1. Introduction
Psoriasis is one of the most common chronic skin diseases. It is estimated that it affects 2–4% of the worldwide population [
1]. The etiopathogenesis of psoriasis has not been fully understood. It is suspected that genetic factors, as well as autoimmune mechanism are involved, which are additionally modified by environmental factors [
2]. The essence of psoriasis is the hyperproliferation of epidermal cells and parakeratosis, which leads to erythematous-infiltrative, scaly plaques [
3]. Nowadays, psoriasis should be acknowledged as a kind of systemic disease associated or leading to development of many other disorders and shortening the patients’ life expectancy to about 5 years [
4]. Some of the most important comorbidities of psoriasis are undoubtedly metabolic disorders [
5]. Many investigations aimed to study this relationship, some of them with conflicting results, nevertheless majority of research has proved psoriasis to be related with obesity, arterial hypertension, dyslipidemia or diabetes mellitus (DM), and metabolic syndrome (MS) [
5,
6]. To highlight the association between chronic inflammatory condition in psoriasis with metabolic disturbances, even a term called ‘metaflammation’ has been introduced [
7]. Psoriatics are known to have lipid profile aberrations and increased risk of cardiovascular incidences that could result in death [
4,
5]. What is interesting, associations between the severity of psoriatic skin lesions and intensity of these metabolic disorders have been widely proved [
7] and the risk of cardiovascular disease seems to be elevated especially in patients with severe psoriatic skin lesions [
6]. Moreover, some drugs used in the treatment of dyslipidemia or carbohydrate metabolism disorders were also reported to have beneficial impact on psoriatics’ skin condition [
5,
7].
Cholesteryl ester transfer protein (CETP) is a glycoprotein which takes part in intravascular high-density lipoprotein (HDL) metabolism. CETP is involved in transfer of cholesteryl esters chains and triglycerides (TG) between the HDL fraction and the non-HDL fraction (very low-density lipoproteins, VLDL, and low-density lipoproteins, LDL) [
8,
9]. Due to such properties, CETP is considered a proatherogenic protein since it leads to elevation of LDL and decrease of HDL at the same time [
8,
9]. Obviously CETP concentration is increased in subjects with dyslipidemia [
10].
CETP gene in humans is located on chromosome 16 and studies on subjects with
CETP genes polymorphism have showed that persons whose genotypes resulted in CETP inhibition had lower risk of coronary artery disease [
11].
Sortilin (SORT) is a transmembrane, multi-ligand receptor, which is considered among the Vacuolar protein sorting 10 protein (Vps10p) domain receptor family [
9]. SORT probably participates in glucose metabolism and may have influence on DM development [
9,
12]. SORT was also proved to be engaged in regulatory processes of cell proliferation [
13], and due to its associations with p75 neutrophin receptor (P75NTR), is involved in apoptotic processes [
14].
CETP and SORT have been hardly ever studied in psoriatic patients before, so the available data is scarce. Considering psoriasis is a serious medical, social and economic problem [
15], it should be investigated in relevance to compounds that could potentially become markers of psoriasis comorbidities, complications and indicate the choice of therapy. This is why we analyzed the influence of antipsoriatic therapy on investigated markers and their correlations with metaflammation indicators, which could potentially point into their specific use in daily clinical practice. SORT and CETP may perhaps serve as such markers considering their role in metabolic disorders, which are undoubtedly associated with psoriasis.
3. Discussion
Psoriasis is nowadays perceived as a systemic inflammatory condition characterized by many comorbidities. Although plenty of markers of metabolic disorders have been proved to be also significant in psoriasis, further intensive searching for newer ones is still performed. There is no doubt that psoriatics suffer from aberrations in lipid metabolism but the particular alterations in lipid components sometimes differ between the studies, which makes it difficult to interpret in context of pointing a universal biomarker [
16]. Considering the increased risk of cardiovascular complications and death in psoriatics, as well as complications associated with long-time antipsoriatic therapy, we decided to explore the role of CETP and SORT in psoriatic patients with hope for interesting findings that could be further investigated for potential use in daily clinical practice. Noteworthy, the data on these molecules in psoriatics are very limited, hence it is not an easy task to analyze our results and draw adequate conclusions. Nevertheless, we are one of the first to report information of possible role of CETP and SORT in such patients, which might initiate further research. As far as we are concerned, they have never been studied in other skin diseases, except for one newest paper by Waśkiel-Burnat et al. where SORT has been investigated in subjects with alopecia areata [
17].
We managed to find one study which evaluated serum CETP concentration in psoriatics. Torkhovskaia et al. interestingly found decreased serum CETP level and concluded that there are alterations in reverse cholesterol transport in psoriasis, which may affect cell supply with cholesterol and cells proliferation in consequence [
18]. Indeed, research show that inflammatory condition, including psoriasis, may lead to changes in lipoprotein metabolism and reverse cholesterol transport pathway [
16]. Therefore, although CETP is a known marker of dyslipidemia and its elevated concentrations are observed in such individuals, and although psoriatics are also in increased risk of this disorder, CETP status in such patients may not be easy to establish. We surprisingly did not observe significantly higher CETP concentration in patients comparing to controls. Perhaps other confounders or modifiers take part in that interplay. The role of CETP is still not completely clear because it is suspected that it may also have other nonlipid transfer properties [
11], so its true role in psoriasis is yet to be discovered and may be much more complex. We also need to keep in mind the limitation of our study which is small number of subjects involved.
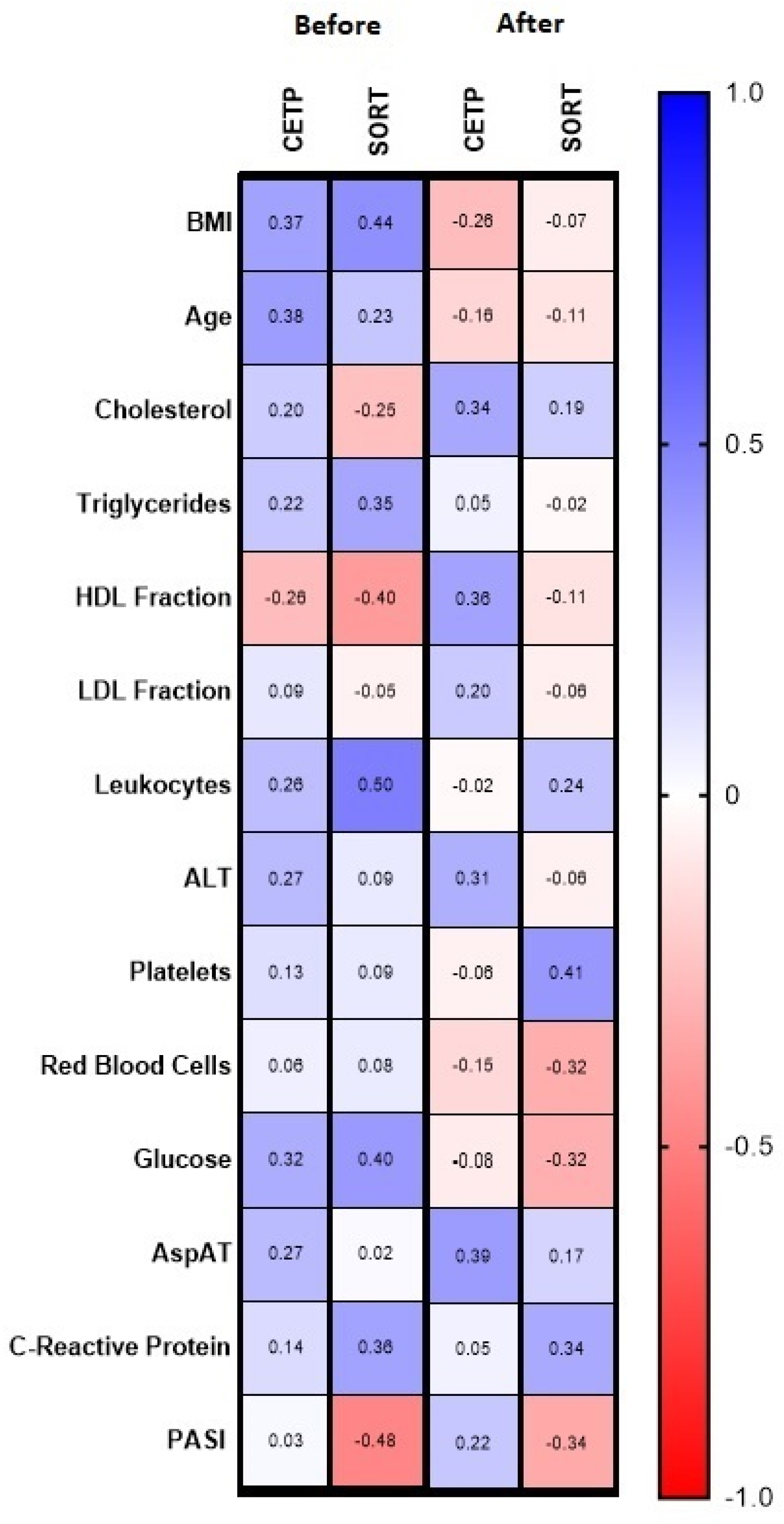
We did not observe any correlation between the psoriasis severity and CETP concentration, but we managed to find a positive correlation with age. Before the administered treatment we did not notice any significant correlations of CETP with laboratory parameters. However, within the subgroups on certain drugs some relations were noted.
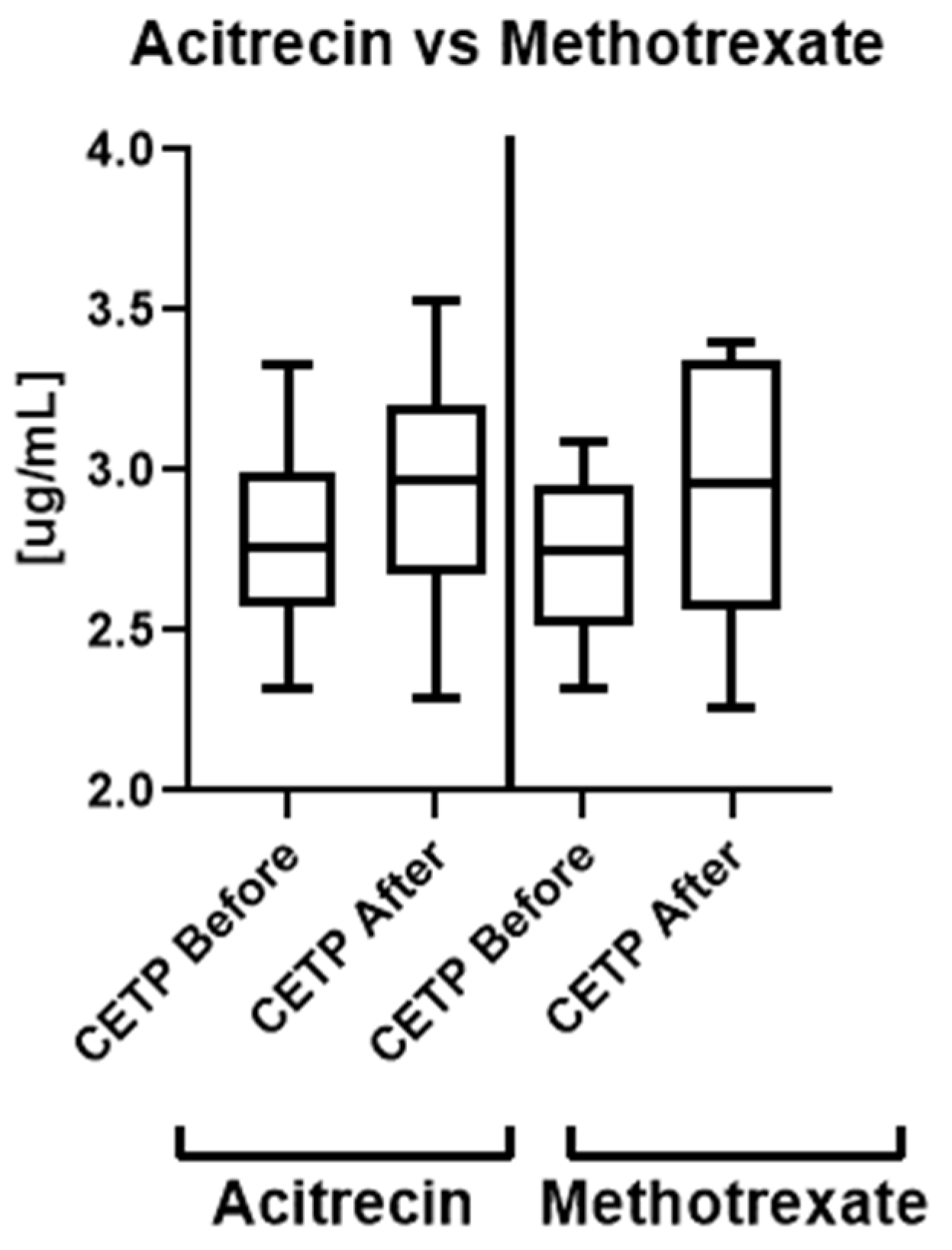
The analysis of the influence of treatment on CETP concentration did not reveal any beneficial outcome, including that particular antipsoriatic systemic drug did not show advantage in administration of one compared to the other. Nevertheless, we also noticed positive correlation between CETP concentration before the treatment with methotrexate and glucose, triglycerides and CRP concentration, which disappeared afterwards. This may indicate that this drug could be preferred in psoriatics with intense inflammatory condition, carbohydrates metabolism disorders and hypertriglyceridemia especially in order to modify or lower the further metabolic complications. Furthermore, CETP seems to exert a protective role in these disorders development in psoriasis. We found positive correlation between the liver function enzymes activity and CETP concentration after the treatment with acitretin, which is known to negatively affect this organ. Therefore, a potential idea for future research is to consider CETP as a marker of the side effects of acitretin in psoriatics.
As for SORT investigation, its serum concentration has not been studied in psoriatics before. The only study was the assessment of SORT expression in psoriatic epidermis, which was significantly increased [
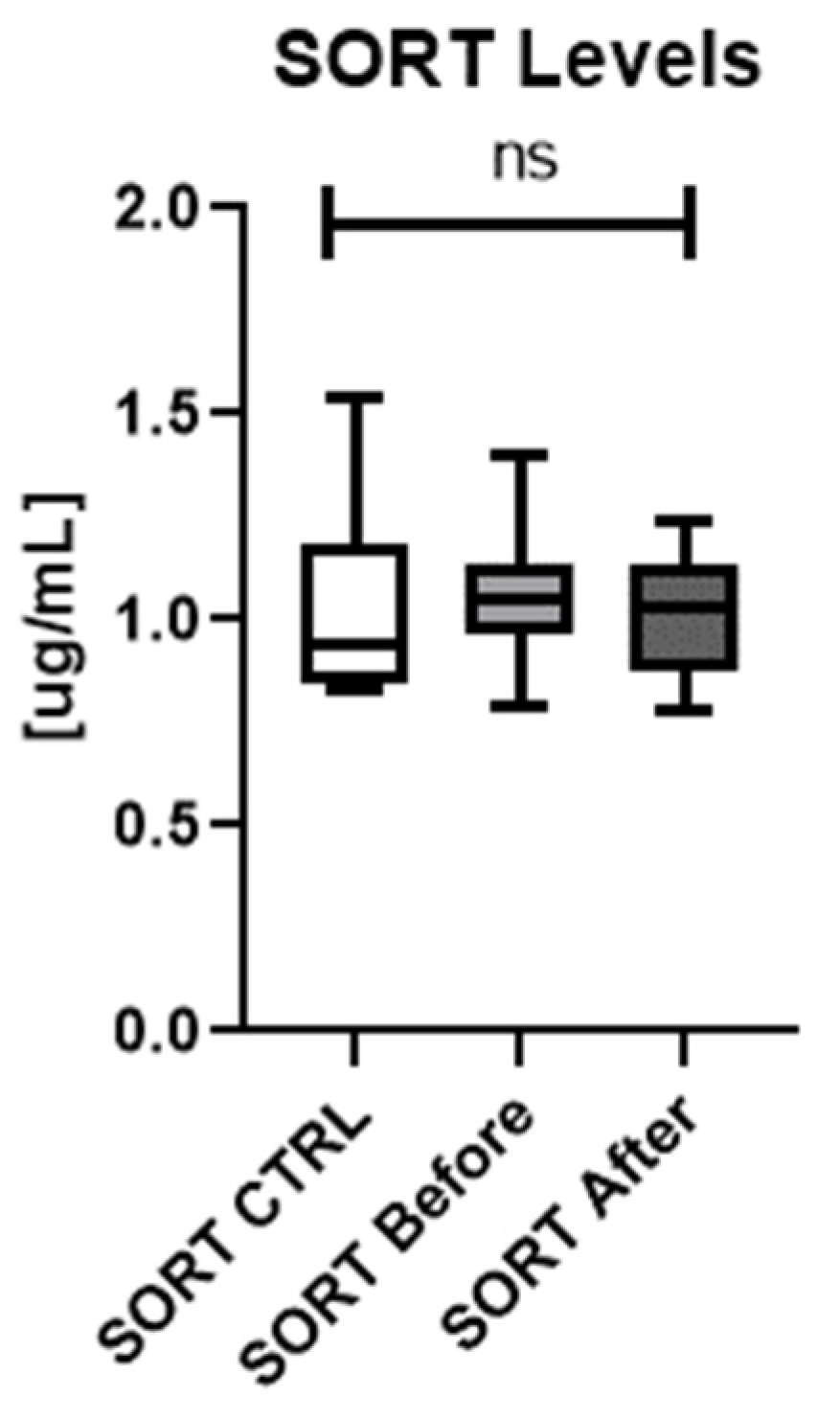
14]. In our study SORT serum concentration did not differ significantly between patients and controls and did not change after the treatment, although it perhaps should be verified on larger cohorts.
The second area of SORT involvement is apoptosis. In our previously published review paper [
9], we made a suggestion that SORT may actually be an apoptosis-promoting agent in psoriasis. As we found a negative correlation between the SORT concentration and PASI, we may assume that SORT could become a part of compensatory mechanism in psoriasis. Therefore, in patients with low SORT concentration we observed high PASI (severe skin lesions) and in patients with high SORT concentration–low PASI (less severe skin lesions).
As for laboratory parameters, SORT positively correlated with glucose and triglycerides concentration and negatively with HDL. In addition to the positive correlation of SORT and BMI, we may suspect that SORT could be studied as a marker of metabolic complications in psoriatics but still not used as a solitary indicator.
Another interesting finding is that SORT is positively correlated with inflammation indicators, which perhaps points the protein as a novel potential indicator of metabolically induced inflammatory condition in psoriatics. As these dependencies disappeared after treatment with acitretin, we presume it could be the preferred drug in subjects with high inflammatory markers, which should be proceeded in further studies.
An important observation from our study is that methotrexate caused statistically significant decrease in SORT concentration, which was significantly lower than before the treatment, therefore we believe that this antipsoriatic agent could be considered as the drug of choice in patients with elevated SORT concentration. Our results are preliminary, but furthermore significant links between the protein and metabolic disorders indicators noted additionally prove the broad protective cardiometabolic effects of methotrexate.
As for limitations of our study, it was a single-center research with relatively small number of subjects enrolled. Furthermore, all of the presented results should be interpreted with a higher than usual level of criticism since the sample size and the statistical power of the presented study is relatively low. We are aware that our outcomes should be treated as preliminary but they may point out a potential direction for future studies.
In the future we would like to extend our study and introduce some dietary changes and physical activity to the participants and observe their influence on the investigated proteins. Moreover, it would be valuable to study the impact of hypolipidemic and hypoglycemic drugs on analyzed proteins.
Author Contributions
J.N.: Writing—original draft preparation, Writing—review & editing, Data curation, Resources; A.B.: Conceptualization, Data curation, Investigation, Project administration, Writing—original draft preparation, Writing—review&editing, Supervision, Funding acquisition. J.A.K.: Data curation; Investigation; T.W.K.: Formal analysis; Software; Visualization; Writing—review and editing; M.M.: investigation; I.F.: Project administration; Supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a study grant from the Medical University of Bialystok (no N/ST/ZB/18/002/1149).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Medical University of Bialystok, Poland, no R-I-002/429/2017.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Because of the participant consent obtained as part of the recruitment process, it is not possible to make these data publicly available. The data resented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gisondi, P.; Fostini, A.C.; Fossà, I.; Girolomoni, G.; Targher, G. Psoriasis and the metabolic syndrome. Clin. Dermatol. 2018, 36, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Kishimoto, M.; Sugai, J.; Komine, M.; Ohtsuki, M. Risk Factors for the Development of Psoriasis. Int. J. Mol. Sci. 2019, 20, 4347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokuyama, M.; Mabuchi, T. New Treatment Addressing the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2020, 21, 7488. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Kirby, B. Psoriasis is a systemic disease with multiple cardiovascular and metabolic comorbidities. Dermatol. Clin. 2015, 33, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Mosiewicz, J.; Pietrzak, A.; Chodorowska, G.; Trojnar, M.; Szepietowski, J.; Reich, K.; Rizzo, M. Rational for statin use in psoriatic patients. Arch. Dermatol. Res. 2013, 305, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Sachinidis, A.; Nikolic, D.; Rizzo, M.; Cianflone, D. Psoriasis and acute coronary syndrome risk. Int. J. Cardiol. 2019, 286, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Nowowiejska, J.; Baran, A.; Flisiak, I. Psoriasis and cardiometabolic disorders. Dermatol. Rev. 2020, 107, 508–520. [Google Scholar] [CrossRef]
- Yamashita, S.; Matsuzawa, Y. Re-evaluation of cholesteryl ester transfer protein function in atherosclerosis based upon genetics and pharmacological manipulation. Curr. Opin. Lipidol. 2016, 27, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Krahel, J.A.; Baran, A.; Kamiński, T.W.; Flisiak, I. Proprotein Convertase Subtilisin/Kexin Type 9, Angiopoietin-Like Protein 8, Sortilin, and Cholesteryl Ester Transfer Protein-Friends of Foes for Psoriatic Patients at the Risk of Developing Cardiometabolic Syndrome? Int. J. Mol. Sci. 2020, 21, 3682. [Google Scholar] [CrossRef] [PubMed]
- Chowaniec, Z.; Skoczyńska, A. Plasma lipid transfer proteins: The role of PLTP and CETP in atherogenesis. Adv. Clin. Exp. Med. 2018, 27, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, H.C.F.; Raposo, H.F. Cholesteryl Ester Transfer Protein and Lipid Metabolism and Cardiovascular Diseases. Adv. Exp. Med. Biol. 2020, 1276, 15–25. [Google Scholar] [PubMed]
- Carlo, A.S. Sortilin, a novel APOE receptor implicated in Alzheimer disease. Prion 2013, 7, 378–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Wang, Y.H.; Shi, X.; Ji, J.; Zhan, F.Q.; Leng, H. Sortilin regulates keratinocyte proliferation and apoptosis through the PI3K-AKT signaling pathway. Life Sci. 2021, 278, 119630. [Google Scholar] [CrossRef] [PubMed]
- Truzzi, F.; Marconi, A.; Atzei, P.; Panza, M.C.; Lotti, R.; Dallaglio, K.; Tiberio, R.; Palazzo, E.; Vaschieri, C.; Pincelli, C. p75 neurotrophin receptor mediates apoptosis in transit-amplifying cells and its overexpression restores cell death in psoriatic keratinocytes. Cell Death Differ. 2010, 18, 948–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowowiejska, J.; Baran, A.; Flisiak, I. Mutual Relationship between Sleep Disorders, Quality of Life and Psychosocial Aspects in Patients with Psoriasis. Front. Psychiatry 2021, 12, 674460. [Google Scholar] [CrossRef] [PubMed]
- Feingold, K.R.; Grunfeld, C. The Effect of Inflammation and Infection on Lipids and Lipoproteins; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2022. [Google Scholar]
- Waśkiel-Burnat, A.; Niemczyk, A.; Blicharz, L.; Chmielińska, P.; Zaremba, M.; Gąsecka, A.; Filipiak, K.J.; Olszewska, M.; Rudnicka, L. Chemokine C-C Motif Ligand 7 (CCL7), a Biomarker of Atherosclerosis, Is Associated with the Severity of Alopecia Areata: A Preliminary Study. J. Clin. Med. 2021, 10, 5418. [Google Scholar] [CrossRef] [PubMed]
- Torkhovskaia, T.I.; Fortinskaia, E.S.; Ivanova, L.I.; Nikitina, N.A.; Zakharova, T.S.; Kochetova, M.M.; Kliuchnikova, Z.I.; Sharapova, G.; Khalilov, E.M. Osobennosti lipid-transportnoĭ sistemy pri psoriaze [Characteristics of the lipid transport system in psoriasis]. Vopr Med. Khim. 2002, 48, 297–303. [Google Scholar] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}