
The Interrelationships between Intestinal Permeability and Phlegm Syndrome and Therapeutic Potential of Some Medicinal Herbs



Abstract
:1. Introduction
2. Study Design and Search Approach
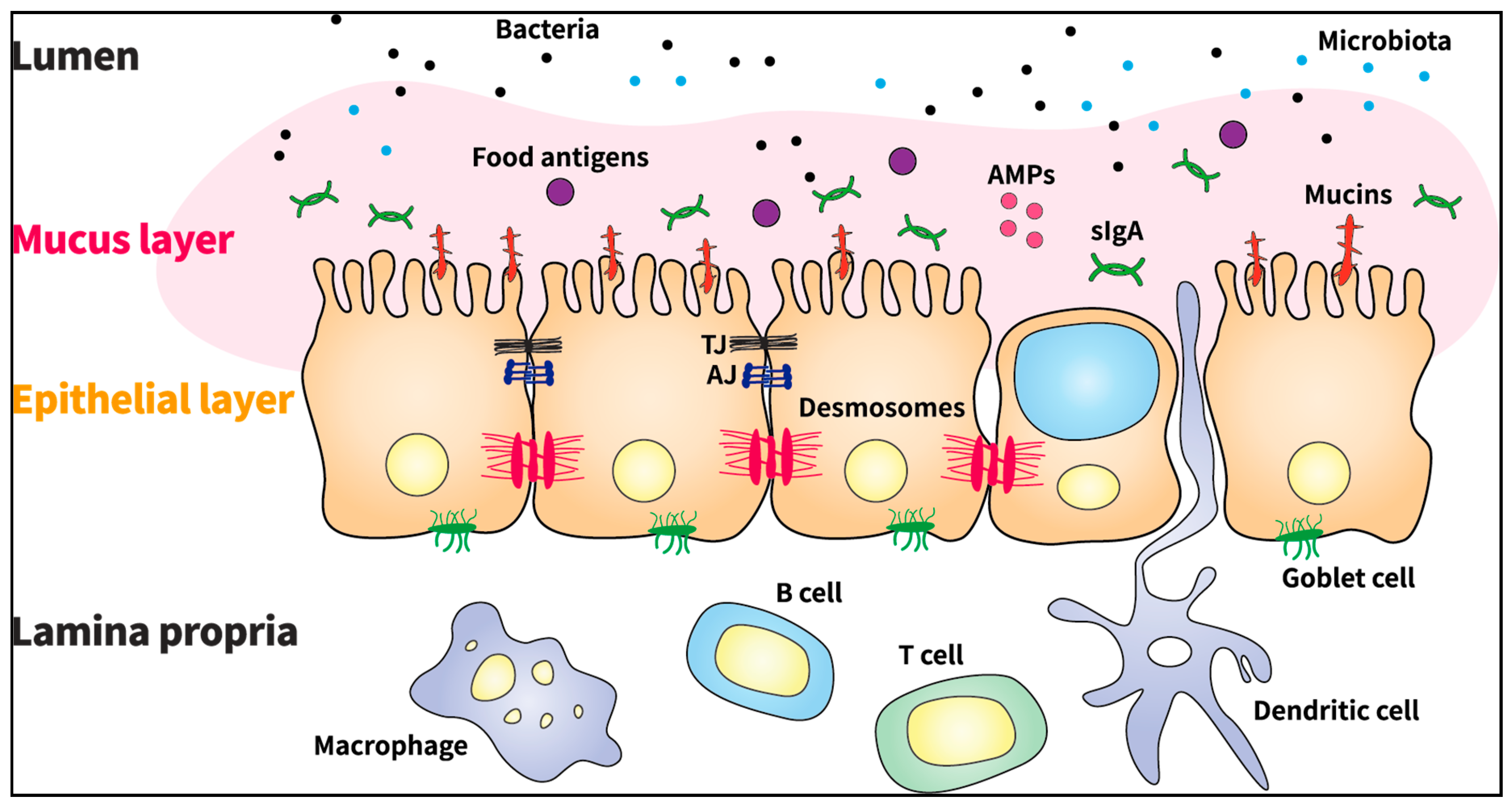
3. Major Components and Regulatory Function of the GI Barrier
4. Detrimental Effects of GI Barrier Dysfunction and Related Diseases
4.1. Inflammatory Bowel Disease (IBD)
4.2. Celiac Disease
4.3. Irritable Bowel Syndrome (IBS)
4.4. Obesity
4.5. Nonalcoholic Steatohepatitis (NASH)
5. Medicinal Plants for Treating Increased GI Permeability
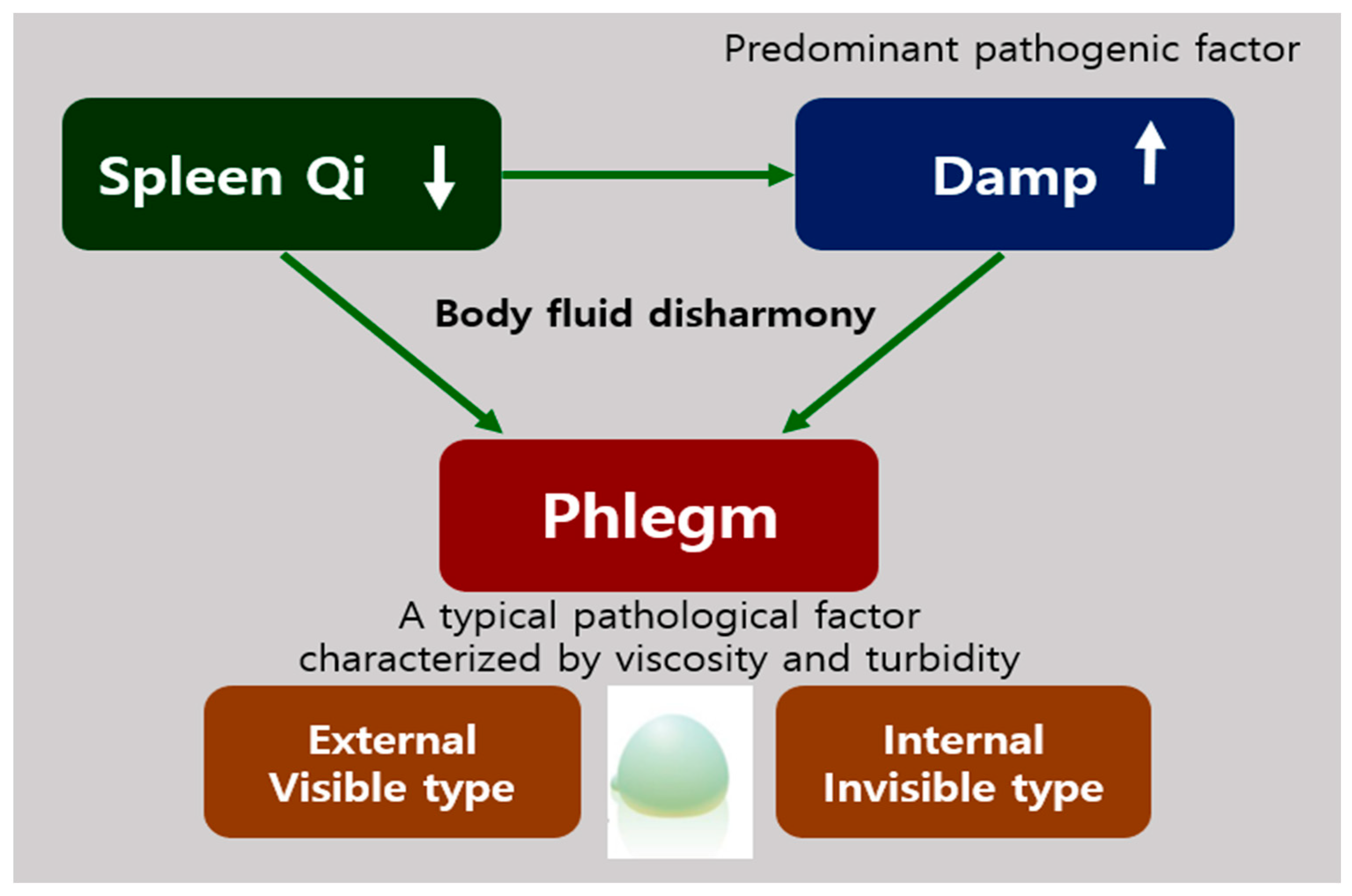
6. What Is Phlegm Syndrome?
7. Diagnosis of Phlegm Syndrome
8. Medicinal Plants for Treating Phlegm Syndrome
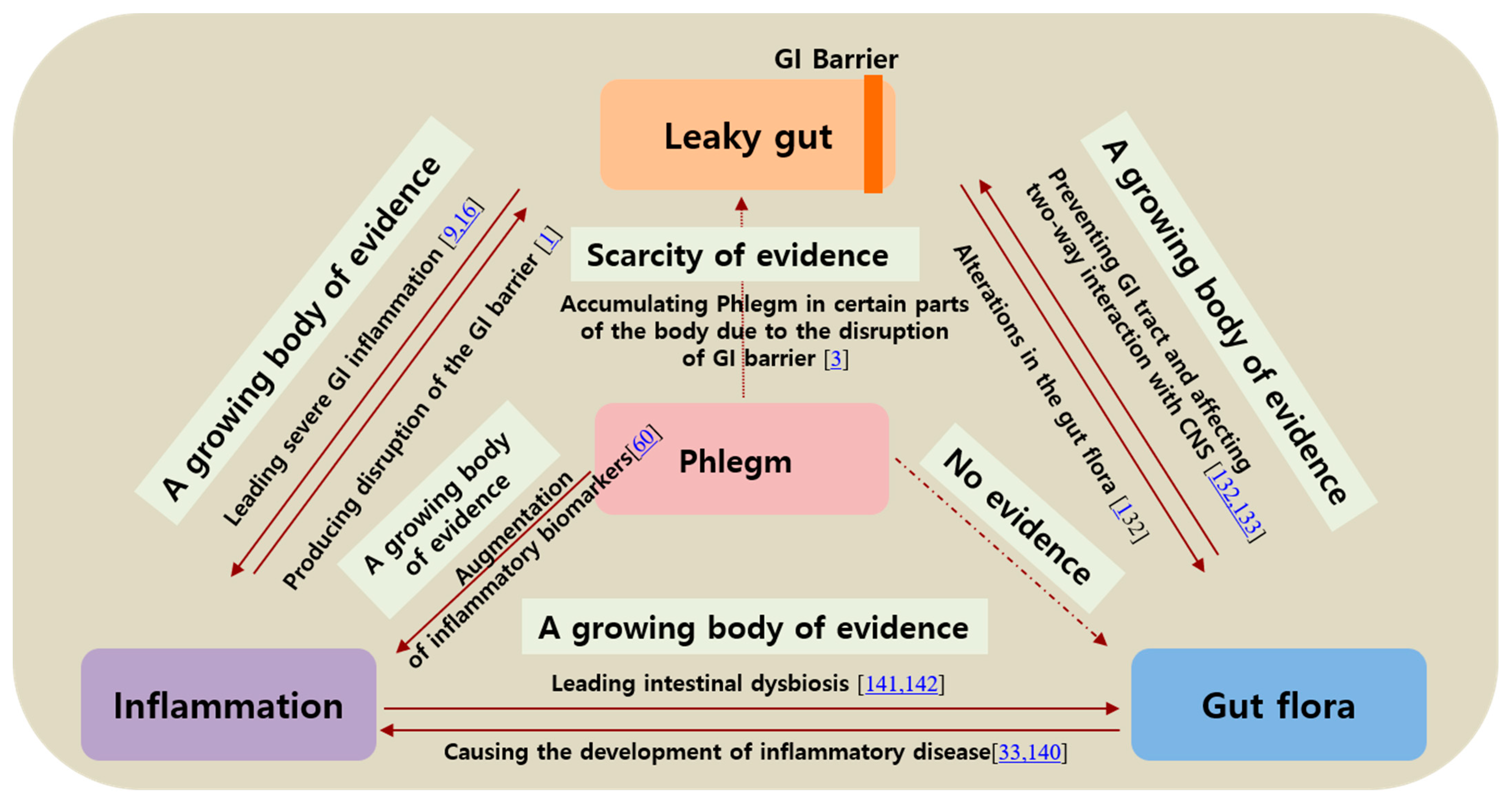
9. The Relation among Phlegm Syndrome, Leaky Gut, and Inflammation
10. Influence on Gut Microbiome Composition
11. Discussion
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vancamelbeke, M.; Vermeire, S. The intestinal barrier: A fundamental role in health and disease. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 821–834. [Google Scholar] [CrossRef]
- König, J.; Wells, J.; Cani, P.; Garcia-Rodenas, C.L.; Macdonald, T.; Mercenier, A.; Whyte, J.; Troost, F.; Brummer, R.-J. Human Intestinal Barrier Function in Health and Disease. Clin. Transl. Gastroenterol. 2016, 7, e196. [Google Scholar] [CrossRef]
- Greenwood, M.T. Dysbiosis, Spleen Qi, Phlegm, and Complex Difficulties. Med. Acupunct. 2017, 29, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Obrenovich, M.E.M. Leaky gut, leaky brain? Microorganisms 2018, 6, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rother, E.T. Systematic literature review X narrative review. Acta. Paul. Enferm. 2007, 20, 5–6. [Google Scholar] [CrossRef] [Green Version]
- Chelakkot, C.; Ghim, J.; Ryu, S.H. Mechanisms regulating intestinal barrier integrity and its pathological implications. Exp. Mol. Med. 2018, 50, 103. [Google Scholar]
- Martini, E.; Krug, S.M.; Siegmund, B.; Neurath, M.F.; Becker, C. Mend your fences: The epithelial barrier and its relationship with mucosal immunity in inflammatory bowel disease. Cell. Mol. Gastroenterol. Hepatol. 2017, 4, 33–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groschwitz, K.R.; Hogan, S.P. Intestinal barrier function: Molecular regulation and disease pathogenesis. J. Allergy Clin. Immunol. 2009, 124, 3–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheru, L.; Saylor, C.F.; Lo, J. Gastrointestinal Barrier Breakdown and Adipose Tissue Inflammation. Curr. Obes. Rep. 2019, 8, 165–174. [Google Scholar] [CrossRef]
- Lee, B.; Moon, K.M.; Kim, C.Y. Tight Junction in the Intestinal Epithelium: Its Association with Diseases and Regulation by Phytochemicals. J. Immunol. Res. 2018, 2018, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, K.E.; Turner, J.R. Myosin light chain kinase: Pulling the strings of epithelial tight junction function. Ann. N. Y. Acad. Sci. 2012, 1258, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoni, L.; Nuding, S.; Wehkamp, J.; Stange, E.F. Intestinal barrier in inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 1165–1179. [Google Scholar] [CrossRef] [PubMed]
- Leaky gut syndromes: Breaking the vicious cycle. Available online: https://healthy.net/2000/12/06/leaky-gut-syndromes-breaking-the-vicious-cycle/ (accessed on 4 February 2021).
- Han, D.-W. Intestinal endotoxemia as a pathogenetic mechanism in liver failure. World J. Gastroenterol. 2002, 8, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Bloembergen, P.; Hofhuis, F.M.; Hol, C.; van Dijk, H. Endotoxin-induced auto-immunity in mice. III. Comparison of different endotoxin preparations. Int. Arch. Allergy Appl. Immunol. 1990, 92, 124–130. [Google Scholar] [CrossRef]
- Michielan, A.; d’ Incà, R. Intestinal permeability in inflammatory bowel disease: Pathogenesis, clinical evaluation, and therapy of leaky gut. Mediat. Inflamm. 2015, 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Hanauer, S.B. Inflammatory bowel disease: Epidemiology, pathogenesis, and therapeutic opportunities. Inflamm. Bowel Dis. 2006, 12, S3–S9. [Google Scholar] [CrossRef]
- Ramasundara, M.; Leach, S.T.; Lemberg, D.A.; Day, A.S. Defensins and inflammation: The role of defensins in inflammatory bowel disease. J. Gastroenterol. Hepatol. 2009, 24, 202–208. [Google Scholar] [CrossRef]
- Wehkamp, J.; Koslowski, M.; Wang, G.; Stange, E.F. Barrier dysfunction due to distinct defensin deficiencies in small intestinal and colonic Crohn’s disease. Mucosal Immunol. 2008, 1, S67–S74. [Google Scholar] [CrossRef] [Green Version]
- Qin, X. Why is damage limited to the mucosa in ulcerative colitis but transmural in Crohn’s disease? World J. Gastrointest. Pathophysiol. 2013, 4, 63–64. [Google Scholar] [CrossRef]
- Noble, C.L.; Nimmo, E.R.; Drummond, H.; Ho, G.T.; Tenesa, A.; Smith, L.; Anderson, N.; Arnott, I.D.R.; Satsangi, J. The contribution of OCTN1/2 variants within the IBD5 locus to disease susceptibility and severity in Crohn’s disease. Gastroenterology 2005, 129, 1854–1864. [Google Scholar] [CrossRef] [Green Version]
- Anderson, C.A.; Boucher, G.; Lees, C.W.; Franke, A.; d’ Amato, M.; Taylor, K.D.; Lee, J.C.; Goyette, P.; Imielinski, M.; Latiano, A.; et al. Meta-analysis identifies 29 additional ulcerative colitis risk loci, increasing the number of confirmed associations to 47. Nat. Genet. 2011, 43, 246–252. [Google Scholar] [CrossRef] [Green Version]
- Piovani, D.; Danese, S.; Peyrin-Biroulet, L.; Nikolopoulos, G.K.; Lytras, T.; Bonovas, S. Environmental risk factors for inflammatory bowel diseases: An umbrella review of meta-analyses. Gastroenterology 2019, 157, 647–659.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Park, J.; Lee, J.-S. Gluten-free diet: A review focusing on wise food choices. EC Nutr. 2018, 13, 673–681. [Google Scholar]
- Lebwohl, B.; Ludvigsson, J.F.; Green, P.H.R. Celiac disease and non-celiac gluten sensitivity. BMJ 2015, 351, h4347. [Google Scholar] [CrossRef] [PubMed]
- Heyman, M.; Abed, J.; Lebreton, C.; Cerf-Bensussan, N. Intestinal permeability in coeliac disease: Insight into mechanisms and relevance to pathogenesis. Gut 2012, 61, 1355–1364. [Google Scholar] [CrossRef]
- Pizzuti, D.; Bortolami, M.; Mazzon, E.; Buda, A.; Guariso, G.; d’ Odorico, A.; Chiarelli, S.; d ’Incà, R.; De, L.F.; Martines, D. Transcriptional downregulation of tight junction protein ZO-1 in active coeliac disease is reversed af-ter a gluten-free diet. Dig. Liver Dis. 2004, 36, 337–341. [Google Scholar] [CrossRef]
- Fasano, A.; Not, T.; Wang, W.; Uzzau, S.; Berti, I.; Tommasini, A.; Goldblum, S.E. Zonulin, a newly discovered modulator of intestinal permeability, and its expression in coeliac disease. Lancet 2000, 355, 1518–1519. [Google Scholar] [CrossRef]
- Shulman, R.J.; Jarrett, M.E.; Cain, K.C.; Broussard, E.K.; Heitkemper, M.M. Associations among gut permeability, inflammatory markers, and symptoms in patients with irritable bowel syndrome. J. Gastroenterol. 2014, 49, 1467–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, A.C.; Talley, N.J. Mucosal inflammation as a potential etiological factor in irritable bowel syndrome: A systematic review. J. Gastroenterol. 2011, 46, 421–431. [Google Scholar] [CrossRef]
- Matricon, J.; Meleine, M.; Gelot, A.; Piche, T.; Dapoigny, M.; Müller, E.; Ardid, D. Review article: Associations between immune activation, intestinal permeability and the irritable bowel syndrome. Aliment. Pharmacol. Ther. 2012, 36, 1009–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camilleri, M.; Madsen, K.; Spiller, R.; Meerveld, B.G.-V.; Verne, G.N. Intestinal barrier function in health and gastrointestinal disease. Neurogastroenterol. Motil. 2012, 24, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Cani, P.D.; Bibiloni, R.; Knauf, C.; Waget, A.; Neyrinck, A.M.; Delzenne, N.M.; Burcelin, R. Changes in gut microbiota control metabolic endotoxemia-induced inflammation in high-fat diet-induced obesity and diabetes in mice. Diabetes 2008, 57, 1470–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, T.; Hara, H. Dietary fat and bile juice, but not obesity, are responsible for the increase in small intestinal permeability induced through the suppression of tight junction protein expression in LETO and OLETF rats. Nutr. Metab. 2010, 7, 19. [Google Scholar]
- Arrese, M.; Cabrera, D.; Kalergis, A.M.; Feldstein, A.E. Innate Immunity and Inflammation in NAFLD/NASH. Dig. Dis. Sci. 2016, 61, 1294–1303. [Google Scholar] [CrossRef] [Green Version]
- Yeoh, N.; Burton, J.P.; Suppiah, P.; Reid, G.; Stebbings, S. The Role of the Microbiome in Rheumatic Diseases. Curr. Rheumatol. Rep. 2013, 15, 314. [Google Scholar] [CrossRef]
- Yarandi, S.S.; Peterson, D.A.; Treisman, G.J.; Moran, T.H.; Pasricha, P.J. Modulatory Effects of Gut Microbiota on the Central Nervous System: How Gut Could Play a Role in Neuropsychiatric Health and Diseases. J. Neurogastroenterol. Motil. 2016, 22, 201–212. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A. Zonulin and Its Regulation of Intestinal Barrier Function: The Biological Door to Inflammation, Autoimmunity, and Cancer. Physiol. Rev. 2011, 91, 151–175. [Google Scholar] [CrossRef] [Green Version]
- Scarpellini, E.; Lupo, M.; Iegri, C.; Gasbarrini, A.; de Santis, A.; Tack, J. Intestinal permeability in non-alcoholic fatty liver disease: The gut-liver axis. Rev. Recent Clin. Trials 2014, 9, 141–147. [Google Scholar]
- Lee, Y.B.; Byun, E.J.; Kim, H.S. Potential Role of the Microbiome in Acne: A Comprehensive Review. J. Clin. Med. 2019, 8, 987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, M.; Gershon, M.D. The bowel and beyond: The enteric nervous system in neurological disorders. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 517–528. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, K.; Mulak, A. Brain-Gut-Microbiota Axis in Alzheimer’s Disease. J. Neurogastroenterol. Motil. 2019, 25, 48–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishehsari, F.; Magno, E.; Swanson, G.; Desai, V.; Voigt, R.M.; Forsyth, C.B.; Keshavarzian, A. Alcohol and Gut-Derived Inflammation. Alcohol Res. 2017, 38, 163–171. [Google Scholar]
- Ponte, R.; Mehraj, V.; Ghali, P.; Couëdel-Courteille, A.; Cheynier, R.; Routy, J.-P. Reversing Gut Damage in HIV Infection: Using Non-Human Primate Models to Instruct Clinical Research. EBioMedicine 2016, 4, 40–49. [Google Scholar] [CrossRef]
- Rogler, G.; Rosano, G. The heart and the gut. Eur. Heart J. 2013, 35, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Du Preez, S.; Corbitt, M.; Cabanas, H.; Eaton, N.; Staines, D.; Marshall-Gradisnik, S. A systematic review of enteric dysbiosis in chronic fatigue syndrome/myalgic encephalomyelitis. Syst. Rev. 2018, 7, 241. [Google Scholar] [CrossRef]
- Ho, K.Y.; Gwee, K.A.; Cheng, Y.K.; Yoon, K.H.; Hee, H.T.; Omar, A.R. Nonsteroidal anti-inflammatory drugs in chronic pain: Implications of new data for clinical practice. J. Pain Res. 2018, 11, 1937–1948. [Google Scholar] [CrossRef] [Green Version]
- Van Elburg, R.M.; Uil, J.J.; van Aalderen, W.M.; Mulder, C.J.; Heymans, H.S. Intestinal permeability in exocrine pancreatic insufficiency due to cystic fibrosis or chronic pancreatitis. Pediatr. Res. 1996, 39, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Smecuol, E.; Sugai, E.; Niveloni, S.; Vázquez, H.; Pedreira, S.; Mazure, R.; Moreno, M.L.; Label, M.; Mauriño, E.; Fasano, A.; et al. Permeability, zonulin production, and enteropathy in dermatitis herpetiformis. Clin. Gastroenterol. Hepatol. 2005, 3, 335–341. [Google Scholar] [CrossRef]
- Mack, D.R.; Flick, J.A.; Durie, P.R.; Rosenstein, B.J.; Ellis, L.E.; Perman, J.A. Correlation of intestinal lactulose permeability with exocrine pancreatic dysfunction. J. Pediatr. 1992, 120, 696–701. [Google Scholar] [CrossRef]
- Humbert, P.; Bidet, A.; Treffel, P.; Drobacheff, C.; Agache, P. Intestinal permeability in patients with psoriasis. J. Dermatol. Sci. 1991, 2, 324–326. [Google Scholar] [CrossRef]
- Buhner, S.; Reese, I.; Kuehl, F.; Lochs, H.; Zuberbier, T. Pseudoallergic reactions in chronic urticaria are associated with altered gastroduodenal permeability. Allergy 2004, 59, 1118–1123. [Google Scholar] [CrossRef]
- Pike, M.G.; Heddle, R.J.; Boulton, P.; Turner, M.W.; Atherton, D.J. Increased Intestinal Permeability in Atopic Eczema. J. Investig. Dermatol. 1986, 86, 101–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kukuruzovic, R.; Robins-Browne, R.M.; Anstey, N.M.; Brewster, D.R. Enteric pathogens, intestinal permeability and nitric oxide production in acute gastroenteritis. Pediatr. Infect. Dis. J. 2002, 21, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Rapin, J.R.; Wiernsperger, N. Possible links between intestinal permeablity and food processing: A potential therapeutic niche for glutamine. Clinics 2010, 65, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Ohno, T.; Mochiki, E.; Kuwano, H. The Roles of Motilin and Ghrelin in Gastrointestinal Motility. Int. J. Pept. 2010, 2010, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Kong, M.; Liu, S.; Chen, G.; Wang, P. Effect of reinforcing kidney-essence, removing phlegm, and promoting mental therapy on treating Alzheimer’s disease. J. Tradit. Chin. Med. 2013, 33, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.-K.; Zhou, T. Syndrome Differentiation and Treatment Experience of Acne. J. Liaoning Univ. Tradit. Chin. Med. 2012, 7, 13–15. [Google Scholar]
- Chen, J.; Xie, S.; Xu, Q. Logistic Regression analysis on the symptom quantitative diagnosis of the common excess syndromes of AIDS. J. Tradit. Chin. Med. 2009, 7. [Google Scholar]
- Cao, Y.X.; Dong, J.C.; Du, Y.J. Biomarkers and inflammatory characteristics for microcosmic syndrome differentiation of cold-phlegm syndrome and heat-phlegm syndrome in patients with bronchial asthma. Chin. J. Integr. Trad. West Med. 2010, 30, 828–832. [Google Scholar]
- Tollerud, D.J.; O’Connor, G.T.; Sparrow, D.; Weiss, S.T. Asthma, Hay Fever, and Phlegm Production Associated with Distinct Patterns of Allergy Skin Test Reactivity, Eosinophilia, and Serum IgE Levels: The Normative Aging Study. Am. Rev. Respir. Dis. 1991, 144, 776–781. [Google Scholar] [CrossRef]
- Wong, V.C.-N.; Chu, V.L.-Y. Autism spectrum disorder and traditional Chinese medicine (acupuncture). Increasing Aware. Child Adolesc. Ment. Health 2010, 18, 227. [Google Scholar]
- Zhang, Z.-M.; Ren, P.-H.; Guan, W.-J. Symptom-based treatment with traditional Chinese medicine in bronchi-ectasis patients with hemoptysis. J. Thorac. Dis. 2017, 9, E884–E886. [Google Scholar] [CrossRef] [Green Version]
- Brett, J. Assessment of Irritable Bowel Syndrome Using Traditional Chinese Medicine—A Critique of Recent Studies. J. Complement. Med. Altern. Heal. 2017, 3, 2. [Google Scholar] [CrossRef]
- Liu, X.-Q.; Peng, D.-H.; Wang, Y.-P.; Xie, R.; Chen, X.-L.; Yu, C.-Q.; Li, X.-T. Diagnostic Accuracy of Chinese Medicine Diagnosis Scale of Phlegm and Blood Stasis Syndrome in Coronary Heart Disease: A Study Protocol. Chin. J. Integr. Med. 2019, 25, 515–520. [Google Scholar] [CrossRef]
- Zhang, Q.-Y.; Liang, H.; Gong, H.-W.; Huang, H.-Y.; Zhou, X.-Q.; Sun, X. Correlations between Phlegm Syndrome of Chinese Medicine and Coronary Angiography: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2015, 2015, 1–12. [Google Scholar] [CrossRef]
- Yang, Z.; Zhao, J.; Liu, J.; Liu, B.; Xie, M. Comparative evaluation in treating qi-yin deficiency and phlegm stasis syndrome of type 2 diabetes mellitus in a rat model. J. Tradit. Chin. Med. Sci. 2019, 6, 59–66. [Google Scholar] [CrossRef]
- Cao, J.; Fan, Y.-P.; Ding, C.-Y. Observation on TCM syndrome of epilepsy. JBUTCM 2007, 30, 285. [Google Scholar]
- Bai, D.; Song, J. Plasma metabolic biomarkers for syndrome of phlegm and blood stasis in hyperlipidemia and atherosclerosis. J. Tradit. Chin. Med. 2012, 32, 578–583. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, Q.; Li, L.; Li, Y.; Zhang, H.; Zheng, L.; Yang, L.; Zheng, Y.; Yang, Y.; Peng, G.; et al. Phlegm-dampness constitution: Genomics, susceptibility, adjustment and treatment with traditional Chinese medicine. Am. J. Chin. Med. 2013, 41, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Mo, S.; Wang, J.; Li, Y.; Wang, C.Z.; Wan, J.Y.; Zhang, Z.; Chen, Y.; Sun, R.; Yuan, C.-S.; et al. Genome-wide DNA methylation profiles of phlegm-dampness constitution. Cell. Physiol. Biochem. 2018, 45, 1999–2008. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Jiang, Y.-K.; Cai, Y.-B. Effects of resolving phlegm method on fibrinolytic status in non-alcoholic steatohepatitis patients of phlegm and blood-stasis syndrome. Chin. J. Integr. Trad. West. Med. 2006, 26, 1090–1093. [Google Scholar]
- Lee, T.C.; Lo, L.C.; Wu, F.C. Traditional Chinese medicine for metabolic syndrome via TCM pattern differentiation: Tongue diagnosis for predictor. Evid. Based Complement. Alternat. Med. 2016, 2016, 1971295. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Chen, P.; Zou, Y.; Jiang, L.; Geng, H.; Yan, R.; Wang, S.; Zhu, L. Clinical relevance of Chinese syndrome factors and thromboelastography levels in patients with phlegm-heat and fu-organ excess syndrome. J. Tradit. Chin. Med. Sci. 2019, 6, 211–217. [Google Scholar] [CrossRef]
- Xie, D.; Qian, J. Analysis of characteristics about treating phlegm syndrome in approaches of phlegmatic scrofula. J. Zhejiang Chin. Med Univ. 2014, 2, 142–143. [Google Scholar]
- Bosch, P.; de Rover, P.; Staudte, H.; Lim, S.; Noort, M.V.D. Schizophrenia, Depression, and Sleep Disorders: Their Traditional Oriental Medicine Equivalents. J. Acupunct. Meridian Stud. 2015, 8, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Bose, S.; Kim, G.-C.; Hong, S.-U.; Kim, J.-H.; Kim, J.-E.; Kim, H. Flos Lonicera Ameliorates Obesity and Associated Endotoxemia in Rats through Modulation of Gut Permeability and Intestinal Microbiota. PLoS ONE 2014, 9, e86117. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Cho, N.; Kim, E.-M.; Park, K.-S.; Kang, Y.W.; Nam, J.H.; Nam, M.S.; Kim, K.K. Cudrania tricuspidata leaf extracts and its components, chlorogenic acid, kaempferol, and quercetin, increase claudin 1 expression in human keratinocytes, enhancing intercellular tight junction capacity. Appl. Biol. Chem. 2020, 63, 1–9. [Google Scholar] [CrossRef]
- Suzuki, T.; Hara, H. Quercetin enhances intestinal barrier function through the assembly of Zonula [corrected] Occludens-2, Occludin, and Claudin-1 and the expression of Claudin-4 in Caco-2 cells. J. Nutr. 2009, 139, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Tanabe, S.; Hara, H. Kaempferol enhances intestinal barrier function through the cytoskeletal association and expression of tight junction proteins in Caco-2 cells. J. Nutr. 2011, 141, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virgili, F.; Marino, M. Regulation of cellular signals from nutritional molecules: A specific role for phytochemicals, beyond antioxidant activity. Free Radic. Biol. Med. 2008, 45, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Z.; Mi, S.; Zhou, L.; Zhou, Y.; Li, J.; Liu, W.; Deng, Z.; Yin, Y. Chlorogenic acid enhances intestinal barrier by decreasing MLCK expression and promoting dynamic distribution of tight junction proteins in colitic rats. J. Funct. Foods 2016, 26, 698–708. [Google Scholar] [CrossRef]
- Liehr, M.; Mereu, A.; Pastor, J.J.; Quintela, J.C.; Staats, S.; Rimbach, G.; Ipharraguerre, I.R. Olive oil bioactives protect pigs against experimentally-induced chronic inflammation independently of alterations in gut microbiota. PLoS ONE 2017, 12, e0174239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, M.; Xuan, S.H.; Park, S.N. Optimization of the extraction process and antioxidant capacity of Coptis chinensis Franch extract through cluster analysis. Appl. Chem. Eng. 2018, 29, 604–612. [Google Scholar]
- Li, C.; Ai, G.; Wang, Y.; Lu, Q.; Lou, C.-D.; Tan, L.; Lin, G.; Liu, Y.; Li, Y.; Zeng, H.; et al. Oxyberberine, a novel gut microbiota-mediated metabolite of berberine, possesses superior anti-colitis effect: Impact on intestinal epithelial barrier, gut microbiota profile and TLR4-MyD88-NF-κB pathway. Pharmacol. Res. 2020, 152, 104603. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.; Wang, P.; Sun, C.; He, W.; Wang, F. Amelioration of IFN-γ and TNF-α-Induced Intestinal Epithelial Barrier Dysfunction by Berberine via Suppression of MLCK-MLC Phosphorylation Signaling Pathway. PLoS ONE 2013, 8, e61944. [Google Scholar] [CrossRef]
- Bose, S.; Kim, H. Evaluation of in vitro anti-inflammatory activities and protective effect of fermented preparations of rhizoma atractylodis macrocephalae on intestinal barrier function against lipopolysaccharide insult. Evid. Based Complement. Alternat. Med. 2013, 2013, 363076. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.L.; Liu, X.Q.; Xie, R.; Peng, D.H.; Wang, Y.P.; Zhou, X.; Wang, B.; Mo, C.-W.; Xu, Q.; Li, X. Expert consensus of syndrome differentiation for phlegm turbidity syndrome for coronary heart disease. Evid. Based Complement. Alternat. Med. 2018, 2018, 8184673. [Google Scholar] [CrossRef]
- Kim, H.; Ku, B.; Kim, J.Y.; Park, Y.-J.; Park, Y.-B. Confirmatory and Exploratory Factor Analysis for Validating the Phlegm Pattern Questionnaire for Healthy Subjects. Evid. Based Complement. Altern. Med. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Wikipedia. Phlegm. Available online: https://en.wikipedia.org/wiki/Phlegm (accessed on 4 February 2021).
- Wolfe, K.J.; Cyr, D.M. Amyloid in neurodegenerative diseases: Friend or foe? Semin. Cell Dev. Biol. 2011, 22, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Wang, J.; Zhao, C.; Song, J.; Tian, G.; Li, Y. Polymorphism of ABCG2 Gene in Hyperuricemia Patients of Han And Uygur Ethnicity with Phlegm/Non-Phlegm Block in Xinjiang, China. Med. Sci. Monit. 2018, 24, 6305–6312. [Google Scholar] [CrossRef]
- Zhang, Z.; Hu, J. Recent Advances and Perspective of Studies on Phlegm Syndrome in Chinese Medicine. Evid. Based Complement. Altern. Med. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.-N. Current concept of Spleen-Stomach theory and Spleen deficiency syndrome in TCM. World J. Gastroenterol. 1998, 4, 2–6. [Google Scholar] [CrossRef]
- Cha, M.H.; Jones, A.D.; Ko, M.M.; Zhang, C.; Lee, M.S. Metabolic Profiles Distinguish Non-Dampness-Phlegm and Dampness-Phlegm Patterns among Korean Patients with Acute Cerebral Infarction. Evid. Based Complement. Altern. Med. 2013, 2013, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dashtdar, M.; Dashtdar, M.R.; Dashtdar, B.; Kardi, K.; Shirazi, M.K. The Concept of Wind in Traditional Chinese Medicine. J. Pharmacopunct. 2016, 19, 293–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buriani, A.; Garcia-Bermejo, M.L.; Bosisio, E.; Xu, Q.; Li, H.; Dong, X.; Simmonds, M.S.; Carrara, M.; Tejedor, N.; Lucio-Cazana, J.; et al. Omic techniques in systems biology approaches to traditional Chinese medicine research: Present and future. J. Ethnopharmacol. 2012, 140, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Ko, M.M.; Moon, T.-W.; Cha, M.H.; Lee, M.S. Association of the UCP-1 single nucleotide polymorphism A-3826G with the dampness-phlegm pattern among Korean stroke patients. BMC Complement. Altern. Med. 2012, 12, 180. [Google Scholar] [CrossRef] [Green Version]
- Zhi, L.; Zhang, D.; Yan, J.-Q.; Li, Q.-L.; Tang, Q.-L. Classification of hyperspectral medical tongue images for tongue diagnosis. Comput. Med. Imaging Graph. 2007, 31, 672–678. [Google Scholar] [CrossRef]
- Kim, S.-R.; Choi, W.; Yeo, I.; Nam, D.-H. Comparative Analysis of Tongue Indices between Patients with and without a Self-Reported Yin Deficiency: A Cross-Sectional Study. Evid. Based Complement. Altern. Med. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- Chung, Y.-F.; Hu, C.-S.; Yeh, C.-C.; Luo, C.-H. How to standardize the pulse-taking method of traditional Chinese medicine pulse diagnosis. Comput. Biol. Med. 2013, 43, 342–349. [Google Scholar] [CrossRef]
- Li, W.; Mao, B.; Wang, G.; Wang, L.; Chang, J.; Zhang, Y.; Wan, M.-H.; Guo, J.; Zheng, Y.-Q. Effect of Tanreqing injection on treatment of acute exacerbation of chronic obstructive pulmonary disease with Chinese medicine syndrome of retention of phlegm and heat in Fei. Chin. J. Integr. Med. 2010, 16, 131–137. [Google Scholar] [CrossRef]
- Wang, P.; Liao, X.; Xie, Y.-M.; Chai, Y.; Li, L.-H. Tanreqing injection for acute bronchitis disease: A systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2016, 25, 143–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Zhong, P.-P.; Tao, Y.-Y. Metabolic profiling of endogenous bile acids: A novel method to assess hepatoprotective effect of Tanreqing capsule on carbontetrachloride-induced liver injury in rats. Chin. J. Nat. Med. 2018, 16, 0271–0283. [Google Scholar] [CrossRef]
- Liu, M.; Zhong, X.; Li, Y.; Zheng, F.; Wu, R.; Sun, Y.; Zhang, J. Xuan Bai Cheng Qi formula as an adjuvant treatment of acute exacerbation of chronic obstructive pulmonary disease of the syndrome type phlegm-heat obstructing the lungs: A multicenter, randomized, double-blind, placebo-controlled clinical trial. BMC Complement. Altern. Med. 2014, 14, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.F.; Zhou, W.; Suthisisang, C.; Yang, J.Y. Traditional medicine for treatment of neurodegenerative diseases. Evid. Based Complement. Alternat. Med. 2014, 2014, 169821. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.-H.; Liu, Y.-D.; Guan, Y.; Liu, N.-W. Effect of Yinian Jiangya Yin on Primary Hypertension in Early Stage—A Clinical Observations on 40 Patients. J. Tradit. Chin. Med. 2010, 30, 171–175. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Han, L.; Sheng, T.; He, Q.; Liang, J. Effects of replenishing qi, promoting blood circulation and resolving phlegm on vascular endothelial function and blood coagulation system in senile patients with hyperlipemia. J. Tradit. Chin. Med. 2006, 26, 120–124. [Google Scholar]
- Meng, F.-C.; Wu, Q.-S.; Wang, R.; Li, S.-P.; Lin, L.-G.; Chen, P.; Zhang, Q.-W. A novel strategy for quantitative analysis of major ginsenosides in Panacis Japonici Rhizoma with a standardized reference fraction. Molecules 2017, 22, 2067. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.; Chen, L.; Li, J.; Wang, Z.; Xin, Z.; Zhang, Y.; Ren, D.; Yi, L. Characterization and authentication of Acori Tatarinowii Rhizoma and its adulterants by UPLC-Orbitrap-MS/MS chromatographic fingerprints, elements profiles and chemometric methods. Microchem. J. 2019, 144, 285–295. [Google Scholar] [CrossRef]
- Zhang, Y.; Qi, D.; Gao, Y.; Liang, C.; Zhang, Y.; Ma, Z.; Liu, Y.; Peng, H.; Zhang, Y.; Qin, H.; et al. History of uses, phytochemistry, pharmacological activities, quality control and toxicity of the root of Stephania tetrandra S. Moore: A review. J. Ethnopharmacol. 2020, 260, 112995. [Google Scholar] [CrossRef]
- Zaini, N.A.M.; Anwar, F.; Hamid, A.A.; Saari, N. Kundur [Benincasa hispida (Thunb.) Cogn.]: A potential source for valuable nutrients and functional foods. Food Res. Int. 2011, 44, 2368–2376. [Google Scholar] [CrossRef]
- Liu, L.; Liu, T.; Li, G.; Wang, Q.; Ng, T. Isolation and determination of p-hydroxybenzoylcholine in traditional Chinese medicine Semen sinapis Albae. Ana.l Bioanal. Chem. 2003, 376, 854–858. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Zheng, S.Q. A meta-analysis of Wendan decoction in the treatment of diabetic gastroparesis. TMR Clin. Res. 2019, 2, 82–90. [Google Scholar]
- Ko, M.M.; Park, T.-Y.; Lee, J.A.; Kang, B.-K.; Lee, J.; Lee, M.S. A Study of Tongue and Pulse Diagnosis in Traditional Korean Medicine for Stroke Patients Based on Quantification Theory Type II. Evid. Based Complement. Altern. Med. 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Wang, J.; Ma, Q.; Li, Y.; Li, P.; Wang, M.; Wang, T.; Wang, C.; Wang, T.; Zhao, B. Research progress on traditional Chinese medicine syndromes of diabetes mellitus. Biomed. Pharmacother. 2020, 121, 109565. [Google Scholar] [CrossRef]
- Wiseman, N.; Ye, F. Theory of Chinese medicine. In A Practical Dictionary of Chinese Medicine, 2nd ed.; Paradigm Publications: Brookline, MA, USA, 1997. [Google Scholar]
- Wu, S.; Jiang, Y.-H.; Yang, C.-H.; Meng, X.-Q.; Hao, N.; Qi, Y.-Z. Establishment and Evaluation of Hypertensive Rat Model with Excessive Accumulation of Phlegm-dampness Syndrome. Zhongguo Zhong Xi Yi Jie He Za Zhi = Chin. J. Integr. Tradit. West. Med. 2016, 36, 222–228. [Google Scholar]
- Zhang, L.; Zhang, Q.; You, Y.; Zhou, M.; Wang, L.; Chen, H.; Yan, X.; Liu, X.; Liu, W. Investigation of evolution rules of phlegm and blood stasis syndrome in hyperlipidemia and atherosclerosis by NMR-based metabolic profiling and metabonomic approaches. Zhongguo Zhong Xi Yi Jie He Za Zhi = Chin. J. Integr. Tradit. West. Med. 2015, 35, 3823–3833. [Google Scholar]
- Braniste, V.; Al-Asmakh, M.; Kowal, C.; Anuar, F.; Abbaspour, A.; Toth, M.; Korecka, A.; Bakocevic, N.; Ng, L.G.; Kundu, P.; et al. The gut microbiota influences blood-brain barrier permeability in mice. Sci. Transl. Med. 2014, 6, 263ra158. [Google Scholar] [CrossRef] [Green Version]
- Main, B.S.; Minter, M.R. Microbial Immuno-Communication in Neurodegenerative Diseases. Front. Neurosci. 2017, 11, 151. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, A.F.; Erickson, M.A.; Rhea, E.M.; Salameh, T.S.; Banks, W.A. Gut reactions: How the blood-brain barrier connects the microbiome and the brain. Exp. Biol. Med. 2018, 243, 159–165. [Google Scholar] [CrossRef]
- Sperber, A.D.; Dekel, R. Irritable bowel syndrome and co-morbid gastrointestinal and extra-gastrointestinal functinoal syndromes. J. Neurogastroenterol. Motil. 2010, 16, 2. [Google Scholar]
- Na, B.-J.; Choi, S.-H. Clinical analysis of the 991 outpatients with gastrointestinal symptoms and extra-gastrointestinal symptoms. J. Korean Orient. Med. 2012, 33, 107–120. [Google Scholar]
- Choi, H.-S.; Kim, J.-K.; Choi, S.-H. Recent advances in diagnosis of gastrointestinal disease. J. Korean Orient. Med. Diagn. 2009, 13, 1–9. [Google Scholar]
- The Society of Phlegm Mass Syndrome. Available online: http://www.phlegmmass.or.kr/ (accessed on 4 February 2021).
- Kim, S.-D.; Choi, S.-H. A case report for the refractory functional dyspepsia treated by Phlegm-Mass Therapy. J. Phlegm Mass Syndr. 2020, 3, 76–80. [Google Scholar]
- Chen, R.; Liang, F.X.; Huang, Y.X.; Li, B. Study on relationship between TCM syndrome types (Xin-qi and Xin-yang deficiency) and contents of cytokines (tumor necrosis factor-alpha and interleukins) in patients with congestive heart failure. Chin. J. Integr. Trad. West Med. 2004, 24, 876–878. [Google Scholar]
- Bi, Y.-F.; Mao, J.-Y.; Wang, X.-L.; Li, B.; Hou, Y.-Z.; Zhao, Z.-Q.; Ge, Y.B.; Zhao, G.F. Expert survey for Chinese medicine syndrome characteristics of different clinical types of coronary artery disease based on the Delphi method. Chin. J. Integr. Trad. West Med. 2014, 34, 1192–1196. [Google Scholar]
- Wu, A.; Zhang, D.; Gao, Y.; Lou, L.; Zhu, H.; Chai, L.; Lv, X.; Sun, Y.; Zhu, L.; Wang, S. The correlation between high-sensitivity c-reactive protein, matrix metallopeptidase, and traditional Chinese medicine syndrome in patients with hypertension. Evid. Based Complement. Alternat. Med. 2013, 2013, 780937. [Google Scholar] [CrossRef] [Green Version]
- Jakobsson, H.E.; Rodriguez-Pineiro, A.M.; Schutte, A.; Ermund, A.; Boysen, P.; Bemark, M.; Sommer, F.; Bäckhed, F.; Hansson, G.C.; Johansson, M.E.V. The composition of the gut microbiota shapes the colon mucus barrier. EMBO Rep. 2015, 16, 164–177. [Google Scholar] [CrossRef]
- Belizario, J.E.; Faintuch, J.; Garay-Malpartida, M. Gut microbiome dysbiosis and immunometabolism: New frontiers for treatment of metabolic diseases. Mediat. Inflamm. 2018, 2018, 2037838. [Google Scholar] [CrossRef]
- Carding, S.; Verbeke, K.; Vipond, D.T.; Corfe, B.M.; Owen, L.J. Dysbiosis of the gut microbiota in disease. Microb. Ecol. Health Dis. 2015, 26, 26191. [Google Scholar] [CrossRef]
- Han, A.; Bennett, N.; Ahmed, B.; Whelan, J.; Donohoe, D.R. Butyrate decreases its own oxidation in colorectal cancer cells through inhibition of histone deacetylases. Oncotarget 2018, 9, 27280–27292. [Google Scholar] [CrossRef]
- Jiminez, J.A.; Uwiera, T.C.; Abbott, D.W.; Uwiera, R.R.E.; Inglis, G.D. Butyrate supplementation at high concentrations alters enteric bacterial communities and reduces intestinal inflammation in mice infected with citrobacter rodentium. MSphere 2017, 2, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saffouri, G.B.; Shields-Cutler, R.R.; Chen, J.; Yang, Y.; Lekatz, H.R.; Hale, V.L.; Cho, J.M.; Battaglioli, E.J.; Bhattarai, Y.; Thompson, K.J.; et al. Small intestinal microbial dysbiosis underlies symptoms associated with functional gastrointestinal disorders. Nat. Commun. 2019, 10, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, X.; Bao, Q.; Di, S.; Zhao, Y.; Zhao, S.; Zhang, H.; Lian, F.; Tong, X. The interaction between the gut microbiota and herbal medicines. Biomed. Pharmacother. 2019, 118, 109252. [Google Scholar] [CrossRef]
- An, K.; Shengjie, Z.; Jinjun, S.; Liuqing, D. Gut microbiota-mediated deglycosylation of ginsenoside Rb1 in rats: In vitro and in vivo insights from quantitative ultra-performance liquid chromatography-mass spectrometry analysis. Anal. Methods 2015, 7, 6173–6181. [Google Scholar] [CrossRef]
- Zeng, M.Y.; Inohara, N.; Nuñez, G. Mechanisms of inflammation-driven bacterial dysbiosis in the gut. Mucosal Immunol. 2017, 10, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, K.A.; Bertha, M.; Hofmekler, T.; Chopra, P.; Vatanen, T.; Srivatsa, A.; Prince, J.; Kumar, A.; Sauer, C.; Zwick, M.E.; et al. Dysbiosis, inflammation, and response to treatment: A longitudinal study of pediatric subjects with newly diagnosed inflammatory bowel disease. Genome Med. 2016, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pickard, J.M.; Zeng, M.Y.; Caruso, R.; Núñez, G. Gut microbiota: Role in pathogen colonization, immune responses, and inflammatory disease. Immunol. Rev. 2017, 279, 70–89. [Google Scholar] [CrossRef] [PubMed]
- Kamada, N.; Seo, S.-U.; Chen, G.Y.; Núñez, G. Role of the gut microbiota in immunity and inflammatory disease. Nat. Rev. Immunol. 2013, 13, 321–335. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Diseases related to Increased GI Barrier Permeability | Diseases Related to Phlegm Syndrome |
| Alzheimer’s disease [42] Acne [40] AIDS, HIV infection [44] Alcoholism [43] Atopy/Eczema [40,53] Autism [41] Cancers [38] Celiac disease [26] Chronic fatigue and immune dysfunction syndrome [46] Chronic arthritis/pain treated with NSAIDs [47] Coronary heart disease [45] Crohn’s disease [17] Cystic fibrosis [48] Dermatitis herpetiformis [49] Diabetes mellitus [33] Gastroenteritis [54] Inflammatory bowel disease [12] Irritable bowel syndrome [55,56] Nonalcoholic fatty liver disease [39] Obesity [33] Pancreatic dysfunction [50] Psoriasis [51] Rheumatoid arthritis [36] Schizophrenia [37] Urticaria [52] Ulcerative colitis [17] | Alzheimer’s disease (dementia) [57] Acne [58] AIDS, HIV infection [59] Asthma [60] Atopy [61] Autism [62] Bronchiectasis [63] Cancers [3] Celiac disease [64] Coronary heart disease [65] Coronary artery disease [66] Diabetes mellitus [67] Irritable bowel syndrome [64] Epilepsy [68] Hyperlipidemia [69] Hypertension [70] Metabolic syndrome [71] Nonalcoholic fatty liver disease [72] Obesity [73] Stroke [74] Scrofula [75] Schizophrenia [76] |
| Symptoms Associated with Leaky Gut Syndrome | Symptoms Associated with Phlegm Syndrome |
| Arthralgias Abdominal distension Abdominal pain Cognitive and memory deficits Diarrhea Fatigue and malaise Fevers of unknown origin Food intolerances Myalgias Poor exercise tolerance Skin rashes Shortness of breath | Bitter taste Tightness in Chest Dizziness Dry mouth and throat Fatigue Feeling muzzy and heaviness in the head and body Forgetfulness General edema Palpitations Insomnia Irritability Sticky mouth Swelling pain of head and eyes |
| Medicinal Plants (MPs) | Major Components 1 | Design | Disease or Beneficial Effects on Health | Primary Mechanism of Action | References |
|---|---|---|---|---|---|
| Flos Lonicera Thunb | organic acids, flavonoids, iridoid glycosides, saponins | in vitro in vivo | obesity obesity related metabolic endotoxemia | regulating of intestinal microbiota and permeability | [77] |
| Cudrania tricuspidata | chlorogenic acid, flavonoids (kaempferol, quercetin) | in vitro in vitro in vivo | atopy the enhancement of tight junction capacity | upregulating both mRNA and protein expressions of claudin-1 | [78,79,80,82] |
| Olea europaea | polyphenols, flavonoids, secoiridoids | in vivo | nonalcoholic steatohepatitis, nonalcoholic fatty liver disease | lowered extracellular signal-regulated kinase activation in hepatocytes | [83] |
| Coptidis rhizome | berberine | in vivo in vitro | ulcerative colitis and Crohn’s disease | suppression of MLCK-MLC phosphorylation signaling pathway | [85,86] |
| Rhizoma Atractylodis Macrocephalae (fermented by Bacillus licheniformis) | sesquiterpene (atractylon, atractylenolide I, II, III), sesquiterpenoid (atractyloside A) | in vitro | several gastrointestinal diseases including food allergies, inflammatory bowel disease, irritable bowel syndrome | protecting on IECs against LPS-insult | [87] |
| Formula | Medicinal Plants | Major Components | Disease or beneficial Effects on Health | Primary Mechanism of Action | References |
|---|---|---|---|---|---|
| Tanrequing (TRQ) | Radix Scutellariae | flavonoids, lignin | Acute exacerbation of chronic obstructive pulmonary disease Phlegm-Heat syndrome | removing internal Heat, releasing internal toxins, and promoting expectoration of Phlegm | [102,103] |
| bear bile powder | - | ||||
| goral horn | - | ||||
| Flos Lonicerae | iridoid, secoiridoid, phenolic, triterpene, triterpene | ||||
| Fructus Forsythiae | phenolic, lignan | ||||
| Xuan Bai Cheng Qi | Gypsum fibrosum (gypsum) | calcium sulfate | Acute exacerbation of chronic obstructive pulmonary disease Phlegm-Heat syndrome | suppressing proinflammatory cytokines including TNF-α, IL-4, IL-8, IL-1β, and IL-6 detected during COPD exacerbation | [105] |
| Rheum officinale Baill (rhubarb root and rhizome) | dianthrone glycoside, anthraquinone | ||||
| Armeniacae amarum (apricot seed or kernel) | amygdalin, prunasin | ||||
| Trichosanthes kirilowii (trichosanthes peel) | triterpene (karounidiol, 3-epidarounidiol, and bryonolol, among others.) | ||||
| Bushenhuatanyizhi | Radix Polygoni Multiflori | emodin, chrysophanol, phycion, rhein, chrysophanol anthrone, resveratrol, piceid, epicatechin | Alzheimer’s disease Phlegm-Dampness and Turbidity syndrome | reinforcing Kidney Essence, removing Phlegm, and promoting mental therapy | [57,106] |
| Rhizoma Panacis Japonici | P. japonicas saponins (Chikusetsusaponin V, Pseudoginsenoside RT1, Chikusetsusaponin IV, Chikusetsusaponin Iva) [109] | ||||
| Rhizoma Acori Tatarinowii | phenylpropanoids (β-asarone, α-asarone, tatarinoids B, isoacoramone), lignin (ligraminol D) [110] | ||||
| Caulis Bambusae In Taeniam | phenylpropanoid (p-coumaric acid) | ||||
| Rhizoma Pinelliae | phenolic (homogentisic acid, 3,4-dihydroxybenzaldehyde) | ||||
| Poria | triterpenoids (pachymic acid, eburicoic acid, and tumulosic acid, among others) | ||||
| Radix Palygalae | saponin (polygalasaponin, tenuifolin), triterpene (senegenin), xanthone (1,2,3,7-teteramethoxyxanthone, 6-hydroxy-1,2,3,7-tetramethoxyxanthone) | ||||
| Qingjian | Nelumbo nucifera (Lotus Leaf) | alkaloids (neferine, nuciferine) flavonoids (catechin, kaempferol, quercetin) | Obesity Phlegm-Dampness syndrome | dissolving Phlegm, removing Dampness, and replenishing spleen and moving Qi | [70] |
| Typha angustifolia L. | saponins, flavonoids, coumarins | ||||
| Stephania tetrandra S.Moore | alkaloids (tetrandrine and fangchinoline, among others), flavonoids (stephaflavone A, stephaflavone B), steroids (β-sitosterol, β-stigmasterol) [111] | ||||
| Benincasa his pida(Thunb.)Cogn | triterpenes (alnusenol, multiflorenol, isomultiflorenol), sterols (lupeol, lupeol acetate, β-sitosterol), glycosides, saccharides, caretenes, β-sitosterin, tannins and uronic acid [112] | ||||
| Astragalus membranaceus (Fisch.) Bunge. | isoflavonoids (astraisoflavan, formonetin, astrapterocarpan), saponins (astragaloside I, isoastragaloside) | ||||
| Cyperus rotundus L. | sesquiterpene (cyperene, cyperol, α-cyperone, cyperotundone, cyperolone) | ||||
| Semen Sinapis Albae | glucosinolate (sinalbin), myrosinase, sinapine, 4-hydroxybenzylamine, p-hydroxybenzyl isothiocyanate, choline, β- sitosterol [113] | ||||
| Atractylodes macrocephala Koidz. | sesquiterpene (atractylon, atractylenolide I, atractylenolide II, atractylenolide III), sesquiterpenoid (atractyloside A) | ||||
| Alisma plantago-aquatica Linn. | triterpenoid (alisol A, alisol A 240acetate, alisol B, alisol B 23-acetate), sesquiterpenoid (alismol) | ||||
| Rheum palmatum L. | Dianthrone glycoside (sennoside A), dianthrone glycoside (sennoside A), anthraquinone (chrysophanol, emodin, aloe-emodin, rhein) | ||||
| gold | - | ||||
| Yinian Jiangya Yin | Ramulus Uncariae cum Uncis | alkaloid (rhynchophylline, corynoxeine, isocorynoxeine, isorhynchophylline, geissochizine methyl ether) | Hypertension Phlegm and blood stasis syndrome | calming the liver, nourishing tendons, removing Phlegm, and clearing Meridians | [107] |
| Concha Haliotidis | CaCo3 | ||||
| Plastrum Testudinis | (+)-4-cholesten-3-one, cholesterol miristate, sterol | ||||
| Rhizoma Pinelliae Praeparata | phenolic (homogentisic acid, 3,4-dihydroxybenzaldehyde) The ingredients of Pinellia ternata Breitenbach were described. | ||||
| Pericarpium Citri Reticulatae | flavonoids (hesperidin, neohesperidin, poncirin and naringin, among others), monoterpene | ||||
| Fructus Aurantii | flavonoids (hesperidin, neohesperidin, poncirin, naringin), monoterpene | ||||
| Herba Leonuri | alkaloids (leonurine, stachydrine), flavonoid (rutin), terpene (prehispanolone, leosibirin) | ||||
| Radix Achyranthis Bidentatae | steroids (ecdysterone, inokosterone, ponasteroside A, rubrosterone) | ||||
| Ramulus Loranthi | flavonoids (avicularin, quercitrin), terpene (oleanolic acid, a-amyrin, corianin) | ||||
| Radix Polygoni Multiflori | emodin, chrysophanol, phycion, rhein, chrysophanol anthrone, resveratrol, piceid, epicatechin | ||||
| Danshen Jueming | Radix Pseudostellariae | palmitic acid, linoleic acid, glycenal 1-monolinolate, behenic acid, 2-minaline | Hyperlipemia Phlegm syndrome | regulating blood lipid and metabolism of lipoproteins in senile hyperlipemia | [108] |
| Radix Salviae Miltiorrhizae | penolic (salvianolic acid B), diterpene (tanshinone I, tanshinone IIA, miltirone, cryptotanshinone) | ||||
| Semen Cassiae | anthraquinone (chrysophanoll, physcion, emodin, obtusifolin, obtusin) | ||||
| Fructus Crataegi | flavonoid (quercetin), pinnatifinoside A, B, C, crataegolic acid | ||||
| Rhizoma Alismatis | triterpenoid (alisol A, alisol A 24-acetate, alisol B, alisol B 23-acetate, alismol), sesquiterpenoid (alismol) | ||||
| Pericarpium Citri Reticulatae | flavonoids (hesperidin, neohesperidin, poncirin, and naringin, among others), monoterpene | ||||
| Hirudo | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Choi, T.J.; Kang, K.S.; Choi, S.-H. The Interrelationships between Intestinal Permeability and Phlegm Syndrome and Therapeutic Potential of Some Medicinal Herbs. Biomolecules 2021, 11, 284. https://doi.org/10.3390/biom11020284
Park J, Choi TJ, Kang KS, Choi S-H. The Interrelationships between Intestinal Permeability and Phlegm Syndrome and Therapeutic Potential of Some Medicinal Herbs. Biomolecules. 2021; 11(2):284. https://doi.org/10.3390/biom11020284
Chicago/Turabian StylePark, Junghyun, Tae Joon Choi, Ki Sung Kang, and Seo-Hyung Choi. 2021. "The Interrelationships between Intestinal Permeability and Phlegm Syndrome and Therapeutic Potential of Some Medicinal Herbs" Biomolecules 11, no. 2: 284. https://doi.org/10.3390/biom11020284
APA StylePark, J., Choi, T. J., Kang, K. S., & Choi, S. -H. (2021). The Interrelationships between Intestinal Permeability and Phlegm Syndrome and Therapeutic Potential of Some Medicinal Herbs. Biomolecules, 11(2), 284. https://doi.org/10.3390/biom11020284