

Serum Metabolomic Profiles in Critically Ill Patients with Shock on Admission to the Intensive Care Unit


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Healthy Volunteers
2.2. Metabolomic Studies
2.3. Proton Nuclear Magnetic Resonance (1H-NMR)
2.4. Biological Data and Treatments
3. Statistics
4. Results
4.1. Biological Data and Treatments
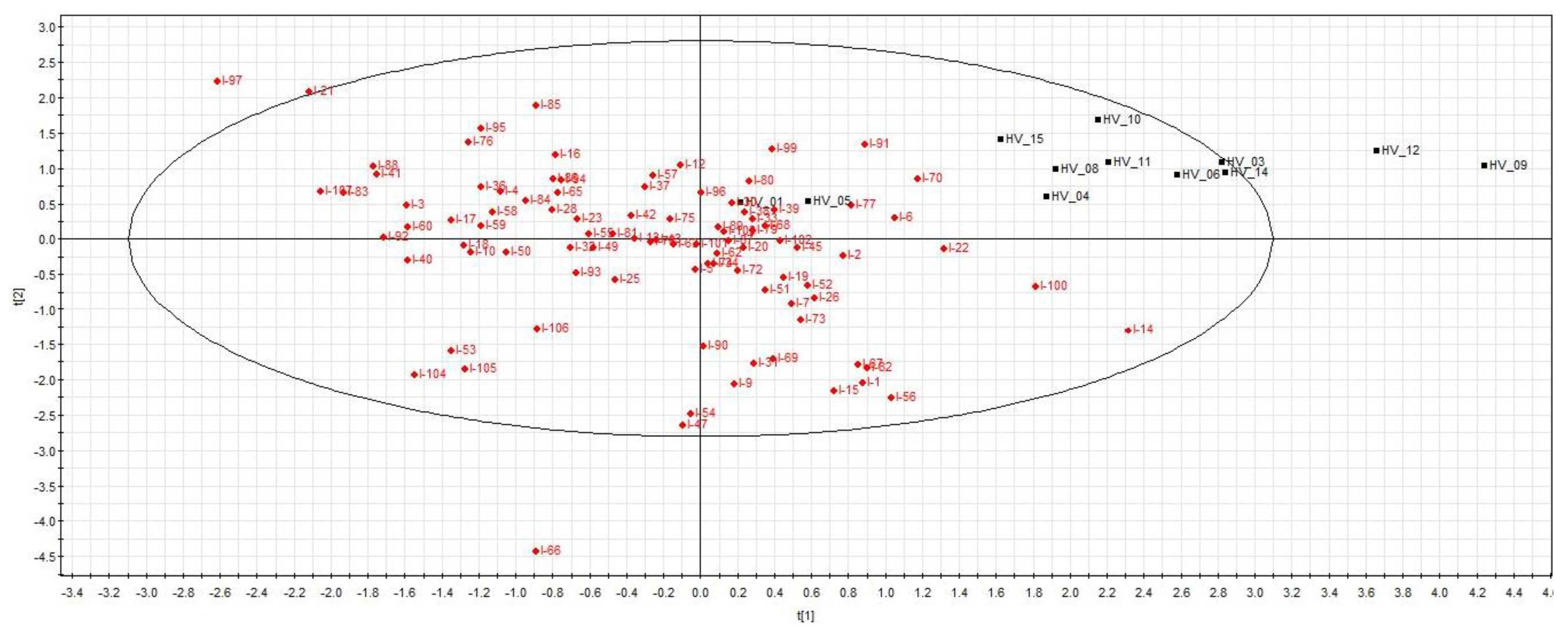
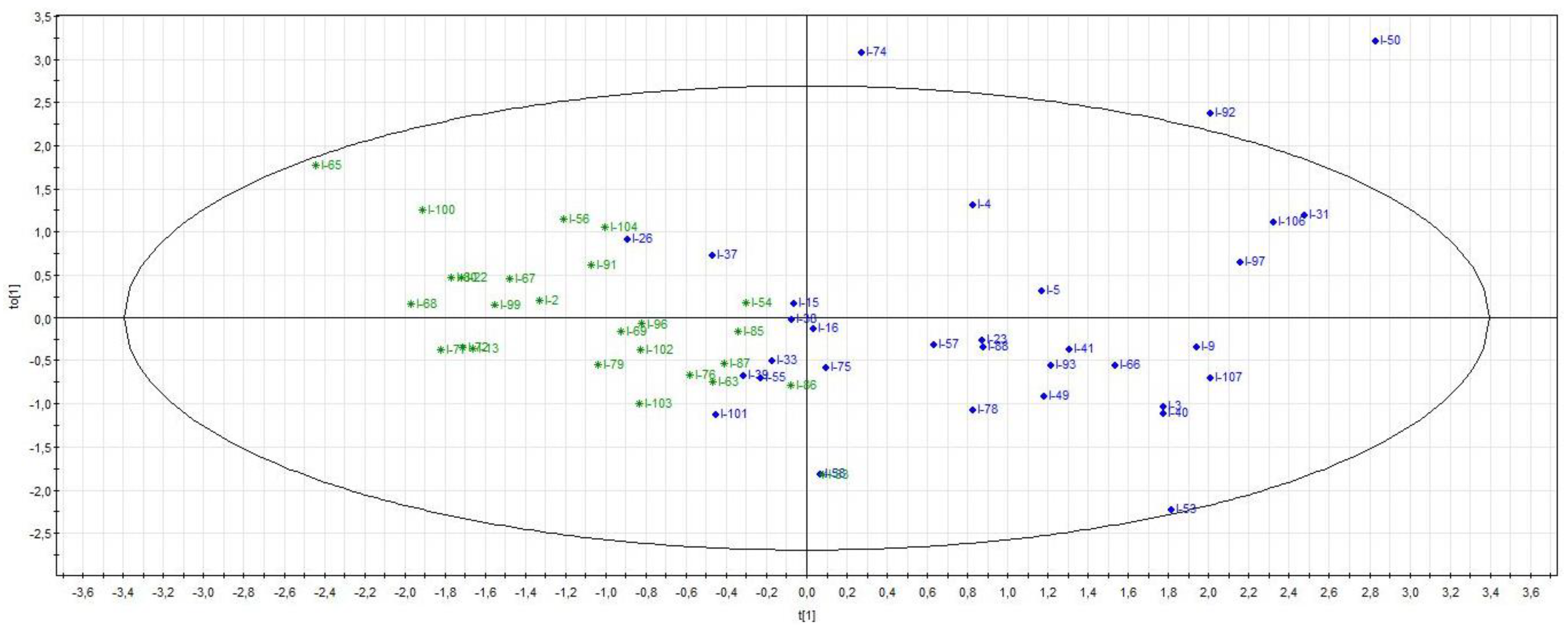
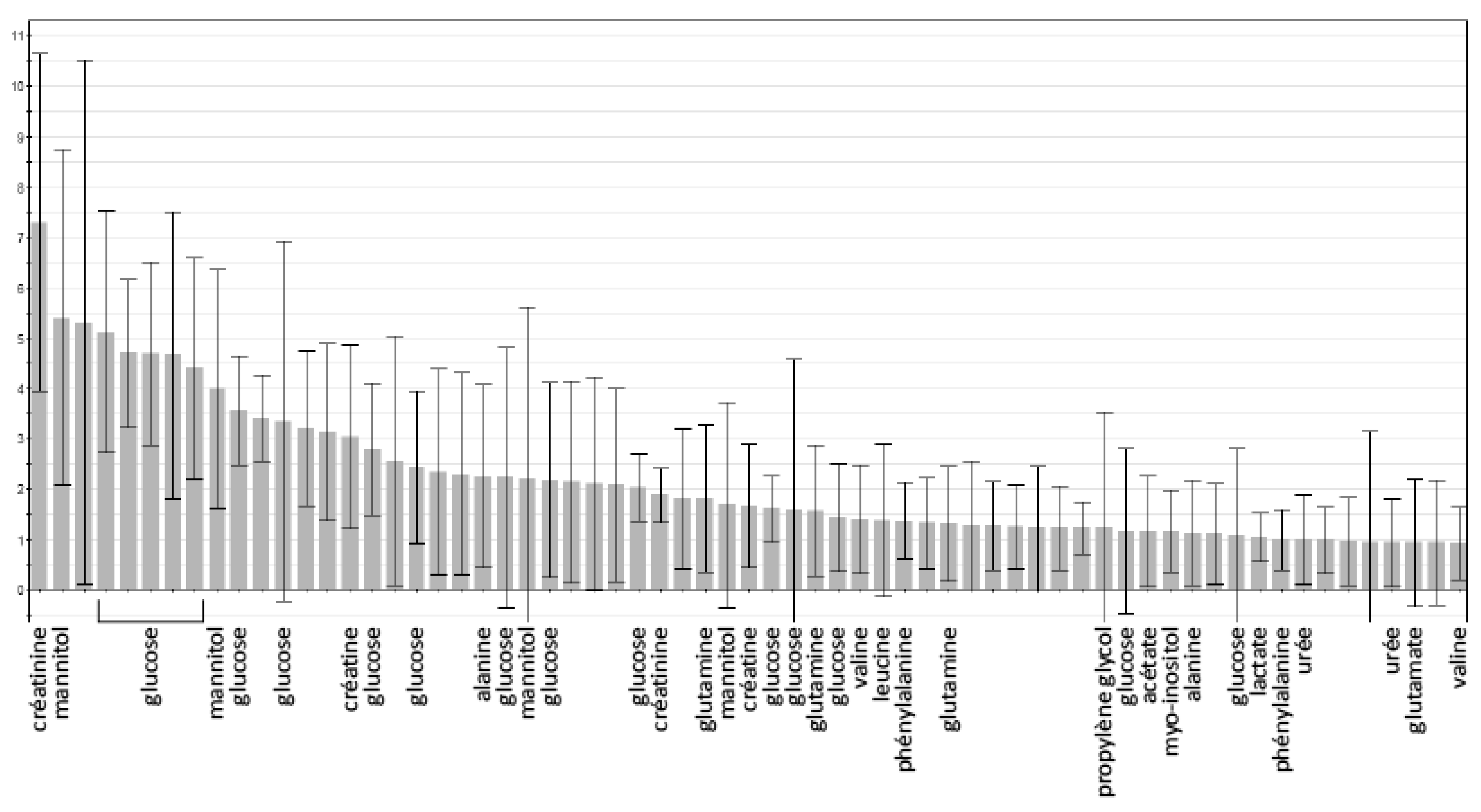
4.2. Metabolomic Studies
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Preiser, J.C.; Ichai, C.; Orban, J.C. Groeneveld ABJ: Metabolic response to the stress of critical illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef]
- Nicholson, J.K.; Lindon, J.C.; Holmes, E. “Metabonomics”: Understanding the metabolomic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica 1999, 29, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Hill, D.W.; Petty, N.M.; Melchert, R.B.; Luo, B.; Grant, D.F.; Dey, D.K. Statistical approach to metabonomic analysis of rat urine following surgical trauma. J. Chemom. 2006, 20, 87–98. [Google Scholar] [CrossRef]
- Serkova, N.J.; Van Rheen, Z.; Tobias, M.; Pitzer, J.E.; Wilkinson, J.E.; Stringer, K.A. Utility of magnetic resonance imaging and nuclear magnetic resonance-based metabolomics for quantification of inflammatory lung injury. Am. J. Physiol. Cell. Mol. Physiol. 2008, 295, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.-Y.; Xu, P.-B.; Yan, S.-K.; Meng, H.-B.; Yang, G.-J.; Dai, W.-X.; Liu, X.-R.; Li, J.-B.; Deng, X.-M.; Zhang, W.-D. A metabonomic approach to early prognostic evaluation of experimental sepsis by1H NMR and pattern recognition. NMR Biomed. 2009, 22, 601–608. [Google Scholar] [CrossRef]
- Hussain, H.; Vutipongsatorn, K.; Jiménez, B.; Antcliffe, D.B. Patient Stratification in Sepsis: Using Metabolomics to Detect Clinical Phenotypes, Sub-Phenotypes and Therapeutic Response. Metabolites 2022, 12, 376. [Google Scholar] [CrossRef]
- Cohen, M.J.; Serkova, N.J.; Wiener-Kronish, J.; Pittet, J.F. Niemann CU. 1H-NMR-based metabolic signatures of clinical outcomes in trauma patients-beyond lactate and base excess. J. Trauma 2010, 69, 31–40. [Google Scholar]
- Stringer, K.A.; Serkova, N.J.; Karnovsky, A.; Guire, K.; Paine, R.; Standiford, T.J. Metabolic consequences of sepsis-induced acute lung injury revealed by plasma 1H-nuclear magnetic resonance quantitative metabolomics and computational analysis. Am. J. Physiol. Lung Cell Mol. Physiol. 2011, 300, L4–L11. [Google Scholar] [CrossRef]
- Mickiewicz, B.; Duggan, G.E.; Winston, B.W.; Doig, C.; Kubes, P.; Vogel, H.J.; Alberta Sepsis Network. Metabolic Profiling of Serum Samples by 1H Nuclear Magnetic Resonance Spectroscopy as a Potential Diagnostic Approach for Septic Shock. Crit. Care Med. 2014, 42, 1140–1149. [Google Scholar] [CrossRef]
- Mearelli, F.; Fiotti, N.; Giansante, C.; Casarsa, C.; Orso, D.; De Helmersen, M.; Altamura, N.; Ruscio, M.; Castello, L.M.; Colonetti, E.; et al. Derivation and validation of a biomarker-based clinical algorithm to rule out sepsis from non-infectious systemic inflammatory response syndrome at emergency department admission: A multicenter prospective study. Crit. Care Med. 2018, 46, 1421–1429. [Google Scholar] [CrossRef]
- Ferrer, R.; Martin-Loeches, I.; Phillips, G.; Osborn, T.M.; Townsend, S.; Dellinger, R.P.; Artigas, A.; Schorr, C.; Levy, M.M. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: Results from a guideline-based performance improvement program. Crit. Care Med. 2014, 42, 1749–1755. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Worley, B.; Powers, R. Multivariate analysis in metabolomics. Curr. Metab. 2013, 1, 92–107. [Google Scholar]
- Revelly, J.-P.; Tappy, L.; Martinez, A.; Bollmann, M.; Cayeux, M.-C.; Berger, M.M.; Chioléro, R.L. Lactate and glucose metabolism in severe sepsis and cardiogenic shock. Crit. Care Med. 2005, 33, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Bellomo, R. Stress hyperglycemia: An essential survival response! Crit. Care 2013, 17, 305. [Google Scholar] [CrossRef] [PubMed]
- Klaude, M.; Fredriksson, K.; Tjäder, I.; Hammarqvist, F.; Ahlman, B.; Rooyackers, O.; Wernerman, J. Proteasome proteolytic activity in skeletal muscle is increased in patients with sepsis. Clin. Sci. 2007, 112, 499–506. [Google Scholar] [CrossRef]
- Su, L.; Li, H.; Xie, A.; Liu, D.; Rao, W.; Lan, L.; Li, X.; Li, F.; Xiao, K.; Wang, H.; et al. Dynamic Changes in Amino Acid Concentration Profiles in Patients with Sepsis. PLoS ONE 2015, 10, e0121933. [Google Scholar] [CrossRef]
- Izquierdo-García, J.L.; Nin, N.; Ruíz-Cabello, J.; Rojas, Y.; de Paula, M.; López-Cuenca, S.; Morales, L.; Martínez-Caro, L.; Fernández-Segoviano, P.; Esteban, A.; et al. A metabolomic approach for diagnosis of experimental sepsis. Intensiv. Care Med. 2011, 37, 2023–2032. [Google Scholar] [CrossRef]
- Kopterides, P.; Nikitas, N.; Vassiliadi, D.; Orfanos, S.E.; Theodorakopoulou, M.; Ilias, I.; Boutati, E.; Dimitriadis, G.; Maratou, E.; Diamantakis, A.; et al. Microdialysis-assessed interstitium alterations during sepsis: Relationship to stage, infection and pathogen. Intensive Care Med. 2011, 37, 1756–1764. [Google Scholar] [CrossRef]
- Mickiewicz, B.; Tam, P.; Jenne, C.N.; Leger, C.; Wopng, J.; Winston, B.W.; Doig, C.; Kubes, P.; Vogel, H.J. Alberta Sepsis Network. Integration of metabolic and inflammatory mediator profiles as a potential prognostic approach for septic shock in the intensive care unit. Crit. Care 2015, 19, 11. [Google Scholar] [CrossRef]
- Chung, K.-P.; Chen, G.-Y.; Chuang, T.-Y.; Huang, Y.T.; Chen, Y.F.; Liu, W.L.; Chren, Y.J.; Hsu, C.L.; Huang, M.T.; Kuo, C.H.; et al. Increased plasma acetylcarnitine in sepsis is associated with multiple organ dysfunction and mortality: A multicenter cohort study. Crit. Care Med. 2019, 47, 210–218. [Google Scholar] [CrossRef]
- Jennaro, T.S.; Puskarich, M.; McCann, M.R.; Gillies, C.E.; Pai, M.P.; Karnovsky, A.; Evans, C.R.; Jones, A.E.; Stringer, K.A. Using l -Carnitine as a Pharmacologic Probe of the Interpatient and Metabolic Variability of Sepsis. Pharmacotherapy 2020, 40, 913–923. [Google Scholar] [CrossRef]
- Sotoda, Y.; Negoro, M.; Wakabayashi, I. Involvement of decreased myo-inositol transport in lipopolysaccharide-induced depression of phosphoinositide hydrolysis in vascular smooth muscle. FEBS Lett. 2002, 519, 227–230. [Google Scholar] [CrossRef]
- Sjöberg, R.L.; Bergenheim, T.; Mören, L.; Antti, H.; Lindgren, C.; Naredi, S.; Lindvall, P. Blood metabolomic predictors of 1-year outcome in subarachnoid hemorrhage. Neurocrit. Care 2015, 23, 225–232. [Google Scholar] [CrossRef]
- Seymour, C.W.; Yende, S.; Scott, M.J.; Pribis, J.; Mohney, R.P.; Bell, L.N.; Chen, Y.F.; Zuckerbraun, B.S.; Bigbee, W.L.; Yealy, D.M.; et al. Metabolomics in pneumonia and sepsis: An anlysis of the GenIMS cohort study. Intensive Care Med. 2013, 39, 1423–1434. [Google Scholar] [CrossRef]
- D’Alessandro, A.; Slaughter, A.L.; Peltz, E.D.; Moore, E.E.; Silliman, C.C.; Wither, M.; Nemkov, T.; Bacon, A.W.; Fragoso, M.; Banerjee, A.; et al. Trauma/hemorrhagic shock investigates aberrant metabolic flux through glycolytic pathways, as revealed by preliminary (13)C-glucose labeling metabolomics. J. Transl. Med. 2015, 13, 253. [Google Scholar] [CrossRef]
- Garcia-Simon, M.; Morales, J.M.; Modesto-Alapont, V.; Gonzalez-Marrachelli, V.; Vento-Rehues, R.; Jorda-Miñana, A.; Blanquer-Olivas, J.; Monleon, D. Prognosis Biomarkers of Severe Sepsis and Septic Shock by 1H NMR Urine Metabolomics in the Intensive Care Unit. PLoS ONE 2015, 10, e0140993. [Google Scholar] [CrossRef]
- Mickiewicz, B.; Vogel, H.J.; Wong, H.R.; Winston, B.W. Metabolomics as a Novel Approach for Early Diagnosis of Pediatric Septic Shock and Its Mortality. Am. J. Respir. Crit. Care Med. 2013, 187, 967–976. [Google Scholar] [CrossRef]
- Mao, H.; Wang, H.; Wang, B.; Liu, X.; Gao, H.; Xu, M.; Zhao, H.; Deng, X.; Lin, D. Systemic Metabolic Changes of Traumatic Critically Ill Patients Revealed by an NMR-Based Metabonomic Approach. J. Proteome Res. 2009, 8, 5423–5430. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Chen, J.; Liang, Q.; Zheng, H.; Ye, Y.; Nan, W.; Zhang, X.; Gao, H.; Li, Y. Metabolomics profile in acute respiratory distress syndrome by nuclear magnetic resonance spectroscopy in patients with community-acquired pneumonia. Respir. Res. 2022, 23, 172. [Google Scholar] [CrossRef] [PubMed]
- Choong See, K. Personalizing care for critically ill adults using omics: A concise review of potential clinical applications. Cells 2023, 12, 541. [Google Scholar]
- Stringer, K.A.; Younger, J.G.; McHugh, C.; Yeomans, L.; Finkel, M.A.; Puskarich, M.A.; Jones, A.E.; Trexel, J.; Karnovsky, A. Whole blood reveals more metabolic detail of the human metabolome than serum as measured by 1H-NMR spectroscopy: Implications for sepsis metabolomics. Shock 2015, 44, 200–208. [Google Scholar] [CrossRef]
- Amathieu, R.; Legrand, M. Metabolomics in anesthesiology and critical care: Time for the big leap? Ann. Fr. Anesth. Reanim. 2014, 33, 155–157. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Value |
|---|---|
| Age (years) | 67 ± 14 |
| Male/Female | 58/52 |
| BMI | 27.4 ± 7.3 |
| SOFA Score | 6 ± 3 |
| APACHE II Score | 20 ± 9 |
| Groups | |
| Sepsis, n (%) | 37 (34) |
| Septic shock, n (%) | 39 (35) |
| Cardiogenic or obstructive shock, n (%) | 6 (5) |
| ICU controls, n (%) | 28 (26) |
| Comorbidities | |
| IDDM, n (%) | 14 (12) |
| NIDDM, n (%) | 19 (17) |
| Chronic arterial hypertension a, n (%) | 62 (56) |
| Chronic renal failure b, n (%) | 23 (21) |
| Length of ICU stay (days) | 8 ± 6 |
| ICU mortality, n (%) | 16 (15) |
| 28-day mortality, n (%) | 28 (25) |
| 90-day mortality, n (%) | 32 (29) |
| ICU Control Group (n = 28) | Sepsis (n = 37) | Septic Shock (n = 39) | Other Shock (n = 6) | p Value | |
|---|---|---|---|---|---|
| Sex (F:M) | 14:14 | 10:27 | 20:19 | 1:5 | 0.07 |
| Age | 60 [48–74] | 65 [57–75] | 69 [62–80] | 78 [53–88] | 0.13 |
| BMI | 27.5 [25–30.8] | 27.9 [22.4–33.0] | 26.4 [21.8–31.1] | 24.4 [22.9–32.7] | 0.95 |
| ICU days | 6 [4–7) ]€ | 6 [4–8] € | 9 [6–12] | 3 [3–7] € | 0.005 |
| SOFA | 4 [2–7] € | 3 [3–5] € | 9 [7–10] | 7 [5–8] | <0.001 |
| APACHE II | 17 [14–22] | 16 [11–21 ]% € | 22 [7–30] | 26 [23–30] | <0.001 |
| Arterial hypertension, n | 17 | 24 | 19 | 2 | 0.32 |
| CRF, n | 4 | 9 | 8 | 2 | 0.67 |
| IDDM, n | 4 | 6 | 3 | 1 | 0.7 |
| NIDDM, n | 3 | 11 | 5 | 0 | 0.09 |
| Oral nutrition, n | 5 $ | 17 € | 6 | 1 | 0.012 |
| Enteral nutrition, n | 6 | 5 | 11 | 1 | 0.47 |
| Parenteral nutrition, n | 0 | 0 | 0 | 0 | 1 |
| ICU survival, n (%) | 25 (89) | 34 (92) | 30 (77) | 5 (83) | 0.28 |
| 28-day survival, n (%) | 24 (86) | 30 (81) | 23 (59) | 5 (83) | 0.05 |
| 90-day survival, n (%) | 22 (79) | 28 (76) | 23 (59) | 5 (83) | 0.25 |
| Biological Data | ICU Control Group (n = 28) | Sepsis (n = 37) | Septic Shock (n = 39) | Other Shock (n = 6) | p Value |
|---|---|---|---|---|---|
| Lactate (mEq/L) | 1.2 ( [0.8–1.7] | 0.9 [0.7–1.4] | 1.6 [1.2–2.4] $ | 3.1 [1.9–6.6] $ | 0.001 |
| Glycemia (mg/dL) | 142 [125–157] | 149 [109–227] | 164 [123–183] | 181 [140–187] | 0.52 |
| Hemoglobin (g/dL) | 12.2 [10.0–14.4] | 11.2 [10.1–13.7] | 10.1 [9.2–11.7] £ $ | 10.4 [9.6–11.0] £ | 0.007 |
| White blood cells (10.3/mm3) | 13.1 [11.4–15.9] | 11.4 [7.8–15.2] | 17.4 [10.6–24.5] | 21.4 [19.9–29.7] £ | 0.018 |
| Platelets (10.3/mm3) | 223 [184–281] | 235 [183–311] | 230 [142–370] | 232 [176–276] | 0.94 |
| C-reactive protein (mg/dL) | 19 [9–52] € | 109 [64–208] % £ | 222 [118–297] | 15 [5–26] € | <0.001 |
| Bilirubin (mg/dL) | 0.5 [0.4–0.8] | 0.6 [0.4–1.0] | 0.7 [0.5–2.1] | 0.6 [0.3–1.1] | 0.29 |
| BUN (mg/dL) | 17.7 [11.7–24.3] € | 19.6 [13.5–33.6] € | 32.2 [22.9–57.4] | 25.7 [15.9–42.9] | <0.001 |
| Creatinin (mg/dL) | 0.8 [0.7–0.9] € | 0.7 [0.7–1.3] € | 1.5 [0.9–2.8] | 1.3 [0.8–2.2] | <0.001 |
| Albumin (g/L) | 32 [28–35] € | 30 [27–33] | 27 [22–31] | 29 [23–30] | 0.037 |
| Treatment and Parameters | ICU Control Group (n = 28) | Sepsis (n = 37) | Septic Shock (n = 39) | Other Shock (n = 6) | p Value |
|---|---|---|---|---|---|
| Midazolam (mg/h) | 0 [0–2] | 0 [0–0] | 1.5 [0–3.3] $ | 1 [0–4] | 0.036 |
| Morphine (mg/h) | 0 [0–2] | 0 [0–0] | 0 [0–2] | 1 [0–2] | 0.22 |
| Dobutamine (μg/kg/min) | 0 [0–0] | 0 [0–0] | 0 [0–0] | 1 [0–4] $ £ € | <0.001 |
| Norepinephrin (μg/kg/min) | 0 [0–0] | 0 [0–0] | 0.2 [0.07–0.25] $ £ | 0.14 [0.06–0.2] $ £ | <0.001 |
| PaO2/FiO2 | 250 [183–299] | 175 [135–250] | 196 [143–306] | 190 [164–279] | 0.22 |
| Heart rate (beat/min) | 73 [61–92] | 101 [79–111] £ | 97 [85–109] £ | 100 [75–112] | 0.001 |
| Mean arterial pressure (mmHg) | 85 [75–93] | 82 [75–92] | 69 [64–74] $ £ | 65 [61–71] £ $ | <0.001 |
| Temperature (° Celcius) | 36.6 [35.7–37.1] | 36.8 [36.3–37.1] | 36.7 [36.4–37.7] | 35.1 [34.5–35.8] € $ | 0.007 |
| ICU Control Group (n = 26) | Sepsis (n = 31) | Septic Shock (n = 37) | Other Shock (n = 5) | p Value | |
|---|---|---|---|---|---|
| Phenylalanine | 0.00803 [0.0068–0.00967] £ * | 0.0103 [0.00822–0.0143] | 0.0113 [0.00916–0.0142] | 0.986 [0.00744–0.0124] | 0.004 |
| Lactate | 1.357 [1.062–1.821] | 1.2 [0.869–1.605) £ | 1.616 [1.218–2.08] | 2.12 5 [1.181–2.987] | 0.017 |
| Carnitine | 0.06 [0.0453–0.0916] £ | 0.0634 [0.0353–0.0785] £ | 0.1 [0.0655–0.164] | 0.0958 [0.0929–0.145] | 0.016 |
| Urea | 0.0228 [0–0.0442] £ | 0.025 [0–0.0414] £ | 0.0752 [0.0289–0.156] | 0.0647 [0.0153–0.124] | <0.001 |
| Myo-inositol | 0.0085 [0–0.0153] £ | 0.00838 [0–0.0222] £ | 0.0216 [0.00864–0.0421] | 0.0148 [0.00819–0.0292] | 0.001 |
| Creatinine | 0.0314 [0.0282–0.0424] ** £ | 0.0313 [0.0257–0.0485] £ | 0.0708 [0.041–0.105] | 0.0783 [0.0563–0.123] | 0.002 |
| Creatinine (singulet) | 0.0475 [0.0475–0.0554] £ | 0.0463 [0.0399–0.0615] ** £ | 0.0863 [0.0583–0.149] | 0.101 [0.0752–0.16] | <0.001 |
| Creatine | 0.0189 [0.0113–0.0259] £ * | 0.0382 [0.0169–0.0731] | 0.0645 [0.0287–0.136] | 0.0245 [0.0128–0.0527] | <0.001 |
| Creatine | 0.0183 [0.0121–0.0219] £ | 0.029 [0.0161–0.0622] £ | 0.0458 [0.0319–0.103] | 0.0145 [0.012–0.0415] £ | <0.001 |
| Citrate | 0.0314 [0.0234–0.0355] * | 0.0227 [0.018–0.0297] ** | 0.0277 [0.0201–0.0343] | 0.037 [0.0319–0.0503] | 0.004 |
| Pyruvate | 0.0377 [0.0282–0.0533] | 0.0334 [0.0246–0.0487] £ | 0.0509 [0.0395–0.0671] | 0.047 [0.0296–0.102] | 0.015 |
| 2-hydroxyisovalerate | 0.00529 [0−0.0851] ** | 0.00862 [0−0.0147] | 0.00841 [0.00474–0.0185] | 0.0714 [0.0446–0.0854] * £ | 0.002 |
| Mannitol | 0.0213 [0.00938–0.122] £ | 0.00882 [0.00513–0.017] £ | 0.0958 [0.024–0.313] | 0.00918 [0.00663–0.0446] £ | <0.001 |
| Glycerol | 0.177 [0.135–0.229] | 0.169 [0.151–0.205] | 0.169 [0.137–0.212] | 0.2 [0.153–0.211] | 0.984 |
| TMAO | 0.0554 [0.00988–0.117] | 0.0518 [0.0372–0.0851] | 0.0847 [0.051–0.124] | 0.121 [0.0733–0.22] | 0.205 |
| Ethanol | 0.00498 [0–0.0111] | 0.00758 [0.00578–0.0184] | 0.00766 [0.00213–0.0124] | 0.0134 [0.00172–0.0232] | 0.173 |
| 3-hydroxyxisobutyrate | 0.0105 [0.00732–0.014] | 0.0125 [0.0093–0.0175] | 0.0161 [0.0117–0.0212] | 0.0135 [0.0097–0.0196] | 0.166 |
| Isoleucine | 0.0242 [0.0178–0.0312] | 0.0301 [0.0212–0.0396] | 0.0257 [0.0185–0.0325] | 0.0211 [0.0202–0.0307] | 0.33 |
| Tyrosine | 0.0196 [0.0151–0.0226] | 0.0198 [0.0159–0.027] | 0.0187 [0.0147–0.0278] | 0.0209 [0.0132–0.0271] | 0.96 |
| Glucose | 0.583 [0.492–0.657] | 0.664 [0.559–0.969] | 0.699 [0.486–0.791] | 0.833 [0.613–0.914] | 0.078 |
| Choline | 0.0177 [0.0126–0.0232] | 0.0229 [0.0146–0.0276] | 0.0191 [0.0114–0.0279] | 0.0248 [0.0226–0.0306] | 0.242 |
| Acetylcarnitine | 0.00873 [0.00764–0.0173] | 0.0136 [0.00405–0.0192] | 0.0192 [0.00708–0.0327) | 0.015 [0.013–0.0293] | 0.115 |
| Malonate | 0 [0–0.00426] | 0.00313 [0–0.0112] | 0 [0–0.0087] | 0 [0–0.00497] | 0.465 |
| Glutamine | 0.183 [0.134–0.222] | 0.262 [0.184–0.28] | 0.18 [0.119–0.206] | 0.181 [0.132–0.206] | 0.337 |
| 3-hydroxybutyrate | 0.0181 [0–0.0374] | 0.018 [0–0.0545] | 0.0183 [0–0.0545] | 0.0145 [0–0.0508] | 0.993 |
| Acetoacetate | 0.0136 [0.0103–0.0295] | 0.0199 [0.00971–0.0385] | 0.0163 [0.00923–0.0256] | 0.0195 [0.00916–0.0306] | 0.864 |
| Acetone | 0 [0−0.003] | 0.00201 [0–0.046] | 0 [0−0.00333] | 0 [0−0.00136] | 0.338 |
| Acetate | 0.0209 [0.172–0.0283] | 0.0189 [0.014–0.0241) | 0.0188 [0.0165–0.0252] | 0.0244 [0.0171–0.0507] | 0.327 |
| Alanine | 0.17 [0.143–0.259] | 0.158 [0.123–0.199) | 0.173 [0.126–0.208) | 0.22 [0.196–0.342] | 0.163 |
| Peak 1.44 | 0 [0–0] £ | 0 [0–0] | 0 [0–0.0154] | 0 [0–0.0331] | 0.03 |
| Peak 1.41 | 0 [0–0] £ | 0 [0–0.0176] | 0.0097 [0.00307–0.0638] | 0 [0–0] £ | <0.001 |
| 3-hydroxybutyrate | 0.0635 [0.0354–0.147] | 0.0536 [0.0357–0.195] | 0.0722 [0.0282–0.182] | 0.0461 [0.0318–0.011] | 0.961 |
| Propylene glycol | 0 [0−0.142] | 0.0068 [0–0.059] | 0.0272 [0−0.201) | 0 [0−0.332] | 0.258 |
| Valine | 0.101 [0.0844–0.116] | 0.114 [0.0931–0.146] | 0.0877 [0.0733–0.163] | 0.102 [0.0977–0.124] | 0.343 |
| Betaine | 0.0201 [0.0132–0.0283] | 0.0248 [0.0178–0.0396] | 0.023 [0.0127–0.0301] | 0.0231 [0.0204–0.0362] | 0.149 |
| Leucine | 0.0826 [0.0675–0.103] | 0.116 [0.0874–0.134] | 0.0883 [0.0597–0.141] | 0.108 [0.0858–0.129] | 0.06 |
| Hydroxybutyrate | 0.0467 [0.0317–0.0629] | 0.0645 [0.0481–0.0919] | 0.0571 [0.0333–0.0985] | 0.0714 [0.0446–0.0854] | 0.186 |
| Metabolites | Length of ICU Stay | ICU Mortality | 28-Day Mortality | 90-Day Mortality |
|---|---|---|---|---|
| Phenylalanine | rs = −0.18 | rs = 0.06 | rs = −0.08 | rs = −0.05 |
| p = 0.07 | p = 0.55 | p = 0.44 | p = 0.61 | |
| Mannitol | rs = −0.07 | rs = −0.1 | rs = −0.13 | rs = −0.15 |
| p = 0.53 | p = 0.35 | p = 0.22 | p = 0.14 | |
| Carnitine | rs = 0.03 | rs = −0.1 | rs = −0.02 | rs = 0.05 |
| p = 0.79 | p = 0.41 | p = 0.87 | p = 0.65 | |
| Lactate | rs = −0.13 | rs = −0.13 | rs = −0.2 | rs = −0.17 |
| p = 0.20 | p = 0.2 | p = 0.04 | p = 0.1 | |
| Urea | rs = −0.13 | rs = −0.10 | rs = −0.08 | rs = −0.02 |
| p = 0.19 | p = 0.31 | p = 0.42 | p = 0.88 | |
| Myo-inositol | rs = −0.12 | rs = −0.03 | rs = −0.06 | rs = 0.06 |
| p = 0.25 | p = 0.76 | p = 0.55 | p = 0.54 | |
| Creatinine | rs = −0.15 | rs = −0.08 | rs = −0.1 | rs = −0.02 |
| p = 0.14 | p = 0.42 | p = 0.34 | p = 0.85 | |
| Creatine | rs = −0.17 | rs = 0.07 | rs = 0.04 | rs = 0.007 |
| p = 0.1 | p = 0.52 | p = 0.73 | p = 0.94 | |
| Pyruvate | rs = −0.04 | rs = −007 | rs = −0.07 | rs = −0.03 |
| p = 0.7 | p = 0.95 | p = 0.49 | p = 0.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thooft, A.; Conotte, R.; Colet, J.-M.; Zouaoui Boudjeltia, K.; Biston, P.; Piagnerelli, M. Serum Metabolomic Profiles in Critically Ill Patients with Shock on Admission to the Intensive Care Unit. Metabolites 2023, 13, 523. https://doi.org/10.3390/metabo13040523
Thooft A, Conotte R, Colet J-M, Zouaoui Boudjeltia K, Biston P, Piagnerelli M. Serum Metabolomic Profiles in Critically Ill Patients with Shock on Admission to the Intensive Care Unit. Metabolites. 2023; 13(4):523. https://doi.org/10.3390/metabo13040523
Chicago/Turabian StyleThooft, Aurélie, Raphaël Conotte, Jean-Marie Colet, Karim Zouaoui Boudjeltia, Patrick Biston, and Michaël Piagnerelli. 2023. "Serum Metabolomic Profiles in Critically Ill Patients with Shock on Admission to the Intensive Care Unit" Metabolites 13, no. 4: 523. https://doi.org/10.3390/metabo13040523
APA StyleThooft, A., Conotte, R., Colet, J. -M., Zouaoui Boudjeltia, K., Biston, P., & Piagnerelli, M. (2023). Serum Metabolomic Profiles in Critically Ill Patients with Shock on Admission to the Intensive Care Unit. Metabolites, 13(4), 523. https://doi.org/10.3390/metabo13040523