
Effects of Systemic or Local Administration of Mesenchymal Stem Cells from Patients with Osteoporosis or Osteoarthritis on Femoral Fracture Healing in a Mouse Model

 ,
,  , ,
, ,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Isolation and Culture of Human MSCs
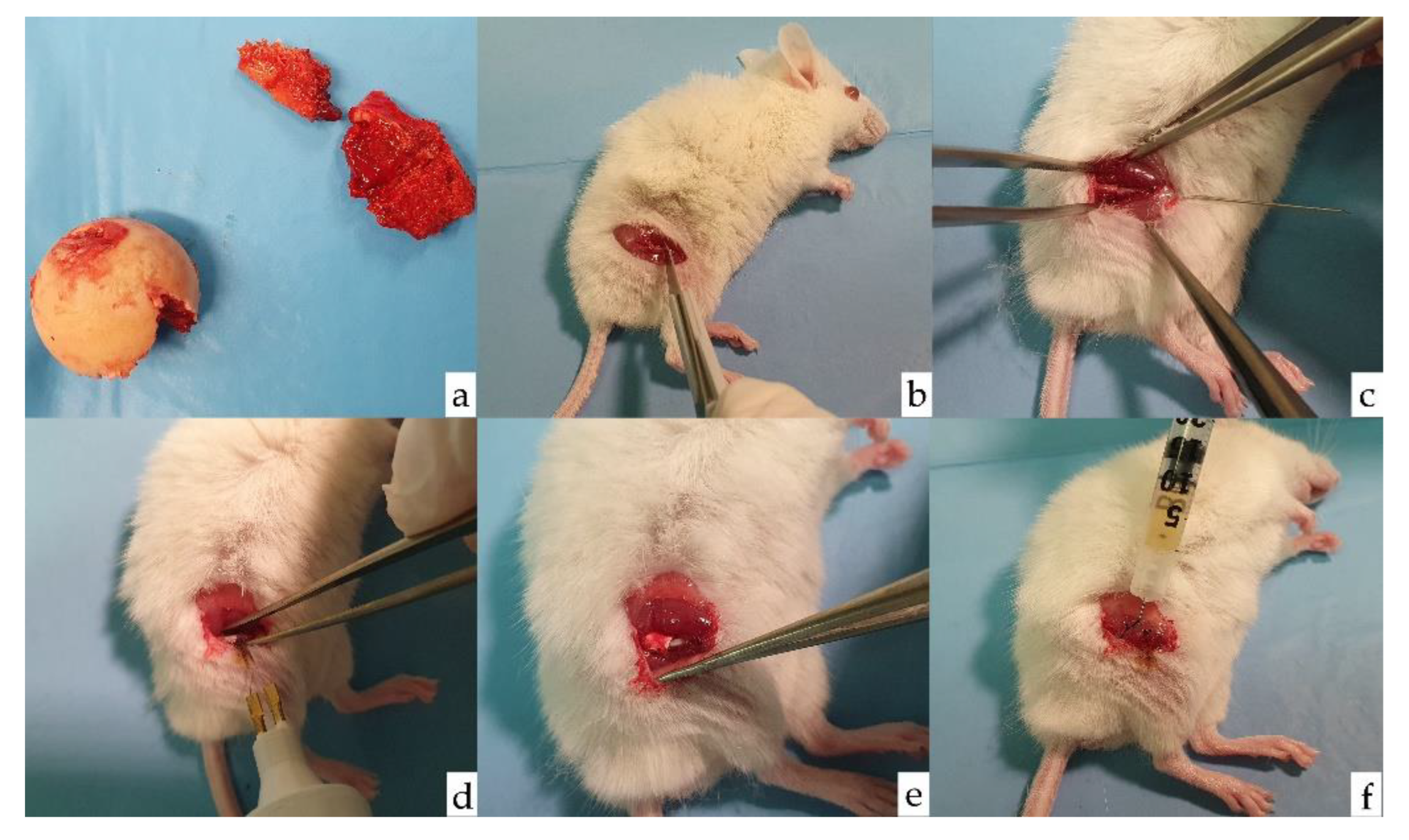
2.2. Experimental Animals and Surgical Procedures
2.3. Experimental Groups
2.4. Radiological Analysis
2.5. Histological Analysis
2.6. Data Analysis
3. Results
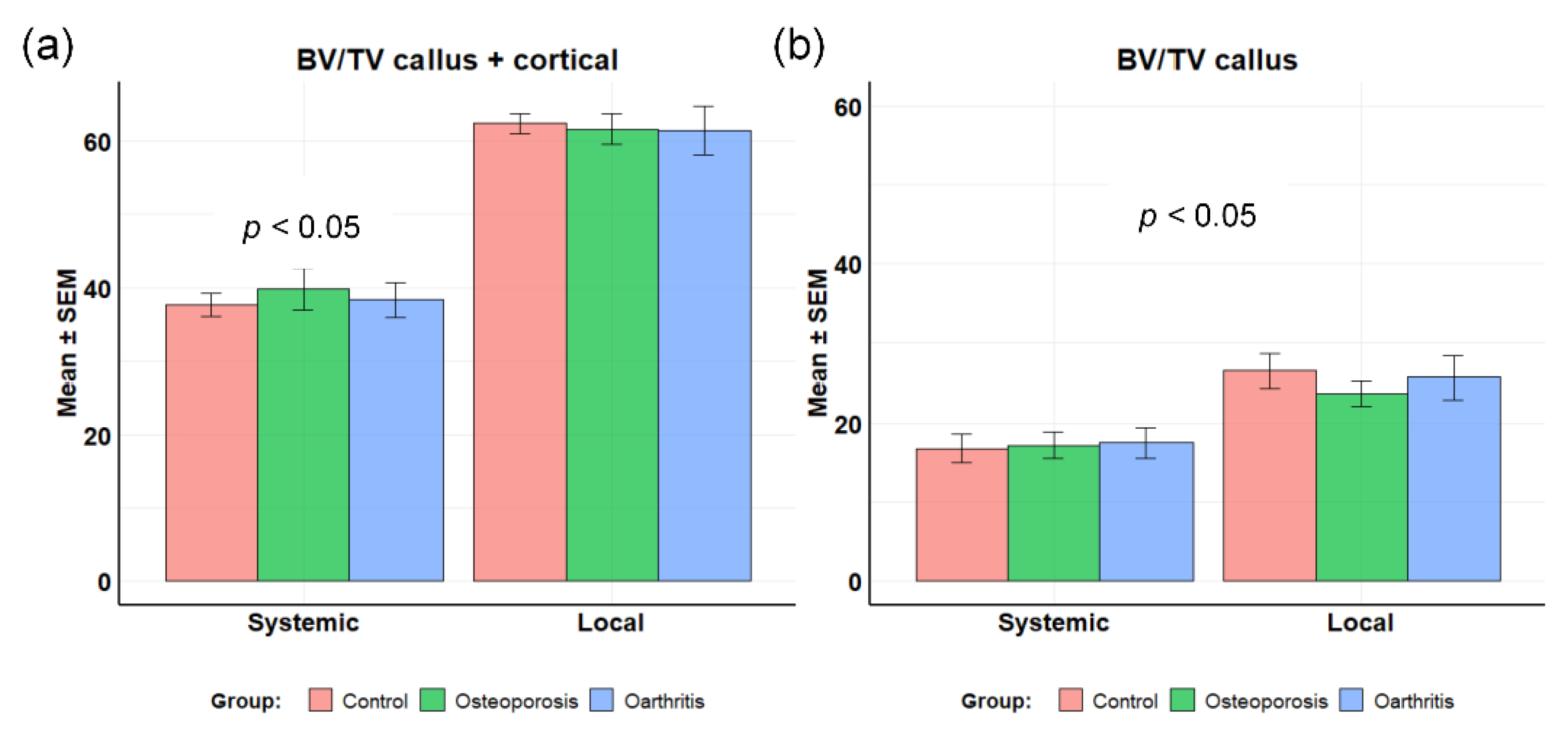
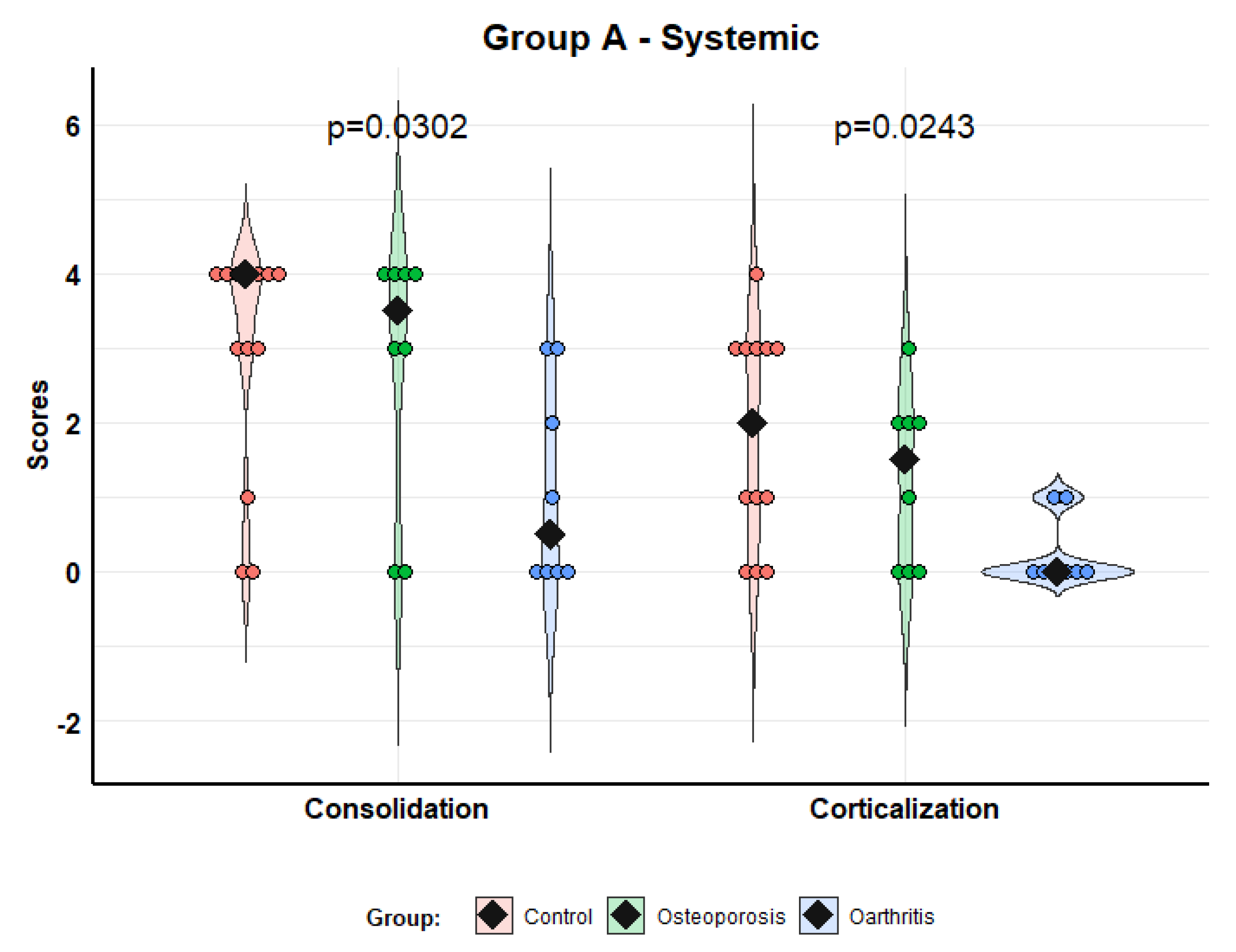
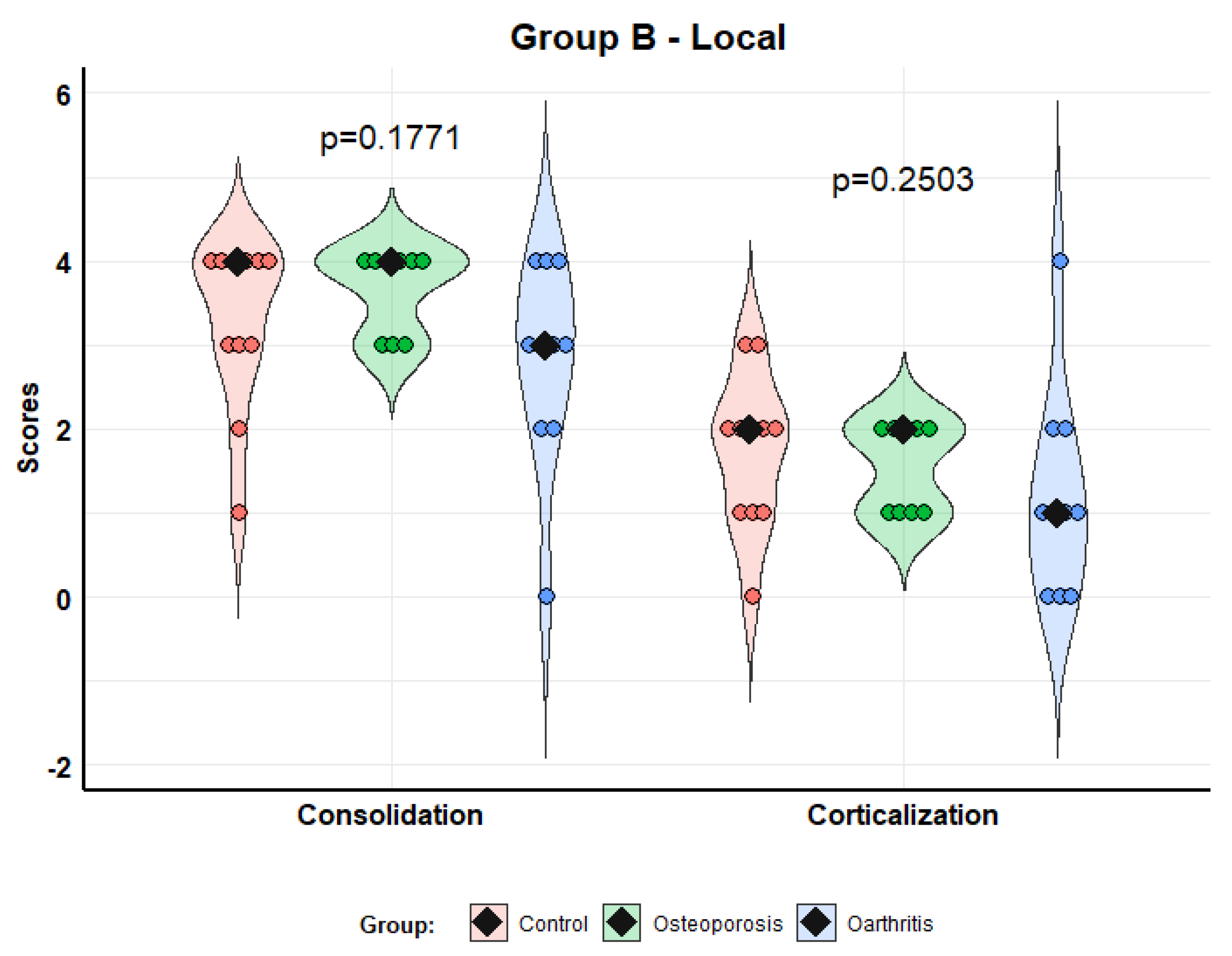
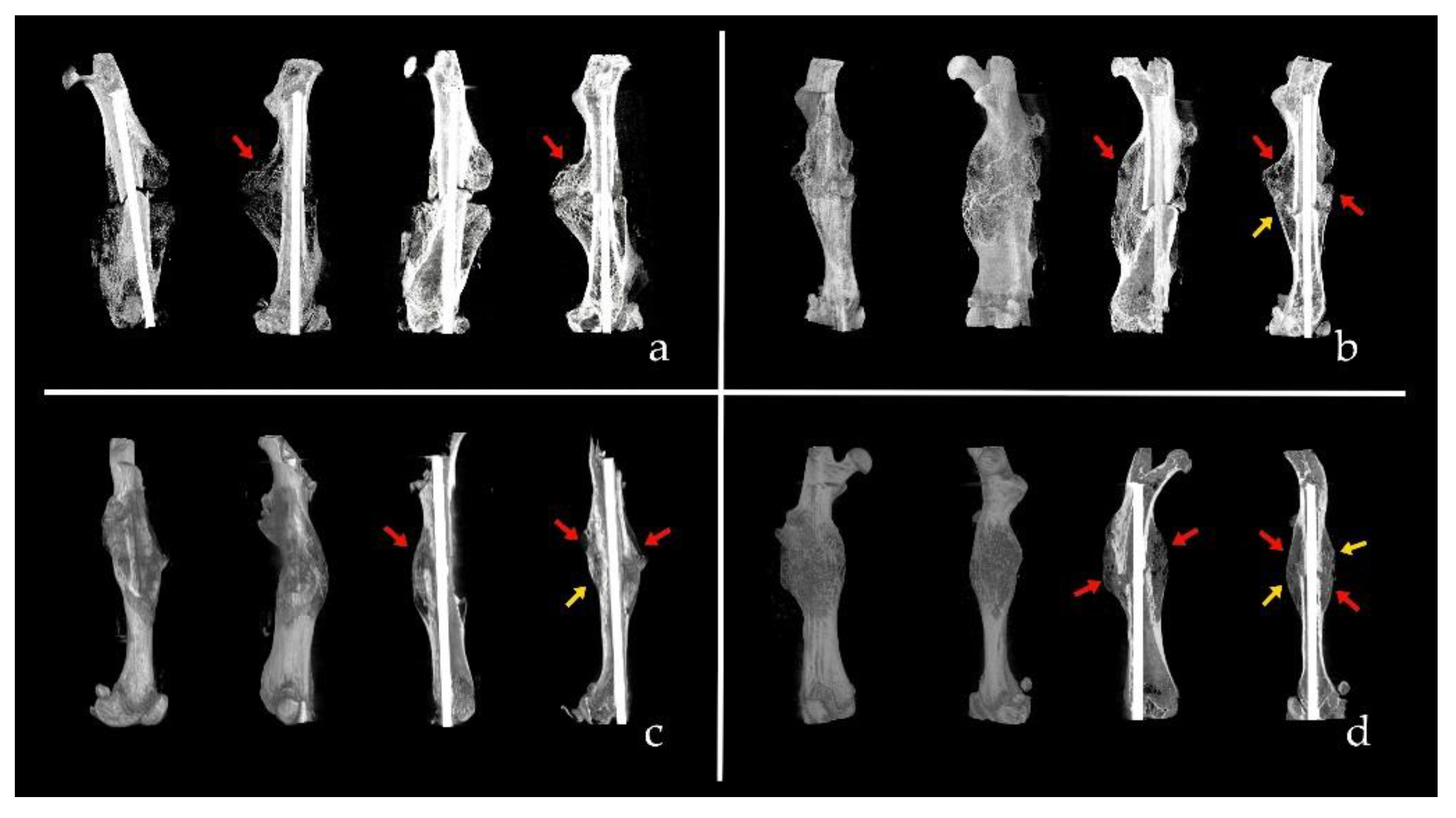
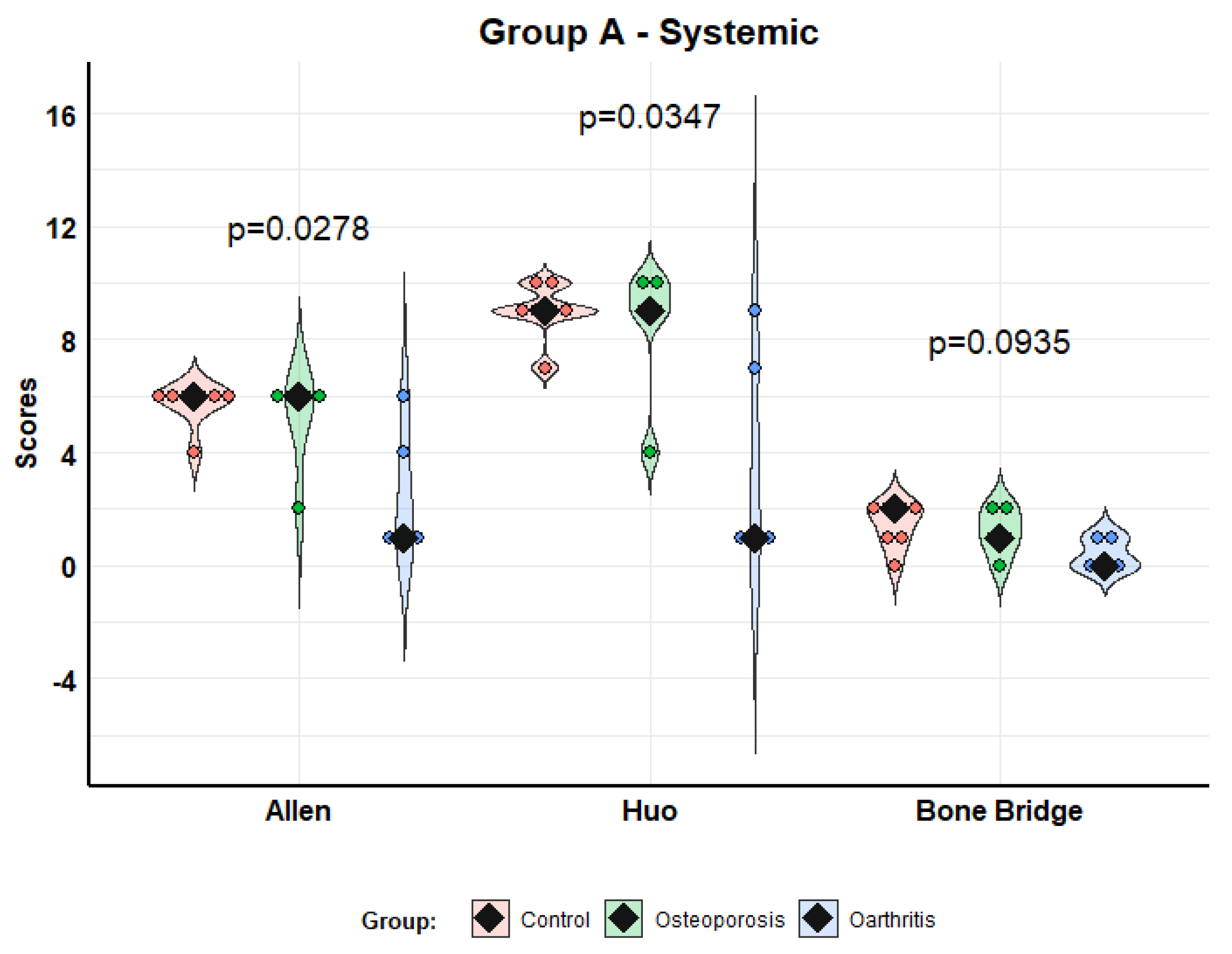
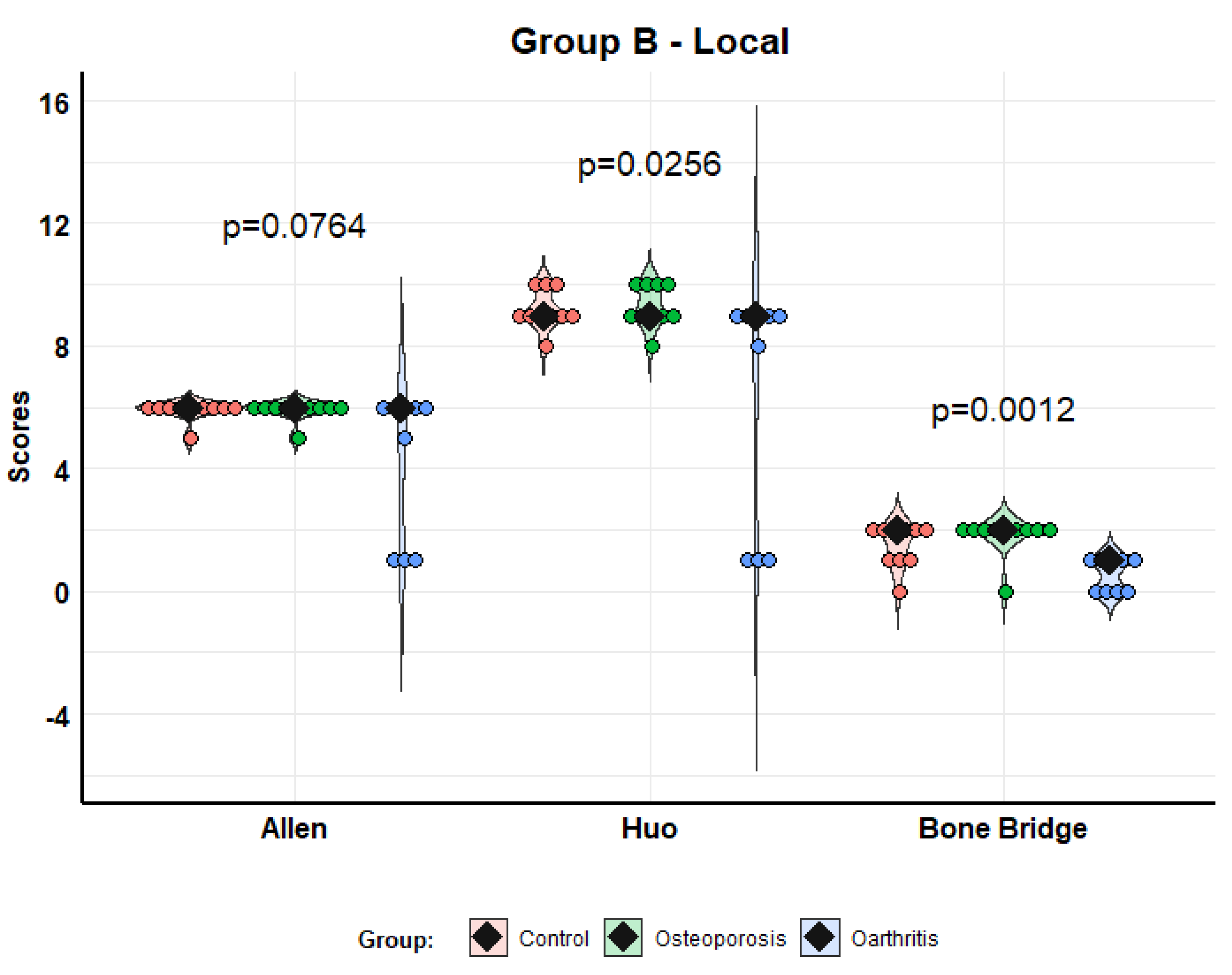
3.1. Radiological Study
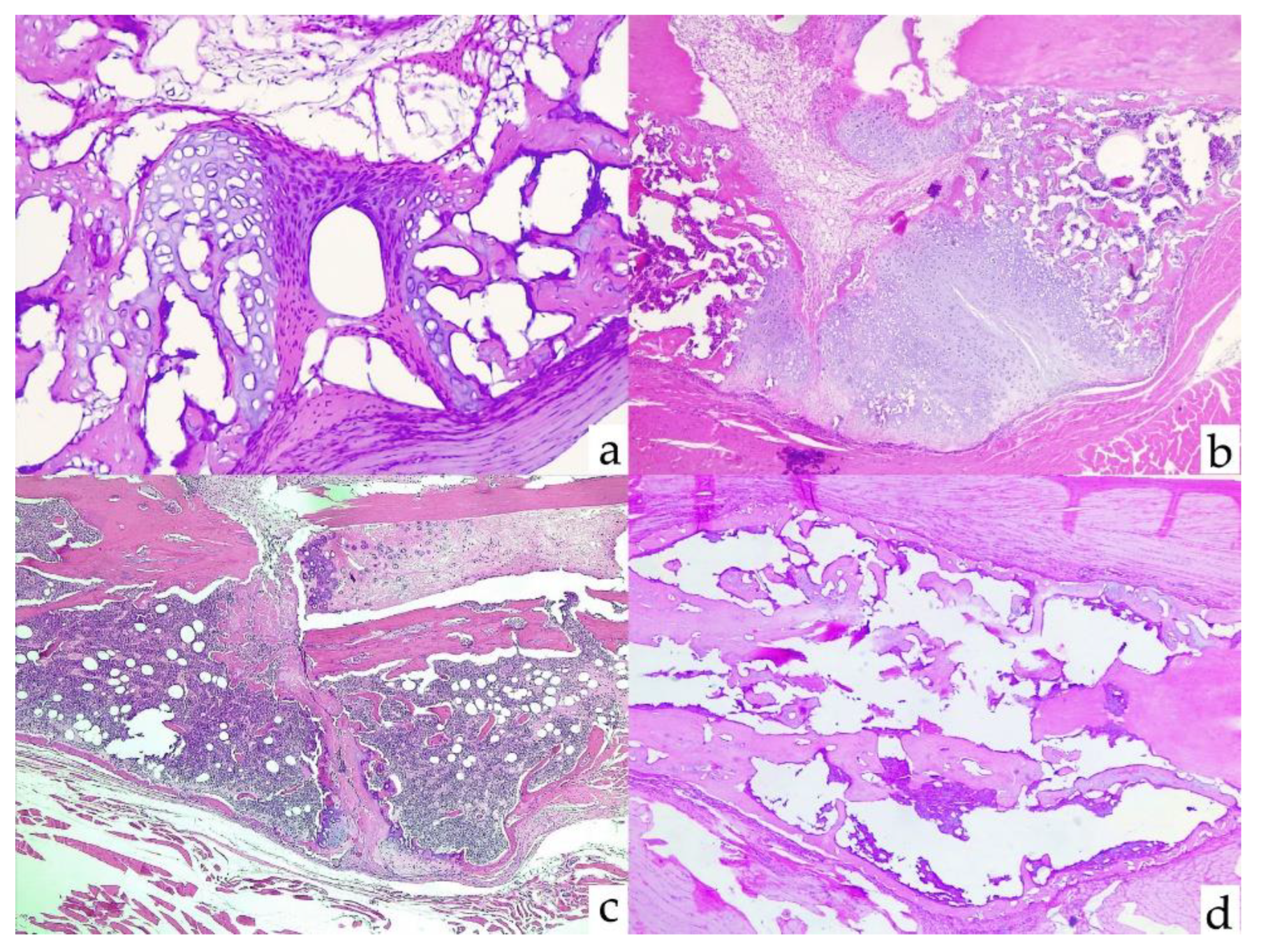
3.2. Fracture Histology
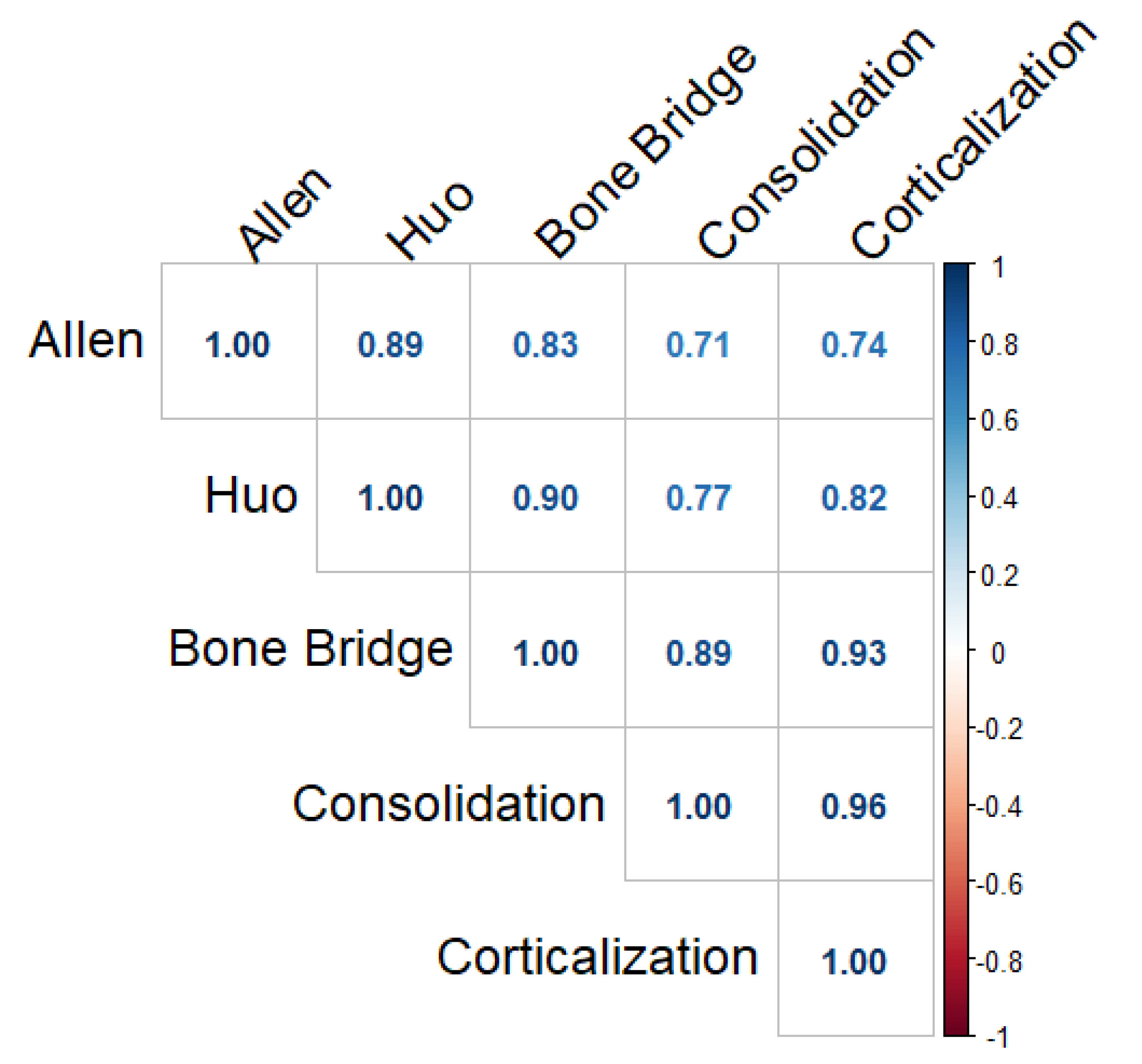
3.3. Correlation between Radiological and Histological Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Assiotis, A.; Sachinis, N.P.; Chalidis, B.E. Pulsed electromagnetic fields for the treatment of tibial delayed unions and nonunions. A prospective clinical study and review of the literature. J. Orthop. Surg. Res. 2012, 7, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, A.N.; Donahue, S.W.; Wojda, S.J.; McIlwraith, C.W.; Kawcak, C.E.; Ehrhart, N.; Goodrich, L.R. The challenges of promoting osteogenesis in segmental bone defects and osteoporosis: Challenges of Promoting Osteogenesis. J. Orthop. Res. 2018, 36, 1559–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, P.; Histing, T.; Holstein, J.H.; Klein, M.; Laschke, M.W.; Matthys, R.; Menger, M.D. Rodent animal models of delayed bone healing and non-union formation: A comprehensive review. Eur. Cell Mater. 2013, 26, 1–12, discussion 12–14. [Google Scholar] [CrossRef] [PubMed]
- Schlickewei, C.W.; Kleinertz, H.; Thiesen, D.M.; Mader, K.; Priemel, M.; Frosch, K.-H.; Keller, J. Current and Future Concepts for the Treatment of Impaired Fracture Healing. Int. J. Mol. Sci. 2019, 20, 5805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez-Barrena, E.; Rosset, P.; Lozano, D.; Stanovici, J.; Ermthaller, C.; Gerbhard, F. Bone fracture healing: Cell therapy in delayed unions and nonunions. Bone 2015, 70, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Katsimbri, P. The biology of normal bone remodeling. Eur. J. Cancer Care 2017, 26, e12740. [Google Scholar] [CrossRef]
- Bentivegna, A.; Roversi, G.; Riva, G.; Paoletta, L.; Redaelli, S.; Miloso, M.; Dalprà, L. The Effect of Culture on Human Bone Marrow Mesenchymal Stem Cells: Focus on DNA Methylation Profiles. Stem Cells Int. 2016, 2016, 5656701. [Google Scholar] [CrossRef] [Green Version]
- Iaquinta, M.R.; Mazzoni, E.; Manfrini, M.; D’Agostino, A.; Trevisiol, L.; Nocini, R.; Trombelli, L.; Barbanti-Brodano, G.; Martini, F.; Tognon, M. Innovative biomaterials for bone regrowth. Int. J. Mol. Sci. 2019, 20, 618. [Google Scholar] [CrossRef] [Green Version]
- Abdel Meguid, E.; Ke, Y.; Ji, J.; El-Hashash, A.H.K. Stem cells applications in bone and tooth repair and regeneration: New insights, tools, and hopes. J. Cell. Physiol. 2018, 233, 1825–1835. [Google Scholar] [CrossRef]
- Takeuchi, R.; Katagiri, W.; Endo, S.; Kobayashi, T. Exosomes from conditioned media of bone marrow-derived mesenchymal stem cells promote bone regeneration by enhancing angiogenesis. PLoS ONE 2019, 14, e0225472. [Google Scholar] [CrossRef]
- Yang, X.; Yang, J.; Lei, P.; Wen, T. LncRNA MALAT1 shuttled by bone marrow-derived mesenchymal stem cells-secreted exosomes alleviates osteoporosis through mediating microRNA-34c/SATB2 axis. Aging (Albany NY) 2019, 11, 8777–8791. [Google Scholar] [CrossRef] [PubMed]
- Crivelli, B.; Chlapanidas, T.; Perteghella, S.; Lucarelli, E.; Pascucci, L.; Brini, A.T.; Ferrero, I.; Marazzi, M.; Pessina, A.; Torre, A.L. Mesenchymal stem/stromal cell extracellular vesicles: From active principle to next generation drug delivery system. J. Control. Release 2017, 262, 104–117. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Li, X.; Zhang, Y.; Han, Y.; Chang, F.; Ding, J. Mesenchymal Stem Cells for Regenerative Medicine. Cells 2019, 8, 886. [Google Scholar] [CrossRef] [Green Version]
- Hou, W.; Ye, C.; Li, W.; Zhang, W.; He, R.; Zheng, Q. Bioengineering application using co-cultured mesenchymal stem cells and preosteoclasts may effectively accelerate fracture healing. Med. Hypotheses 2019, 123, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Iaquinta, M.R.; Mazzoni, E.; Bononi, I.; Rotondo, J.C.; Mazziotta, C.; Montesi, M.; Sprio, S.; Tampieri, A.; Tognon, M.; Martini, F. Adult Stem Cells for Bone Regeneration and Repair. Front. Cell Dev. Biol. 2019, 7, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.; McKee, C.; Bakshi, S.; Walker, K.; Hakman, E.; Halassy, S.; Svinarich, D.; Dodds, R.; Govind, C.K.; Chaudhry, G.R. Mesenchymal stem cells: Cell therapy and regeneration potential. J. Tissue Eng. Regen. Med. 2019, 13, 1738–1755. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.-H.; Ho, K.-N.; Lee, Y.-B.; Chou, M.-J.; Lew, W.-Z.; Huang, H.-M.; Lai, P.-C.; Feng, S.-W. Melatonin enhances osteogenic differentiation of dental pulp mesenchymal stem cells by regulating MAPK pathways and promotes the efficiency of bone regeneration in calvarial bone defects. Stem Cell Res. Ther. 2022, 13, 73. [Google Scholar] [CrossRef]
- López-Delgado, L.; Del Real, A.; Sañudo, C.; Garcia-Ibarbia, C.; Laguna, E.; Menendez, G.; Garcia-Montesinos, B.; Santurtun, A.; Merino, J.; Pérez-Núñez, I.M.; et al. Osteogenic capacity of mesenchymal stem cells from patients with osteoporotic hip fractures in vivo. Connect. Tissue Res. 2022, 63, 243–255. [Google Scholar] [CrossRef]
- Del Real, A.; Pérez-Campo, F.M.; Fernández, A.F.; Sañudo, C.; Ibarbia, C.G.; Pérez-Núñez, M.I.; Criekinge, W.V.; Braspenning, M.; Alonso, M.A.; Fraga, M.F.; et al. Differential analysis of genome-wide methylation and gene expression in mesenchymal stem cells of patients with fractures and osteoarthritis. Epigenetics 2017, 12, 113–122. [Google Scholar] [CrossRef]
- Farr, J.N.; Khosla, S. Cellular Senescence in Bone. Bone 2019, 121, 121–133. [Google Scholar] [CrossRef]
- Farr, J.N.; Fraser, D.G.; Wang, H.; Jaehn, K.; Ogrodnik, M.B.; Weivoda, M.M.; Drake, M.T.; Tchkonia, T.; LeBrasseur, K.N.; Kirkland, J.L. Identification of Senescent Cells in the Bone Microenvironment. J. Bone Miner. Res. 2016, 31, 1920–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farr, J.N.; Xu, M.; Weivoda, M.M.; Monroe, D.G.; Fraser, D.G.; Onken, J.L.; Negley, B.A.; Sfeir, J.G.; Ogrodnik, M.B.; Hachfeld, C.M.; et al. Targeting cellular senescence prevents age-related bone loss in mice. Nat. Med. 2017, 23, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Allen, H.L.; Wase, A.; Bear, W.T. Indomethacin and aspirin: Effect of nonsteroidal anti-inflammatory agents on the rate of fracture repair in the rat. Acta Orthop. Scand. 1980, 51, 595–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, M.H.; Troiano, N.W.; Pelker, R.R.; Gundberg, C.M.; Friedlaender, G.E. The influence of ibuprofen on fracture repair: Biomechanical, biochemical, histologic, and histomorphometric parameters in rats. J. Orthop. Res. 1991, 9, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Yin, C.; Zhao, F.; Ali, A.; Ma, J.; Qian, A. Mesenchymal Stem Cells: Cell Fate Decision to Osteoblast or Adipocyte and Application in Osteoporosis Treatment. Int. J. Mol. Sci. 2018, 19, 360. [Google Scholar] [CrossRef] [Green Version]
- Iso, Y.; Yamaya, S.; Sato, T.; Poole, C.N.; Isoyama, K.; Mimura, M.; Shinji, K.; Youichi, K.; Youichi, T.; Jeffrey, L.S. Distinct mobilization of circulating CD271+ mesenchymal progenitors from hematopoietic progenitors during aging and after myocardial infarction. Stem Cells Transl. Med. 2012, 1, 462–468. [Google Scholar] [CrossRef]
- Watson, L.; Elliman, S.J.; Coleman, C.M. From isolation to implantation: A concise review of mesenchymal stem cell therapy in bone fracture repair. Stem Cell Res. Ther. 2014, 5, 51. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.; Xu, L.; Zhang, Y.; Sun, Y.; Li, G. Systemic and Local Administration of Allogeneic Bone Marrow-Derived Mesenchymal Stem Cells Promotes Fracture Healing in Rats. Cell Transplant. 2015, 24, 2643–2655. [Google Scholar] [CrossRef] [Green Version]
- Funakoshi, K.; Bagheri, M.; Zhou, M.; Suzuki, R.; Abe, H.; Akashi, H. Highly sensitive and specific Alu-based quantification of human cells among rodent cells. Sci. Rep. 2017, 7, 13202. [Google Scholar] [CrossRef]
- Chikate, T.R.; Tang, L. Tracking and Imaging of Transplanted Stem Cells in Animals. Methods Mol. Biol. 2020, 2150, 45–56. [Google Scholar] [CrossRef]
- Real, A.D.; López-Delgado, L.; Sañudo, C.; Pérez-Núñez, M.I.; Laguna, E.; Menéndez, G.; Garcés, C.; García-Montesinos, B.; García-Ibarbia, C.; Santurtún, A.; et al. Método sensible para monitorizar la migración de las células madre mesenquimales de la médula ósea en modelos murinos. Rev. Osteoporos Metab. Miner. 2020, 12, 40–44. [Google Scholar] [CrossRef]
- Chen, R.; Hao, Z.; Wang, Y.; Zhu, H.; Hu, Y.; Chen, T.; Zhang, P.; Li, J. Mesenchymal Stem Cell–Immune Cell Interaction and Related Modulations for Bone Tissue Engineering. Stem Cells Int. 2022, 2022, 7153584. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALLEN | |
|---|---|
| Score | Histological Findings |
| 1 | Pseudoarthrosis: fibrous tissue between the fragments |
| 2 | Incomplete union: fibrous and cartilaginous tissue |
| 3 | Complete union with cartilaginous tissue |
| 4 | Incomplete bone union with areas of ossification: the equivalent amount of cartilage and trabecular bone |
| 5 | Incomplete bone union with a predominance of bone cells |
| 6 | Complete bone consolidation: bone between both bone fragments |
| HUO | |
| Score | Histological findings |
| 1 | Fibrous tissue |
| 2 | Predominantly fibrous tissue with a small amount of cartilage |
| 3 | An equal mixture of fibrous and cartilaginous tissue |
| 4 | Predominantly cartilage with a small amount of fibrous tissue |
| 5 | Cartilage |
| 6 | Predominantly cartilage with a small amount of immature bone |
| 7 | An equal mixture of cartilage and immature bone |
| 8 | Predominantly immature bone with a small amount of cartilage |
| 9 | Union of fracture fragments by immature bone |
| 10 | Union of fracture fragments by mature bone |
| BONE BRIDGE | |
| Score | Histological findings |
| 0 | No bone bridge |
| 1 | Bone bridge in one cortex |
| 2 | Bone bridge in two cortices |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laguna, E.; Pérez-Núñez, M.I.; del Real, Á.; Menéndez, G.; Sáinz-Aja, J.A.; López-Delgado, L.; Sañudo, C.; Martín, A.; Mazorra, R.; Ferreño, D.; et al. Effects of Systemic or Local Administration of Mesenchymal Stem Cells from Patients with Osteoporosis or Osteoarthritis on Femoral Fracture Healing in a Mouse Model. Biomolecules 2022, 12, 722. https://doi.org/10.3390/biom12050722
Laguna E, Pérez-Núñez MI, del Real Á, Menéndez G, Sáinz-Aja JA, López-Delgado L, Sañudo C, Martín A, Mazorra R, Ferreño D, et al. Effects of Systemic or Local Administration of Mesenchymal Stem Cells from Patients with Osteoporosis or Osteoarthritis on Femoral Fracture Healing in a Mouse Model. Biomolecules. 2022; 12(5):722. https://doi.org/10.3390/biom12050722
Chicago/Turabian StyleLaguna, Esther, María Isabel Pérez-Núñez, Álvaro del Real, Guillermo Menéndez, José A. Sáinz-Aja, Laura López-Delgado, Carolina Sañudo, Alicia Martín, Remigio Mazorra, Diego Ferreño, and et al. 2022. "Effects of Systemic or Local Administration of Mesenchymal Stem Cells from Patients with Osteoporosis or Osteoarthritis on Femoral Fracture Healing in a Mouse Model" Biomolecules 12, no. 5: 722. https://doi.org/10.3390/biom12050722
APA StyleLaguna, E., Pérez-Núñez, M. I., del Real, Á., Menéndez, G., Sáinz-Aja, J. A., López-Delgado, L., Sañudo, C., Martín, A., Mazorra, R., Ferreño, D., García-Montesinos, B., & Riancho, J. A. (2022). Effects of Systemic or Local Administration of Mesenchymal Stem Cells from Patients with Osteoporosis or Osteoarthritis on Femoral Fracture Healing in a Mouse Model. Biomolecules, 12(5), 722. https://doi.org/10.3390/biom12050722