1H-NMR Urinary Metabolic Profile, A Promising Tool for the Management of Infants with Human Cytomegalovirus-Infection

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patients
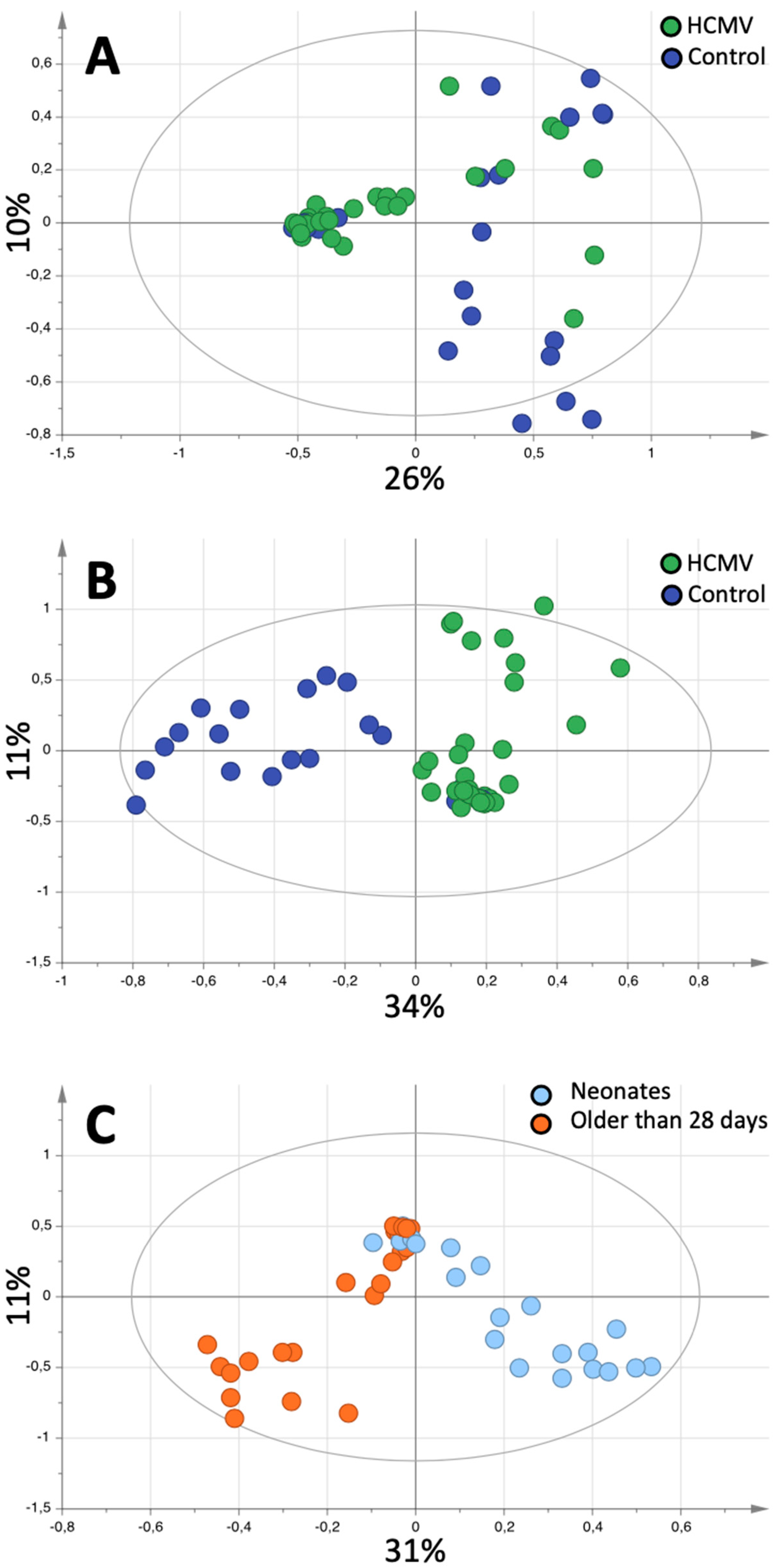
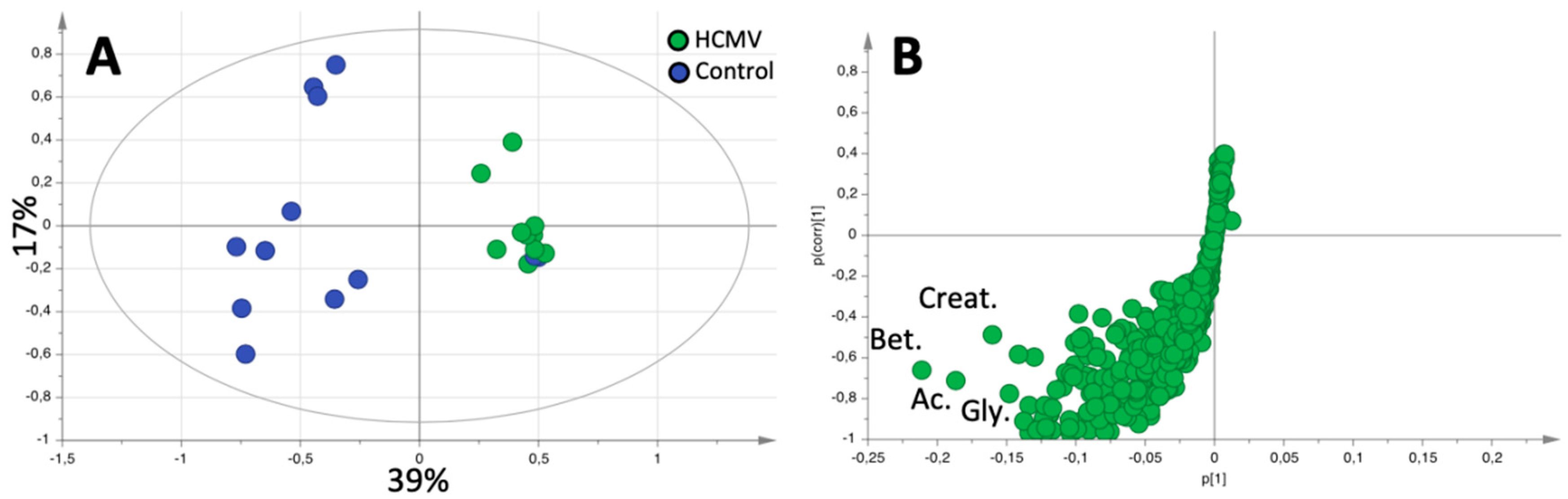
2.2. Pattern Recognition
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Definitions
4.3. Samples
4.4. NMR Spectroscopy
4.5. Data Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Luck, S.E.; Wieringa, J.W.; Blázquez-Gamero, D.; Henneke, P.; Schuster, K.; Butler, K.; Capretti, M.G.; Cilleruelo, M.J.; Curtis, N.; Garofoli, F.; et al. Congenital Cytomegalovirus: A European Expert Consensus Statement on Diagnosis and Management. Pediatr. Infect. Dis. J. 2017, 36, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Rawlinson, W.D.; Boppana, S.B.; Fowler, K.B.; Kimberlin, D.W.; Lazzarotto, T.; Alain, S.; Daly, K.; Doutré, S.; Gibson, L.; Giles, M.L.; et al. Congenital cytomegalovirus infection in pregnancy and the neonate: Consensus recommendations for prevention, diagnosis, and therapy. Lancet Infect. Dis. 2017, 17, e177–e188. [Google Scholar] [CrossRef]
- Fanos, V.; Antonucci, R.; Barberini, L.; Noto, A.; Atzori, L. Clinical application of metabolomics in neonatology. J. Matern. Fetal Neonatal Med. 2012, 25, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Grosse, S.D.; Ross, D.S. New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection. Rev. Med. Virol. 2007, 17, 355–363. [Google Scholar] [CrossRef]
- Kimberlin, D.W.; Lin, C.Y.; Sánchez, P.J.; Demmler, G.J.; Dankner, W.; Shelton, M.; Jacobs, R.F.; Vaudry, W.; Pass, R.F.; Kiell, J.M.; et al. Effect of ganciclovir therapy on hearing in symptomatic congenital cytomegalovirus disease involving the central nervous system: A randomized, controlled trial. J. Pediatr. 2003, 1, 16–25. [Google Scholar] [CrossRef]
- Kimberlin, D.W.; Jester, P.M.; Sánchez, P.J.; Ahmed, A.; Arav-Boger, R.; Michaels, M.G.; Ashouri, N.; Englund, J.A.; Estrada, B.; Jacobs, R.F.; et al. Valganciclovir for symptomatic congenital cytomegalovirus disease. N. Engl. J. Med. 2015, 372, 933–943. [Google Scholar] [CrossRef]
- Fanos, V.; Locci, E.; Noto, A.; Lazzarotto, T.; Manzoni, P.; Atzori, L.; Lanari, M. Urinary metabolomics in newborns infected by human cytomegalovirus: A preliminary investigation. Early Hum. Dev. 2013, 89, S58–S61. [Google Scholar] [CrossRef]
- Munger, J.; Bajad, S.U.; Coller, H.A.; Shenk, T.; Rabinowitz, J.D. Dynamics of the cellular metabolome during human cytomegalovirus infection. PLoS Pathog. 2006, 2, e132. [Google Scholar] [CrossRef]
- Alarcón, A.; Baquero-Artigao, F. Review and guidelines on the prevention, diagnosis and treatment of postnatal cytomegalovirus infection. An. Pediatr. (Barc.) 2011, 74, 52.e1–52.e13. [Google Scholar]
- Pérez, A.; Apolinar, E.; Acosta, B.; Ribes, C.; Díaz, C.; Muñoz, A. Perinatal cytomegalovirus infection in preterm infants. An. Esp. Pediatr. 2002, 57, 244–248. [Google Scholar]
- Ross, S.A.; Ahmed, A.; Palmer, A.L.; Michaels, M.G.; Sánchez, P.J.; Stewart, A.; Bernstein, D.I.; Feja, K.; Fowler, K.B.; Boppana, S.B.; et al. Newborn Dried Blood Spot Polymerase Chain Reaction to Identify Infants with Congenital Cytomegalovirus-Associated Sensorineural Hearing Loss. J. Pediatr. 2017, 184, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Vives-Oñós, I.; Soler-Palacín, P.; Codina-Grau, M.G.; Martín-Nalda, A.; López-Galera, R.M.; Marín-Soria, J.L.; Figueras-Nadal, C. Can we rule out a congenital cytomegalovirus infection when the result of polymerase chain reaction in dried blood spots is negative? Enferm. Infecc. Microbiol. Clin. 2014, 32, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Cesare Marincola, F.; Noto, A.; Caboni, P.; Reali, A.; Barberini, L.; Lussu, M.; Murgia, F.; Santoru, M.L.; Atzori, L.; Fanos, V. A metabolomic study of preterm human and formula milk by high resolution NMR and GC/MS analysis: Preliminary results. J. Matern. Fetal Neonatal Med. 2012, 25, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Vives-Oñós, I.; Codina-Grau, M.G.; Noguera-Julian, A.; Blázquez-Gamero, D.; Fortuny, C.; Baquero-Artigao, F.; Frick, M.A.; Saavedra-Lozano, J.; Goycochea-Valdivia, W.; Rives-Ferreiro, M.T.; et al. Is Polymerase Chain Reaction in Neonatal Dried Blood Spots Reliable for the diagnosis of congenital cytomegalovirus infection? Pediatr. Infect. Dis. J. 2019, 38, 520–524. [Google Scholar]
- Fanos, V.; Barberini, L.; Antonucci, R.; Atzori, L. Metabolomics in neonatology and pediatrics. Clin. Biochem. 2011, 44, 452–454. [Google Scholar] [CrossRef]
- Fanos, V.; Antonucci, R.; Barberini, L.; Atzori, L. Urinary metabolomics in newborns and infants. Adv. Clin. Chem. 2012, 58, 193–223. [Google Scholar]
- Raamsdonk, L.M.; Teusink, B.; Broadhurst, D.; Zhang, N.; Hayes, A.; Walsh, M.C.; Berden, J.A.; Brindle, K.M.; Kell, D.B.; Rowland, J.J.; et al. A functional genomics strategy that uses metabolome data to reveal the phenotype of silent mutations. Nat. Biotechnol. 2001, 19, 45–50. [Google Scholar] [CrossRef]
- Ellis, D.I.; Dunn, W.B.; Grin, J.L.; Allwood, J.W.; Goodacre, R. Metabolic fingerprinting as a diagnostic tool. Pharmacogenomics 2007, 8, 1243–1266. [Google Scholar] [CrossRef]
- Wilson, I.D. Drugs, bugs, and personalized medicine: Pharmacometabonomics enters the ring. Proc. Natl. Acad. Sci. USA 2009, 106, 14187–14188. [Google Scholar] [CrossRef]
- Fanos, V.; Yurdakök, M. Personalized neonatal medicine. J. Matern. Fetal Neonatal Med. 2010, 23, 4–6. [Google Scholar] [CrossRef]
- Mirnezami, R.; Nicholson, J.; Darzi, A. Preparing for precision medicine. N. Engl. J. Med. 2012, 366, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.; Wilson, I.D.; Nicholson, J.K. Metabolic phenotyping in health and disease. Cell 2008, 134, 714–717. [Google Scholar] [CrossRef] [PubMed]
- Barba, I.; Andres, M.; Dorado, D.G. Metabolomics and heart diseases: From basic to clinical approach. Curr. Med. Chem. 2019, 26, 46–59. [Google Scholar] [CrossRef] [PubMed]
- Atzori, L.; Antonucci, R.; Barberini, L.; Griffin, J.L.; Fanos, V. Metabolomics: A new tool for the neonatologist. J. Matern. Fetal Neonatal Med. 2009, 22, 50–53. [Google Scholar] [CrossRef] [PubMed]
- Hyde, M.J.; Beckonert, O.P.; Yap, I.K.S.; Booms, C.; Gale, C.R.K.; Logan, K.; Karataza, A.; Murgasova, D.; Holmes, E.; Modi, N. The effect of preterm delivery on the urinary metabolome. In Summer Meeting; The Neonatal Society: Nottingham, UK, 2010; Available online: www.neonatalsociety.ac.uk (accessed on 24 November 2019).
- Gu, H.; Pan, Z.; Xi, B.; Hainline, B.E.; Shanaiah, N.; Asiago, V.; Gowda, G.A.; Raftery, D. 1H NMR metabolomics study of age profiling in children. NMR Biomed. 2009, 22, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Fanos, V.; Iacovidou, N.; Puddu, M.; Ottonello, G.; Noto, A.; Atzori, L. Metabolomics in neonatal life. Early Hum. Dev. 2013, 89, S7–S10. [Google Scholar] [CrossRef]
- Kenny, L.C.; Broadhurst, D.I.; Dunn, W.; Brown, M.; North, R.A.; McCowan, L.; Roberts, C.; Cooper, G.J.; Kell, D.B.; Baker, P.N.; et al. Robust early pregnancy prediction of later preeclampsia using metabolomic biomarkers. Hypertension 2010, 56, 741–749. [Google Scholar] [CrossRef]
- Mussap, M.; Zaffanello, M.; Fanos, V. Metabolomics: A challenge for detecting and monitoring inborn errors of metabolism. Ann. Transl. Med. 2018, 6, 338. [Google Scholar] [CrossRef]
- Mussap, M.; Noto, A.; Cibecchini, F.; Fanos, V. The importance of biomarkers in neonatology. Semin. Fetal Neonatal Med. 2013, 18, 56–64. [Google Scholar] [CrossRef]
- Lee, A.H.; Shannon, C.P.; Amenyogbe, N.; Bennike, T.B.; Diray-Arce, J.; Idoko, O.T.; Gill, E.E.; Ben-Othman, R.; Pomat, W.S.; van Haren, S.D.; et al. Dynamic molecular changes during the first week of human life follow a robust developmental trajectory. Nat. Commun. 2019, 10, 1092. [Google Scholar] [CrossRef]
- Wishart, D.S. NMR metabolomics: A look ahead. J. Magn. Reson. 2019, 306, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Trump, S.; Laudi, S.; Unruh, N.; Goelz, R.; Leibfritz, D. 1H-NMR metabolic profiling of human neonatal urine. MAGMA 2006, 19, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, A.M.; Ramadas, E.H.; Kennedy, M.A. Potential effect of diaper and cotton ball contamination on NMR- and LC/MS-based metabonomics studies of urine from newborn babies. Anal. Chem. 2011, 83, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Bouatra, S.; Aziat, F.; Mandal, R.; Guo, A.C.; Wilson, M.R.; Knox, C.; Bjorndahl, T.C.; Krishnamurthy, R.; Saleem, F.; Liu, P.; et al. The human urinary metabolome. PLoS ONE 2013, 8, e73076. [Google Scholar] [CrossRef] [PubMed]
- Ueland, P.M. Choline and betaine in health and disease. J. Inherit. Metab. Dis. 2011, 34, 3–15. [Google Scholar] [CrossRef]
- Ducker, G.S.; Rabinowitz, J.D. One-Carbon Metabolism in Health and Disease. Cell Metab. 2017, 25, 27–42. [Google Scholar] [CrossRef] [Green Version]
- McMahon, K.E.; Farrell, P.M. Measurement of free choline concentrations in maternal and neonatal blood by micropyrolysis gas chromatography. Clin. Chim. Acta 1985, 149, 1–12. [Google Scholar] [CrossRef]
- Fattuoni, C.; Palmas, F.; Noto, A.; Barberini, L.; Mussap, M.; Grapov, D.; Dessì, A.; Casu, M.; Casanova, A.; Furione, M.; et al. Primary HCMV infection in pregnancy from classic data towards metabolomics: An exploratory analysis. Clin. Chim. Acta 2016, 460, 23–32. [Google Scholar] [CrossRef]
- Vastag, L.; Koyuncu, E.; Grady, S.L.; Shenk, T.E.; Rabinowitz, J.D. Divergent effects of human cytomegalovirus and herpes simplex virus-1 on cellular metabolism. PLoS Pathog. 2011, 7, e1002124. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Clippinger, A.J.; Alwine, J.C. Viral effects on metabolism: Changes in glucose and glutamine utilization during human cytomegalovirus infection. Trends Microbiol. 2011, 19, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Madsen, R.; Lundstedt, T.; Trygg, J. Chemometrics in metabolomics–a review in human disease diagnosis. Anal. Chim. Acta 2010, 659, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Atzori, L.; Antonucci, R.; Barberini, L.; Locci, E.; Marincola, F.C.; Scano, P.; Cortesi, P.; Agostiniani, R.; Defraia, R.; Weljie, A.; et al. 1H-NMR-based metabolomic analysis of urine from preterm and term neonates. Front. Biosci. 2011, E3, 1005–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syggelou, A.; Iacovidou, N.; Atzori, L.; Xanthos, T.; Fanos, V. Metabolomics in the developing human being. Pediatr. Clin. North. Am. 2012, 59, 1039–1058. [Google Scholar] [CrossRef] [PubMed]
- Dessi, A.; Ottonello, G.; Fanos, V. Physiopathology of intrauterine growth retardation: From classic data to metabolomics. J. Matern. Fetal Neonatal Med. 2012, 25, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Paladini, P.; Paladini, A.; Noto, A.; Atzori, L.; Barberini, L.; Puxeddu, E. Urinary metabolomics in twins at birth. J. Pediatr. Neonat. Individual Med. 2012, 1, 113. [Google Scholar]
- Nicholson, J.K.; Holmes, E.; Kinross, J.M.; Darzi, A.W.; Takats, Z.; Lindon, J.C. Metabolic phenotyping in clinical and surgical environments. Nature 2012, 491, 384–392. [Google Scholar] [CrossRef]
- Bothwell, J.H.F.; Griffin, J.L. An introduction to biological nuclear magnetic resonance spectroscopy. Biol. Rev. Camb. Philos. Soc. 2011, 86, 493–510. [Google Scholar] [CrossRef]
- Eriksson, L.; Trygg, J.; Wold, S. CV-ANOVA for significance testing of PLS and OPLS® models. J. Chemom. 2008, 22, 594–600. [Google Scholar] [CrossRef]
- Barba, I.; de León, G.; Martín, E.; Cuevas, A.; Aguade, S.; Candell-Riera, J.; Barrabés, J.A.; Garcia-Dorado, D. Nuclear magnetic resonance-based metabolomics predicts exercise-induced ischemia in patients with suspected coronary artery disease. Magn. Reson. Med. 2008, 60, 27–32. [Google Scholar] [CrossRef]
- Barba, I.; Andrés, M.; Picón, I.; Aguade-Bruix, S.; Garcia-Dorado, D. Sex differences in the 1H-NMR metabolic profile of serum in cardiovascular risk patients. Sci. Rep. 2019, 9, 2380. [Google Scholar] [CrossRef] [Green Version]
- Atzori, L.; Barberini, L.; Santoru, M.L.; Antonucci, R.; Fanos, V. Metabolomics explained to perinatologists and pediatricians. J. Matern. Fetal Neonatal Med. 2012, 25, 10–12. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | Cases (%) | Controls (%) | p * | ||
|---|---|---|---|---|---|
| Number of patients | cHCMV 11 (35.5) | pHCMV 20 (64.5) | Total 31 (58.5) | 22 (41.5) | |
| Sex: Male | 5 (45.5) | 11 (55) | 16 (51.6) | 11 (50) | ns |
| Female | 6 (54.5) | 9 (45) | 15 (48.4) | 11 (50) | |
| Chronological age range (median), days | 0–37 (1) | 35–122 (63) | 0–122 (56) | 0–115 (3) | 0.006 |
| Chronological age: ≤28 days of life | 10 (90.9) | 0 (0) | 10 (32.3) | 16 (72.7) | 0.0054 |
| >28 days of life | 1 (9.1) | 20 (100) | 21 (67.7) | 6 (27.3) | |
| Gestational age range, weeks | 34–41 | 243/7–415/7 | 243/7–415/7 | 27–404/7 | ns |
| Corrected age^, weeks: Term | 6 (54.5) | 14 (70) | 20 (64.5) | 11 (50) | ns |
| Preterm | 5 (45.5) | 6 (30) | 11 (35.5) | 11 (50) | |
| Birth weight, grams, range (median) | 1475–4000 (2455) | 500–3840 (1035) | 500–4000 (1475) | 870–3955 (1710) | ns |
| Type of delivery: Cesarean section | 7 (63.6) | 16 (80) | 23 (74.2) | 15 (68.2) | ns |
| Vaginal delivery | 4 (36.4) | 4 (20) | 8 (25.8) | 7 (31.8) | |
| Multiple birth | 3 (27.3) | 7 (35) | 10 (32.3) | 5 (22.7) | ns |
| Diet: Breastfed | 5 (45.4) | 10 (50) | 15 (48.3) | 13 (59.1) | ns |
| Formula milk | 2 (18.2) | 6 (30) | 8 (25.8) | 7 (31.8) | |
| Mixed lactation | 3 (27.3) | 3 (15) | 6 (19.4) | - | |
| Fasting | 1 (9.1) | 1 (5) | 2 (64.5) | 2 (9.1) | |
| Supplement to main diet: Intravenous serum | 4 (36.4) | 1 (5) | 5 (16.1) | - | ns |
| Parenteral nutrition | - | 1 (5) | 1 (32.2) | 7 (31.8) | |
| Fortification of breast milk | - | 6 (30) | 6 (19.4) | 2 (9.1) | |
| Other comorbidities: Intrauterine growth restriction | 3(27.3) | 4(20) | 7 (22.6) | 1 (4.5) | ns |
| Congenital heart disease | - | 1 (4.5) | 1 (3.2) | 2 (9.1) | |
| Diaphragmatic hernia | 1 (9.1) | - | 1 (3.2) | - | |
| Esophageal atresia | - | 1(4.5) | 1 (3.2) | - | |
| Cystic fibrosis | - | 1(4.5) | 1 (3.2) | - | |
| Polymalformative syndrome | - | - | - | 1(4.5) | |
| 22q11 deletion syndrome | - | 1(4.5) | 1 (3.2) | - | |
| Severe combined immunodeficiency | - | - | - | 1(4.5) | |
| Model | R2X | R2Y | Q2 | p (CV-ANOVA) |
|---|---|---|---|---|
| HCMV infection vs. control | 0.436 | 0.581 | 0.293 | 0.03 |
| cHCMV vs. pHCMV | 0.345 | 0.255 | 0.0847 | 0.499 |
| Sex | 0.237 | 0.378 | 0.0693 | 0.509 |
| Chronological age | 0.350 | 0.269 | 0.14 | 0.003 |
| Gestational age | No Fit | |||
| Corrected age | No Fit | |||
| Type of delivery | No Fit | |||
| Multiple birth | No Fit | |||
| Diet | No Fit |
| Metabolites | Concentration, mM (mean ± SD) | Incidence |
|---|---|---|
| 1-Methylnicotinamide | 0.346 ± 0.063 | 69% |
| Oxoglutarate | 0.469 ± 0.099 | 40% |
| Acetate | 1.451 ± 0.496 | 88% |
| Alanine | 0.255 ± 0.049 | 79% |
| Betaine | 0.949 ± 0.128 | 100% |
| Cadaverine | 0.078 | 2% |
| Carnitine | 0.542 ± 0.123 | 31% |
| Choline | 0.122 ± 0.123 | 6% |
| Citrate | 1.327 ± 0.240 | 62% |
| Creatine | 0.377 ± 0.008 | 6% |
| Creatinine | 1.323 ± 0.240 | 100% |
| Dimethylamine | 0.271 ± 0.044 | 100% |
| Fumarate | 0.045 ± 0.014 | 38% |
| Gallate | 1.370 ± 0.923 | 4% |
| Glycine | 1.280 ± 0.181 | 100% |
| Hippurate | 0.151 ± 0.034 | 23% |
| Histidine | 0.142 ± 0.024 | 48% |
| Lactate | 0.404 ± 0.070 | 44% |
| N.N-Dimethylglycine | 0.141 ± 0.033 | 98% |
| Propylene glycol | 0.395 ± 0.129 | 8% |
| Succinate | 0.340 ± 0.140 | 100% |
| Taurine | 0.656 ± 0.114 | 40% |
| Threonine | 0.051 | 2% |
| Tyrosine | 0.045 ± 0.008 | 4% |
| myo-Inositol | 1.523 ± 0.245 | 60% |
| Metabolites | Cases | Controls | p |
|---|---|---|---|
| Acetate | 0.306 ± 0.624 | 0.606 ± 1.275 | 0.571 |
| Alanine | 0.052 ± 0.023 | 0.157 ± 0.147 | 0.038 |
| Betaine | 0.225 ± 0.070 | 0.619 ± 0.585 | 0.048 |
| Creatinine | 0.443 ± 0.389 | 1.081 ± 1.423 | 0.186 |
| Dimethylamine | 0.058 ± 0.046 | 0.226 ± 0.248 | 0.048 |
| Glycine | 0.300 ± 0.150 | 0.978 ± 0.790 | 0.015 |
| Succinate | 0.061 ± 0.117 | 0.094 ± 0.092 | 0.473 |
| Metabolites | Cases | Controls | p |
|---|---|---|---|
| Acetate | 0.459 ± 0.935 | 0.909 ± 1.913 | 0.302 |
| Alanine | 0.078 ± 0.034 | 0.236 ± 0.220 | 0.456 |
| Betaine | 0.338 ± 0.105 | 0.929 ± 0.878 | 0.535 |
| Creatinine | 0.665 ± 0.583 | 1.622 ± 2.135 | 0.764 |
| Dimethylamine | 0.086 ± 0.069 | 0.339 ± 0.372 | 0.637 |
| Glycine | 0.450 ± 0.225 | 1.468 ± 1.185 | 0.781 |
| Succinate | 0.091 ± 0.176 | 0.140 ± 0.138 | 0.420 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frick, M.A.; Barba, I.; Fenoy-Alejandre, M.; López-López, P.; Baquero-Artigao, F.; Rodríguez-Molino, P.; Noguera-Julian, A.; Nicolás-López, M.; de la Fuente-Juárez, A.; Codina-Grau, M.G.; et al. 1H-NMR Urinary Metabolic Profile, A Promising Tool for the Management of Infants with Human Cytomegalovirus-Infection. Metabolites 2019, 9, 288. https://doi.org/10.3390/metabo9120288
Frick MA, Barba I, Fenoy-Alejandre M, López-López P, Baquero-Artigao F, Rodríguez-Molino P, Noguera-Julian A, Nicolás-López M, de la Fuente-Juárez A, Codina-Grau MG, et al. 1H-NMR Urinary Metabolic Profile, A Promising Tool for the Management of Infants with Human Cytomegalovirus-Infection. Metabolites. 2019; 9(12):288. https://doi.org/10.3390/metabo9120288
Chicago/Turabian StyleFrick, Marie Antoinette, Ignasi Barba, Marina Fenoy-Alejandre, Paula López-López, Fernando Baquero-Artigao, Paula Rodríguez-Molino, Antoni Noguera-Julian, Marta Nicolás-López, Asunción de la Fuente-Juárez, Maria Gemma Codina-Grau, and et al. 2019. "1H-NMR Urinary Metabolic Profile, A Promising Tool for the Management of Infants with Human Cytomegalovirus-Infection" Metabolites 9, no. 12: 288. https://doi.org/10.3390/metabo9120288
APA StyleFrick, M. A., Barba, I., Fenoy-Alejandre, M., López-López, P., Baquero-Artigao, F., Rodríguez-Molino, P., Noguera-Julian, A., Nicolás-López, M., de la Fuente-Juárez, A., Codina-Grau, M. G., Esperalba Esquerra, J., Linde-Sillo, Á., & Soler-Palacín, P. (2019). 1H-NMR Urinary Metabolic Profile, A Promising Tool for the Management of Infants with Human Cytomegalovirus-Infection. Metabolites, 9(12), 288. https://doi.org/10.3390/metabo9120288