
Intestinal Absorption Study of a Granular Form of Ferric Pyrophosphate

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Fe Content in Tested Formulations
2.2. Gastroresistance
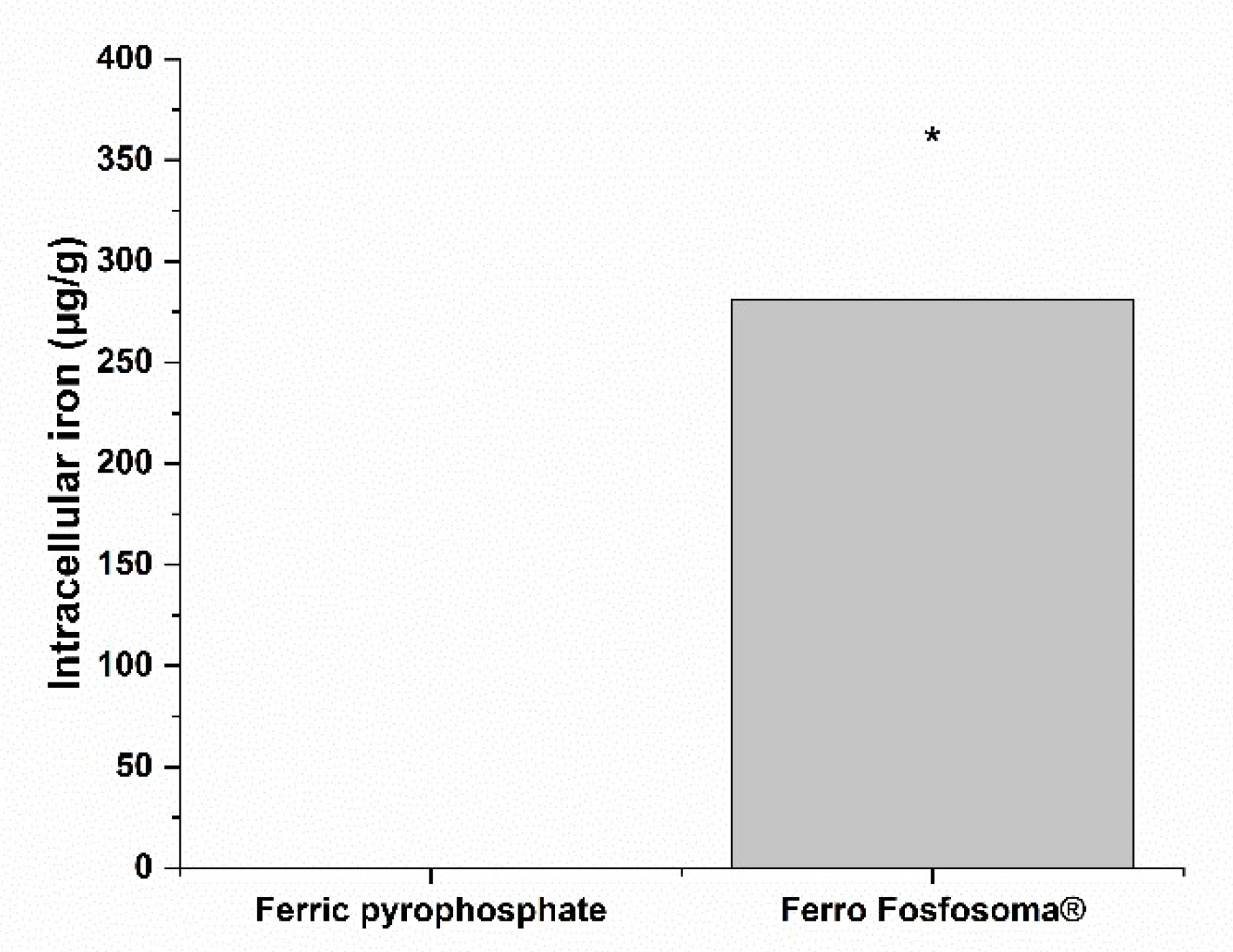
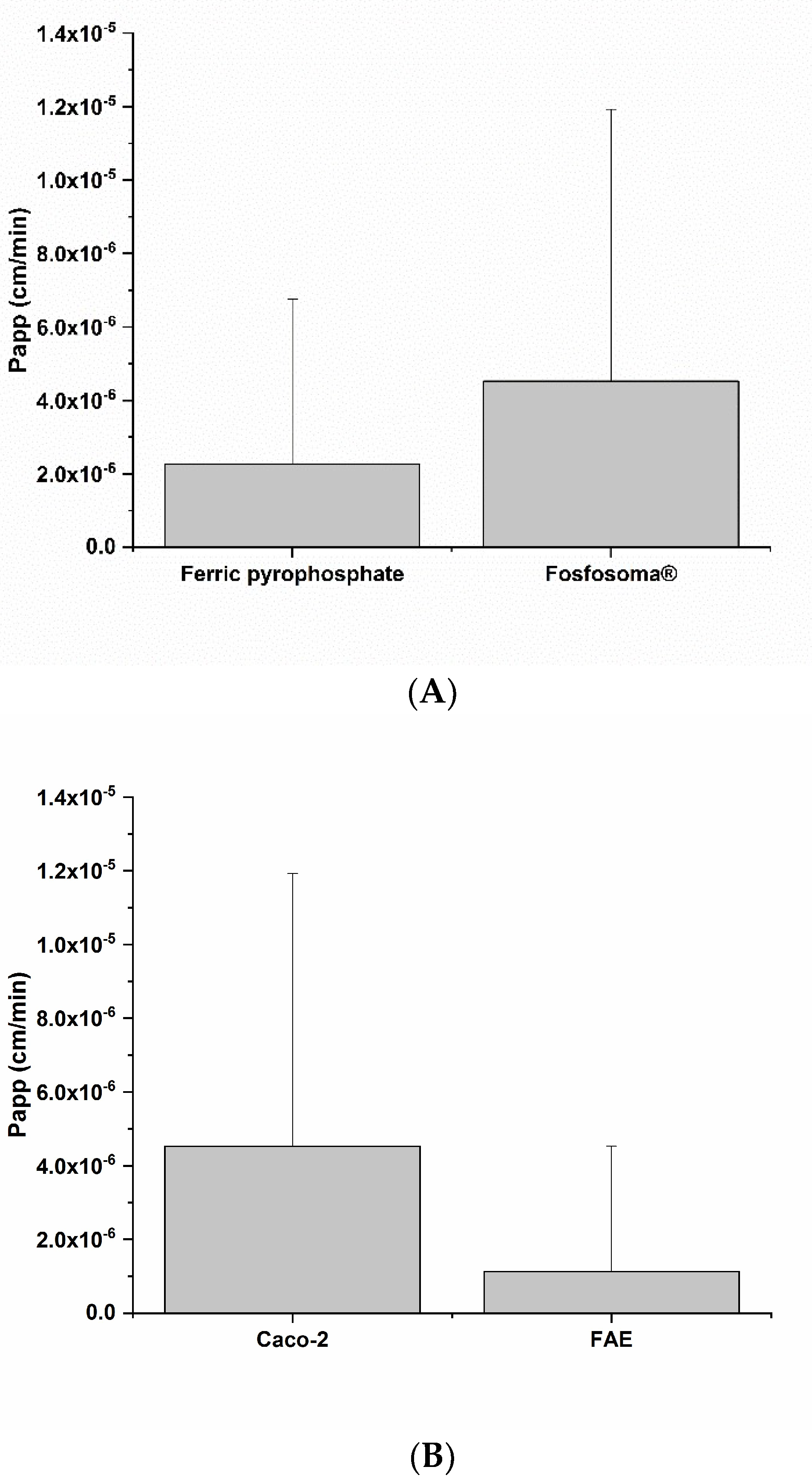
2.3. Fe Intestinal Absorption
2.4. Impact of Fe-Based Formulations on Intestinal Epithelium
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Formulation Composition
4.3. Cell Cultures
4.3.1. Caco-2 Cell Culture
4.3.2. Raji Cell Culture
4.4. Fe Content Determination in the Fe-Based Formulations
4.5. Determination of Gastroresistance of Fe-Based Formulation
4.6. Determination of Fe-Based Formulation Bioaccessibility
4.7. Intestinal Epithelium In Vitro Model
4.8. Evaluation of Fe Intestinal Absorption
4.9. Determination of Intracellular Ferritin
4.10. Vitality and Barrier Integrity of the Intestinal Epithelium Model
4.11. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). 2017. Available online: https://www.who.int/news-room/factsheets/detail/cardiovascular-diseases-(cvds) (accessed on 4 April 2022).
- Andrews, P.A.; Green, R.; Conrad, M.E.; Andrews, N.C. Disorders of iron metabolism. N. Engl. J. Med. 2000, 342, 1293–1294. [Google Scholar] [CrossRef] [PubMed]
- Hentze, M.W.; Muckenthaler, M.U.; Galy, B.; Camaschella, C. Two to Tango: Regulation of Mammalian Iron Metabolism. Cell 2010, 142, 24–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieu, P.T.; Heiskala, M.; Peterson, P.A.; Yang, Y. The roles of iron in health and disease. Mol. Asp. Med. 2001, 22, 1–87. [Google Scholar] [CrossRef]
- Ponka, P. Cellular iron metabolism. Kidney Int. Suppl. 1999, 55, 2–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludwig, H.; Evstatiev, R.; Kornek, G.; Aapro, M.; Bauernhofer, T.; Buxhofer-Ausch, V.; Fridrik, M.; Geissler, D.; Geissler, K.; Gisslinger, H.; et al. Iron metabolism and iron supplementation in cancer patients. Wien. Klin. Wochenschr. 2015, 127, 907–919. [Google Scholar] [CrossRef] [Green Version]
- Auerbach, M.; Adamson, J.W. How we diagnose and treat iron deficiency anemia. Am. J. Hematol. 2016, 91, 31–38. [Google Scholar] [CrossRef]
- Cook, J.D.; Ready, M.B. Efficacy of weekly compared with daily iron supplementation. Am. J. Clin. Nutr. 1995, 62, 117–120. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.A.; Fisher, S.A.; Doree, C.; Di Angelantonio, E.; Roberts, D.J. Oral or parenteral iron supplementation to reduce deferral, iron deficiency and/or anaemia in blood donors. Cochrane Database Syst. Rev. 2014, 2014, 7. [Google Scholar] [CrossRef]
- Santiago, P. Ferrous versus ferric oral iron formulations for the treatment of iron deficiency: A clinical overview. Sci. World J. 2012, 2012, 846824. [Google Scholar] [CrossRef]
- Pastore, P.; Roverso, M.; Tedesco, E.; Micheletto, M.; Mantovan, E.; Zanella, M.; Benetti, F. Comparative Evaluation of Intestinal Absorption and Functional Value of Iron Dietary Supplements and Drug with Different Delivery Systems. Molecules 2020, 25, 5989. [Google Scholar] [CrossRef]
- Giordano, G.; Mondello, P.; Tambaro, R.; De Maria, M.; D’Amico, F.; Sticca, G.; Di Falco, C. Intravenous iron support vs oral liposomal iron support in patients with refractory anemia treated with Epo alpha. Monocentric prospective study. Leuk. Res. 2011, 35, S137. [Google Scholar] [CrossRef]
- Xu, Z.; Liu, S.; Wang, H.; Gao, G.; Yu, P.; Chang, Y. Encapsulation of Iron in Liposomes Significantly Improved the Efficiency of Iron Supplementation in Strenuously Exercised Rats. Biol. Trace Elem. Res. 2014, 162, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Pisani, A.; Riccio, E.; Sabbatini, M.; Andreucci, M.; Del Rio, A.; Visciano, B. Effect of oral liposomal iron versus intravenous iron for treatment of iron deficiency anaemia in CKD patients: A randomized trial. Nephrol. Dial. Transplant. 2015, 30, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Pappalardo, A.; Currenti, W.; Ponzio, R.; Mellini, G.; Nicolosi, D.; Longhitano, L.; Tibullo, D.; Castorina, S.; Palumbo, G. Effects of micronised microencapsulated ferric pyrophosphate supplementation in patients with advanced cancer and iron deficiency: A single-centre cohort pilot study. Blood Transfus. 2019, 17, 196–199. [Google Scholar] [CrossRef]
- Blanco-Rojo, R.; Pérez-Granados, A.M.; Toxqui, L.; González-Vizcayno, C.; Delgado, M.A.; Vaquero, M.P. Efficacy of a microencapsulated iron pyrophosphate-fortified fruit juice: A randomised, double-blind, placebo-controlled study in Spanish iron-deficient women. Br. J. Nutr. 2011, 105, 1652–1659. [Google Scholar] [CrossRef] [Green Version]
- Zečkanović, A.; Kavčič, M.; Prelog, T.; Šmid, A.; Jazbec, J. Micronized, Microencapsulated Ferric Iron Supplementation in Randomized Clinical Study of Efficacy and Safety. Nutrients 2021, 13, 1087. [Google Scholar] [CrossRef]
- Hussain, U.; Zia, K.; Iqbal, R.; Saeed, M.; Ashraf, N. Efficacy of a Novel Food Supplement (Ferfer®) Containing Microencapsulated Iron in Liposomal Form in Female Iron Deficiency Anemia. Cureus 2019, 11, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Glahn, R.P.; Lee, O.A.; Yeung, A.; Goldman, M.I.; Miller, D.D. Caco-2 cell ferritin formation predicts nonradiolabeled food iron availability in an in vitro digestion/Caco-2 cell culture model. J. Nutr. 1998, 128, 1555–1561. [Google Scholar] [CrossRef] [Green Version]
- Wurzburg, O.B. Starch, modified starch and dextrin. In Proceedings of the Seminar in Products of the Corn Refining Industry, Washington, DC, USA, 1978; pp. 22–32. [Google Scholar]
- Kernéis, S.; Bogdanova, A.; Kraehenbuhl, J.P.; Pringault, E. Conversion by Peyer’s patch lymphocytes of human enterocytes into M cells that transport bacteria. Science 1997, 277, 949–952. [Google Scholar] [CrossRef]
- Qi, X.; Zhang, Y.; Guo, H.; Hai, Y.; Luo, Y.; Yue, T. Mechanism and intervention measures of iron side effects on the intestine. Crit. Rev. Food Sci. Nutr. 2020, 60, 2113–2125. [Google Scholar] [CrossRef]
- Andrews, C.M.; Lane, D.W.; Bradley, J.G. Iron pre-load for major joint replacement. Transfus. Med. 1997, 7, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Goddard, A.F.; James, M.W.; McIntyre, A.S.; Scott, B.B. Guidelines for the management of iron deficiency anaemia. Gut 2011, 60, 1309–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neutra, M.R.; Mantis, N.J.; Kraehenbuhl, J.P. Collaboration of epithelial cells with organized mucosal lymphoid tissues. Nat. Immunol. 2001, 2, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Jang, M.H.; Kweon, M.; Iwatani, K.; Yamamoto, M.; Terahara, K.; Sasakawa, C.; Suzuki, T.; Nochi, T.; Yokota, Y.; Rennert, P.D.; et al. Intestinal villous M cells: An antigen entry site in the mucosal epithelium. Proc. Natl. Acad. Sci. USA 2004, 101, 6110–6115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walczak, A.P.; Fokkink, R.; Peters, R.; Tromp, P.; Rivera, Z.E.H.; Rietjens, I.M.C.M.; Hendriksen, P.J.M.; Bouwmeester, H. Behaviour of silver nanoparticles and silver ions in an in vitro human gastrointestinal digestion model. Nanotoxicology 2013, 7, 1198–1210. [Google Scholar] [CrossRef]
- Scheers, N.M.; Almgren, A.B.; Sandberg, A.S. Proposing a Caco-2/HepG2 cell model for in vitro iron absorption studies. J. Nutr. Biochem. 2014, 25, 710–715. [Google Scholar] [CrossRef] [Green Version]
- Rieux, A.D.; Ragnarsson, E.G.E.; Gullberg, E.; Préat, V.; Schneider, Y.J.; Artursson, P. Transport of nanoparticles across an in vitro model of the human intestinal follicle associated epithelium. Eur. J. Pharm. Sci. 2005, 25, 455–465. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Declared Amount (%) | Measured Amount (%) | Recovery (%) | |
|---|---|---|---|
| Ferric pyrophosphate | 30 | 25 ± 0.3 | 83.4 ± 1.4 |
| Ferro Fosfosoma® | 11 | 11.6 ± 0.1 | 105.8 ± 0.6 |
| Ferric Pyrophosphate | Ferro Fosfosoma® | |
|---|---|---|
| Fe (%) | 7.5 ± 0.5 | 3.4 ± 0.2 |
| Fe Expected Amount (mg) | Fe Measured Amount (mg) | Recovery (%) | |
|---|---|---|---|
| Ferric pyrophosphate | 30 | 29.3 ± 2.6 | 97.7 ± 8.7 |
| Ferro Fosfosoma® | 30 | 32.4 ± 0.4 | 108.1 ± 1.5 |
| Fe Intestinal Absorption (µg/g) | |
|---|---|
| Ferric pyrophosphate | <LOD |
| Ferro Fosfosoma® | 281.12 ± 73.25 |
| Fe Intestinal Absorption (µg/g) | |
|---|---|
| Caco-2 | 281.12 ± 73.25 |
| FAE | 646.22 ± 53.13 |
| Ferritin Level (Fold Change) | |
|---|---|
| Ferric pyrophosphate | 1 |
| Ferro Fosfosoma® | 2.54 |
| Ferritin Level (Fold Change) | |
|---|---|
| Caco-2 | 1 |
| FAE | 2.89 |
| TEER (Ohms × cm2) | ||
|---|---|---|
| Pre-Treatment | Recovery 24 h | |
| Ferric pyrophosphate | 626.25 ± 70.88 | 604.58 ± 56.64 |
| Ferro Fosfosoma® | 660.8 ± 30.02 | 665.83 ± 16.64 |
| TEER (Ohms × cm2) | ||
|---|---|---|
| Pre-Treatment | Recovery 24 h | |
| Caco-2 | 660.8 ± 30.02 | 665.83 ± 16.64 |
| FAE | 797.21 ± 35.25 | 634.58 ± 21.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Micheletto, M.; Gaio, E.; Tedesco, E.; Di Maira, G.; Mantovan, E.; Zanella, M.; Pastore, P.; Roverso, M.; Favaro, G.; Benetti, F. Intestinal Absorption Study of a Granular Form of Ferric Pyrophosphate. Metabolites 2022, 12, 463. https://doi.org/10.3390/metabo12050463
Micheletto M, Gaio E, Tedesco E, Di Maira G, Mantovan E, Zanella M, Pastore P, Roverso M, Favaro G, Benetti F. Intestinal Absorption Study of a Granular Form of Ferric Pyrophosphate. Metabolites. 2022; 12(5):463. https://doi.org/10.3390/metabo12050463
Chicago/Turabian StyleMicheletto, Marta, Elisa Gaio, Erik Tedesco, Giovanni Di Maira, Etienne Mantovan, Michela Zanella, Paolo Pastore, Marco Roverso, Gabriella Favaro, and Federico Benetti. 2022. "Intestinal Absorption Study of a Granular Form of Ferric Pyrophosphate" Metabolites 12, no. 5: 463. https://doi.org/10.3390/metabo12050463
APA StyleMicheletto, M., Gaio, E., Tedesco, E., Di Maira, G., Mantovan, E., Zanella, M., Pastore, P., Roverso, M., Favaro, G., & Benetti, F. (2022). Intestinal Absorption Study of a Granular Form of Ferric Pyrophosphate. Metabolites, 12(5), 463. https://doi.org/10.3390/metabo12050463