Increased Expression of the Leptin Gene in Adipose Tissue of Patients with Chronic Kidney Disease–The Possible Role of an Abnormal Serum Fatty Acid Profile

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
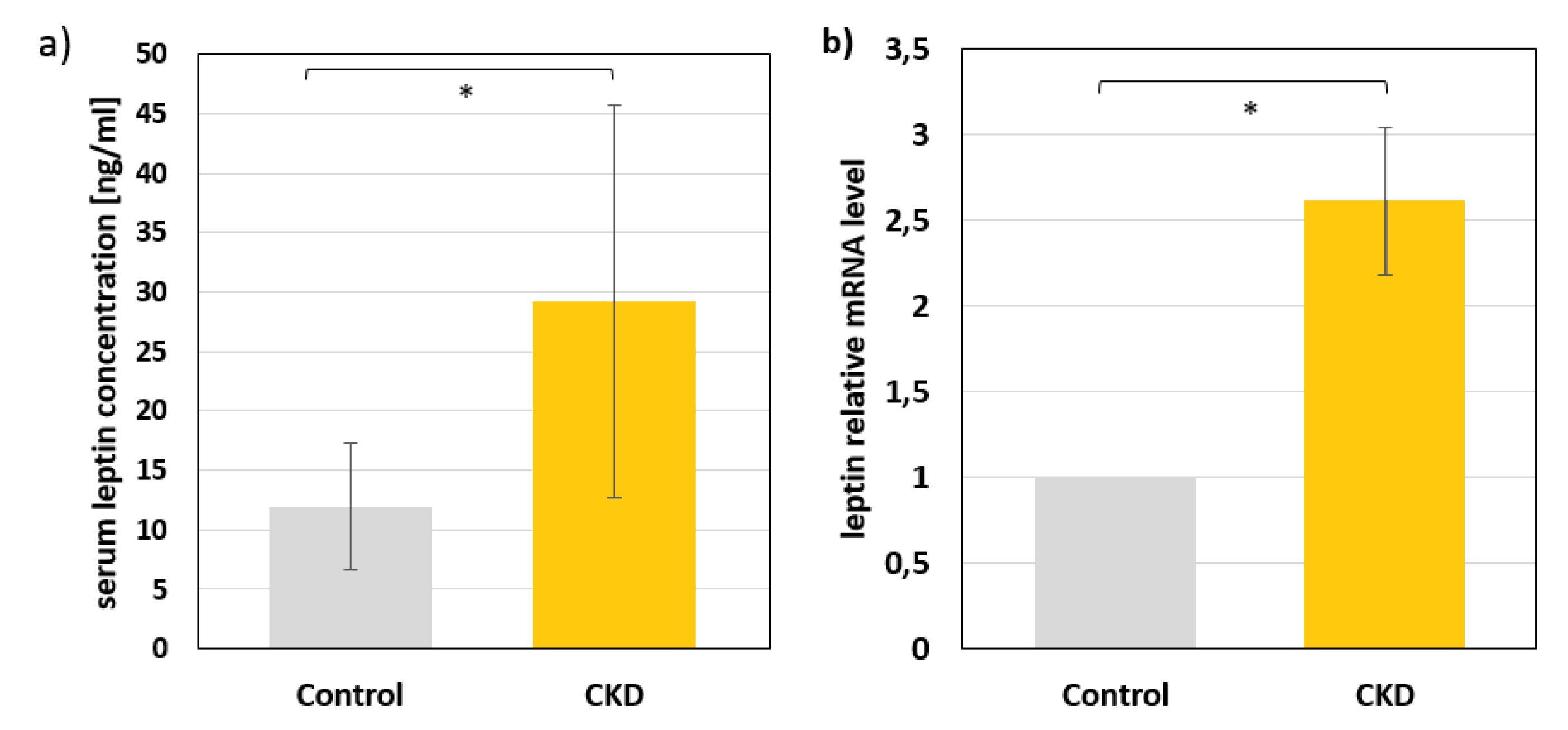
2.1. Leptin Levels in Serum and mRNA Levels in Subcutaneous Adipose Tissue of Study Subjects
2.2. Serum Fatty Acid Profile of Study Subjects
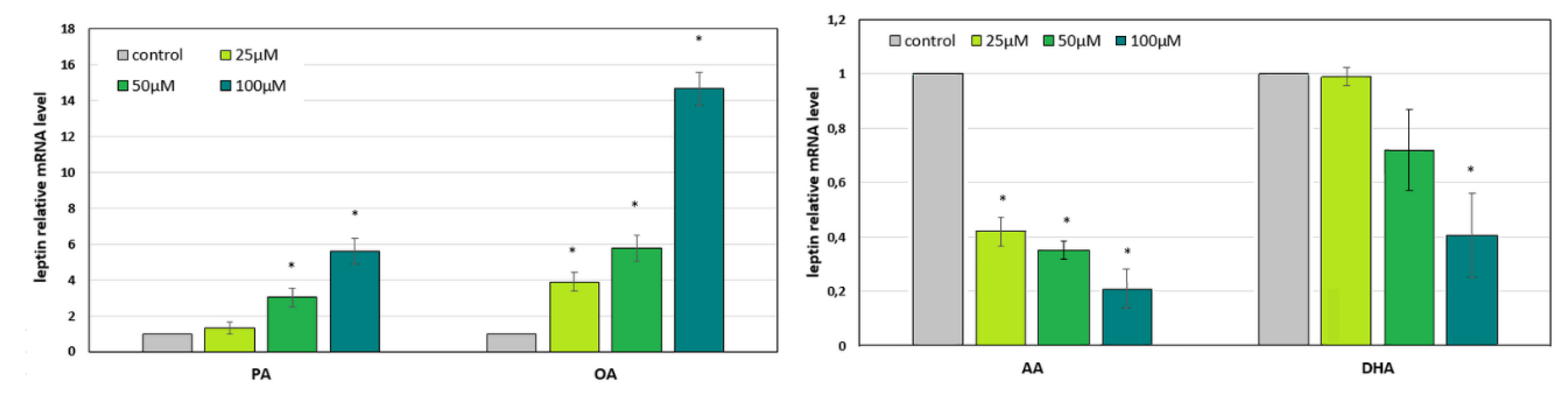
2.3. The Effect of the CKD-Related Abnormal Fatty Acid Profile on the Expression of Leptin in In Vitro Cultured Adipocytes
3. Discussion
4. Materials and Methods
4.1. Study Subjects
4.2. Materials and Reagents
4.3. Serum Leptin Assay
4.4. Serum Fatty Acid Profile Analysis
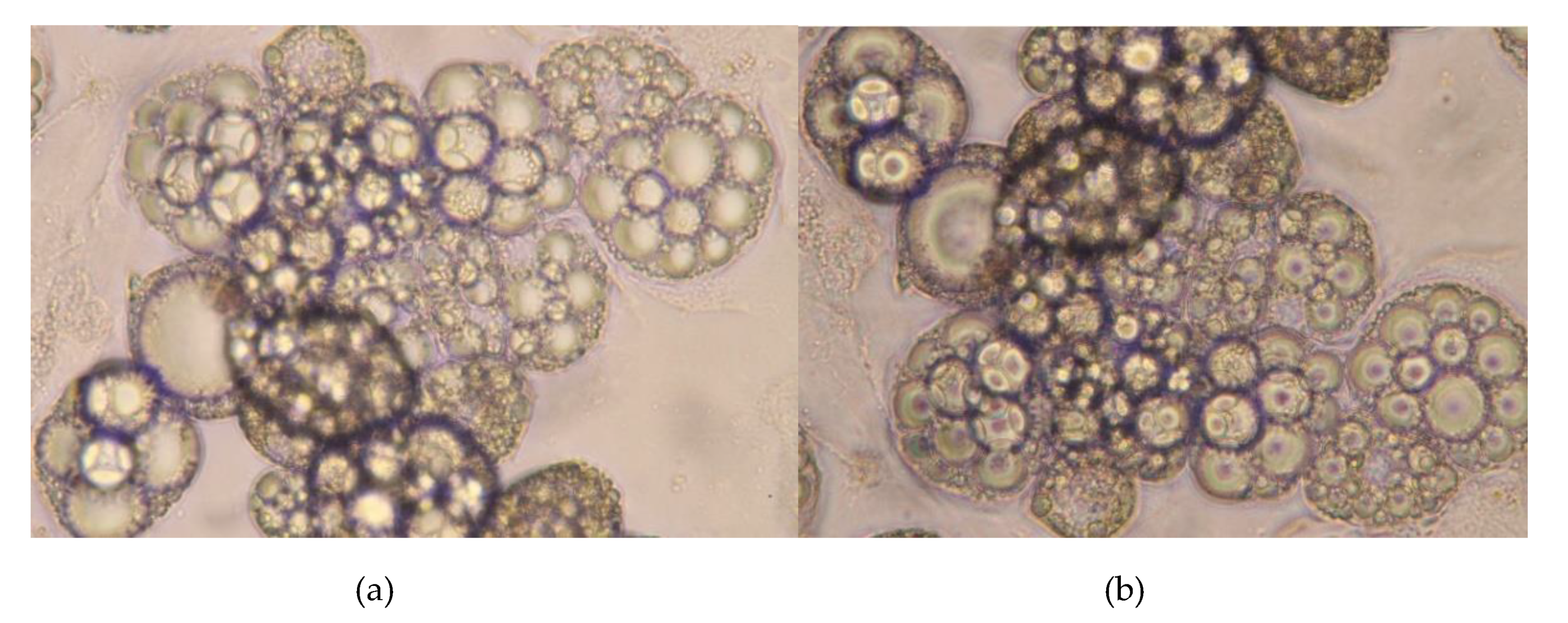
4.5. Adipocyte Culture, Differentiation, and Treatment
4.6. Gene Expression Analyses
4.7. Statistics
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | Arachidonic acid |
| BMI | Body mass index |
| BUN | Blood urea nitrogen |
| CKD | Chronic kidney disease |
| CRP | C-reactive protein |
| CVD | Cardiovascular disease |
| DHA | Docosahexaenoic acid |
| DMEM | Dulbecco‘s modified Eagle‘s medium |
| FA | Fatty acid |
| FAME | Fatty acid methyl esters |
| FBS | Fetal bovine serum |
| GC-MS | Gas chromatography-mass spectrometry |
| HOMA-IR | Homeostatic model assessment of insulin resistance |
| IBMX | 3-isobutyl-1-methylxanthine |
| MUFA | Monounsaturated fatty acid |
| OA | Oleic acid |
| PA | Palmitic acid |
| PUFA | Polyunsaturated fatty acid |
| SAT | Subcutaneous adipose tissue |
| SFA | Saturated fatty acid |
| TC | Total cholesterol |
| TG | Triacylglycerols |
References
- Zdrojewski, Ł.; Zdrojewski, T.; Rutkowski, M.; Bandosz, P.; Król, E.; Wyrzykowski, B.; Rutkowski, B. Prevalence of chronic kidney disease in a representative sample of the Polish population: Results of the NATPOL 2011 survey. Nephrol. Dial. Transplant. 2016, 31, 433–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Zhang, Y.; Youl Hyun, Y.; Ryu, S.; Choi, Y.; Cho, J.; Kwon, M.-J.; Lee, K.-B.; Kim, H.; Jung, H.-S.; et al. Metabolically healthy obesity and development of chronic kidney disease: A cohort study. Ann. Intern. Med. 2016, 164, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Spoto, B.; Pisano, A.; Zoccali, C. Insulin resistance in chronic kidney disease: A systematic review. Am. J. Physiol. Physiol. 2016, 311, F1087–F1108. [Google Scholar] [CrossRef] [Green Version]
- Kovesdy, C.P.; Furth, S.L.; Zoccali, C. Obesity and Kidney Disease: Hidden Consequences of the Epidemic. Am. J. Hypertens. 2017, 30, 328–336. [Google Scholar] [CrossRef]
- Yu, J.Z.; Kalantar-Zadeh, K.; Rhee, C.M. Adiponectin and Leptin in Kidney Disease Patients. In Endocrine Disorders in Kidney Disease; Springer International Publishing: Cham, Switzerland, 2019; pp. 277–290. [Google Scholar]
- Marchelek-Mysliwiec, M.; Wisniewska, M.; Nowosiad-Magda, M.; Safranow, K.; Kwiatkowska, E.; Banach, B.; Dołegowska, B.; Dołegowska, K.; Stepniewska, J.; Domanski, L.; et al. Association Between Plasma Concentration of Klotho Protein, Osteocalcin, Leptin, Adiponectin, and Bone Mineral Density in Patients with Chronic Kidney Disease. Horm. Metab. Res. 2018, 50, 816–821. [Google Scholar] [CrossRef]
- Canpolat, N.; Sever, L.; Agbas, A.; Tasdemir, M.; Oruc, C.; Ekmekci, O.B.; Caliskan, S. Leptin and ghrelin in chronic kidney disease: Their associations with protein-energy wasting. Pediatr. Nephrol. 2018, 33, 2113–2122. [Google Scholar] [CrossRef]
- Noor, S.; Alam, F.; Fatima, S.S.; Khan, M.; Rehman, R. Role of Leptin and dyslipidemia in chronic kidney disease. Pak. J. Pharm. Sci. 2018, 31, 893–897. [Google Scholar]
- Abella, V.; Scotece, M.; Conde, J.; Pino, J.; Gonzalez-Gay, M.A.; Gómez-Reino, J.J.; Mera, A.; Lago, F.; Gómez, R.; Gualillo, O. Leptin in the interplay of inflammation, metabolism and immune system disorders. Nat. Rev. Rheumatol. 2017, 13, 100–109. [Google Scholar] [CrossRef]
- Friedman, J. The long road to leptin. J. Clin. Invest. 2016, 126, 4727–4734. [Google Scholar] [CrossRef] [Green Version]
- Akchurin, O.M.; Kaskel, F. Update on inflammation in chronic kidney disease. Blood Purif. 2015, 39, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.; Liu, B.; Song, J.; Bao, S.; Zhen, J.; Lv, Z.; Wang, R. Leptin promotes endothelial dysfunction in chronic kidney disease through AKT/GSK3β and β-catenin signals. Biochem. Biophys. Res. Commun. 2016, 480, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Mao, S.; Fang, L.; Liu, F.; Jiang, S.; Wu, L.; Zhang, J. Leptin and chronic kidney diseases. J. Recept. Signal Transduct. 2018, 38, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.C.; Teo, B.W.; Tai, E.S.; Lim, S.C.; Chan, C.M.; Sethi, S.; Wong, T.Y.; Sabanayagam, C. Elevated serum leptin, adiponectin and leptin to adiponectin ratio is associated with chronic kidney disease in Asian adults. PLoS ONE 2015, 10, e0122009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czumaj, A.; Śledziński, T.; Carrero, J.-J.; Stepnowski, P.; Sikorska-Wisniewska, M.; Chmielewski, M.; Mika, A. Alterations of fatty acid profile may contribute to dyslipidemia in chronic kidney disease by influencing hepatocyte metabolism. Int. J. Mol. Sci. 2019, 20, 2470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczuko, M.; Kaczkan, M.; Drozd, A.; Maciejewska, D.; Palma, J.; Owczarzak, A.; Marczuk, N.; Rutkowski, P.; Małgorzewicz, S. Comparison of fatty acid profiles in a group of female patients with Chronic Kidney Diseases (CKD) and Metabolic Syndrome (MetS)–similar trends of changes, different pathophysiology. Int. J. Mol. Sci. 2019, 20, 1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madsen, T.; Christensen, J.H.; Svensson, M.; Witt, P.M.; Toft, E.; Schmidt, E.B. Marine n-3 polyunsaturated fatty acids in patients with end-stage renal failure and in subjects without kidney disease: A comparative study. J. Ren. Nutr. 2011, 21, 169–175. [Google Scholar] [CrossRef]
- Hager, M.R.; Narla, A.D.; Tannock, L.R. Dyslipidemia in patients with chronic kidney disease. Rev. Endocr. Metab. Disord. 2017, 18, 29–40. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Žutelija, M.; Mavrinac, V.; Orlic, L. Dyslipidemia in patients with chronic kidney disease: Etiology and management. Int. J. Nephrol. Renovasc. Dis. 2017, 10, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Moradi, H.; Vaziri, N.D. Molecular mechanisms of disorders of lipid metabolism in chronic kidney disease Publication Date. Front. Biosci. 2018, 23, 146–161. [Google Scholar]
- Tsimihodimos, V.; Dounousi, E.; Siamopoulos, K.C. Dyslipidemia in chronic kidney disease: An approach to pathogenesis and treatment. Am. J. Nephrol. 2008, 28, 958–973. [Google Scholar] [CrossRef] [PubMed]
- Hellström, L.; Wahrenberg, H.; Hruska, K.; Reynisdottir, S.; Arner, P. Mechanisms behind gender differences in circulating leptin levels. J. Intern. Med. 2000, 247, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimburger, O.; Lonnqvist, F.; Danielsson, A.; Nordenstrom, J.; Stenvinkel, P. Serum immunoreactive leptin concentration and its relation to the body fat content in chronic renal failure. J. Am. Soc. Nephrol. 1997, 8, 1423–1430. [Google Scholar] [PubMed]
- Merabet, E.; Dagogo-Jack, S.; Coyne, D.W.; Klein, S.; Santiago, J.V.; Hmiel, S.P.; Landt, M. Increased plasma leptin concentration in end-stage renal disease. J. Clin. Endocrinol. Metab. 1997, 82, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Zhang, J.; Yuan, Y.; Zha, X.; Xing, C.; Shen, C.; Shen, Z.; Qin, C.; Zeng, M.; Yang, G.; et al. Association of increased serum leptin with ameliorated anemia and malnutrition in stage 5 chronic kidney disease patients after parathyroidectomy. Sci. Rep. 2016, 6, 27918. [Google Scholar] [CrossRef] [PubMed]
- Daschner, M.; Tönshoff, B.; Blum, W.F.; Englaro, P.; Wingen, A.M.; Schaefer, F.; Wühl, E.; Rascher, W.; Mehls, O. Inappropriate elevation of serum leptin levels in children with chronic renal failure. European Study Group for Nutritional Treatment of Chronic Renal Failure in Childhood. J. Am. Soc. Nephrol. 1998, 9, 1074–1079. [Google Scholar]
- Odamaki, M.; Furuya, R.; Yoneyama, T.; Nishikino, M.; Hibi, I.; Miyaji, K.; Kumagai, H. Association of the serum leptin concentration with weight loss in chronic hemodialysis patients. Am. J. Kidney Dis. 1999, 33, 361–368. [Google Scholar] [CrossRef]
- Diez, J.J.; Iglesias, P.; Fernandez-Reyes, M.J.; Aguilera, A.; Bajo, M.A.; Alvarez-Fidalgo, P.; Codoceo, R.; Selgas, R. Serum concentrations of leptin, adiponectin and resistin, and their relationship with cardiovascular disease in patients with end-stage renal disease. Clin. Endocrinol. 2005, 62, 242–249. [Google Scholar] [CrossRef]
- Ines, M.; Silva, B.; Vale, B.S.; Lemos, C.C.S.; Torres, M.R.S.G.; Bregman, R. Body adiposity index assess body fat with high accuracy in nondialyzed chronic kidney disease patients. Obesity 2013, 21, 546–552. [Google Scholar]
- Frühbeck, G.; Catalán, V.; Rodríguez, A.; Ramírez, B.; Becerril, S.; Salvador, J.; Portincasa, P.; Colina, I.; Gómez-Ambrosi, J. Involvement of the leptin-adiponectin axis in inflammation and oxidative stress in the metabolic syndrome. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Yadav, V.K.; Oury, F.; Suda, N.; Liu, Z.W.; Gao, X.B.; Confavreux, C.; Klemenhagen, K.C.; Tanaka, K.F.; Gingrich, J.A.; Guo, X.E.; et al. A serotonin-dependent mechanism explains the leptin regulation of bone mass, appetite, and energy expenditure. Cell 2009, 138, 976–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordfors, L.; Lönnqvist, F.; Heimbürger, O.; Danielsson, A.; Schalling, M.; Stenvinkel, P. Low leptin gene expression and hyperleptinemia in chronic renal failure. Kidney Int. 1998, 54, 1267–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witasp, A.; Carrero, J.J.; Heimbürger, O.; Lindholm, B.; Hammarqvist, F.; Stenvinkel, P.; Nordfors, L. Increased expression of pro-inflammatory genes in abdominal subcutaneous fat in advanced chronic kidney disease patients. J. Intern. Med. 2011, 269, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.H.M.; Lam, K.S.L.; Xu, A. Heterogeneity of white adipose tissue: Molecular basis and clinical implications. Exp. Mol. Med. 2016, 48, e215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.-H.; Kim, S.-N.; Kwon, H.-J.; Granneman, J.G. Metabolic heterogeneity of activated beige/brite adipocytes in inguinal adipose tissue. Sci. Rep. 2017, 7, 39794. [Google Scholar] [CrossRef] [Green Version]
- Lynes, M.D.; Tseng, Y.-H. Deciphering adipose tissue heterogeneity. Ann. N. Y. Acad. Sci. 2018, 1411, 5–20. [Google Scholar] [CrossRef]
- Kowalska, K.; Olejnik, A.; Rychlik, J.; Grajek, W. Cranberries (Oxycoccus quadripetalus) inhibit lipid metabolism and modulate leptin and adiponectin secretion in 3T3-L1 adipocytes. Food Chem. 2015, 185, 383–388. [Google Scholar] [CrossRef]
- Kuroda, M.; Tominaga, A.; Nakagawa, K.; Nishiguchi, M.; Sebe, M.; Miyatake, Y.; Kitamura, T.; Tsutsumi, R.; Harada, N.; Nakaya, Y.; et al. DNA methylation suppresses leptin gene in 3T3-L1 adipocytes. PLoS ONE 2016, 11, e0160532. [Google Scholar] [CrossRef]
- Tsubai, T.; Noda, Y.; Ito, K.; Nakao, M.; Seino, Y.; Oiso, Y.; Hamada, Y. Insulin elevates leptin secretion and mRNA levels via cyclic AMP in 3T3-L1 adipocytes deprived of glucose. Heliyon 2016, 2, e00194. [Google Scholar] [CrossRef] [Green Version]
- Jenks, M.Z.; Fairfield, H.E.; Johnson, E.C.; Morrison, R.F.; Muday, G.K. Sex steroid hormones regulate leptin transcript accumulation and protein secretion in 3T3-L1 cells. Sci. Rep. 2017, 7, 8232. [Google Scholar] [CrossRef]
- Folch, J.; Lees, M.; SLOANE STANLEY, G.H. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FA | CONTROL | CKD |
|---|---|---|
| 14:0 | 1.16 ± 0.31 | 1.11 ± 0.50 |
| 16:0 | 22.9 ± 1.62 | 24.1 ± 2.10 * |
| 18:0 | 6.96 ± 0.72 | 6.80 ± 0.98 |
| OTHER SFAs | 1.22 ± 0.09 | 1.36 ± 0.09 |
| TOTAL SFAs | 32.3 ± 1.83 | 33.4 ± 3.02 * |
| 14:1 | 0.07 ± 0.02 | 0.05 ± 0.03 |
| 16:1 | 2.81 ± 0.85 | 2.95 ± 0.79 |
| 18:1 | 25.7 ± 3.15 | 28.9 ± 3.63 * |
| OTHER MUFAs | 0.49 ± 0.08 | 0.65 ± 0.11 * |
| TOTAL MUFAs | 29.1 ± 1.08 | 32.6 ± 1.22 * |
| 18:3 n-3 | 0.31 ± 0.11 | 0.20 ± 0.09 * |
| 20:5 n-3 | 0.94 ± 0.60 | 0.61 ± 0.26 * |
| 22:6 n-3 | 1.03 ± 0.43 | 0.83 ± 0.38 * |
| OTHER N-3 PUFAs | 0.37 ± 0.1 | 0.34 ± 0.13 |
| TOTAL N-3 PUFAs | 2.66 ± 1.04 | 1.98 ± 0.71 * |
| 18:2 n-6 | 26.1 ± 3.59 | 22.9 ± 4.79 * |
| 20:4 n-6 | 5.31 ± 1.14 | 4.53 ± 1.31 * |
| OTHER N-6 PUFAs | 1.42 ± 0.34 | 1.10 ± 0.32 |
| TOTAL N-6 PUFAs | 32.8 ± 3.82 | 28.6 ± 5.39 * |
| Parameter | CONTROL | CKD |
|---|---|---|
| AGE (years) | 47 ± 14.9 | 51 ± 13.0 |
| BMI (kg/m2) | 26.0 ± 3.8 | 25.9 ± 4.8 |
| CREATININE (mg/dL) | 0.9 ± 0.2 | 6.15 ± 2.5 * |
| BUN (mg/dL) | 15.1 ± 3.6 | 44.8 ± 25.0 * |
| ALBUMIN (g/L) | 39.5 ± 3.9 | 37.5 ± 4.6 |
| CRP (mg/dL) | 2.1 ± 2.5 | 4.9 ± 6.1 * |
| TG (mg/dL) | 115.6 ± 59.6 | 150.2 ± 73.7 * |
| TC (mg/dL) | 195.9 ± 45.5 | 200.6 ± 48.0 |
| GLUCOSE (mg/dL) | 96.2 ± 20.2 | 102.7 ± 27.8 |
| INSULIN (mU/mL) | 9.4 ± 5.4 | 9.6 ± 6.2 |
| HOMA-IR | 2.35 ± 2.0 | 2.8 ± 2.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korczyńska, J.; Czumaj, A.; Chmielewski, M.; Śledziński, M.; Mika, A.; Śledziński, T. Increased Expression of the Leptin Gene in Adipose Tissue of Patients with Chronic Kidney Disease–The Possible Role of an Abnormal Serum Fatty Acid Profile. Metabolites 2020, 10, 98. https://doi.org/10.3390/metabo10030098
Korczyńska J, Czumaj A, Chmielewski M, Śledziński M, Mika A, Śledziński T. Increased Expression of the Leptin Gene in Adipose Tissue of Patients with Chronic Kidney Disease–The Possible Role of an Abnormal Serum Fatty Acid Profile. Metabolites. 2020; 10(3):98. https://doi.org/10.3390/metabo10030098
Chicago/Turabian StyleKorczyńska, Justyna, Aleksandra Czumaj, Michał Chmielewski, Maciej Śledziński, Adriana Mika, and Tomasz Śledziński. 2020. "Increased Expression of the Leptin Gene in Adipose Tissue of Patients with Chronic Kidney Disease–The Possible Role of an Abnormal Serum Fatty Acid Profile" Metabolites 10, no. 3: 98. https://doi.org/10.3390/metabo10030098
APA StyleKorczyńska, J., Czumaj, A., Chmielewski, M., Śledziński, M., Mika, A., & Śledziński, T. (2020). Increased Expression of the Leptin Gene in Adipose Tissue of Patients with Chronic Kidney Disease–The Possible Role of an Abnormal Serum Fatty Acid Profile. Metabolites, 10(3), 98. https://doi.org/10.3390/metabo10030098