
Bioavailability of Reduced Coenzyme Q10 (Ubiquinol-10) in Burn Patients

 , , , ,
, , , , 


Abstract
:1. Introduction
2. Results
2.1. Study Population
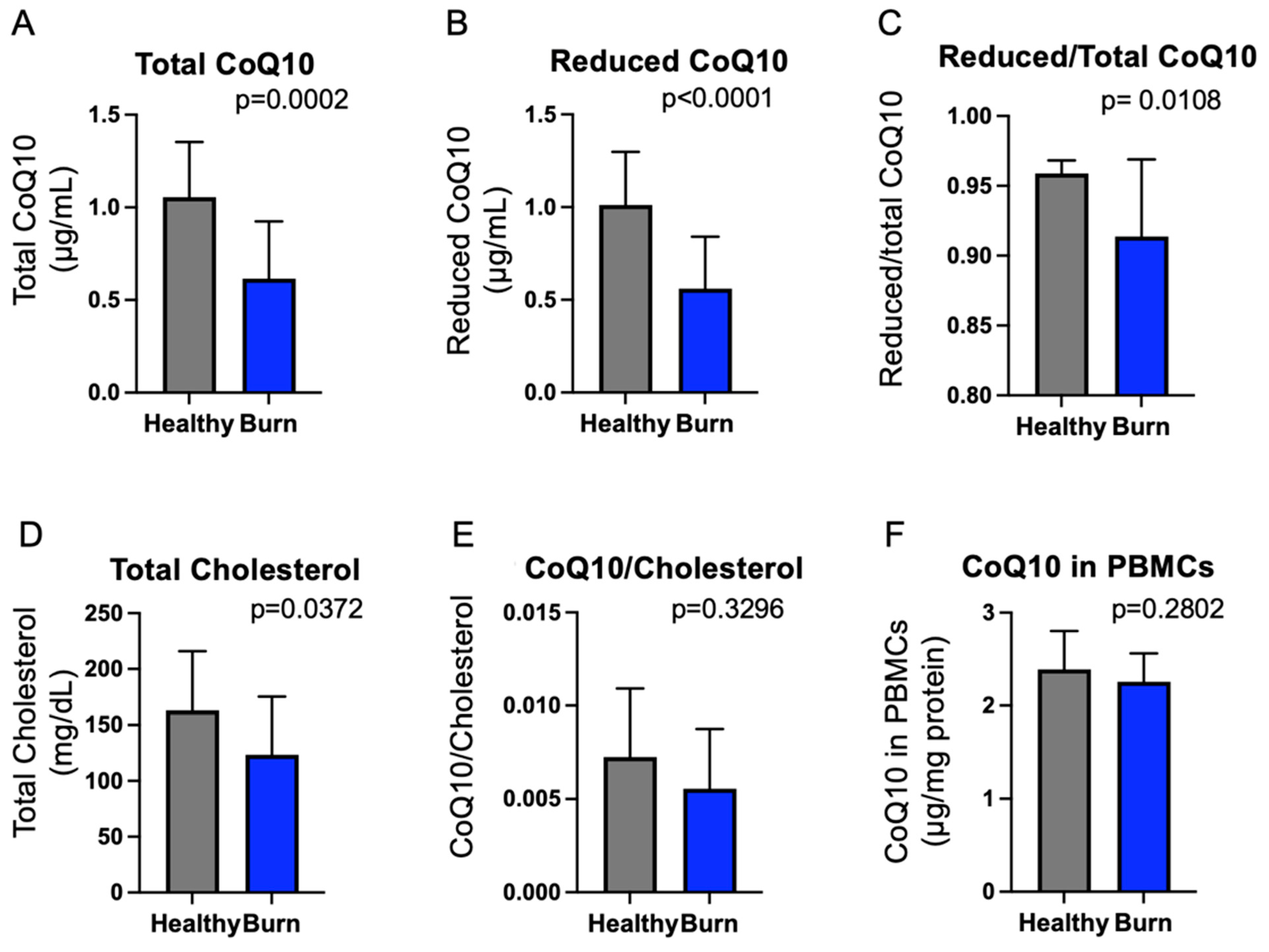
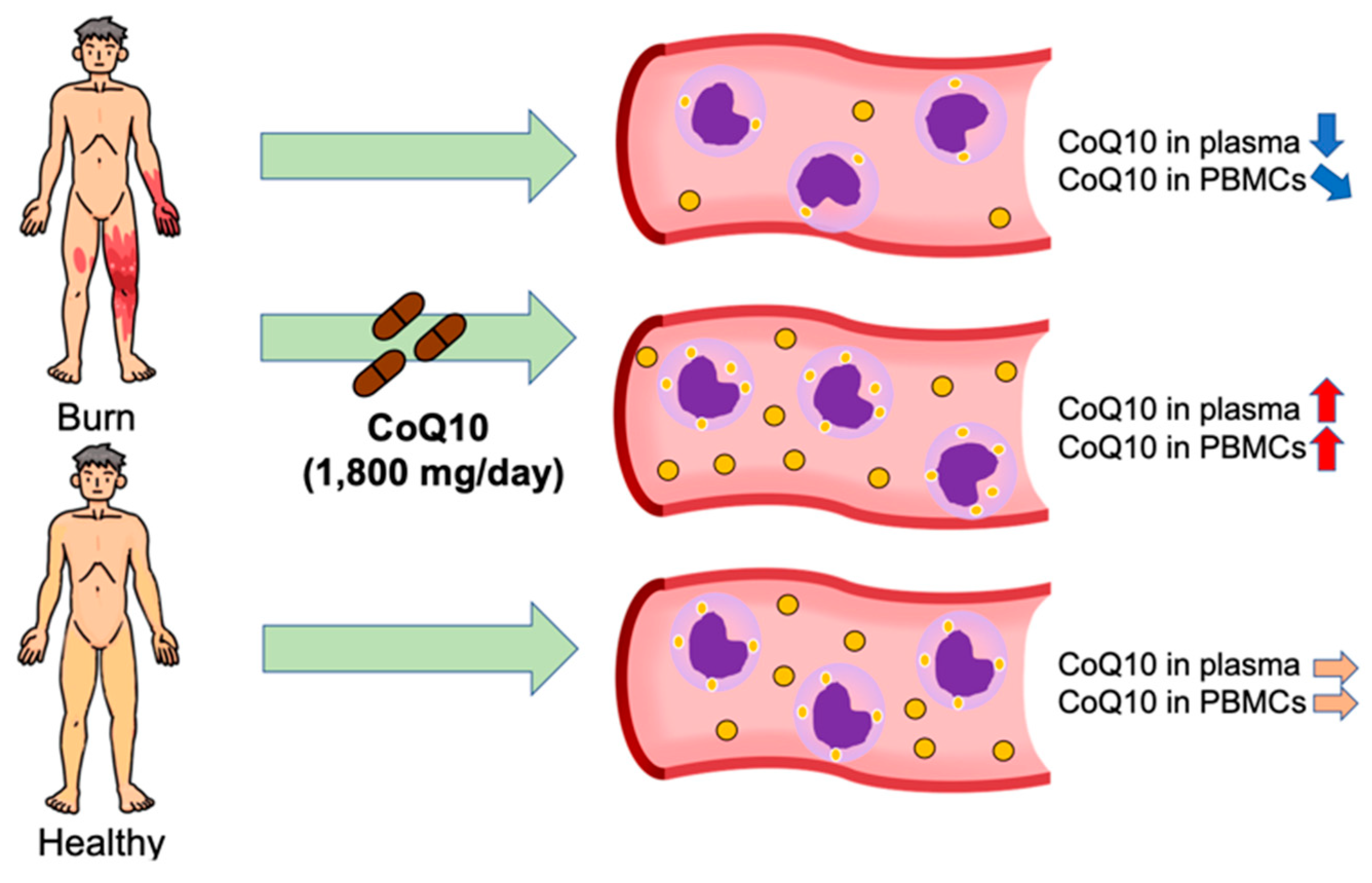
2.2. Plasma CoQ10 Concentrations and Total CoQ10 Content in PBMCs Were Lower in Burn Patients Compared with Healthy Volunteers
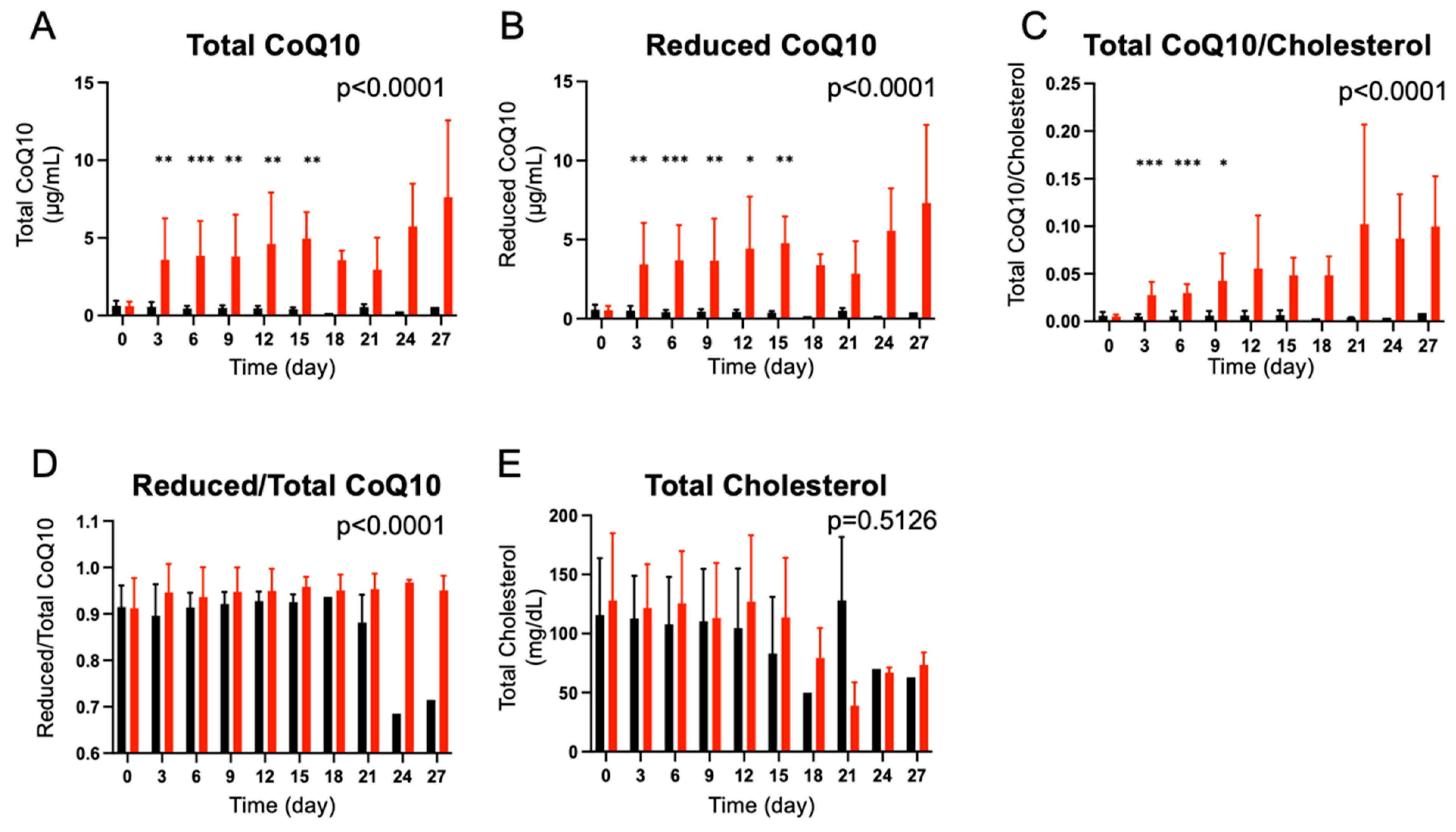
2.3. CoQ10 Supplementation Increased Plasma CoQ10 Concentrations and Reduced/Total CoQ10 Ratio in Burn Patients
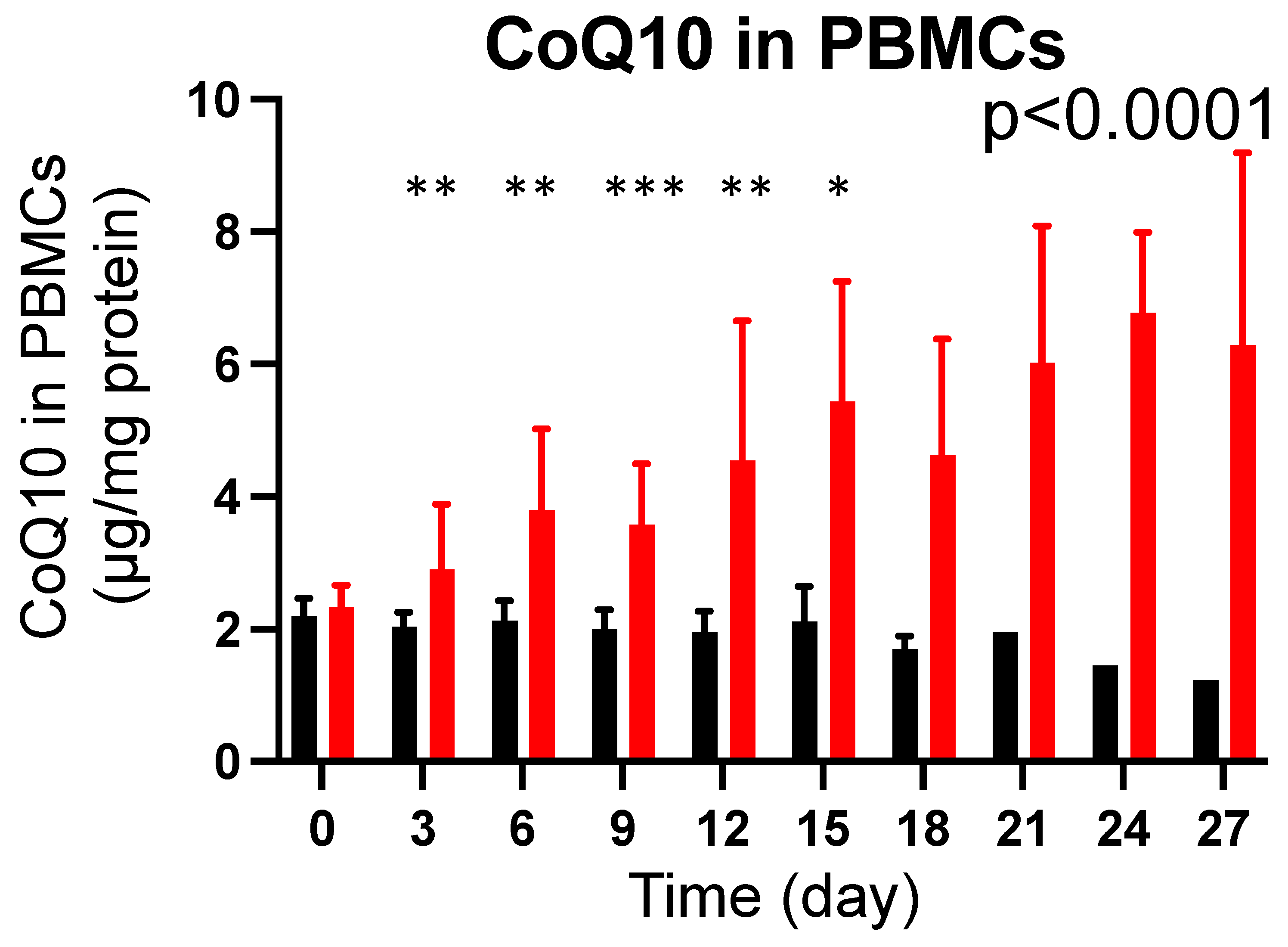
2.4. CoQ10 Supplementation Increased Total CoQ10 Content in PBMCs in Burn Patients
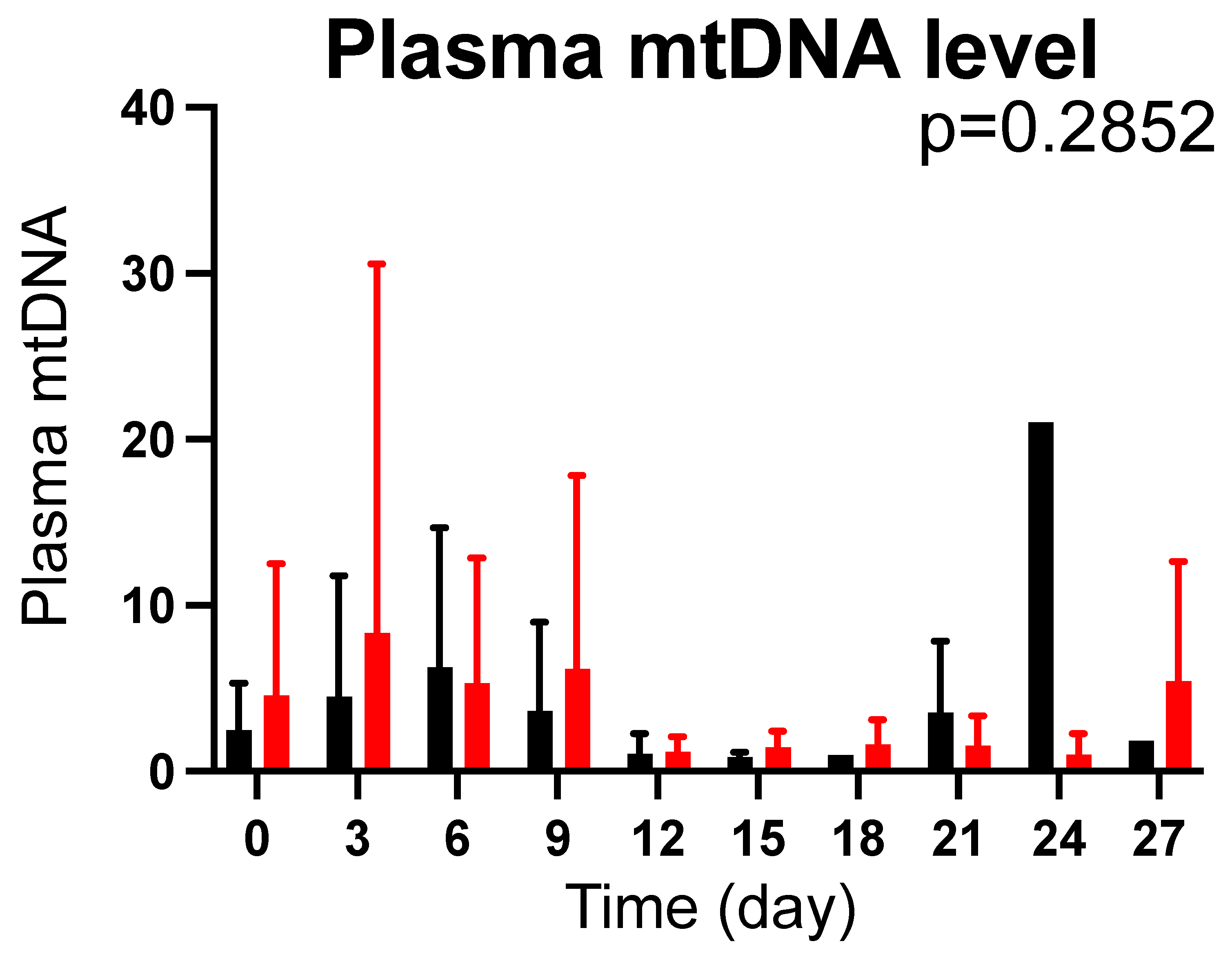
2.5. Effects of CoQ10 Supplementation on Plasma mtDNA Levels in Burn Patients
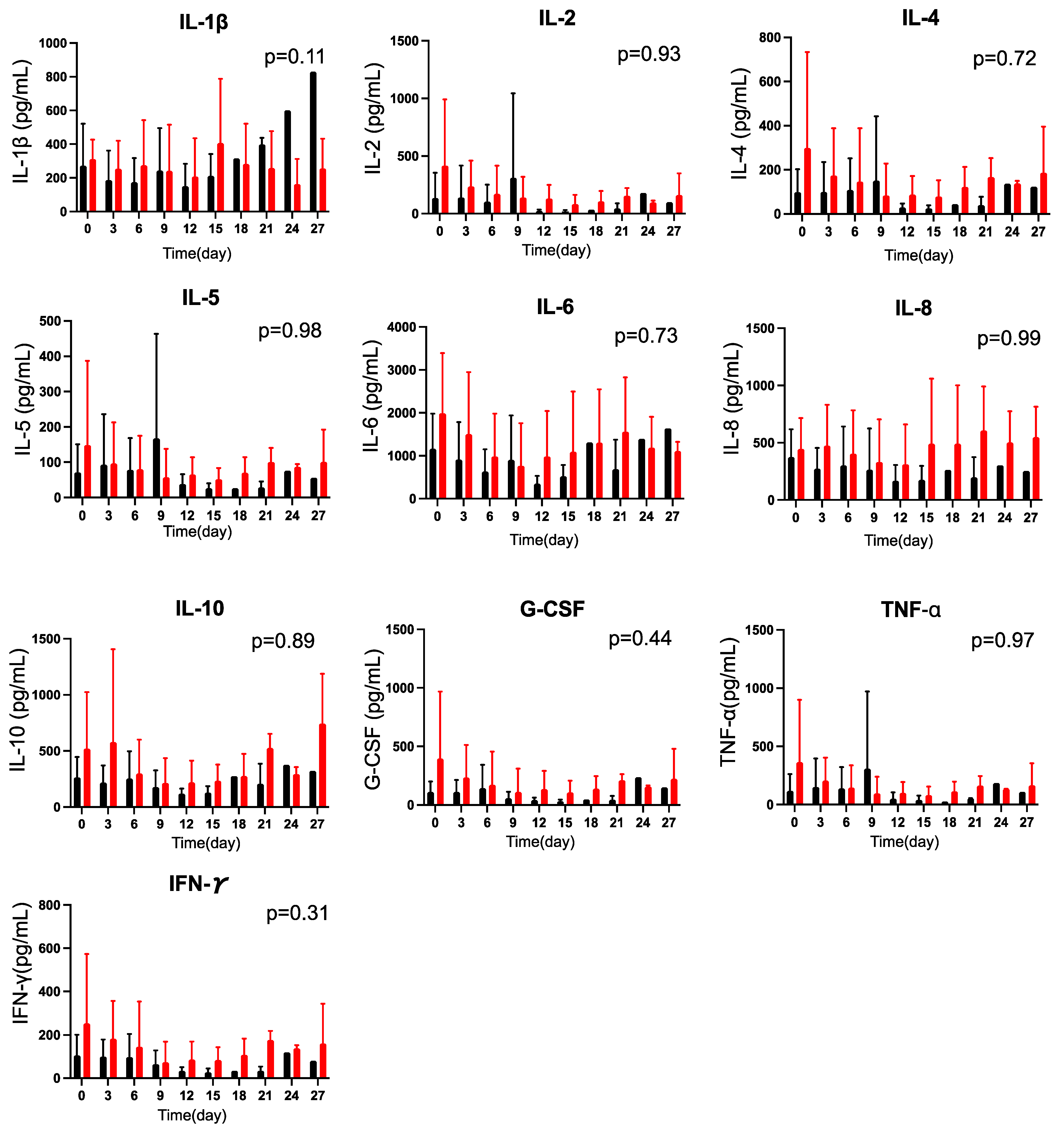
2.6. Effects of CoQ10 Supplementation on Plasma Cytokine Concentrations in Burn Patients
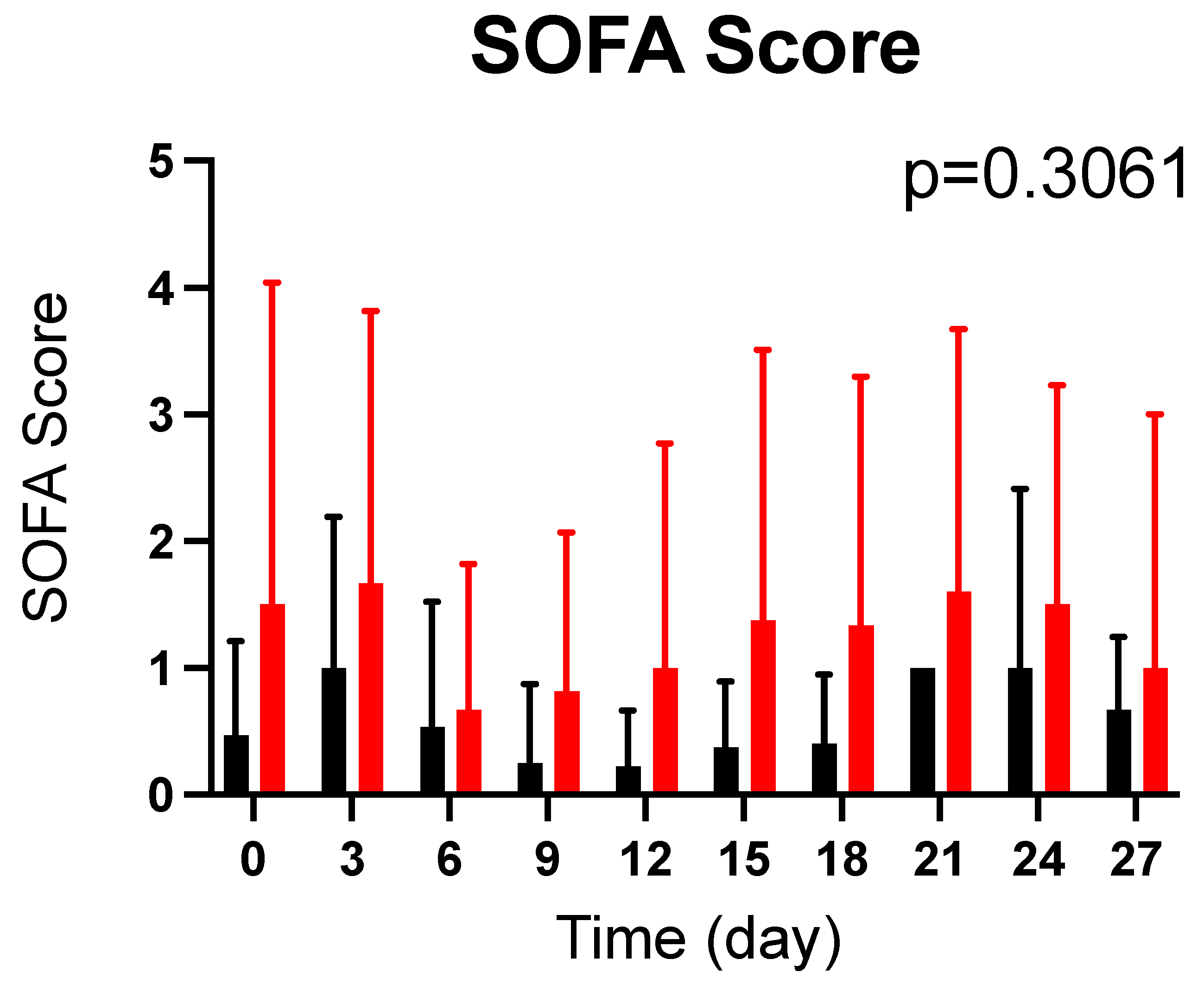
2.7. Effects of CoQ10 Supplementation on SOFA Score in Burn Patients
3. Discussion
4. Materials and Methods
4.1. Design and Setting
4.2. Study Population
4.3. Supplementation with Reduced CoQ10 (Ubiquinol-10)
4.4. Blood Samples and Clinical Data Collection
4.5. Measurement of CoQ10 Levels
4.6. Measurement of Plasma mtDNA Levels
4.7. Measurement of Plasma Cytokines
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miles, M.V.; Morrison, J.A.; Horn, P.S.; Tang, P.H.; Pesce, A.J. Coenzyme Q10 changes are associated with metabolic syndrome. Clin. Chim. Acta 2004, 344, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Langsjoen, P.H.; Langsjoen, A.M. Comparison study of plasma coenzyme Q10 levels in healthy subjects supplemented with ubiquinol versus ubiquinone. Clin. Pharmacol. Drug Dev. 2014, 3, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Quinzii, C.M.; Hirano, M. Primary and secondary CoQ(10) deficiencies in humans. Biofactors 2011, 37, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Littlefield, N.; Beckstrand, R.L.; Luthy, K.E. Statins’ effect on plasma levels of Coenzyme Q10 and improvement in myopathy with supplementation. J. Am. Assoc. Nurse Pract. 2014, 26, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Avis, H.J.; Hargreaves, I.P.; Ruiter, J.P.; Land, J.M.; Wanders, R.J.; Wijburg, F.A. Rosuvastatin lowers coenzyme Q10 levels, but not mitochondrial adenosine triphosphate synthesis, in children with familial hypercholesterolemia. J. Pediatr. 2011, 158, 458–462. [Google Scholar] [CrossRef]
- Cotan, D.; Cordero, M.D.; Garrido-Maraver, J.; Oropesa-Avila, M.; Rodriguez-Hernandez, A.; Gomez Izquierdo, L.; De la Mata, M.; De Miguel, M.; Lorite, J.B.; Infante, E.R.; et al. Secondary coenzyme Q10 deficiency triggers mitochondria degradation by mitophagy in MELAS fibroblasts. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2011, 25, 2669–2687. [Google Scholar] [CrossRef]
- Sacconi, S.; Trevisson, E.; Salviati, L.; Ayme, S.; Rigal, O.; Redondo, A.G.; Mancuso, M.; Siciliano, G.; Tonin, P.; Angelini, C.; et al. Coenzyme Q10 is frequently reduced in muscle of patients with mitochondrial myopathy. Neuromuscul. Disord. NMD 2010, 20, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Montero, R.; Grazina, M.; Lopez-Gallardo, E.; Montoya, J.; Briones, P.; Navarro-Sastre, A.; Land, J.M.; Hargreaves, I.P.; Artuch, R. Coenzyme Q(1)(0) deficiency in mitochondrial DNA depletion syndromes. Mitochondrion 2013, 13, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Mourier, A.; Motori, E.; Brandt, T.; Lagouge, M.; Atanassov, I.; Galinier, A.; Rappl, G.; Brodesser, S.; Hultenby, K.; Dieterich, C.; et al. Mitofusin 2 is required to maintain mitochondrial coenzyme Q levels. J. Cell Biol. 2015, 208, 429–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefely, J.A.; Pagliarini, D.J. Biochemistry of Mitochondrial Coenzyme Q Biosynthesis. Trends Biochem. Sci. 2017, 42, 824–843. [Google Scholar] [CrossRef]
- Mugoni, V.; Postel, R.; Catanzaro, V.; De Luca, E.; Turco, E.; Digilio, G.; Silengo, L.; Murphy, M.P.; Medana, C.; Stainier, D.Y.; et al. Ubiad1 is an antioxidant enzyme that regulates eNOS activity by CoQ10 synthesis. Cell 2013, 152, 504–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuhara, S.; Asai, A.; Sahani, N.D.; Martyn, J.A. Mitochondria, endoplasmic reticulum, and alternative pathways of cell death in critical illness. Crit. Care Med. 2007, 35, S488–S495. [Google Scholar] [CrossRef] [PubMed]
- Thiessen, S.E.; Van den Berghe, G.; Vanhorebeek, I. Mitochondrial and endoplasmic reticulum dysfunction and related defense mechanisms in critical illness-induced multiple organ failure. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 2534–2545. [Google Scholar] [CrossRef] [PubMed]
- Sterling, J.P.; Lombardi, V.C. Decreasing the Likelihood of Multiple Organ Dysfunction Syndrome in Burn Injury with Early Antioxidant Treatment. Antioxidants 2021, 10, 1192. [Google Scholar] [CrossRef]
- Itagaki, K.; Rica, I.; Konecna, B.; Kim, H.I.; Park, J.; Kaczmarek, E.; Hauser, C.J. Role of Mitochondria-Derived Danger Signals Released after Injury in Systemic Inflammation and Sepsis. Antioxid. Redox Signal. 2021, 35, 1273–1290. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Raoof, M.; Chen, Y.; Sumi, Y.; Sursal, T.; Junger, W.; Brohi, K.; Itagaki, K.; Hauser, C.J. Circulating mitochondrial DAMPs cause inflammatory responses to injury. Nature 2010, 464, 104–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itagaki, K.; Kaczmarek, E.; Lee, Y.T.; Tang, I.T.; Isal, B.; Adibnia, Y.; Sandler, N.; Grimm, M.J.; Segal, B.H.; Otterbein, L.E.; et al. Mitochondrial DNA released by trauma induces neutrophil extracellular traps. PLoS ONE 2015, 10, e0120549. [Google Scholar] [CrossRef]
- Schafer, S.T.; Franken, L.; Adamzik, M.; Schumak, B.; Scherag, A.; Engler, A.; Schonborn, N.; Walden, J.; Koch, S.; Baba, H.A.; et al. Mitochondrial DNA: An Endogenous Trigger for Immune Paralysis. Anesthesiology 2016, 124, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Coppadoro, A.; Berra, L.; Kumar, A.; Pinciroli, R.; Yamada, M.; Schmidt, U.H.; Bittner, E.A.; Kaneki, M. Critical illness is associated with decreased plasma levels of coenzyme Q10: A cross-sectional study. J. Crit. Care 2013, 28, 571–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassiliou, A.G.; Mastora, Z.; Jahaj, E.; Keskinidou, C.; Pratikaki, M.E.; Kampisiouli, E.; Orfanos, S.E.; Kotanidou, A.; Dimopoulou, I. Serum Coenzyme Q10 Levels are Decreased in Critically-Ill Septic Patients: Results From a Preliminary Study. Biol. Res. Nurs. 2021, 23, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Donnino, M.W.; Cocchi, M.N.; Salciccioli, J.D.; Kim, D.; Naini, A.B.; Buettner, C.; Akuthota, P. Coenzyme Q10 levels are low and may be associated with the inflammatory cascade in septic shock. Crit. Care 2011, 15, R189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocchi, M.N.; Giberson, B.; Berg, K.; Salciccioli, J.D.; Naini, A.; Buettner, C.; Akuthota, P.; Gautam, S.; Donnino, M.W. Coenzyme Q10 levels are low and associated with increased mortality in post-cardiac arrest patients. Resuscitation 2012, 83, 991–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakazawa, H.; Ikeda, K.; Shinozaki, S.; Yasuhara, S.; Yu, Y.M.; Martyn, J.A.J.; Tompkins, R.G.; Yorozu, T.; Inoue, S.; Kaneki, M. Coenzyme Q10 protects against burn-induced mitochondrial dysfunction and impaired insulin signaling in mouse skeletal muscle. FEBS Open Bio 2019, 9, 348–363. [Google Scholar] [CrossRef] [PubMed]
- Shults, C.W.; Flint Beal, M.; Song, D.; Fontaine, D. Pilot trial of high dosages of coenzyme Q10 in patients with Parkinson’s disease. Exp. Neurol. 2004, 188, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, K.L.; Shefner, J.; Zhang, H.; Betensky, R.; O’Brien, M.; Yu, H.; Fantasia, M.; Taft, J.; Beal, M.F.; Traynor, B.; et al. Tolerance of high-dose (3000 mg/day) coenzyme Q10 in ALS. Neurology 2005, 65, 1834–1836. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Camacho, J.D.; Bernier, M.; Lopez-Lluch, G.; Navas, P. Coenzyme Q10 Supplementation in Aging and Disease. Front. Physiol. 2018, 9, 44. [Google Scholar] [CrossRef] [Green Version]
- Fotino, A.D.; Thompson-Paul, A.M.; Bazzano, L.A. Effect of coenzyme Q(1)(0) supplementation on heart failure: A meta-analysis. Am. J. Clin. Nutr. 2013, 97, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeldt, F.L.; Haas, S.J.; Krum, H.; Hadj, A.; Ng, K.; Leong, J.Y.; Watts, G.F. Coenzyme Q10 in the treatment of hypertension: A meta-analysis of the clinical trials. J. Hum. Hypertens. 2007, 21, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Suksomboon, N.; Poolsup, N.; Juanak, N. Effects of coenzyme Q10 supplementation on metabolic profile in diabetes: A systematic review and meta-analysis. J. Clin. Pharm. Ther. 2015, 40, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Sabbatinelli, J.; Orlando, P.; Galeazzi, R.; Silvestri, S.; Cirilli, I.; Marcheggiani, F.; Dludla, P.V.; Giuliani, A.; Bonfigli, A.R.; Mazzanti, L.; et al. Ubiquinol Ameliorates Endothelial Dysfunction in Subjects with Mild-to-Moderate Dyslipidemia: A Randomized Clinical Trial. Nutrients 2020, 12, 1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beal, M.F.; Oakes, D.; Shoulson, I.; Henchcliffe, C.; Galpern, W.R.; Haas, R.; Juncos, J.L.; Nutt, J.G.; Voss, T.S.; Ravina, B.; et al. A randomized clinical trial of high-dosage coenzyme Q10 in early Parkinson disease: No evidence of benefit. JAMA Neurol. 2014, 71, 543–552. [Google Scholar] [CrossRef] [PubMed]
- McGarry, A.; McDermott, M.; Kieburtz, K.; de Blieck, E.A.; Beal, F.; Marder, K.; Ross, C.; Shoulson, I.; Gilbert, P.; Mallonee, W.M.; et al. A randomized, double-blind, placebo-controlled trial of coenzyme Q10 in Huntington disease. Neurology 2017, 88, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, B.A.; Lorson, L.; White, C.M.; Thompson, P.D. A randomized trial of coenzyme Q10 in patients with confirmed statin myopathy. Atherosclerosis 2015, 238, 329–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, S.; Nojima, J.; Kajimoto, O.; Yamaguti, K.; Nakatomi, Y.; Kuratsune, H.; Watanabe, Y. Ubiquinol-10 supplementation improves autonomic nervous function and cognitive function in chronic fatigue syndrome. Biofactors 2016, 42, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Bhagavan, H.N.; Chopra, R.K. Coenzyme Q10: Absorption, tissue uptake, metabolism and pharmacokinetics. Free Radic. Res. 2006, 40, 445–453. [Google Scholar] [CrossRef]
- Miles, M.V. The uptake and distribution of coenzyme Q10. Mitochondrion 2007, 7, S72–S77. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, J.; Chen, X.Q.; Oliver Chen, C.Y. Ubiquinol is superior to ubiquinone to enhance Coenzyme Q10 status in older men. Food Funct. 2018, 9, 5653–5659. [Google Scholar] [CrossRef]
- Failla, M.L.; Chitchumroonchokchai, C.; Aoki, F. Increased bioavailability of ubiquinol compared to that of ubiquinone is due to more efficient micellarization during digestion and greater GSH-dependent uptake and basolateral secretion by Caco-2 cells. J. Agric. Food Chem. 2014, 62, 7174–7182. [Google Scholar] [CrossRef]
- Garcia-Corzo, L.; Luna-Sanchez, M.; Doerrier, C.; Ortiz, F.; Escames, G.; Acuna-Castroviejo, D.; Lopez, L.C. Ubiquinol-10 ameliorates mitochondrial encephalopathy associated with CoQ deficiency. Biochim. Biophys. Acta 2014, 1842, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Nozaki, S.; Goto, M.; Kaneko, K.I.; Hayashinaka, E.; Irie, S.; Nishiyama, A.; Kasai, K.; Fujii, K.; Wada, Y.; et al. PET imaging of (11)C-labeled coenzyme Q10: Comparison of biodistribution between [(11)C]ubiquinol-10 and [(11)C]ubiquinone-10. Biochem. Biophys. Res. Commun. 2019, 512, 611–615. [Google Scholar] [CrossRef]
- Desbats, M.A.; Lunardi, G.; Doimo, M.; Trevisson, E.; Salviati, L. Genetic bases and clinical manifestations of coenzyme Q10 (CoQ 10) deficiency. J. Inherit. Metab. Dis. 2015, 38, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Bhagavan, H.N.; Chopra, R.K. Plasma coenzyme Q10 response to oral ingestion of coenzyme Q10 formulations. Mitochondrion 2007, 7, S78–S88. [Google Scholar] [CrossRef] [PubMed]
- Huntington Study, G. A randomized, placebo-controlled trial of coenzyme Q10 and remacemide in Huntington’s disease. Neurology 2001, 57, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Shults, C.W.; Oakes, D.; Kieburtz, K.; Beal, M.F.; Haas, R.; Plumb, S.; Juncos, J.L.; Nutt, J.; Shoulson, I.; Carter, J.; et al. Effects of coenzyme Q10 in early Parkinson disease: Evidence of slowing of the functional decline. Arch. Neurol. 2002, 59, 1541–1550. [Google Scholar] [CrossRef]
- Alleva, R.; Tomasetti, M.; Bompadre, S.; Littarru, G.P. Oxidation of LDL and their subfractions: Kinetic aspects and CoQ10 content. Mol. Aspects Med. 1997, 18, S105–S112. [Google Scholar] [CrossRef]
- Johansen, K.; Theorell, H.; Karlsson, J.; Diamant, B.; Folkers, K. Coenzyme Q10, alpha-tocopherol and free cholesterol in HDL and LDL fractions. Ann. Med. 1991, 23, 649–656. [Google Scholar] [CrossRef]
- Tomasetti, M.; Alleva, R.; Solenghi, M.D.; Littarru, G.P. Distribution of antioxidants among blood components and lipoproteins: Significance of lipids/CoQ10 ratio as a possible marker of increased risk for atherosclerosis. Biofactors 1999, 9, 231–240. [Google Scholar] [CrossRef]
- Miles, M.V.; Horn, P.S.; Tang, P.H.; Morrison, J.A.; Miles, L.; DeGrauw, T.; Pesce, A.J. Age-related changes in plasma coenzyme Q10 concentrations and redox state in apparently healthy children and adults. Clin. Chim. Acta 2004, 347, 139–144. [Google Scholar] [CrossRef]
- Kaikkonen, J.; Nyyssonen, K.; Tuomainen, T.P.; Ristonmaa, U.; Salonen, J.T. Determinants of plasma coenzyme Q10 in humans. FEBS Lett. 1999, 443, 163–166. [Google Scholar] [CrossRef] [Green Version]
- Vanni, H.E.; Gordon, B.R.; Levine, D.M.; Sloan, B.J.; Stein, D.R.; Yurt, R.W.; Saal, S.D.; Parker, T.S. Cholesterol and interleukin-6 concentrations relate to outcomes in burn-injured patients. J. Burn Care Rehabil. 2003, 24, 133–141. [Google Scholar] [CrossRef]
- Vemula, M.; Berthiaume, F.; Jayaraman, A.; Yarmush, M.L. Expression profiling analysis of the metabolic and inflammatory changes following burn injury in rats. Physiol. Genom. 2004, 18, 87–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordero, M.D.; Cotán, D.; del-Pozo-Martín, Y.; Carrión, A.M.; de Miguel, M.; Bullón, P.; Sánchez-Alcazar, J.A. Oral coenzyme Q10 supplementation improves clinical symptoms and recovers pathologic alterations in blood mononuclear cells in a fibromyalgia patient. Nutrition 2012, 28, 1200–1203. [Google Scholar] [CrossRef] [PubMed]
- Niklowitz, P.; Sonnenschein, A.; Janetzky, B.; Andler, W.; Menke, T. Enrichment of coenzyme Q10 in plasma and blood cells: Defense against oxidative damage. Int. J. Biol. Sci. 2007, 3, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Wigginton, J.G.; Maass, D.L.; Ma, L.; Carlson, D.; Wolf, S.E.; Minei, J.P.; Zang, Q.S. Estrogen-provided cardiac protection following burn trauma is mediated through a reduction in mitochondria-derived DAMPs. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H882–H894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczesny, B.; Brunyanszki, A.; Ahmad, A.; Olah, G.; Porter, C.; Toliver-Kinsky, T.; Sidossis, L.; Herndon, D.N.; Szabo, C. Time-Dependent and Organ-Specific Changes in Mitochondrial Function, Mitochondrial DNA Integrity, Oxidative Stress and Mononuclear Cell Infiltration in a Mouse Model of Burn Injury. PLoS ONE 2015, 10, e0143730. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Xu, F.; Si, S.; Zhao, X.; Bi, S.; Cen, Y. Mitochondrial DNA-Induced Inflammatory Responses and Lung Injury in Thermal Injury Rat Model: Protective Effect of Epigallocatechin Gallate. J. Burn Care Res. 2017, 38, 304–311. [Google Scholar] [CrossRef]
- Carter, D.W.; Prudovsky, I.; Kacer, D.; Soul, T.; Kumpel, C.; Pyburn, K.; Palmeri, M.; Kramer, R.; Rappold, J. Tranexamic acid suppresses the release of mitochondrial DAMPs and reduces lung inflammation in a murine burn model. J. Trauma Acute Care Surg. 2019, 86, 617–624. [Google Scholar] [CrossRef]
- Liu, R.; Xu, F.; Bi, S.; Zhao, X.; Jia, B.; Cen, Y. Mitochondrial DNA-Induced Inflammatory Responses and Lung Injury in Thermal Injury Murine Model: Protective Effect of Cyclosporine-A. J. Burn Care Res. 2019, 40, 355–360. [Google Scholar] [CrossRef]
- Wu, Y.; Hao, C.; Liu, X.; Han, G.; Yin, J.; Zou, Z.; Zhou, J.; Xu, C. MitoQ protects against liver injury induced by severe burn plus delayed resuscitation by suppressing the mtDNA-NLRP3 axis. Int. Immunopharmacol. 2020, 80, 106189. [Google Scholar] [CrossRef]
- Tsuji, D.; Nakazawa, H.; Yorozu, T.; Kaneki, M. Protective effects of farnesyltransferase inhibitor on sepsis-induced morphological aberrations of mitochondria in muscle and increased circulating mitochondrial DNA levels in mice. Biochem. Biophys. Res. Commun. 2021, 556, 93–98. [Google Scholar] [CrossRef]
- Picca, A.; Lezza, A.M.S.; Leeuwenburgh, C.; Pesce, V.; Calvani, R.; Bossola, M.; Manes-Gravina, E.; Landi, F.; Bernabei, R.; Marzetti, E. Circulating Mitochondrial DNA at the Crossroads of Mitochondrial Dysfunction and Inflammation During Aging and Muscle Wasting Disorders. Rejuvenation Res. 2018, 21, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Yeh, F.L.; Lin, W.L.; Shen, H.D.; Fang, R.H. Changes in serum tumour necrosis factor-alpha in burned patients. Burns 1997, 23, 6–10. [Google Scholar] [CrossRef]
- Hur, J.; Yang, H.T.; Chun, W.; Kim, J.H.; Shin, S.H.; Kang, H.J.; Kim, H.S. Inflammatory cytokines and their prognostic ability in cases of major burn injury. Ann. Lab. Med. 2015, 35, 105–110. [Google Scholar] [CrossRef]
- Pileri, D.; Accardo Palombo, A.; D’Amelio, L.; D’Arpa, N.; Amato, G.; Masellis, A.; Cataldo, V.; Mogavero, R.; Napoli, B.; Lombardo, C.; et al. Concentrations of cytokines IL-6 and IL-10 in plasma of burn patients: Their relationship to sepsis and outcome. Ann. Burn. Fire Disasters 2008, 21, 182–185. [Google Scholar]
- Vindenes, H.; Ulvestad, E.; Bjerknes, R. Increased levels of circulating interleukin-8 in patients with large burns: Relation to burn size and sepsis. J. Trauma 1995, 39, 635–640. [Google Scholar] [CrossRef]
- Marano, M.A.; Fong, Y.; Moldawer, L.L.; Wei, H.; Calvano, S.E.; Tracey, K.J.; Barie, P.S.; Manogue, K.; Cerami, A.; Shires, G.T.; et al. Serum cachectin/tumor necrosis factor in critically ill patients with burns correlates with infection and mortality. Surg. Gynecol. Obstet. 1990, 170, 32–38. [Google Scholar]
- Drost, A.C.; Burleson, D.G.; Cioffi, W.G., Jr.; Jordan, B.S.; Mason, A.D., Jr.; Pruitt, B.A., Jr. Plasma cytokines following thermal injury and their relationship with patient mortality, burn size, and time postburn. J. Trauma 1993, 35, 335–339. [Google Scholar] [CrossRef] [Green Version]
- Mandrup-Poulsen, T.; Wogensen, L.D.; Jensen, M.; Svensson, P.; Nilsson, P.; Emdal, T.; Mølvig, J.; Dinarello, C.A.; Nerup, J. Circulating interleukin-1 receptor antagonist concentrations are increased in adult patients with thermal injury. Crit. Care Med. 1995, 23, 26–33. [Google Scholar] [CrossRef]
- Accardo Palumbo, A.; Forte, G.I.; Pileri, D.; Vaccarino, L.; Conte, F.; D’Amelio, L.; Palmeri, M.; Triolo, A.; D’Arpa, N.; Scola, L.; et al. Analysis of IL-6, IL-10 and IL-17 genetic polymorphisms as risk factors for sepsis development in burned patients. Burns 2012, 38, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.L.; O’Sullivan, C.; O’Riordain, M.; O’Riordain, D.; Lyons, A.; Doherty, J.; Mannick, J.A.; Rodrick, M.L. Is circulating endotoxin the trigger for the systemic inflammatory response syndrome seen after injury? Ann. Surg. 1997, 225, 530–541; discussion 541–533. [Google Scholar] [CrossRef]
- Fan, L.; Feng, Y.; Chen, G.C.; Qin, L.Q.; Fu, C.L.; Chen, L.H. Effects of coenzyme Q10 supplementation on inflammatory markers: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2017, 119, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Zhai, J.; Bo, Y.; Lu, Y.; Liu, C.; Zhang, L. Effects of Coenzyme Q10 on Markers of Inflammation: A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0170172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osler, T.; Glance, L.G.; Hosmer, D.W. Simplified estimates of the probability of death after burn injuries: Extending and updating the baux score. J. Trauma 2010, 68, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Lorente, J.A.; Vallejo, A.; Galeiras, R.; Tomicic, V.; Zamora, J.; Cerda, E.; de la Cal, M.A.; Esteban, A. Organ dysfunction as estimated by the sequential organ failure assessment score is related to outcome in critically ill burn patients. Shock 2009, 31, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.H.; Miles, M.V.; Steele, P.; DeGrauw, A.; Chuck, G.; Schroer, L.; Pesce, A. Anticoagulant effects on plasma coenzyme Q(10) estimated by HPLC with coulometric detection. Clin. Chim. Acta 2002, 318, 127–131. [Google Scholar] [CrossRef]
- Venegas, V.; Wang, J.; Dimmock, D.; Wong, L.J. Real-time quantitative PCR analysis of mitochondrial DNA content. Curr. Protoc. Hum. Genet. 2011, 68, 19.7.1–19.7.12. [Google Scholar] [CrossRef]
- Laird, N.M.; Ware, J.H. Random-effects models for longitudinal data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placebo (n = 15) | CoQ10 (n = 14) | p-Value * | Healthy Volunteers (n = 11) | |
|---|---|---|---|---|
| Age (y.o.) | 48.2 ± 18.7 | 49.3 ± 15.7 | 0.87 | 34.5 ± 8.5 |
| Females, n (%) | 6 (40%) | 2 (14%) | n/a | 5 (45%) |
| Height (cm) | 168.9 ± 7.3 | 173.9 ± 7.6 | 0.09 | |
| Body Weight (kg) | 81.6 ± 13.1 | 78.9 ± 12.7 | 0.62 | |
| BMI | 28.6 ± 4.5 | 26.3 ± 4.7 | 0.18 | |
| TBSA (%) | 13.8 ± 10.7 | 19.2 ± 19.4 | 0.35 | |
| Revised Baux Score | 67.3 ± 27.3 | 69.9 ± 24.9 | 0.62 | |
| SOFA Score | 0.5 ± 0.9 | 0.9 ± 1.3 | 0.14 | |
| LOS (day) | 22.7 ± 23.1 | 22.6 ± 13.7 | 0.98 | |
| Type of burn | ||||
| Scald | 2 | 2 | n/a | |
| Flame | 12 | 11 | n/a | |
| Contact | 1 | 1 | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuriyama, N.; Nakamura, T.; Nakazawa, H.; Wen, T.; Berra, L.; Bittner, E.A.; Goverman, J.; Kaneki, M. Bioavailability of Reduced Coenzyme Q10 (Ubiquinol-10) in Burn Patients. Metabolites 2022, 12, 613. https://doi.org/10.3390/metabo12070613
Kuriyama N, Nakamura T, Nakazawa H, Wen T, Berra L, Bittner EA, Goverman J, Kaneki M. Bioavailability of Reduced Coenzyme Q10 (Ubiquinol-10) in Burn Patients. Metabolites. 2022; 12(7):613. https://doi.org/10.3390/metabo12070613
Chicago/Turabian StyleKuriyama, Naohide, Tomoyuki Nakamura, Harumasa Nakazawa, Tyler Wen, Lorenzo Berra, Edward A. Bittner, Jeremy Goverman, and Masao Kaneki. 2022. "Bioavailability of Reduced Coenzyme Q10 (Ubiquinol-10) in Burn Patients" Metabolites 12, no. 7: 613. https://doi.org/10.3390/metabo12070613
APA StyleKuriyama, N., Nakamura, T., Nakazawa, H., Wen, T., Berra, L., Bittner, E. A., Goverman, J., & Kaneki, M. (2022). Bioavailability of Reduced Coenzyme Q10 (Ubiquinol-10) in Burn Patients. Metabolites, 12(7), 613. https://doi.org/10.3390/metabo12070613