
Pathogenetic Mechanisms of Liver-Associated Injuries, Management, and Current Challenges in COVID-19 Patients

 ,
,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
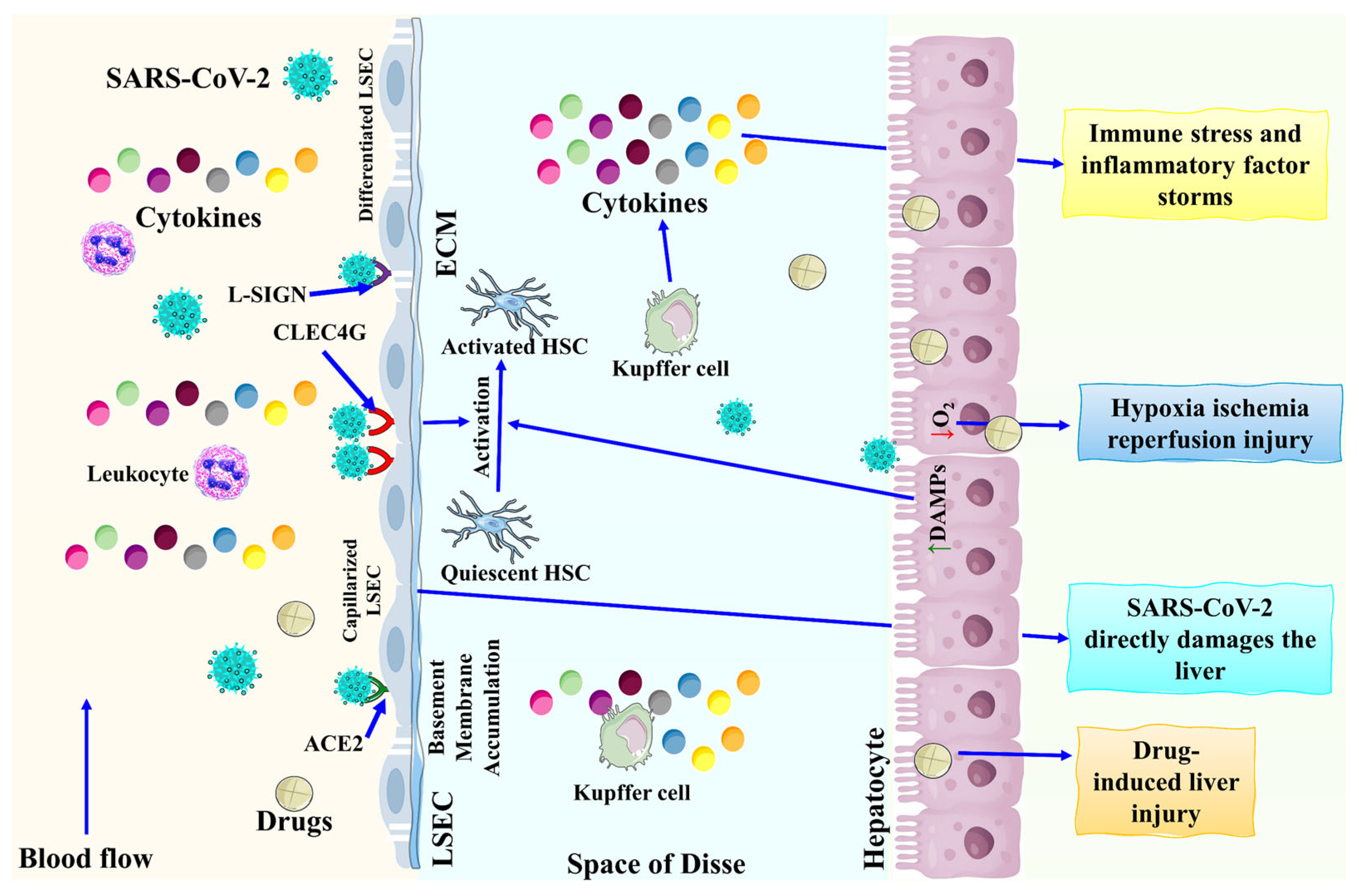
2. Pathophysiological Mechanisms of COVID-19-Associated Liver Injury
2.1. Hepatotropism Mechanisms of Liver Injury
2.2. Hepatic Ischemia and Hypoxia Reperfusion Injury
2.3. A Mechanism for Hyper-Inflammation of CRS and RAS Livery Injury
2.4. Drug-Induced Liver Injury
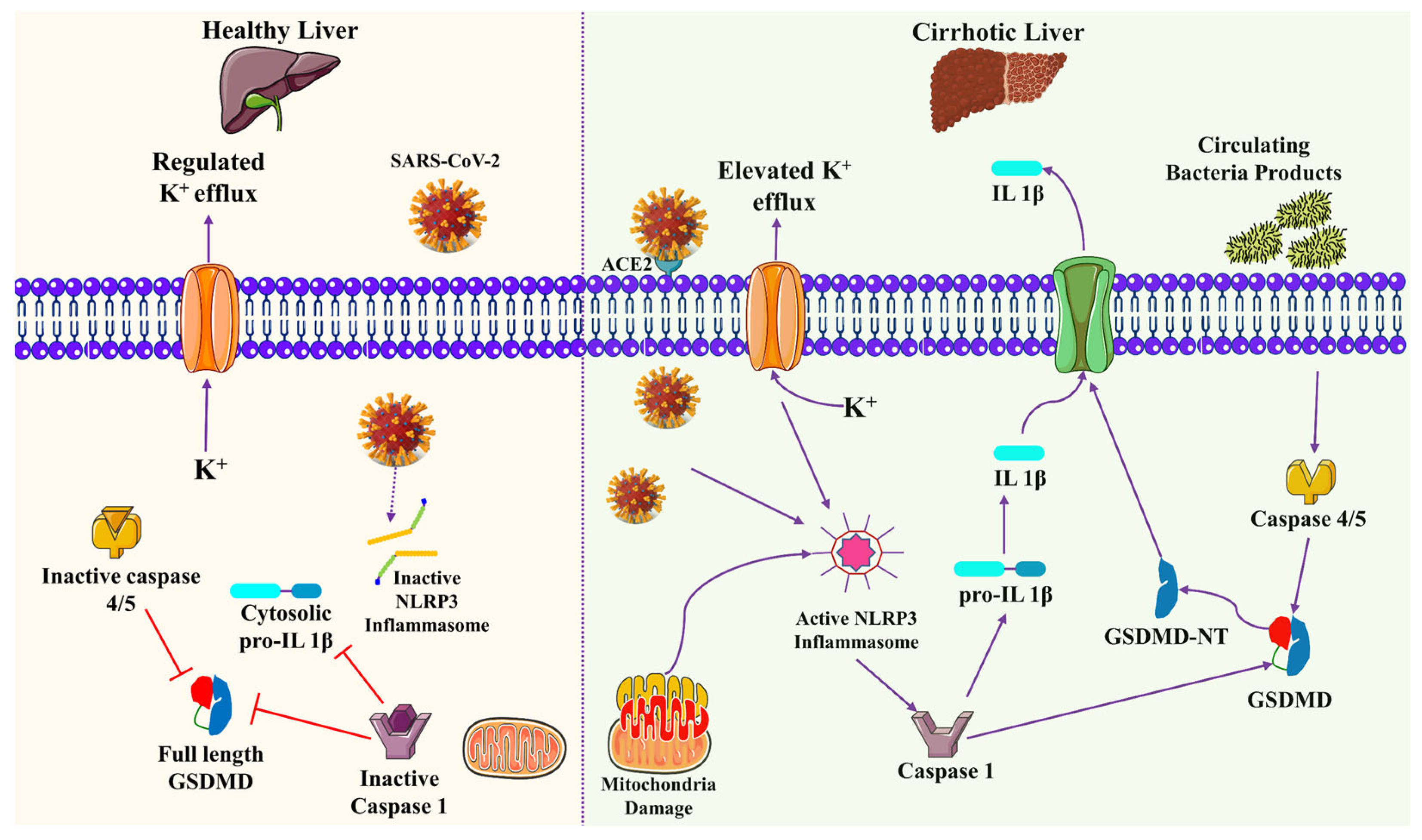
2.5. Mitochondrial Dysfunctional Liver Injury
3. Chronic Liver Disease in COVID-19 Patients
3.1. Non-Alcoholic Fatty Liver Disease (NAFLD)
3.2. Alcohol-Related Liver Disease (ARLD)
3.3. Liver Cirrhosis and Hepatocellular Carcinoma
3.4. Liver Transplantation
4. Management of Liver Injury in COVID-19 Patients
4.1. Non-Alcoholic Fatty Liver Disease (NAFLD)
4.2. Autoimmune Hepatitis
4.3. Liver Cirrhosis and Hepatocellular Carcinoma (HCC)
5. Current Challenges of Liver Injury in COVID-19 Patients
6. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19); StatPearl: Treasure Island, FL, USA, 2022. [Google Scholar]
- Du, M.; Yang, S.; Liu, M.; Liu, J. COVID-19 and liver dysfunction: Epidemiology, association and potential mechanisms. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101793. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Huang, D.; Yu, H.; Zhu, Z.; Xia, Z.; Su, Y.; Li, Z.; Zhou, G.; Gou, J.; Qu, J. COVID-19: Abnormal liver function tests. J. Hepatol. 2020, 73, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Effenberger, M.; Grander, C.; Grabherr, F.; Griesmacher, A.; Ploner, T.; Hartig, F.; Bellmann-Weiler, R.; Joannidis, M.; Zoller, H.; Weiss, G. Systemic inflammation as fuel for acute liver injury in COVID-19. Dig. Liver Dis. 2021, 53, 158–165. [Google Scholar] [CrossRef]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef]
- Leowattana, W. Angiotensin-converting enzyme 2 receptors, chronic liver diseases, common medications, and clinical outcomes in coronavirus disease 2019 patients. World J. Virol. 2021, 10, 86–96. [Google Scholar] [CrossRef]
- Zhong, P.; Xu, J.; Yang, D.; Shen, Y.; Wang, L.; Feng, Y.; Du, C.; Song, Y.; Wu, C.; Hu, X. COVID-19-associated gastrointestinal and liver injury: Clinical features and potential mechanisms. Signal Transduct. Target Ther. 2020, 5, 256. [Google Scholar] [CrossRef]
- Sodeifian, F.; Seyedalhosseini, Z.S.; Kian, N.; Eftekhari, M.; Najari, S.; Mirsaeidi, M.; Farsi, Y.; Nasiri, M.J. Drug-induced liver injury in COVID-19 patients: A systematic review. Front. Med. 2021, 8, 731436. [Google Scholar] [CrossRef]
- Moon, A.M.; Curtis, B.; Mandrekar, P.; Singal, A.K.; Verna, E.C.; Fix, O.K. Alcohol-Associated Liver Disease Before and After COVID-19—An Overview and Call for Ongoing Investigation. Hepatol. Commun. 2021, 5, 1616–1621. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Sepanlou, S.G.; Safiri, S.; Bisignano, C.; Ikuta, K.S.; Merat, S.; Saberifiroozi, M.; Poustchi, H.; Tsoi, D.; Colombara, D.V.; Abdoli, A. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 245–266. [Google Scholar] [CrossRef] [Green Version]
- Elghannam, M.T.; Hassanien, M.H.; Ameen, Y.A.; ELattar, G.M.; ELRay, A.A.; Turky, E.A.; ELTalkawy, M.D. COVID-19 and liver diseases. Egypt Liver J. 2022, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Liu, Y.; Cheng, Z.; Yu, X.; Li, Y. COVID-19-associated liver injury: Clinical characteristics, pathophysiological mechanisms and treatment management. Biomed. Pharmacother. 2022, 154, 113568. [Google Scholar] [CrossRef] [PubMed]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.v.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Pirola, C.J.; Sookoian, S. SARS-CoV-2 virus and liver expression of host receptors: Putative mechanisms of liver involvement in COVID-19. Liver Int. 2020, 40, 2038–2040. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Khlegi, A.; Sekaran, A.; Reddy, R.; Sharma, M.; Tirumalle, S.; Gora, B.A.; Somireddy, A.; Reddy, J.; Menon, B. POST COVID-19 Cholestasis: A case series and review of literature. J. Clin. Exp. Hepatol. 2022, 12, 1580–1590. [Google Scholar] [CrossRef]
- Zhao, B.; Ni, C.; Gao, R.; Wang, Y.; Yang, L.; Wei, J.; Lv, T.; Liang, J.; Zhang, Q.; Xu, W. Recapitulation of SARS-CoV-2 infection and cholangiocyte damage with human liver ductal organoids. Protein Cell 2020, 11, 771–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Q.; Xie, Q.; Shi, C.-C.; Xiang, X.-G.; Lin, L.-Y.; Gong, B.-D.; Zhao, G.-D.; Wang, H.; Jia, N.-N. Expression of angiotensin-converting enzyme 2 in CCL4-induced rat liver fibrosis. Int. J. Mol. Med. 2009, 23, 717–723. [Google Scholar]
- Wei, C.; Wan, L.; Yan, Q.; Wang, X.; Zhang, J.; Yang, X.; Zhang, Y.; Fan, C.; Li, D.; Deng, Y. HDL-scavenger receptor B type 1 facilitates SARS-CoV-2 entry. Nat. Metab. 2020, 2, 1391–1400. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, A.; van de Peppel, I.P.; Bodewes, F.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J. Abnormal liver function tests in patients with COVID-19: Relevance and potential pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lei, J.; Li, Z.; Yan, L. Potential effects of coronaviruses on the liver: An update. Front. Med. 2021, 8, 651658. [Google Scholar] [CrossRef] [PubMed]
- Akhmerov, A.; Marbán, E. COVID-19 and the heart. Circ. Res. 2020, 126, 1443–1455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Ding, X.; Xie, M.; Tian, D.; Xia, L. COVID-19-associated liver injury: From bedside to bench. J. Gastroenterol. 2021, 56, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Shih, A.R.; Misdraji, J. COVID-19: Gastrointestinal and Hepatobiliary Manifestations. Hum. Pathol. 2022, in press. [Google Scholar] [CrossRef]
- Dar, W.A.; Sullivan, E.; Bynon, J.S.; Eltzschig, H.; Ju, C. Ischaemia reperfusion injury in liver transplantation: Cellular and molecular mechanisms. Liver Int. 2019, 39, 788–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhai, Y.; Petrowsky, H.; Hong, J.C.; Busuttil, R.W.; Kupiec-Weglinski, J.W. Ischaemia–reperfusion injury in liver transplantation—From bench to bedside. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 79–89. [Google Scholar] [CrossRef]
- Block, H.; Rossaint, J.; Zarbock, A. The fatal circle of NETs and NET-associated DAMPs contributing to organ dysfunction. Cell 2022, 11, 1919. [Google Scholar] [CrossRef]
- Taneva, G.; Dimitrov, D.; Velikova, T. Liver dysfunction as a cytokine storm manifestation and prognostic factor for severe COVID-19. World J. Hepatol. 2021, 13, 2005–2012. [Google Scholar] [CrossRef]
- Zhan, K.; Liao, S.; Li, J.; Bai, Y.; Lv, L.; Yu, K.; Qiu, L.; Li, C.; Yuan, G.; Zhang, A. Risk factors in patients with COVID-19 developing severe liver injury during hospitalisation. Gut 2021, 70, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Arras, D.; Rose-John, S. IL-6 pathway in the liver: From physiopathology to therapy. J. Hepatol. 2016, 64, 1403–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishimoto, T. Interleukin-6: From basic science to medicine-40 years in immunology. Annu. Rev. Immunol. 2005, 23, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, C.A.; Jones, S.A. IL-6 as a keystone cytokine in health and disease. Nat. Immunol. 2015, 16, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Leng, L.; Cao, R.; Ma, J.; Mou, D.; Zhu, Y.; Li, W.; Lv, L.; Gao, D.; Zhang, S.; Gong, F. Pathological features of COVID-19-associated lung injury: A preliminary proteomics report based on clinical samples. Signal Transduct. Target Ther. 2020, 5, 240. [Google Scholar] [CrossRef]
- Lax, S.F.; Skok, K.; Zechner, P.; Kessler, H.H.; Kaufmann, N.; Koelblinger, C.; Vander, K.; Bargfrieder, U.; Trauner, M. Pulmonary arterial thrombosis in COVID-19 with fatal outcome: Results from a prospective, single-center, clinicopathologic case series. Ann. Intern. Med. 2020, 173, 350–361. [Google Scholar] [CrossRef]
- Ferron, P.-J.; Gicquel, T.; Mégarbane, B.; Clément, B.; Fromenty, B. Treatments in Covid-19 patients with preexisting metabolic dysfunction-associated fatty liver disease: A potential threat for drug-induced liver injury? Biochimie 2020, 179, 266–274. [Google Scholar] [CrossRef]
- Ooi, E.E.; Dhar, A.; Petruschke, R.; Locht, C.; Buchy, P.; Low, J.G.H. Use of analgesics/antipyretics in the management of symptoms associated with COVID-19 vaccination. NPJ Vaccines 2022, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.A.; Vuppalanchi, R.; Fontana, R.J.; Stolz, A.; Kleiner, D.E.; Hayashi, P.H.; Gu, J.; Hoofnagle, J.H.; Chalasani, N. Clinical and histologic features of azithromycin-induced liver injury. Clin. Gastroenterol. Hepatol. 2015, 13, 369–376.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhović, D.; Bojović, J.; Bulatović, A.; Vukčević, B.; Ratković, M.; Lazović, R.; Smolović, B. First case of drug-induced liver injury associated with the use of tocilizumab in a patient with COVID-19. Liver Int. 2020, 40, 1901–1905. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.L.-H.; Wong, V.W.-S.; Yuen, B.W.-Y.; Tse, Y.-K.; Yip, T.C.-F.; Luk, H.W.-S.; Lui, G.C.-Y.; Chan, H.L.-Y. Risk of hepatitis B surface antigen seroreversion after corticosteroid treatment in patients with previous hepatitis B virus exposure. J. Hepatol. 2020, 72, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Andini, R.; Bertolino, L.; Mele, F.; Florio, L.L.; Murino, P.; Corcione, A.; Zampino, R. Early experience with remdesivir in SARS-CoV-2 pneumonia. Infection 2020, 48, 779–782. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, G.; Meschiari, M.; Cozzi-Lepri, A.; Milic, J.; Tonelli, R.; Menozzi, M.; Franceschini, E.; Cuomo, G.; Orlando, G.; Borghi, V. Tocilizumab in patients with severe COVID-19: A retrospective cohort study. Lancet Rheumatol. 2020, 2, e474–e484. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, S.; Suzuki, T.; Sayama, M.; Nakada, T.-a.; Igari, H.; Ishii, I. Suspected cholestatic liver injury induced by favipiravir in a patient with COVID-19. J. Infect. Chemother. 2021, 27, 390–392. [Google Scholar] [CrossRef]
- Dubert, M.; Visseaux, B.; Isernia, V.; Bouadma, L.; Deconinck, L.; Patrier, J.; Wicky, P.-H.; Le Pluart, D.; Kramer, L.; Rioux, C. Case report study of the first five COVID-19 patients treated with remdesivir in France. Int. J. Infect. Dis. 2020, 98, 290–293. [Google Scholar] [CrossRef]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J. Role of oxidative stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) infection: A review. Protein J. 2020, 39, 644–656. [Google Scholar] [CrossRef]
- Ahmed, M.; Ahmed, M.H. Nonalcoholic fatty liver disease and COVID-19: An epidemic that begets pandemic. World J. Clin. Cases 2021, 9, 133–4142. [Google Scholar] [CrossRef]
- Ramanathan, R.; Ali, A.H.; Ibdah, J.A. Mitochondrial Dysfunction Plays Central Role in Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2022, 23, 7280. [Google Scholar] [CrossRef]
- Tarantino, G.; Citro, V.; Balsano, C.; Capone, D. Could SCGF-beta levels be associated with inflammation markers and insulin resistance in male patients suffering from obesity-related NAFLD? Diagnostics 2020, 10, 395. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Pan, X.; Zhou, W.; Gu, X.; Shen, F.; Yang, B.; Hu, Z. Clinical epidemiological analyses of overweight/obesity and abnormal liver function contributing to prolonged hospitalization in patients infected with COVID-19. Int. J. Obes. 2020, 44, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.M.; Caplice, N.M. Is adipose tissue a reservoir for viral spread, immune activation, and cytokine amplification in coronavirus disease 2019? Obesity 2020, 28, 1191–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijnikman, A.S.; Bruin, S.; Groen, A.K.; Nieuwdorp, M.; Herrema, H. Increased expression of key SARS-CoV-2 entry points in multiple tissues in individuals with NAFLD. J. Hepatol. 2021, 74, 748–749. [Google Scholar] [CrossRef]
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Non-alcoholic fatty liver diseases in patients with COVID-19: A retrospective study. J. Hepatol. 2020, 73, 451–453. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.-A. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Mallet, V.; Beeker, N.; Bouam, S.; Sogni, P.; Pol, S.; Beeker, N.; Fontaine, H.; Corouge, M.; Pichard, A.V.; Hollande, C. Prognosis of French COVID-19 patients with chronic liver disease: A national retrospective cohort study for 2020. J. Hepatol. 2021, 75, 848–855. [Google Scholar] [CrossRef]
- Cho, S.I.; Yoon, S.; Lee, H.-J. Impact of comorbidity burden on mortality in patients with COVID-19 using the Korean health insurance database. Sci. Rep. 2021, 11, 6375. [Google Scholar] [CrossRef]
- Cargill, Z.; Kattiparambil, S.; Hansi, N.; Barnabas, A.; Shawcross, D.L.; Williams, R.; Agarwal, K. Severe alcohol-related liver disease admissions post-COVID-19 lockdown: Canary in the coal mine? Frontline Gastroenterol. 2021, 12, 354–355. [Google Scholar] [CrossRef]
- Choudhary, N.S.; Dhampalwar, S.; Saraf, N.; Soin, A.S. Outcomes of COVID-19 in patients with cirrhosis or liver transplantation. J. Clin. Exp. Hepatol. 2021, 11, 713–719. [Google Scholar] [CrossRef]
- Sabaka, P.; Koščálová, A.; Straka, I.; Hodosy, J.; Lipták, R.; Kmotorková, B.; Kachlíková, M.; Kušnírová, A. Role of interleukin 6 as a predictive factor for a severe course of Covid-19: Retrospective data analysis of patients from a long-term care facility during Covid-19 outbreak. BMC Infect. Dis. 2021, 21, 308. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.; Gilg, S.; Björnsson, B.; Hasselgren, K.; Ghorbani, P.; Sauter, C.; Stål, P.; Sandstöm, P.; Sparrelid, E.; Engstrand, J. Impact of post-hepatectomy liver failure on morbidity and short-and long-term survival after major hepatectomy. BJS Open 2022, 6, zrac097. [Google Scholar] [CrossRef] [PubMed]
- Seneviratne, S.L.; Wijerathne, W.; Yasawardene, P.; Somawardana, B. COVID-19 in cancer patients. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 767–797. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Ballester, M.P.; Soffientini, U.; Jalan, R.; Mehta, G. SARS-CoV-2 infection and liver involvement. Hepatol. Int. 2022, 16, 755–774. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Tevethia, H.V.; Premkumar, M.; Arab, J.P.; Candia, R.; Kumar, K.; Kumar, P.; Sharma, M.; Rao, P.N.; Reddy, D.N. Impact of COVID-19 on liver transplant recipients–A systematic review and meta-analysis. EClinicalMedicine 2021, 38, 101025. [Google Scholar] [CrossRef]
- Kullar, R.; Patel, A.P.; Saab, S. COVID-19 in liver transplant recipients. J. Clin. Transl. Hepatol. 2021, 9, 545–550. [Google Scholar] [CrossRef]
- Moon, A.M.; Webb, G.J.; García-Juárez, I.; Kulkarni, A.V.; Adali, G.; Wong, D.K.; Lusina, B.; Dalekos, G.N.; Masson, S.; Shore, B.M. SARS-CoV-2 infections among patients with liver disease and liver transplantation who received COVID-19 vaccination. Hepatol. Commun. 2022, 6, 889–897. [Google Scholar] [CrossRef]
- Sripongpun, P.; Pinpathomrat, N.; Bruminhent, J.; Kaewdech, A. Coronavirus Disease 2019 Vaccinations in Patients With Chronic Liver Disease and Liver Transplant Recipients: An Update. Front. Med. 2022, 9, 924454. [Google Scholar] [CrossRef]
- Sivandzadeh, G.R.; Askari, H.; Safarpour, A.R.; Ejtehadi, F.; Raeis-Abdollahi, E.; Lari, A.V.; Abazari, M.F.; Tarkesh, F.; Lankarani, K.B. COVID-19 infection and liver injury: Clinical features, biomarkers, potential mechanisms, treatment, and management challenges. World J. Clin. Cases 2021, 9, 6178–6200. [Google Scholar] [CrossRef]
- Guarino, M.; Cossiga, V.; Loperto, I.; Esposito, I.; Ortolani, R.; Fiorentino, A.; Pontillo, G.; De Coppi, L.; Cozza, V.; Galeota Lanza, A. COVID-19 in liver transplant recipients: Incidence, hospitalization and outcome in an Italian prospective double-centre study. Sci. Rep. 2022, 12, 4831. [Google Scholar] [CrossRef]
- Mahamid, M.; Nseir, W.; Khoury, T.; Mahamid, B.; Nubania, A.; Sub-Laban, K.; Schifter, J.; Mari, A.; Sbeit, W.; Goldin, E. Nonalcoholic fatty liver disease is associated with COVID-19 severity independently of metabolic syndrome: A retrospective case-control study. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1578–1581. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Fernandez, J.; Ochoa, J.; Ojeda, M.L.; Nogales, F.; Carreras, O.; Díaz-Castro, J. Inflammation and oxidative stress, the links between obesity and COVID-19: A narrative review. J. Physiol. Biochem. 2022, 78, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Cinque, F.; Cespiati, A.; Lombardi, R.; Costantino, A.; Maffi, G.; Alletto, F.; Colavolpe, L.; Francione, P.; Oberti, G.; Fatta, E. Interaction between Lifestyle Changes and PNPLA3 Genotype in NAFLD Patients during the COVID-19 Lockdown. Nutrient 2022, 14, 556. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Fan, J.; Ma, Q.; Han, L.; Cao, Z.; Xu, C.; Luan, J.; Jing, G.; Nan, Y.; Wu, T. A novel nanobody-heavy chain antibody against Angiopoietin-like protein 3 reduces plasma lipids and relieves nonalcoholic fatty liver disease. J. Nanobiotechnol. 2022, 20, 237. [Google Scholar] [CrossRef]
- Wong, G.L.-H.; Wong, V.W.-S.; Thompson, A.; Jia, J.; Hou, J.; Lesmana, C.R.A.; Susilo, A.; Tanaka, Y.; Chan, W.-K.; Gane, E. Management of patients with liver derangement during the COVID-19 pandemic: An Asia-Pacific position statement. Lancet Gastroenterol. Hepatol. 2020, 5, 776–787. [Google Scholar] [CrossRef]
- Lampertico, P. Oral antiviral therapy for HBeAg negative chronic hepatitis B: Better stop or continue? Gut 2015, 64, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Mandel, E.; Peci, A.; Cronin, K.; Capraru, C.I.; Shah, H.; Janssen, H.L.; Tran, V.; Biondi, M.J.; Feld, J.J. The impact of the first, second and third waves of covid-19 on hepatitis B and C testing in Ontario, Canada. J. Viral. Hepat. 2022, 29, 205–208. [Google Scholar] [CrossRef]
- Abdollahi, A.; Salarvand, S.; Mehrtash, V.; Jafarzadeh, B.; Ghalehtaki, R.; Nateghi, S. Is There A Correlation Between COVID-19 and Hepatitis A and Hepatitis E Serum Antibody Level? Iran J. Pathol. 2022, 17, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Sun, Y.-s.; An, R.; Liu, F.; Fang, Q.; Wang, Z.; Xu, T.; Chen, L.; Du, J. Application and progress of the detection technologies in hepatocellular carcinoma. Genes Dis. 2022, in press. [Google Scholar] [CrossRef]
- Amaddeo, G.; Brustia, R.; Allaire, M.; Lequoy, M.; Hollande, C.; Regnault, H.; Blaise, L.; Ganne-Carrié, N.; Séror, O.; Larrey, E. Impact of COVID-19 on the management of hepatocellular carcinoma in a high-prevalence area. JHEP Rep. 2021, 3, 100199. [Google Scholar] [CrossRef]
- Lee, S.-W.; Yang, S.-S.; Lien, H.-C.; Peng, Y.-C.; Tung, C.-F.; Lee, T.-Y. The Combining of Tyrosine Kinase Inhibitors and Immune Checkpoint Inhibitors as First-Line Treatment for Advanced Stage Hepatocellular Carcinoma. J. Clin. Med. 2022, 11, 4874. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.; Cossiga, V.; Capasso, M.; Mazzarelli, C.; Pelizzaro, F.; Sacco, R.; Russo, F.P.; Vitale, A.; Trevisani, F.; Cabibbo, G. Impact of SARS-CoV-2 Pandemic on the Management of Patients with Hepatocellular Carcinoma. J. Clin. Med. 2022, 11, 4475. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Du, Q.; Yan, S.; Guo, X.-G.; He, Y.; Zhu, G.; Zhao, K.; Ouyang, S. Liver injury in COVID-19: Clinical features and treatment management. Virol. J. 2021, 18, 121. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.; Hosri, J.; Bteich, Y.; Dib, A.; Abou Rached, A. COVID-19 and Liver Dysfunction. Cureus 2022, 14, e21302. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Arora, A. Clinical presentation of alcoholic liver disease and non-alcoholic fatty liver disease: Spectrum and diagnosis. Transl. Gastroenterol. Hepatol. 2020, 5, 19. [Google Scholar] [CrossRef]
- Russo, F.P.; Burra, P.; Zanetto, A. COVID-19 and liver disease: Where are we now? Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 277–278. [Google Scholar] [CrossRef]
- Siddiqui, M.A.; Suresh, S.; Simmer, S.; Abu-Ghanimeh, M.; Karrick, M.; Nimri, F.; Musleh, M.; Mediratta, V.; Al-Shammari, M.; Russell, S. Increased morbidity and mortality in COVID-19 patients with liver injury. Dig. Dis. Sci. 2022, 67, 2577–2583. [Google Scholar] [CrossRef]
- Yip, T.C.-F.; Gill, M.; Wong, G.L.-H.; Liu, K. Management of hepatitis B virus reactivation due to treatment of COVID-19. Hepatol. Int. 2022, 16, 257–268. [Google Scholar] [CrossRef]
- Piedade, J.; Pereira, G. COVID-19 in liver transplant recipients. J. Liver Transpl. 2021, 3, 100026. [Google Scholar] [CrossRef]
- Gabarre, P.; Loens, C.; Tamzali, Y.; Barrou, B.; Jaisser, F.; Tourret, J. Immunosuppressive therapy after solid organ transplantation and the gut microbiota: Bidirectional interactions with clinical consequences. Am. J. Transplant. 2022, 22, 1014–1030. [Google Scholar] [CrossRef]
- Susomboon, T.; Kunlamas, Y.; Vadcharavivad, S.; Vongwiwatana, A. The effect of the very low dosage diltiazem on tacrolimus exposure very early after kidney transplantation: A randomized controlled trial. Sci. Rep. 2022, 12, 14247. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Type | Enrolled Patients | Medication Type | Dose Concentration (mg) | Duration | Drug-Induced Liver Injury | Outcomes | References |
|---|---|---|---|---|---|---|---|
| Case Study | 4 | Remdesivir, Hydroxychloroquine | 10 | Daily | Elevated AST and ALT (5–8 times) | Liver cirrhosis, cardiac failure, and organ dysfunction | [44] |
| Randomized design | 158 | Lopinavir, Remdesivir, Corticosteroids | 100 | Daily | AST/ALT (5 times folds) | Adverse effects (Liver dysfunction and circulatory failure) were observed in 102 patients | [45] |
| Case Study | One patient susceptible to medication | Chloroquine, Methylprednisolone, Tocilizumab | 500 | Daily | Transaminase elevated (10 times folds) | Autoimmune liver disease, cytokine release syndrome | [42] |
| Cross-sectional | 417 | Ribavirin, Ritonavir | Undetected thought the study | Throughout treatment | AST/ALT (3 times folds) | Hepatocellular carcinoma, NAFLD | [4] |
| Retrospective | 179 | Tocilizumab | 800 | 24 h | Transaminase sharply after dosage | Liver cirrhosis | [46] |
| Case Study | One patient susceptible to study | Favipiravir | 6000 | Daily | Transaminase was significantly elevated | Cholestasis liver disease | [47] |
| Case Study | 5 | Remdesivir | 200 | Daily | ALT was significantly elevated | Advanced liver disease and renal failure | [48] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naeem, M.; Bano, N.; Manzoor, S.; Ahmad, A.; Munawar, N.; Razak, S.I.A.; Lee, T.Y.; Devaraj, S.; Hazafa, A. Pathogenetic Mechanisms of Liver-Associated Injuries, Management, and Current Challenges in COVID-19 Patients. Biomolecules 2023, 13, 99. https://doi.org/10.3390/biom13010099
Naeem M, Bano N, Manzoor S, Ahmad A, Munawar N, Razak SIA, Lee TY, Devaraj S, Hazafa A. Pathogenetic Mechanisms of Liver-Associated Injuries, Management, and Current Challenges in COVID-19 Patients. Biomolecules. 2023; 13(1):99. https://doi.org/10.3390/biom13010099
Chicago/Turabian StyleNaeem, Muhammad, Naheed Bano, Saba Manzoor, Aftab Ahmad, Nayla Munawar, Saiful Izwan Abd Razak, Tze Yan Lee, Sutha Devaraj, and Abu Hazafa. 2023. "Pathogenetic Mechanisms of Liver-Associated Injuries, Management, and Current Challenges in COVID-19 Patients" Biomolecules 13, no. 1: 99. https://doi.org/10.3390/biom13010099
APA StyleNaeem, M., Bano, N., Manzoor, S., Ahmad, A., Munawar, N., Razak, S. I. A., Lee, T. Y., Devaraj, S., & Hazafa, A. (2023). Pathogenetic Mechanisms of Liver-Associated Injuries, Management, and Current Challenges in COVID-19 Patients. Biomolecules, 13(1), 99. https://doi.org/10.3390/biom13010099