
The Influence of Orthopedic Surgery on Circulating Metabolite Levels, and their Associations with the Incidence of Postoperative Delirium

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Collection and Preparation
2.3. Targeted Metabolomics
2.4. CSF Aβ42, t-tau, and p-tau Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
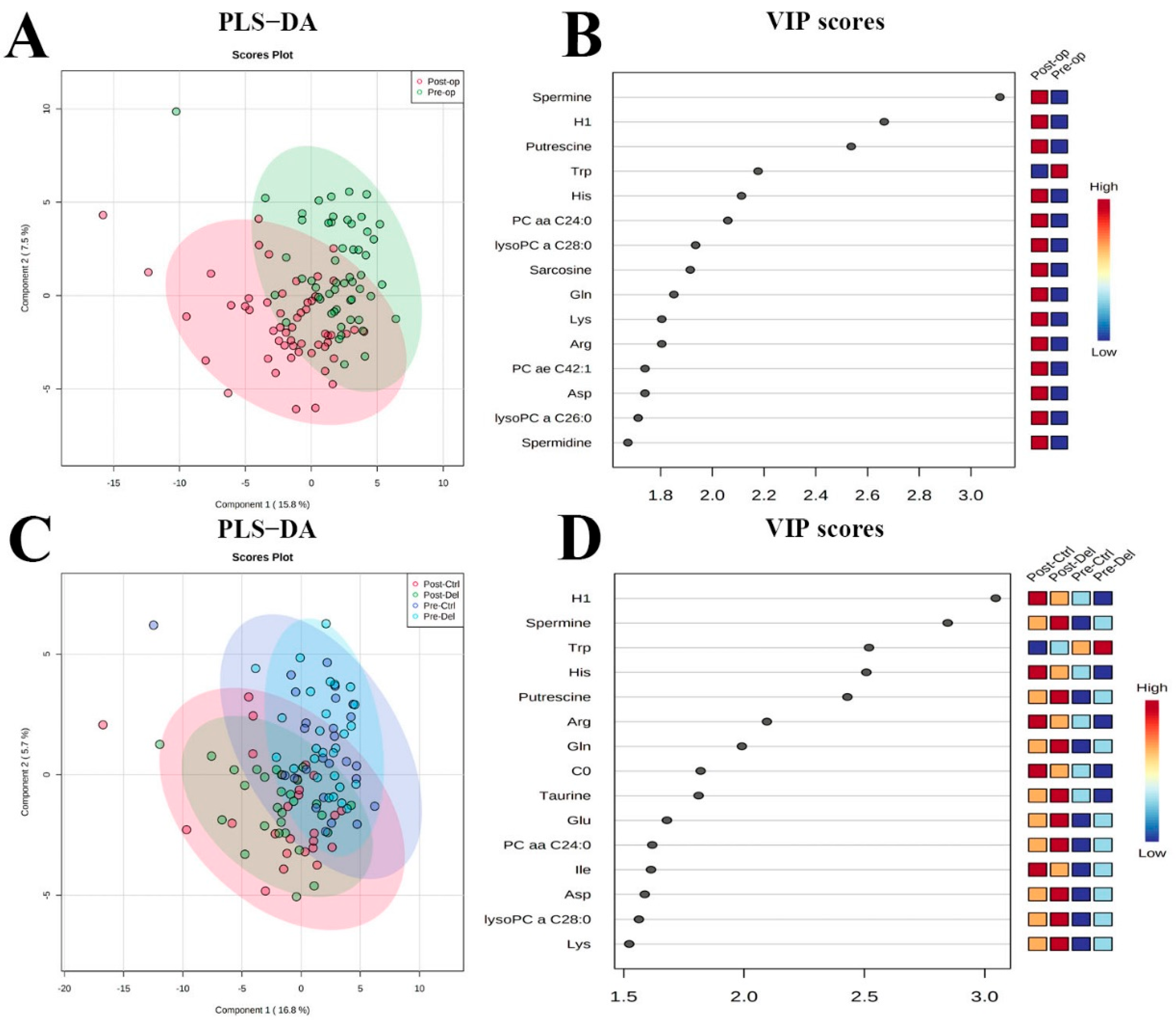
3.2. Analysis of Metabolites
3.3. Predictor Variables for Delirium
3.4. Associations between Perioperative Variables and Metabolites
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Inouye, S.K.; Westendorp, R.G.J.; Saczynski, J.S. Delirium in elderly people. Lancet 2014, 383, 911–922. [Google Scholar] [CrossRef] [Green Version]
- Chaiwat, O.; Chanidnuan, M.; Pancharoen, W.; Vijitmala, K.; Danpornprasert, P.; Toadithep, P.; Thanakiattiwibun, C. Postoperative delirium in critically ill surgical patients: Incidence, risk factors, and predictive scores. BMC Anesthesiol. 2019, 19, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, N.; Park, J.Y. The Motoric Types of Delirium and Estimated Blood Loss during Perioperative Period in Orthopedic Elderly Patients. Biomed. Res. Int. 2018, 2018, 9812041. [Google Scholar] [CrossRef] [PubMed]
- Song, K.J.; Ko, J.H.; Kwon, T.Y.; Choi, B.W. Etiology and Related Factors of Postoperative Delirium in Orthopedic Surgery. Clin. Orthop. Surg. 2019, 11, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhao, X.; Gao, L.; Wang, Y.; Wang, J. Incidence and associated factors of delirium after orthopedic surgery in elderly patients: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 1493–1506. [Google Scholar] [CrossRef]
- Leslie, D.L.; Inouye, S.K. The importance of delirium: Economic and societal costs. J. Am. Geriatr. Soc. 2011, 59, S241–S243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, T.E.; Chen, C.; Wang, Y.; Jung, E.; Swanson, A.; Ing, C.; Garcia, P.S.; Whittington, R.A.; Moitra, V. Association of Delirium with Long-term Cognitive Decline: A Meta-analysis. JAMA Neurol. 2020, 77, 1373–1381. [Google Scholar] [CrossRef]
- National Joint Registry. National Joint Registry14th Annual Report 2017; National Joint Registry: London, UK, 2017. [Google Scholar]
- Royal College of Physicians. National Hip Fracture Database Annual Report 2017; Royal College of Physicians: London, UK, 2017. [Google Scholar]
- Metz, T.O.; Zhang, Q.; Page, J.S.; Shen, Y.; Callister, S.J.; Jacobs, J.M.; Smith, R.D. Future of liquid chromatography–mass spectrometry in metabolic profiling and metabolomic studies for biomarker discovery. Biomark. Med. 2017, 1, 159–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.; Xiao, J.F.; Tuli, L.; Ressom, H.W. LC-MS-based metabolomics. Mol. Biosyst. 2012, 8, 470–481. [Google Scholar] [CrossRef] [Green Version]
- Graham, S.F.; Chevallier, O.P.; Roberts, D.; Hölscher, C.; Elliott, C.T.; Green, B.D. Investigation of the human brain metabolome to identify potential markers for early diagnosis and therapeutic targets of Alzheimer’s disease. Anal. Chem. 2013, 85, 1803–1811. [Google Scholar] [CrossRef] [PubMed]
- Macias, S.; Kirma, J.; Yilmaz, A.; Moore, S.E.; McKinley, M.C.; McKeown, P.P.; Woodside, J.V.; Graham, S.F.; Green, B.D. Application of (1)H-NMR Metabolomics for the Discovery of Blood Plasma Biomarkers of a Mediterranean Diet. Metabolites 2019, 9, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, X.; Cunningham, E.L.; Passmore, A.P.; McGuinness, B.; McAuley, D.F.; Beverland, D.; O’Brien, S.; Mawhinney, T.; Schott, J.M.; Zetterberg, H.; et al. Cerebrospinal Fluid Spermidine, Glutamine and Putrescine Predict Postoperative Delirium Following Elective Orthopaedic Surgery. Sci. Rep. 2019, 9, 4191. [Google Scholar] [CrossRef] [Green Version]
- Schneider, P.; Hampel, H.; Buerger, K. Biological marker candidates of Alzheimer’s disease in blood, plasma, and serum. CNS Neurosci. Ther. 2009, 15, 358–374. [Google Scholar]
- Jiang, Y.; Zhu, Z.; Shi, J.; An, Y.; Zhang, K.; Wang, Y.; Li, S.; Jin, L.; Ye, W.; Cui, M.; et al. Metabolomics in the Development and Progression of Dementia: A Systematic Review. Front. Neurosci. 2019, 13, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, T.N.; Raeburn, C.D.; Angles, E.M.; Moss, M. Low tryptophan levels are associated with postoperative delirium in the elderly. Am. J. Surg. 2008, 196, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watne, L.O.; Idland, A.V.; Fekkes, D.; Raeder, J.; Frihagen, F.; Ranhoff, A.H.; Chaudhry, F.A.; Engedal, K.; Wyller, T.B.; Hassel, B. Increased CSF levels of aromatic amino acids in hip fracture patients with delirium suggests higher monoaminergic activity. BMC Geriatr. 2016, 16, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Zhang, Y.N.; Jia, P.Y.; Wang, W.Y.; Zhou, Q.H.; Sun, L.L.; Zhao, A.H.; Zhang, X.; Wang, X.M.; Li, Y.C.; et al. Preoperative Serum Metabolites Are Associated with Postoperative Delirium in Elderly Hip-Fracture Patients. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Li, Y.; Zhang, Y.; Fang, S.; Xu, X.; Zhao, A.; Zhang, J.; Li, J.V.; Ma, D.; Jia, W.; et al. Post-operative delirium associated with metabolic alterations following hemi-arthroplasty in older patients. Age Ageing 2020, 49, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Zhang, W.; Liu, J.; Song, Y.; Liu, T.; Li, Z.; Wang, X.; Yang, N.; Li, Y.; Han, D.; et al. Metabolomic and Lipidomic Profiling of Preoperative CSF in Elderly Hip Fracture Patients with Postoperative Delirium. Front. Aging Neurosci. 2020, 12, 570210. [Google Scholar] [CrossRef]
- Cuperlovic-Culf, M.; Cunningham, E.L.; Teimoorinia, H.; Surendra, A.; Pan, X.; Bennett, S.A.L.; Jung, M.; McGuiness, B.; Passmore, A.P.; Beverland, D.; et al. Metabolomics and computational analysis of the role of monoamine oxidase activity in delirium and SARS-COV-2 infection. Sci. Rep. 2021, 11, 10629. [Google Scholar] [CrossRef]
- Marcantonio, E.R.; Rudolph, J.L.; Culley, D.; Crosby, G.; Alsop, D.; Inouye, S.K. Serum biomarkers for delirium. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1281–1286. [Google Scholar] [CrossRef] [Green Version]
- Tripp, B.A.; Dillon, S.T.; Yuan, M.; Asara, J.M.; Vasunilashorn, S.M.; Fong, T.G.; Metzger, E.D.; Inouye, S.K.; Xie, Z.; Ngo, L.H.; et al. Targeted metabolomics analysis of postoperative delirium. Sci. Rep. 2021, 11, 1521. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, E.L.; Mawhinney, T.; Beverland, D.; O’Brien, S.; McAuley, D.F.; Cairns, R.; Passmore, P.; McGuinness, B. Observational cohort study examining apolipoprotein E status and preoperative neuropsychological performance as predictors of post-operative delirium in an older elective arthroplasty population. Age Ageing 2017, 46, 779–786. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, E.L.; McGuinness, B.; McAuley, D.F.; Toombs, J.; Mawhinney, T.; O’Brien, S.; Beverland, D.; Schott, J.M.; Lunn, M.P.; Zetterberg, H.; et al. CSF Beta-amyloid 1-42 Concentration Predicts Delirium Following Elective Arthroplasty Surgery in an Observational Cohort Study. Ann. Surg. 2019, 269, 1200–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pegg, A.E. Regulation of ornithine decarboxylase. J. Biol. Chem. 2006, 281, 14529–14532. [Google Scholar] [CrossRef] [Green Version]
- Guerra, G.P.; Mello, C.F.; Bochi, G.V.; Pazini, A.M.; Rosa, M.M.; Ferreira, J.; Rubin, M.A. Spermidine-induced improvement of memory involves a cross-talk between protein kinases C and A. J. Neurochem. 2012, 122, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.K.; Scheunemann, L.; Eisenberg, T.; Mertel, S.; Bhukel, A.; Koemans, T.S.; Kramer, J.M.; Liu, K.S.; Schroeder, S.; Stunnenberg, H.G.; et al. Restoring polyamines protects from age-induced memory impairment in an autophagy-dependent manner. Nat. Neurosci. 2013, 16, 1453–1460. [Google Scholar] [CrossRef]
- Signor, C.; Mello, C.F.; Porto, G.P.; Ribeiro, D.A.; Rubin, M.A. Spermidine improves fear memory persistence. Eur. J. Pharmacol. 2014, 730, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Sigrist, S.J.; Carmona-Gutierrez, D.; Gupta, V.K.; Bhukel, A.; Mertel, S.; Eisenberg, T.; Madeo, F. Spermidine-triggered autophagy ameliorates memory during aging. Autophagy 2014, 10, 178–179. [Google Scholar] [CrossRef] [Green Version]
- Inoue, K.; Tsutsui, H.; Akatsu, H.; Hashizume, Y.; Matsukawa, N.; Yamamoto, T.; Toyo’oka, T. Metabolic profiling of Alzheimer’s disease brains. Sci. Rep. 2013, 3, 2364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trushina, E.; Dutta, T.; Persson, X.M.; Mielke, M.M.; Petersen, R.C. Identification of altered metabolic pathways in plasma and CSF in mild cognitive impairment and Alzheimer’s disease using metabolomics. PLoS ONE 2013, 8, e63644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.; Fleete, M.S.; Jing, Y.; Collie, N.D.; Curtis, M.A.; Waldvogel, H.J.; Faull, R.L.M.; Abraham, W.C.; Zhang, H. Altered arginine metabolism in Alzheimer’s disease brains. Neurobiol. Aging 2014, 35, 1992–2003. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.F.; Chevallier, O.P.; Elliott, C.T.; Holscher, C.; Johnston, J.; McGuinness, B.; Kehoe, P.G.; Passmore, A.P.; Green, B.D. Untargeted Metabolomic Analysis of Human Plasma Indicates Differentially Affected Polyamine and L-Arginine Metabolism in Mild Cognitive Impairment Subjects Converting to Alzheimer’s Disease. PLoS ONE 2015, 10, e0119452. [Google Scholar] [CrossRef] [PubMed]
- Saiki, S.; Sasazawa, Y.; Fujimaki, M.; Kamagata, K.; Kaga, N.; Taka, H.; Li, Y.; Souma, S.; Hatano, T.; Imamichi, Y.; et al. A Metabolic profile of polyamines in parkinson disease: A promising biomarker. Ann. Neurol. 2019, 86, 251–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akyol, S.; Yilmaz, A.; Oh, K.J.; Ugur, Z.; Aydas, B.; McGuinness, B.; Passmore, P.; Kehoe, P.G.; Maddens, M.; Green, B.D.; et al. Evidence that the Kennedy and polyamine pathways are dysregulated in human brain in cases of dementia with Lewy bodies. Brain Res. 2020, 1743, 146897. [Google Scholar] [CrossRef]
- Sandusky-Beltran, L.A.; Kovalenko, A.; Placides, D.S.; Ratnasamy, K.; Ma, C.; Hunt, J.B., Jr.; Liang, H.; Calahatian, J.I.T.; Michalski, C.; Fahnestock, M.; et al. Aberrant AZIN2 and polyamine metabolism precipitates tau neuropathology. J. Clin. Invest. 2021, 131, e126299. [Google Scholar] [CrossRef]
- Strozyk, D.; Blennow, K.; White, L.R.; Launer, L.J. CSF Abeta 42 levels correlate with amyloid-neuropathology in a population-based autopsy study. Neurology 2003, 60, 652–656. [Google Scholar] [CrossRef]
- Handa, A.K.; Fatima, T.; Mattoo, A.K. Polyamines: Bio-Molecules with Diverse Functions in Plant and Human Health and Disease. Front. Chem. 2018, 6, 10. [Google Scholar] [CrossRef] [Green Version]
- Yatin, S.M.; Yatin, M.; Varadarajan, S.; Ain, K.B.; Butterfield, D.A. Role of spermine in amyloid beta-peptide-associated free radical-induced neurotoxicity. J. Neurosci. Res. 2001, 63, 395–401. [Google Scholar] [CrossRef]
- Luo, J.; Yu, C.H.; Yu, H.; Borstnar, R.; Kamerlin, S.C.L.; Gräslund, A.; Abrahams, J.P.; Wärmländer, S.K.T.S. Cellular polyamines promote amyloid-beta (Aβ) peptide fibrillation and modulate the aggregation pathways. ACS Chem. Neurosci. 2013, 4, 454–462. [Google Scholar] [CrossRef]
- Yatin, S.M.; Yatin, M.; Aulick, T.; Ain, K.B.; Butterfield, D.A. Alzheimer’s amyloid beta-peptide associated free radicals increase rat embryonic neuronal polyamine uptake and ornithine decarboxylase activity: Protective effect of vitamin E. Neurosci. Lett. 1999, 263, 17–20. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Unadjusted | Adjusted | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | Odds Ratio | 95% CI | p-Value | |
| Spermine (% change) | 1.019 | 0.995–1.043 | 0.126 | 1.036 | 0.997–1.076 | 0.071 |
| Ornithine (% change) | 1.023 | 0.983–1.064 | 0.263 | 1.037 | 0.964–1.116 | 0.327 |
| Age | 1.012 | 0.916–1.118 | 0.820 | 0.969 | 0.842–1.114 | 0.658 |
| Sex (F/M) | 1.000 | 0.336–2.976 | 1.000 | 0.709 | 0.132–3.815 | 0.689 |
| Surgery Type (hip vs. knee) | 2.879 | 0.948–8.744 | 0.062 | 1.741 | 0.295–10.281 | 0.540 |
| CCI | 1.618 | 0.776–3.372 | 0.199 | 1.431 | 0.425–4.816 | 0.563 |
| Estimated IQ | 0.934 | 0.872–0.999 | 0.047 * | 0.946 | 0.852–1.051 | 0.302 |
| MMSE | 0.711 | 0.528–0.958 | 0.025 * | 0.871 | 0.578–1.311 | 0.507 |
| Aβ42 | 0.995 | 0.992–0.999 | 0.005 ** | 0.994 | 0.989–0.999 | 0.027 * |
| Spermine | Ornithine | |
|---|---|---|
| q-Value | q-Value | |
| Methods and infusions | ||
| Length of surgical time (min) (n = 23) | 1.000 | 1.000 |
| Intraoperative blood loss (mL) (n = 46) | 0.193 | 0.237 |
| Total intraoperative fluid volume (mL) (n = 46) | 0.922 | 0.426 |
| Hartmann’s volume (mL) (n = 41) | 0.930 | 0.930 |
| Tetraspan/gelofusine volume (mL) (n = 39) | 0.477 | 0.736 |
| Premedications | ||
| Multi-premedication (yes/no) (n = 48) | 0.985 | 0.985 |
| PreMed-Ranitidine (yes/no) (n = 48) | 0.878 | 0.878 |
| PreMed-PPI (yes/no) (n = 48) | 0.962 | 0.878 |
| PreMed-Benzodiazepine (yes/no) (n = 48) | 0.975 | 0.970 |
| Anesthesia | ||
| General Anesthesia (yes/no) (n = 54) | 0.385 | 0.242 |
| Perioperative iv midazolam (yes/no) (n = 47) | 0.993 | 0.993 |
| Intraoperative sedation (propofol) (yes/no) (n = 47) | 0.907 | 0.907 |
| Ketamine (yes/no) (n = 48) | 0.138 | 0.887 |
| Painkillers | ||
| Intravenous IV opioid (yes/no) (n = 47) | 0.986 | 0.690 |
| Peripheral nerve block/plexus blockade (yes/no) (n = 47) | 0.571 | 0.040 * |
| Analgesics in recovery (yes/no) (n = 46) | 0.802 | 0.802 |
| Intrathecal diamorphine dose (μg) (n = 48) | 0.913 | 0.976 |
| Antibiotics | ||
| Fluclox (yes/no) (n = 46) | 1.000 | 1.000 |
| Cefuroxime (yes/no) (n = 46) | 0.998 | 0.998 |
| Teicoplanin (yes/no) (n = 46) | 0.967 | 0.967 |
| Gentamicin (yes/no) (n = 46) | 0.994 | 0.994 |
| Others | ||
| Intraoperative tachycardia (yes/no) (n = 45) | 0.581 | 0.134 |
| Intraoperative hypotension (yes/no) (n = 45) | 0.995 | 0.995 |
| Ephedrine (yes/no) (n = 48) | 0.981 | 0.947 |
| Dexamethasone (yes/no) (n = 48) | 0.999 | 0.999 |
| Chlorphenamine (yes/no) (n = 48) | 0.946 | 0.946 |
| Magnesium Sulfate (yes/no) (n = 48) | 0.946 | 0.946 |
| Ondansetron (yes/no) (n = 48) | 0.993 | 0.993 |
| Prochlorperazine (yes/no) (n = 48) | 0.996 | 0.996 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, M.; Pan, X.; Cunningham, E.L.; Passmore, A.P.; McGuinness, B.; McAuley, D.F.; Beverland, D.; O’Brien, S.; Mawhinney, T.; Schott, J.M.; et al. The Influence of Orthopedic Surgery on Circulating Metabolite Levels, and their Associations with the Incidence of Postoperative Delirium. Metabolites 2022, 12, 616. https://doi.org/10.3390/metabo12070616
Jung M, Pan X, Cunningham EL, Passmore AP, McGuinness B, McAuley DF, Beverland D, O’Brien S, Mawhinney T, Schott JM, et al. The Influence of Orthopedic Surgery on Circulating Metabolite Levels, and their Associations with the Incidence of Postoperative Delirium. Metabolites. 2022; 12(7):616. https://doi.org/10.3390/metabo12070616
Chicago/Turabian StyleJung, Mijin, Xiaobei Pan, Emma L. Cunningham, Anthony P. Passmore, Bernadette McGuinness, Daniel F. McAuley, David Beverland, Seamus O’Brien, Tim Mawhinney, Jonathan M. Schott, and et al. 2022. "The Influence of Orthopedic Surgery on Circulating Metabolite Levels, and their Associations with the Incidence of Postoperative Delirium" Metabolites 12, no. 7: 616. https://doi.org/10.3390/metabo12070616
APA StyleJung, M., Pan, X., Cunningham, E. L., Passmore, A. P., McGuinness, B., McAuley, D. F., Beverland, D., O’Brien, S., Mawhinney, T., Schott, J. M., Zetterberg, H., & Green, B. D. (2022). The Influence of Orthopedic Surgery on Circulating Metabolite Levels, and their Associations with the Incidence of Postoperative Delirium. Metabolites, 12(7), 616. https://doi.org/10.3390/metabo12070616