

Salivary Metabolomics in the Diagnosis and Monitoring of Neurodegenerative Dementia



Abstract
:1. Introduction
2. Materials and Methods
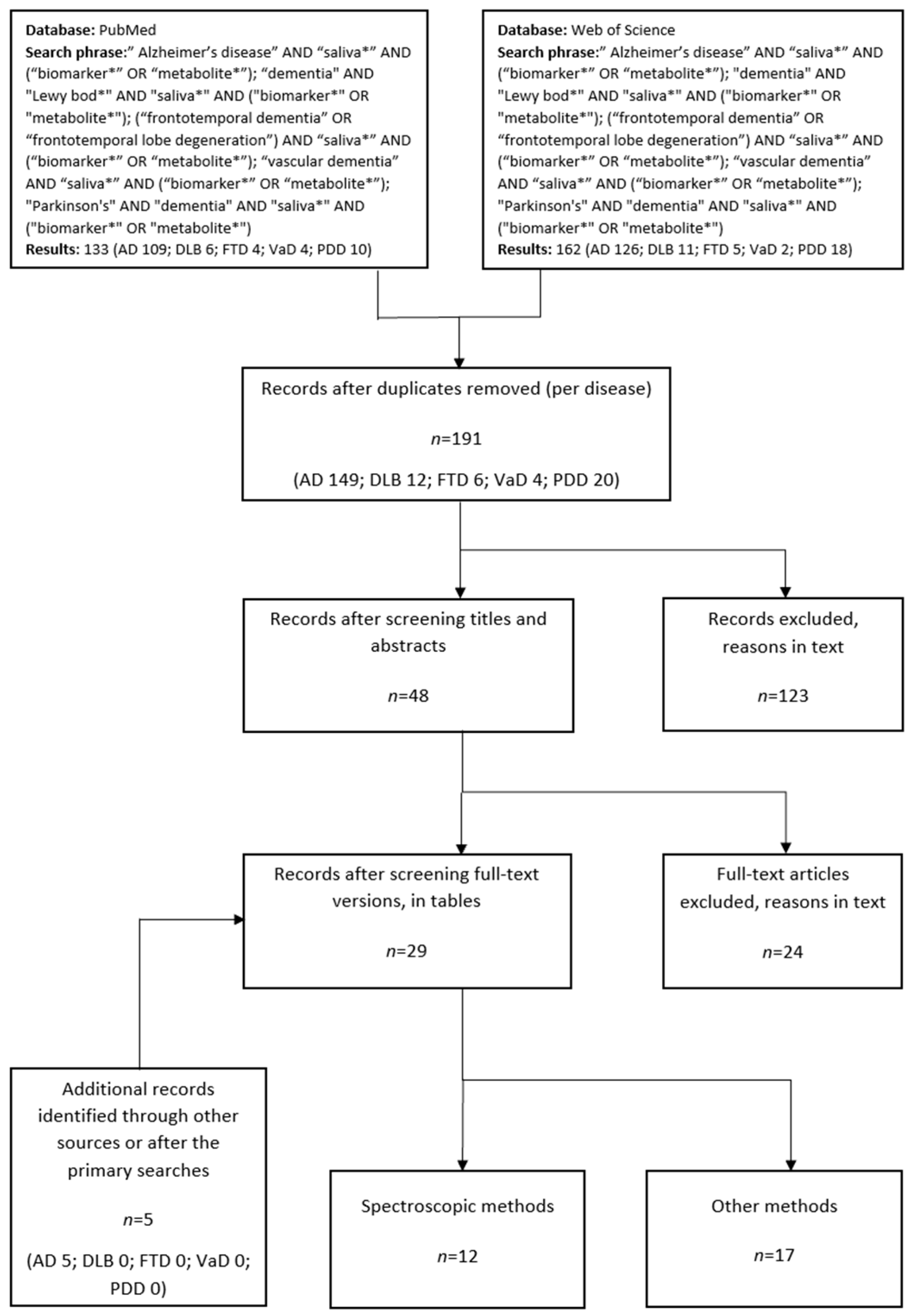
Search Strategy and Study Selection
3. Results

{kind=link}
{kind=link}
| Disease (N) | Method | Metabolites (Elevated/Lowered) | Reference |
|---|---|---|---|
| MCI (8) vs. HC (12) | NMR | acetone, imidazole galactose | [40] |
| MCI (20) vs. HC (20) | LC-FTICR-MS | taurine | [41] |
| MCI (25) vs. HC (25) | FIA-MS/MS | acyl-alkyl phosphatidylcholines | [42] |
| MCI (20) vs. HC (40) | GC-MS | hydroxyphenyl lactate, tyramine, tyrosol cholesterol | [43] |
| MCI (21) vs. HC (19) | LC-MS/MS | transthyretin | [44] |
| MCI (59) vs. HC (131) | MALDI-TOF/TOF MS | lactoferrin | [45] |
| MCI (20)/AD (20) vs. HC (40) | GC-MS | rhamnose, L-tyrosine, L-fucose, L-ornithine, L-aspartate, serotonin | [43] |
| AD (9) vs. HC (12) | NMR | acetone, propionate | [40] |
| AD (116) vs. HC (131) | MALDI-TOF/TOF MS | lactoferrin | [45] |
| AD (21) vs. HC (38) | MALDI-TOF- MS/MS | p-tau/t-tau ratio | [46] |
| AD (29) vs. HC (45) | LC-MS | phenylalanyl-proline, phenylalanyl-phenylalanine, tryptophyl-tyrosine, urocanic acid | [47] |
| AD (256) vs. HC (218) | FUPLC-MS | ornithine, phenyllactic acid, sphinganine-1-phosphate 3-dehydrocarnitine, hypoxanthine, inosine | [48] |
| AD (20) vs. HC (40) | GC-MS | aspartate, ornithine, phenylalanine, pyruvate, tyrosine, putrescine, cholesterol citrate, fumarate, succinate | [43] |
| AD (17) vs. HC (19) | LC-MS/MS | transthyretin | [44] |
| AD (25) vs. HC (25) | FIA-MS/MS | acyl-alkyl phosphatidylcholines | [42] |
| AD (9) vs. MCI (8) | NMR | 5-aminopentanoate, creatine | [40] |
| AD (29) vs. MCI (35) | LC-MS | alanyl-phenylalanine, phenylalanyl-glycine, phenylalanyl-proline | [47] |
| AD (660) vs. MCI (583) | FUPLC-MS | cytidine, L-glutamate, ornithine, phenyllactic acid, pyroglutamate, L-tryptophan, sphinganine-1-phosphate 3-dehydrocarnitine, hypoxanthine, inosine | [49] |
| Dementia (17) (13 AD + 4 VaD) vs. HC (34) | NMR | acetic acid, histamine, propionate dimethyl sulfone, glycerol, succinate, taurine | [36] |
| Dementia (10) (3 AD + 4 FTD + 3 DLB) vs. HC (9) | CE-TOF-MS | arginine, tyrosine | [37] |
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 9 December 2022).
- Reitz, C.; Brayne, C.; Mayeux, R. Epidemiology of Alzheimer disease. Nat. Rev. Neurol. 2011, 7, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Bateman, R.J.; Xiong, C.; Benzinger, T.L.; Fagan, A.M.; Goate, A.; Fox, N.C.; Marcus, D.S.; Cairns, N.J.; Xie, X.; Blazey, T.M.; et al. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N. Engl. J. Med. 2012, 367, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Bloudek, L.M.; Spackman, D.E.; Blankenburg, M.; Sullivan, S.D. Review and meta-analysis of biomarkers and diagnostic imaging in Alzheimer’s disease. J. Alzheimers Dis. 2011, 26, 627–645. [Google Scholar] [CrossRef]
- Palmqvist, S.; Tideman, P.; Cullen, N.; Zetterberg, H.; Blennow, K.; Dage, J.L.; Stomrud, E.; Janelidze, S.; Mattsson-Carlgren, N.; Hansson, O. Prediction of future Alzheimer’s disease dementia using plasma phospho-tau combined with other accessible measures. Nat. Med. 2021, 27, 1034–1042. [Google Scholar] [CrossRef]
- Brookmeyer, R.; Abdalla, N. Estimation of lifetime risks of Alzheimer’s disease dementia using biomarkers for preclinical disease. Alzheimers Dement. 2018, 14, 981–988. [Google Scholar] [CrossRef]
- Dubois, B.; Villain, N.; Frisoni, G.B.; Rabinovici, G.D.; Sabbagh, M.; Cappa, S.; Bejanin, A.; Bombois, S.; Epelbaum, S.; Teichmann, M.; et al. Clinical diagnosis of Alzheimer’s disease: Recommendations of the international working group. Lancet Neurol. 2021, 20, 484–496. [Google Scholar] [CrossRef]
- Solje, E.; Benussi, A.; Buratti, E.; Remes, A.M.; Haapasalo, A.; Borroni, B. State-of-the-art methods and emerging fluid biomarkers in the diagnostics of dementia-a short review and diagnostic algorithm. Diagnostics 2021, 11, 788. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Fábián, T.K.; Hermann, P.; Beck, A.; Fejérdy, P.; Fábián, G. Salivary defense proteins: Their network and role in innate and acquired oral immunity. Int. J. Mol. Sci. 2012, 13, 4295–4320. [Google Scholar] [CrossRef] [PubMed]
- Bardow, A.; Lynge Pedersen, A.M.; Nauntofte, B. Saliva. In Clinical Oral Physiology, 1st ed.; Miles, T.S., Nauntofte, B., Svensson, P., Eds.; Quintessence Publishing Co. Ltd.: Copenhagen, Denmark, 2004; pp. 17–51. [Google Scholar]
- Gardner, A.; Parkes, H.G.; So, P.W.; Carpenter, G.H. Determining bacterial and host contributions to the human salivary metabolome. J. Oral Microbiol. 2019, 11, 1617014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyvärinen, E.; Savolainen, M.; Mikkonen, J.J.W.; Kullaa, A.M. Salivary metabolomics for diagnosis and monitoring diseases: Challenges and possibilities. Metabolites 2021, 11, 587. [Google Scholar] [CrossRef]
- Isenman, L.; Liebow, C.; Rothman, S. The endocrine secretion of mammalian digestive enzymes by exocrine glands. Am. J. Physiol. 1999, 276, E223–E232. [Google Scholar] [CrossRef] [PubMed]
- Mikkonen, J.J.W.; Singh, S.P.; Akhi, R.; Salo, T.; Lappalainen, R.; González-Arriagada, W.A.; Ajudarte Lopes, M.; Kullaa, A.M.; Myllymaa, S. Potential role of nuclear magnetic resonance spectroscopy to identify salivary metabolite alterations in patients with head and neck cancer. Oncol. Lett. 2018, 16, 6795–6800. [Google Scholar] [CrossRef] [PubMed]
- Carlomagno, C.; Bertazioli, D.; Gualerzi, A.; Picciolini, S.; Andrico, M.; Rodà, F.; Meloni, M.; Banfi, P.I.; Verde, F.; Ticozzi, N.; et al. Identification of the raman salivary fingerprint of Parkinson’s disease through the spectroscopic-computational combinatory approach. Front. Neurosci. 2021, 15, 704963. [Google Scholar] [CrossRef]
- Mikkonen, J.J.W.; Raittila, J.; Rieppo, L.; Lappalainen, R.; Kullaa, A.M.; Myllymaa, S. Fourier transform infrared spectroscopy and photoacoustic spectroscopy for saliva analysis. Appl. Spectrosc. 2016, 70, 1502–1510. [Google Scholar] [CrossRef]
- Gleerup, H.S.; Sanna, F.; Høgh, P.; Simrén, J.; Blennow, K.; Zetterberg, H.; Hasselbalch, S.G.; Ashton, N.J.; Simonsen, A.H. Saliva neurofilament light chain is not a diagnostic biomarker for neurodegeneration in a mixed memory clinic population. Front. Aging Neurosci. 2021, 13, 659898. [Google Scholar] [CrossRef]
- Sabbagh, M.N.; Shi, J.; Lee, M.; Arnold, L.; Al-Hasan, Y.; Heim, J.; McGeer, P. Salivary beta amyloid protein levels are detectable and differentiate patients with Alzheimer’s disease dementia from normal controls: Preliminary findings. BMC Neurol. 2018, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Pareja, F.; Antequera, D.; Vargas, T.; Molina, J.A.; Carro, E. Saliva levels of Abeta1-42 as potential biomarker of Alzheimer’s disease: A pilot study. BMC Neurol. 2010, 10, 108. [Google Scholar] [CrossRef]
- Lee, M.; Guo, J.P.; Kennedy, K.; McGeer, E.G.; McGeer, P.L. A method for diagnosing Alzheimer’s disease based on salivary amyloid-β protein 42 levels. J. Alzheimers Dis. 2017, 55, 1175–1182. [Google Scholar] [CrossRef]
- Cui, Y.; Zhang, H.; Zhu, J.; Liao, Z.; Wang, S.; Liu, W. Investigation of whole and glandular saliva as a biomarker for Alzheimer’s disease diagnosis. Brain Sci. 2022, 12, 595. [Google Scholar] [CrossRef]
- Santos, G.A.A.; Olave, E.; Pardi, P.C. Salivary biomarkers in Alzheimer’s disease. Int. J. Morphol. 2020, 38, 230–234. [Google Scholar] [CrossRef]
- Tvarijonaviciute, A.; Zamora, C.; Ceron, J.J.; Bravo-Cantero, A.F.; Pardo-Marin, L.; Valverde, S.; Lopez-Jornet, P. Salivary biomarkers in Alzheimer’s disease. Clin. Oral Investig. 2020, 24, 3437–3444. [Google Scholar] [CrossRef] [PubMed]
- Marksteiner, J.; Defrancesco, M.; Humpel, C. Saliva tau and phospho-tau-181 measured by Lumipulse in patients with Alzheimer’s disease. Front. Aging Neurosci. 2022, 14, 1014305. [Google Scholar] [CrossRef] [PubMed]
- Pekeles, H.; Qureshi, H.Y.; Paudel, H.K.; Schipper, H.M.; Gornistky, M.; Chertkow, H. Development and validation of a salivary tau biomarker in Alzheimer’s disease. Alzheimers Dement. (Amst). 2018, 11, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Pukhalskaia, A.E.; Dyatlova, A.S.; Linkova, N.S.; Kozlov, K.L.; Kvetnaia, T.V.; Koroleva, M.V.; Kvetnoy, I.M. Sirtuins as possible predictors of aging and Alzheimer’s disease development: Verification in the hippocampus and saliva. Bull. Exp. Biol. Med. 2020, 169, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Zalewska, A.; Klimiuk, A.; Zięba, S.; Wnorowska, O.; Rusak, M.; Waszkiewicz, N.; Szarmach, I.; Dzierżanowski, K.; Maciejczyk, M. Salivary gland dysfunction and salivary redox imbalance in patients with Alzheimer’s disease. Sci. Rep. 2021, 11, 23904. [Google Scholar] [CrossRef]
- de la Rubia Ortí, J.E.; Sancho Castillo, S.; Benlloch, M.; Julián Rochina, M.; Corchón Arreche, S.; García-Pardo, M.P. Impact of the relationship of stress and the immune system in the appearance of Alzheimer’s disease. J. Alzheimers Dis. 2017, 55, 899–903. [Google Scholar] [CrossRef]
- Gómez-Gallego, M.; Gómez-García, J. Effects of stress on emotional memory in patients with Alzheimer’s disease and in healthy elderly. Int. Psychogeriatr. 2018, 30, 1199–1209. [Google Scholar] [CrossRef]
- Ashton, N.J.; Ide, M.; Schöll, M.; Blennow, K.; Lovestone, S.; Hye, A.; Zetterberg, H. No association of salivary total tau concentration with Alzheimer’s disease. Neurobiol. Aging 2018, 70, 125–127. [Google Scholar] [CrossRef]
- Katsipis, G.; Tzekaki, E.E.; Tsolaki, M.; Pantazaki, A.A. Salivary GFAP as a potential biomarker for diagnosis of mild cognitive impairment and Alzheimer’s disease and its correlation with neuroinflammation and apoptosis. J. Neuroimmunol. 2021, 361, 577744. [Google Scholar] [CrossRef]
- Kim, C.B.; Choi, Y.Y.; Song, W.K.; Song, K.B. Antibody-based magnetic nanoparticle immunoassay for quantification of Alzheimer’s disease pathogenic factor. J. Biomed. Opt. 2014, 19, 051205. [Google Scholar] [CrossRef] [PubMed]
- González-Sánchez, M.; Bartolome, F.; Antequera, D.; Puertas-Martín, V.; González, P.; Gómez-Grande, A.; Llamas-Velasco, S.; Herrero-San Martín, A.; Pérez-Martínez, D.; Villarejo-Galende, A.; et al. Decreased salivary lactoferrin levels are specific to Alzheimer’s disease. EBioMedicine 2020, 57, 102834. [Google Scholar] [CrossRef]
- Gleerup, H.S.; Jensen, C.S.; Høgh, P.; Hasselbalch, S.G.; Simonsen, A.H. Lactoferrin in cerebrospinal fluid and saliva is not a diagnostic biomarker for Alzheimer’s disease in a mixed memory clinic population. EBioMedicine 2021, 67, 103361. [Google Scholar] [CrossRef]
- Figueira, J.; Jonsson, P.; Nordin Adolfsson, A.; Adolfsson, R.; Nyberg, L.; Öhman, A. NMR analysis of the human saliva metabolome distinguishes dementia patients from matched controls. Mol. Biosyst. 2016, 12, 2562–2571. [Google Scholar] [CrossRef] [PubMed]
- Tsuruoka, M.; Hara, J.; Hirayama, A.; Sugimoto, M.; Soga, T.; Shankle, W.R.; Tomita, M. Capillary electrophoresis-mass spectrometry-based metabolome analysis of serum and saliva from neurodegenerative dementia patients. Electrophoresis 2013, 34, 2865–2872. [Google Scholar] [CrossRef]
- Kumari, S.; Goyal, V.; Kumaran, S.S.; Dwivedi, S.N.; Srivastava, A.; Jagannathan, N.R. Quantitative metabolomics of saliva using proton NMR spectroscopy in patients with Parkinson’s disease and healthy controls. Neurol. Sci. 2020, 41, 1201–1210. [Google Scholar] [CrossRef]
- Figura, M.; Sitkiewicz, E.; Świderska, B.; Milanowski, Ł.; Szlufik, S.; Koziorowski, D.; Friedman, A. Proteomic profile of saliva in Parkinson’s disease patients: A proof of concept study. Brain Sci. 2021, 11, 661. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Geddes, T.; Han, B.; Bahado-Singh, R.O.; Wilson, G.D.; Imam, K.; Maddens, M.; Graham, S.F. Diagnostic biomarkers of Alzheimer’s disease as identified in saliva using 1H NMR-based metabolomics. J. Alzheimers Dis. 2017, 58, 355–359. [Google Scholar] [CrossRef]
- Zheng, J.; Dixon, R.A.; Li, L. Development of isotope labeling LC-MS for human salivary metabolomics and application to profiling metabolome changes associated with mild cognitive impairment. Anal. Chem. 2012, 84, 10802–10811. [Google Scholar] [CrossRef]
- Marksteiner, J.; Oberacher, H.; Humpel, C. Acyl-alkyl-phosphatidlycholines are decreased in saliva of patients with Alzheimer’s disease as identified by targeted metabolomics. J. Alzheimers Dis. 2019, 68, 583–589. [Google Scholar] [CrossRef]
- François, M.; Karpe, A.; Liu, J.W.; Beale, D.; Hor, M.; Hecker, J.; Faunt, J.; Maddison, J.; Johns, S.; Doecke, J.; et al. Salivaomics as a potential tool for predicting Alzheimer’s disease during the early stages of neurodegeneration. J. Alzheimers Dis. 2021, 82, 1301–1313. [Google Scholar] [CrossRef] [PubMed]
- Eldem, E.; Barve, A.; Sallin, O.; Foucras, S.; Annoni, J.M.; Schmid, A.W.; Alberi Auber, L. Salivary proteomics identifies transthyretin as a biomarker of early dementia conversion. J. Alzheimers Dis. Rep. 2022, 6, 31–41. [Google Scholar] [CrossRef]
- Carro, E.; Bartolomé, F.; Bermejo-Pareja, F.; Villarejo-Galende, A.; Molina, J.A.; Ortiz, P.; Calero, M.; Rabano, A.; Cantero, J.L.; Orive, G. Early diagnosis of mild cognitive impairment and Alzheimer’s disease based on salivary lactoferrin. Alzheimers Dement (Amst). 2017, 8, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Sui, Y.T.; Peskind, E.R.; Li, G.; Hwang, H.; Devic, I.; Ginghina, C.; Edgar, J.S.; Pan, C.; Goodlett, D.R.; et al. Salivary tau species are potential biomarkers of Alzheimer’s disease. J. Alzheimers Dis. 2011, 27, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Huan, T.; Tran, T.; Zheng, J.; Sapkota, S.; MacDonald, S.W.; Camicioli, R.; Dixon, R.A.; Li, L. Metabolomics analyses of saliva detect novel biomarkers of Alzheimer’s disease. J. Alzheimers Dis. 2018, 65, 1401–1416. [Google Scholar] [CrossRef]
- Liang, Q.; Liu, H.; Zhang, T.Y.; Jiang, Y.; Xing, H.T.; Zhang, A.H. Metabolomics-based screening of salivary biomarkers for early diagnosis of Alzheimer’s disease. RSC Adv. 2015, 5, 96074–96079. [Google Scholar] [CrossRef]
- Liang, Q.; Liu, H.; Li, X.; Zhang, A.H. High-throughput metabolomics analysis discovers salivary biomarkers for predicting mild cognitive impairment and Alzheimer’s disease. RSC Adv. 2016, 6, 75499–75504. [Google Scholar] [CrossRef]
- Padovani, A.; Benussi, A.; Cantoni, V.; Dell’Era, V.; Cotelli, M.S.; Caratozzolo, S.; Turrone, R.; Rozzini, L.; Alberici, A.; Altomare, D.; et al. Diagnosis of mild cognitive impairment due to Alzheimer’s disease with transcranial magnetic stimulation. J. Alzheimers Dis. 2018, 65, 221–230. [Google Scholar] [CrossRef]
- Bear, M.F.; Connors, B.W.; Paradiso, M.A. (Eds.) Neurotransmitter systems. In Neuroscience: Exploring the Brain, 4th ed.; Wolters Kluwer Ltd.: Philadelphia, PA, USA, 2016; pp. 143–178. [Google Scholar]
- Berger, M.; Gray, J.A.; Roth, B.L. The expanded biology of serotonin. Annu. Rev. Med. 2009, 60, 355–366. [Google Scholar] [CrossRef]
- Cueno, M.E.; Ochiai, K. Gingival periodontal disease (PD) level-butyric acid affects the systemic blood and brain organ: Insights into the systemic inflammation of periodontal disease. Front Immunol. 2018, 9, 1158. [Google Scholar] [CrossRef]
- Leira, Y.; Domínguez, C.; Seoane, J.; Seoane-Romero, J.; Pías-Peleteiro, J.M.; Takkouche, B.; Blanco, J.; Aldrey, J.M. Is periodontal disease associated with Alzheimer’s disease? A systematic review with meta-analysis. Neuroepidemiology 2017, 48, 21–31. [Google Scholar] [CrossRef]
- Holmer, J.; Eriksdotter, M.; Schultzberg, M.; Pussinen, P.J.; Buhlin, K. Association between periodontitis and risk of Alzheimer’s disease, mild cognitive impairment and subjective cognitive decline: A case-control study. J. Clin. Periodontol. 2018, 45, 1287–1298. [Google Scholar] [CrossRef]
- Asher, S.; Stephen, R.; Mäntylä, P.; Suominen, A.L.; Solomon, A. Periodontal health, cognitive decline, and dementia: A systematic review and meta-analysis of longitudinal studies. J. Am. Geriatr. Soc. 2022, 70, 2695–2709. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.B.; Keating, D.J.; Young, R.L.; Wong, M.L.; Licinio, J.; Wesselingh, S. From gut dysbiosis to altered brain function and mental illness: Mechanisms and pathways. Mol. Psychiatry 2016, 21, 738–748. [Google Scholar] [CrossRef]
- Macfarlane, S.; Macfarlane, G.T. Regulation of short-chain fatty acid production. Proc. Nutr. Soc. 2003, 62, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Kimura, I.; Ichimura, A.; Ohue-Kitano, R.; Igarashi, M. Free fatty acid receptors in health and disease. Physiol. Rev. 2020, 100, 171–210. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M.; Romano, F.; Guzzi, N.; Carnevale, G. Full-mouth disinfection and systemic antimicrobial therapy in generalized aggressive periodontitis: A randomized, placebo-controlled trial. J. Clin. Periodontol. 2012, 39, 284–294. [Google Scholar] [CrossRef]
- Rzeznik, M.; Triba, M.N.; Levy, P.; Jungo, S.; Botosoa, E.; Duchemann, B.; Le Moyec, L.; Bernaudin, J.F.; Savarin, P.; Guez, D. Identification of a discriminative metabolomic fingerprint of potential clinical relevance in saliva of patients with periodontitis using 1H nuclear magnetic resonance (NMR) spectroscopy. PLoS ONE 2017, 12, e0182767. [Google Scholar] [CrossRef]
- Louzada, P.R.; Paula Lima, A.C.; Mendonca-Silva, D.L.; Noël, F.; De Mello, F.G.; Ferreira, S.T. Taurine prevents the neurotoxicity of beta-amyloid and glutamate receptor agonists: Activation of GABA receptors and possible implications for Alzheimer’s disease and other neurological disorders. FASEB J. 2004, 18, 511–518. [Google Scholar] [CrossRef]
- Eissa, N.; Sadeq, A.; Sasse, A.; Sadek, B. Role of neuroinflammation in autism spectrum disorder and the emergence of brain histaminergic system. Lessons also for BPSD? Front. Pharmacol. 2020, 11, 886. [Google Scholar] [CrossRef]
- Huang, H.; Li, Y.; Liang, J.; Finkelman, F.D. Molecular regulation of histamine synthesis. Front. Immunol. 2018, 9, 1392. [Google Scholar] [CrossRef] [PubMed]
- Figueira, J.; Gouveia-Figueira, S.; Öhman, C.; Lif Holgerson, P.; Nording, M.L.; Öhman, A. Metabolite quantification by NMR and LC-MS/MS reveals differences between unstimulated, stimulated, and pure parotid saliva. J. Pharm. Biomed. Anal. 2017, 140, 295–300. [Google Scholar] [CrossRef] [PubMed]


| Disease | Metabolites (Elevated/No Association/Lowered) | Method |
|---|---|---|
| AD | amyloid-β42 | ELISA [19,20,21,22] |
| AD | amyloid-β42 | ELISA [23] |
| AD | amyloid-β42 | Luminex assay [24] |
| AD | complement C4 | Luminex assay [24] |
| AD | t-tau | ELISA [23] Lumipulse technology [25] |
| AD | p-tau/t-tau ratio | Antibodies + Western Blot analysis [26] ELISA [22] |
| AD | SIRT1, SIRT3, SIRT6 | ELISA [27] |
| AD | glutathione | Colorimetric method [28] |
| AD | IgA | ELISA [29] |
| AD | cortisol | ELISA [29] |
| AD | cortisol | RIA [30] |
| AD, MCI | t-tau | Single molecule array [31] |
| AD, MCI | GFAP | ELISA [32] quantitative Dot Blot analysis [32] SDS-PAGE + Western Blot analysis [32] |
| AD, MCI | amyloid-β42 | Magnetoimmunoassay [33] |
| AD, FTD | lactoferrin | ELISA [34] |
| AD, MCI, FTD, DLB, VaD, PDD | lactoferrin | ELISA [35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyvärinen, E.; Solje, E.; Vepsäläinen, J.; Kullaa, A.; Tynkkynen, T. Salivary Metabolomics in the Diagnosis and Monitoring of Neurodegenerative Dementia. Metabolites 2023, 13, 233. https://doi.org/10.3390/metabo13020233
Hyvärinen E, Solje E, Vepsäläinen J, Kullaa A, Tynkkynen T. Salivary Metabolomics in the Diagnosis and Monitoring of Neurodegenerative Dementia. Metabolites. 2023; 13(2):233. https://doi.org/10.3390/metabo13020233
Chicago/Turabian StyleHyvärinen, Eelis, Eino Solje, Jouko Vepsäläinen, Arja Kullaa, and Tuulia Tynkkynen. 2023. "Salivary Metabolomics in the Diagnosis and Monitoring of Neurodegenerative Dementia" Metabolites 13, no. 2: 233. https://doi.org/10.3390/metabo13020233
APA StyleHyvärinen, E., Solje, E., Vepsäläinen, J., Kullaa, A., & Tynkkynen, T. (2023). Salivary Metabolomics in the Diagnosis and Monitoring of Neurodegenerative Dementia. Metabolites, 13(2), 233. https://doi.org/10.3390/metabo13020233