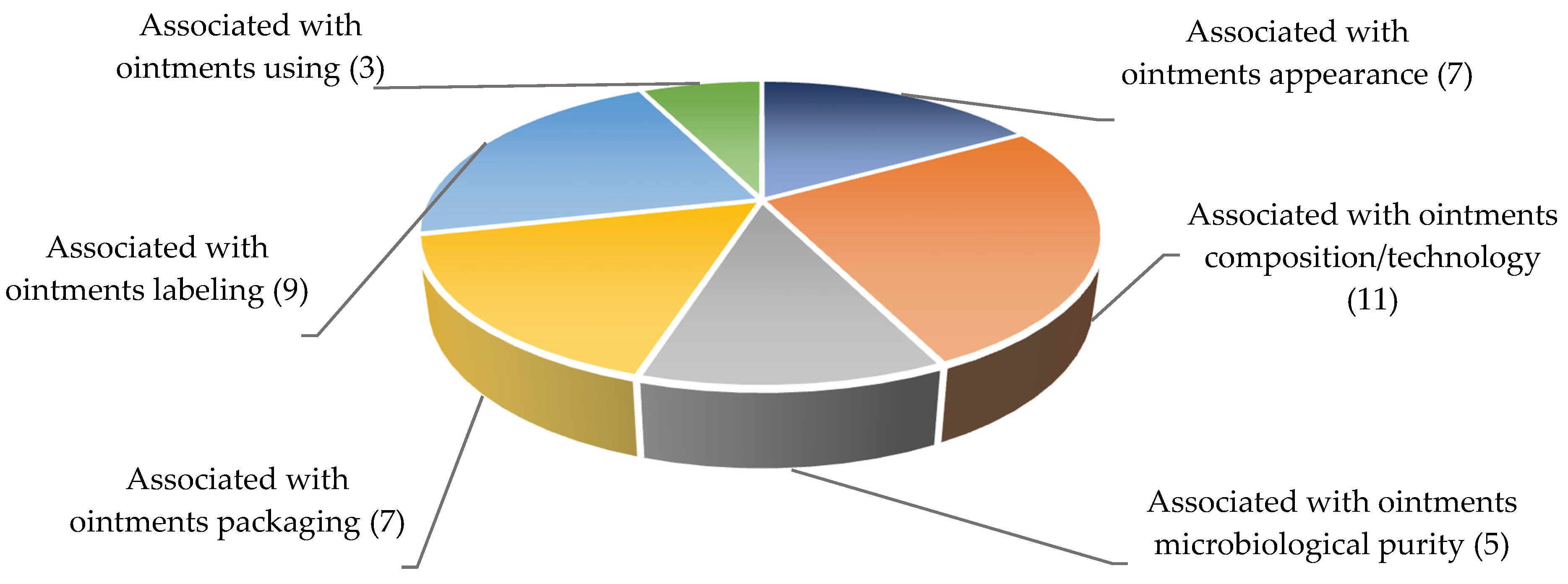
- defects associated with ointments appearance;
- ✓
- defects associated with ointments composition/technology;
- ✓
- defects associated with ointments microbiological purity;
- ✓
- defects associated with ointments packaging;
- ✓
- defects associated with ointments labeling;
- ✓
- defects associated with ointments usage.
- ✓
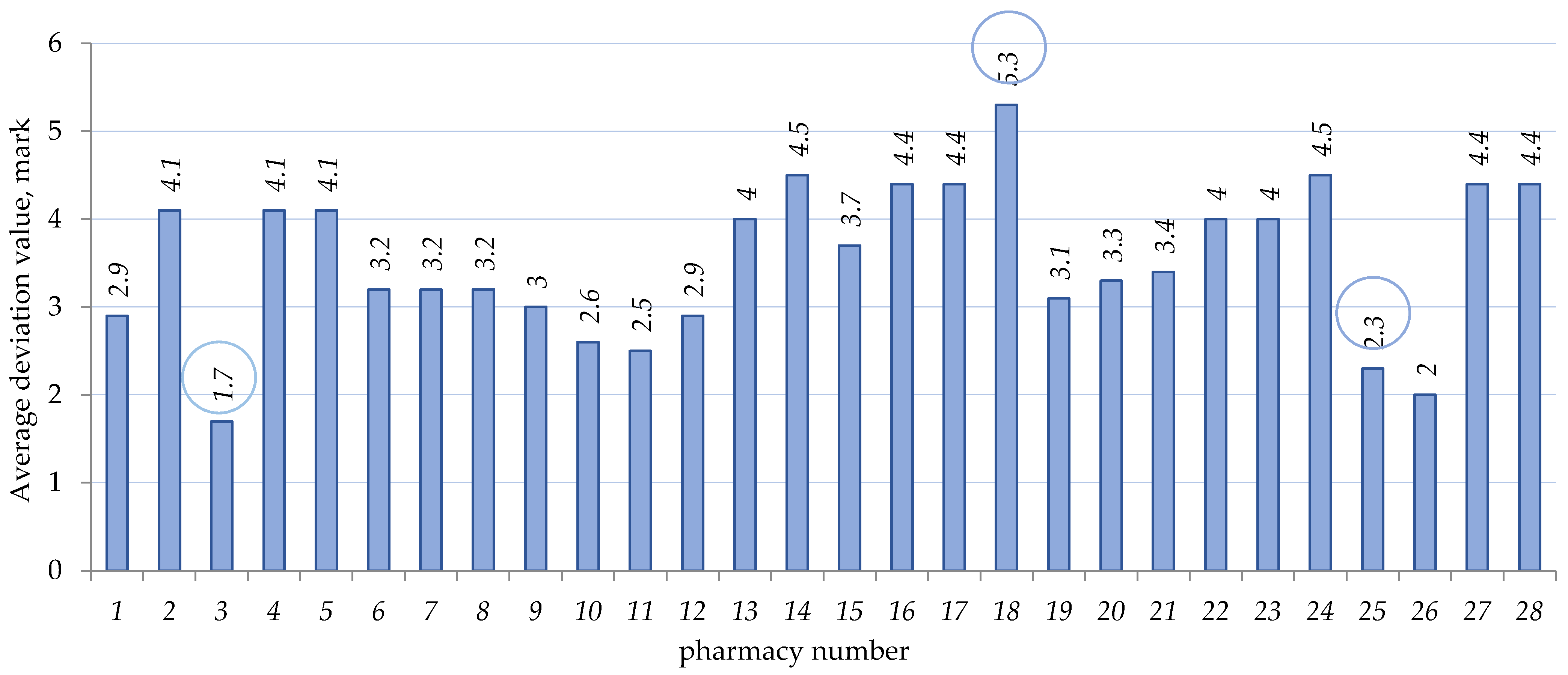
- severity of potential deviation occurrence—5.5 points;
- ✓
- occurrence probability—2.0 points;
- ✓
- detection probability—3.1 points.
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siamidi, A.; Pippa, N.; Demetzos, C. Pharmaceutical compounding: Recent advances, lessons learned and future perspectives. Glob. Drugs Ther. 2017, 2, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Selam, M.N.; Ababu, A. Extemporaneous compounding practice for dermatologic preparations in Ethiopian public hospitals: Regulatory requirements and quality concerns. Risk Manag. Healthc. Policy 2021, 14, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Mohiuddin, A.K. Extemporaneous compounding: Cautions, controversies and convenience. Innov. J. Med. Health Sci. 2019, 9, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Yevtifeeva, O.A. Analytical review of the quality assurance system of extemporaneous medicines in the world developed countries. News Pharm. 2013, 1, 9–18. [Google Scholar]
- European Pharmacopoeia, 10th ed.; European Directorate for the Quality of Medicines: Strasbourg, France, 2020; Available online: https://www.edqm.eu/en/european_pharmacopoeia_10th_edition (accessed on 15 January 2022).
- State Pharmacopoeia of Ukraine, 2nd ed.; Ukrainian Scientific Pharmacopoeial Center for Quality of Medicines: Kharkiv, Ukraine, 2015; Volume 1.
- Pharmaceutical Inspection Co-operation Scheme. Guide to Good Practices for The Preparation of Medicinal Products in Healthcare Establishments: PE 010-4. 2014. Available online: https://picscheme.org/docview/3443 (accessed on 15 January 2022).
- USP Compounding: A Guide for the Compounding Practitioner; The United States Pharmacopoeial Convention: Rockville, MD, USA, 2020.
- Resolution CM/Res (2016)1 on Quality and Safety Assurance Requirements for Medicinal Products Prepared in Pharmacies for the Special Needs of Patients; European Directorate for the Quality of Medicines: Strasbourg, France, 2016; Available online: https://www.edqm.eu/sites/default/files/resolution_cm_res_2016_1_quality_and_safety_assurance_requirements_for_medicinal_products_prepared_in_pharmacies.pdf (accessed on 15 January 2022).
- Therapeutic Goods Administration. Guide to the Interpretation of the PIC/S Guide to GMP for Compounded Medicinal Products: Compounded Medicines and Good Manufacturing Practice (GMP); Ver. 2.0; Australia. 2017. Available online: https://www.tga.gov.au/sites/default/files/compounded-medicines-and-good-manufacturing-practice-gmp.pdf (accessed on 15 January 2022).
- Zdoryk, O.A. Quality assurance strategy of pharmacy compounded drugs. Pharm. J. 2019, 2, 66–72. [Google Scholar] [CrossRef]
- Allen, L.V. Basics of compounding: Implementing United States Pharmacopeia chapter <1163> Quality assurance in pharmaceutical compounding. Part 1. Int. J. Pharm. Compd. 2012, 16, 146–150. [Google Scholar]
- Allen, L.V. Basics of compounding: Implementing United States Pharmacopeia chapter <1163> Quality assurance in pharmaceutical compounding. Part 2: Documentation and verification. Int. J. Pharm. Compd. 2012, 16, 230–234. [Google Scholar]
- Allen, L.V. Basics of compounding: Implementing United States Pharmacopeia chapter <1163> Quality assurance in pharmaceutical compounding. Part 3: Testing. Int. J. Pharm. Compd. 2012, 16, 322–328. [Google Scholar]
- Allen, L.V. Basics of compounding: Implementing United States Pharmacopeia chapter <1163> Quality assurance in pharmaceutical compounding. Part 4: Cleaning and packaging. Int. J. Pharm. Compd. 2012, 16, 405–414. [Google Scholar]
- Allen, L.V. Basics of compounding: Implementing United States Pharmacopeia chapter <1163> Quality assurance in pharmaceutical compounding. Part 5: Outsourcing and responsible personnel. Int. J. Pharm. Compd. 2012, 16, 490–496. [Google Scholar]
- Timko, R.J. Applying quality by design concepts to pharmacy compounding. Int. J. Pharm. Compd. 2015, 19, 453–463. [Google Scholar]
- Preventing Risks Involved with Compounding Medication. Available online: https://www.healthstream.com/resource/blog/preventing-risks-involved-with-compounding-medication (accessed on 15 January 2022).
- Jackson, M.; Lowey, A. Risk management. In Handbook of Extemporaneous Preparation: A Guide to Pharmaceutical Compounding, 1st ed.; Jackson, M., Lowey, A., Eds.; Pharmaceutical Press: London, UK, 2010; pp. 11–23. [Google Scholar]
- Dooms, M.; Carvalho, M. Compounded medication for patients with rare diseases. Orphanet J. Rare Dis. 2018, 13, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheepers, H.P.; Langedijk, J.; Handlos, V.N.; Walser, S.; Schutjens, M.H.; Neef, C. Legislation on the preparation of medicinal products in European pharmacies and the Council of Europe Resolution. Eur. J. Hosp. Pharm. 2017, 24, 224–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheepers, H.P.A.; Handlos, V.N.; Walser, S.; Schutjens, M.D.B.; Neef, C. Impact of the Council of Europe Resolution on quality and safety assurance requirements for medicinal products prepared in pharmacies for the special needs of patients. Eur. J. Hosp. Pharm. 2016, 24, 224–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Conference on Harmonization (ICH) of technical requirements for registration of pharmaceuticals for human use. In ICH Guideline Q9 on Quality Risk Management (EMA/CHMP/ICH/24235/2006); ICH: Geneva, Switzerland, 2015.
- Lambert, A. USP 797: A Breakdown of Low, Medium and High Compounding Risks. Available online: https://www.wolterskluwer.com/en/expert-insights/usp-797-a-breakdown-of-low-medium-and-high-risks (accessed on 15 January 2022).
- Royer, M.; Libessart, M.; Dubaele, J.-M.; Tourneux, P.; Marcon, F. Controlling risks in the compounding process of individually formulated parenteral nutrition: Use of the FMECA method (Failure modes, effects, and criticality analysis). Pharm. Technol. Hosp. Pharm. 2019, 4, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Dozias, G.; Thiec, J.; Le Den, G.; Cogulet, V. Risks associated with the evolution in the compounding process of parenteral nutrition solutions: Use of the “FMECA” method. Pharm. Technol. Hosp. Pharm. 2021, 6, 1–6. [Google Scholar] [CrossRef]
- Boulé, M.; Lachapelle, S.; Collin-Lévesque, L.; Demers, E.; Nguyen, C.; Fournier-Tondreau, M.; Thibault, M.; Lebel, D.; Bussières, J.-F. Failure mode, effect, and criticality analysis of the parenteral nutrition process in a mother-child hospital: The AMELIORE study. Nutr. Clin. Pract. 2018, 33, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Bonnabry, P.; Cingria, L.; Sadeghipour, F.; Ing, H.; Fonzo-Christe, C.; Pfister, R.E. Use of a systematic risk analysis method to improve safety in the production of paediatric parenteral nutrition. Qual. Saf. Health Care 2005, 14, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Mourkogianni, E.; Karatza, A.; Vinni, E.; Papadimitriou, E.; Avgoustakis, K.; Panagi, Z. Assessment and optimization of the pediatric parenteral nutrition preparation process in a hospital pharmacy. J. Parenter. Enteral. Nutr. 2020, 44, 928–939. [Google Scholar] [CrossRef]
- Bourika, K.; Koutras, A.; Kalofonos, H.; Vicha, A.; Tsiata, E.; Papadimitriou, E.; Avgoustakis, K.; Panagi, Z. Improvement of chemotherapy solutions production procedure in a hospital central chemotherapy preparation unit: A systematic risk assessment to prevent avoidable harm in cancer patients. Clinical medicine insights. Oncology 2019, 13, 1179554919852933. [Google Scholar] [CrossRef] [Green Version]
- IEC/ISO 31010:2019; Risk Management—Risk Assessment Techniques. European Ed. 2.0; International Electrotechnical Commission: Geneva, Switzerland, 2019.
- Zdoryk, O.A.; Shtrimaitis, O.V.; Georgiyants, V.A. Risk assessment of compounding and quality control of concentrated solutions in pharmacy conditions. News Pharm. 2014, 1, 16–21. [Google Scholar]
- Savchenko, L.; Pidpruzhnykov, Y.; Ivanauskas, L.; Lukosius, A.; Georgiyants, V. Risk assessment for compounding ointments quality by Ishikawa diagram construction. Farmacia 2021, 69, 688–696. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Respondent | Quantity | Specific Weight, % |
|---|---|---|
| Respondent position | ||
| Head of the pharmacy | 5 | 17.87 |
| Deputy of the pharmacy head | 2 | 7.14 |
| Pharmacist | 9 | 32.14 |
| Pharmacist-analyst | 9 | 32.14 |
| Pharmacist assistant | 3 | 10.71 |
| Work experience | ||
| Up to 10 years | 11 | 40.74 |
| 10–20 years | 7 | 25.93 |
| 20–30 years | 6 | 22.22 |
| 30–40 years | 2 | 7.41 |
| 40–50 years | 1 | 3.70 |
| Defect Group | Defects Average Value, Points | PRN Average Value | % PRN from Total PRN |
|---|---|---|---|
| Defects associated with ointments appearance | 3,2 | 153 | 13 |
| Defects associated with ointments composition/technology | 3,6 | 330 | 29 |
| Defects associated with ointments microbiological purity | 4,9 | 266 | 23 |
| Defects associated with ointments packaging | 3,3 | 156 | 13 |
| Defects associated with ointments labeling | 3,0 | 155 | 13 |
| Defects associated with ointments using | 3,7 | 98 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savchenko, L.; Pidpruzhnykov, Y.; Lesyk, R.; Ivanauskas, L.; Kotvitska, A.; Georgiyants, V. Compounding in Ukraine: Assessment of the Risks for the Ointment’s Quality by the FMECA Method. Sci. Pharm. 2022, 90, 25. https://doi.org/10.3390/scipharm90020025
Savchenko L, Pidpruzhnykov Y, Lesyk R, Ivanauskas L, Kotvitska A, Georgiyants V. Compounding in Ukraine: Assessment of the Risks for the Ointment’s Quality by the FMECA Method. Scientia Pharmaceutica. 2022; 90(2):25. https://doi.org/10.3390/scipharm90020025
Chicago/Turabian StyleSavchenko, Lesia, Yuri Pidpruzhnykov, Roman Lesyk, Liudas Ivanauskas, Alla Kotvitska, and Victoriya Georgiyants. 2022. "Compounding in Ukraine: Assessment of the Risks for the Ointment’s Quality by the FMECA Method" Scientia Pharmaceutica 90, no. 2: 25. https://doi.org/10.3390/scipharm90020025
APA StyleSavchenko, L., Pidpruzhnykov, Y., Lesyk, R., Ivanauskas, L., Kotvitska, A., & Georgiyants, V. (2022). Compounding in Ukraine: Assessment of the Risks for the Ointment’s Quality by the FMECA Method. Scientia Pharmaceutica, 90(2), 25. https://doi.org/10.3390/scipharm90020025