
The Main Therapeutic Applications of Cannabidiol (CBD) and Its Potential Effects on Aging with Respect to Alzheimer’s Disease


{kind=link}
{kind=link}
Abstract
:1. Introduction
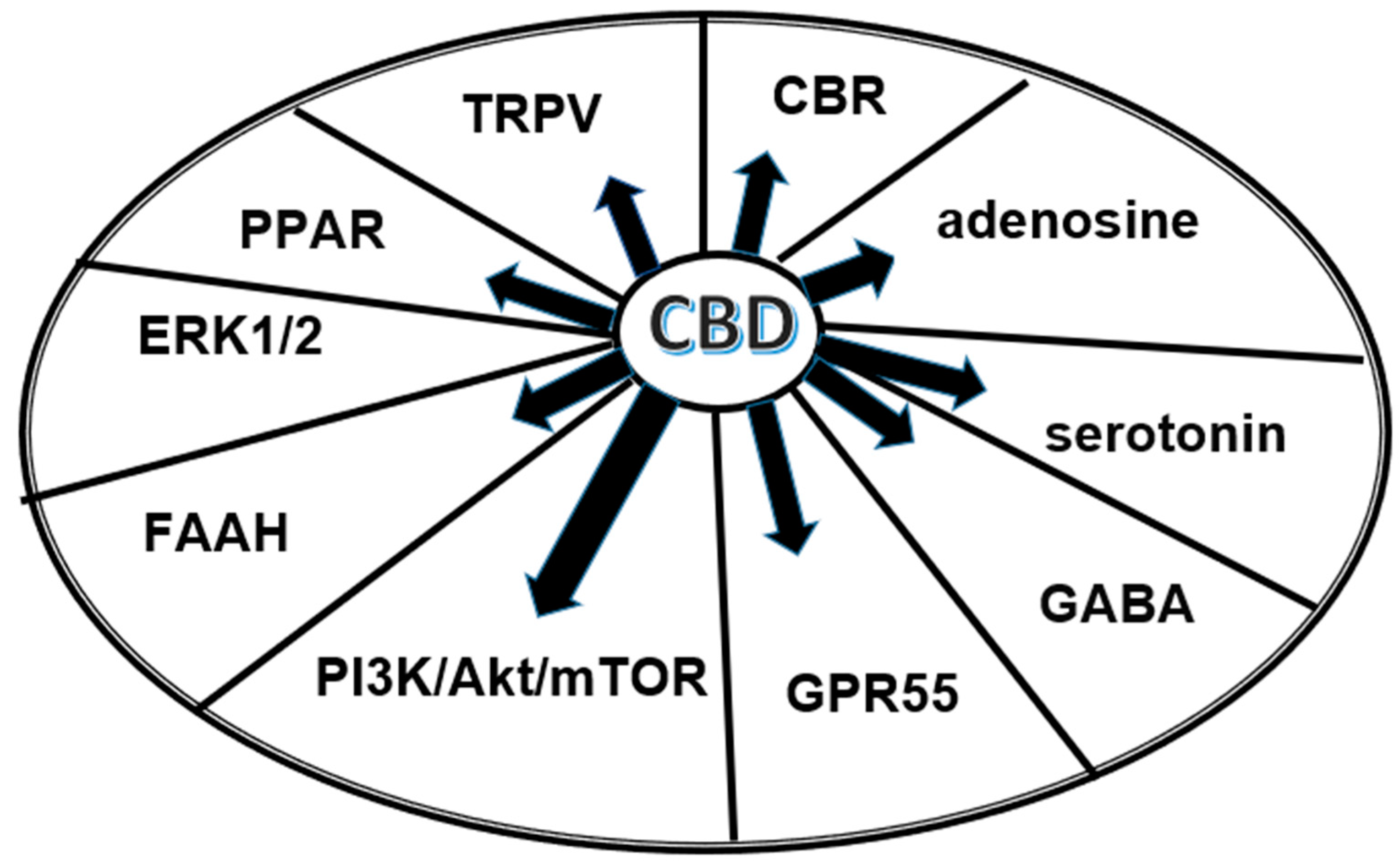
2. Cannabinoids and the Endocannabinoidome
3. Pharmacokinetics and Pharmacodynamics of Cannabinoids
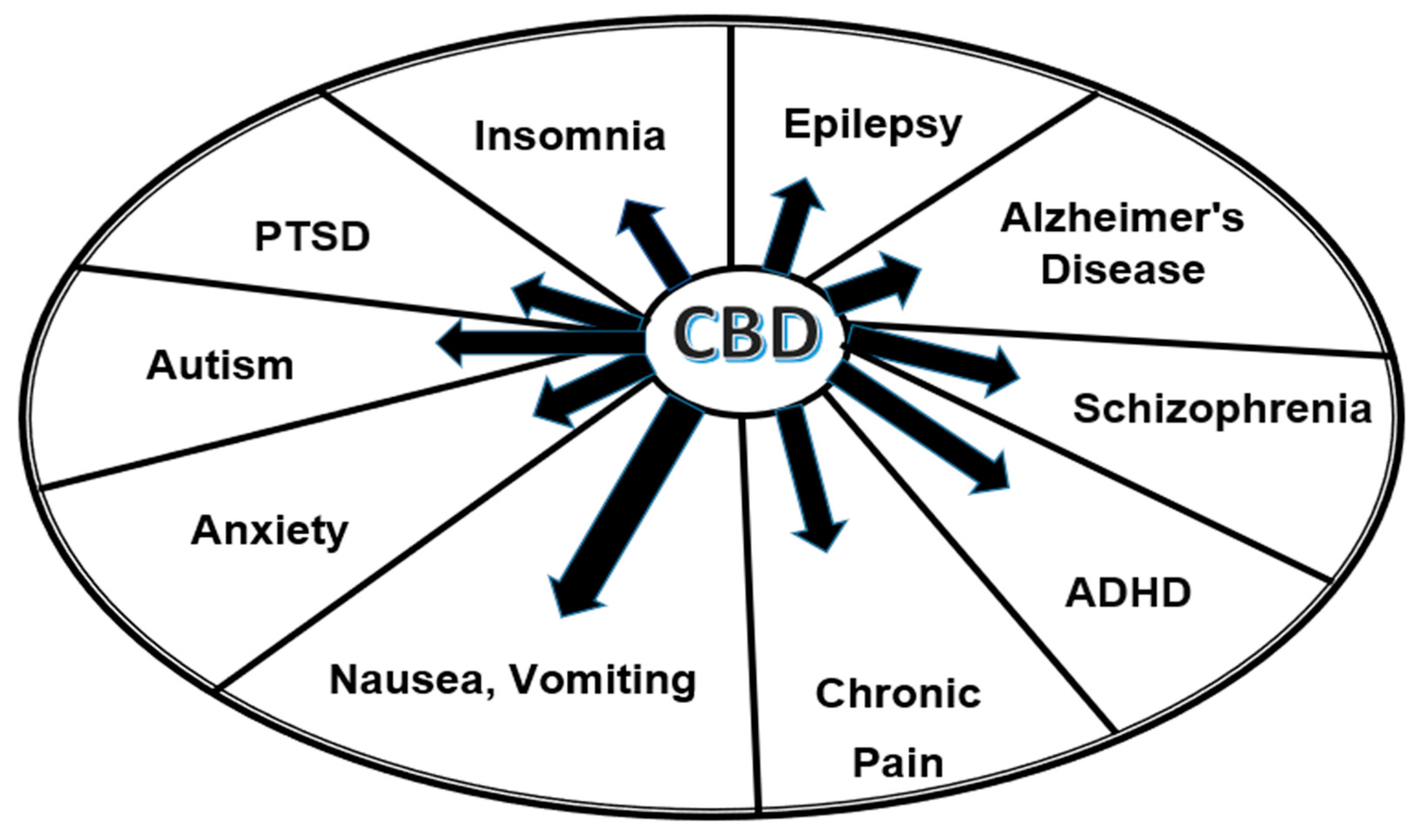
4. Examples of Therapeutical Effects of CBD in Clinical Practice
5. Effects of CBD on Aging Including Alzheimer’s Disease
6. Adverse Effects of CBD and Limitations of Its Use
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kirkwood, T.B.L. Understanding the Odd Science of Aging. Cell 2005, 120, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V.; Wang, J. (Eds.) The Endocannabinoidome: The World of Endocannabinoids and Related Mediators, 1st ed.; Academic Press: Cambridge, MA, USA, 2014. [Google Scholar]
- Piomelli, D. The molecular logic of endocannabinoid signalling. Nat. Rev. Neurosci. 2003, 4, 873–884. [Google Scholar] [CrossRef]
- Di Marzo, V.; Piscitelli, F. The Endocannabinoid System and its Modulation by Phytocannabinoids. Neurotherapeutics 2015, 12, 692–698. [Google Scholar] [CrossRef]
- Pertwee, R.G. Pharmacological actions of cannabinoids. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2005; Volume 168, pp. 1–51. [Google Scholar] [CrossRef]
- Paradisi, A.; Oddi, S.; Maccarrone, M. The Endocannabinoid System in Ageing: A New Target for Drug Development. Curr. Drug Targets 2006, 7, 1539–1552. [Google Scholar] [CrossRef]
- Micale, V.; Di Marzo, V.; Sulcova, A.; Wotjak, C.T.; Drago, F. Endocannabinoid system and mood disorders: Priming a target for new therapies. Pharmacol. Ther. 2013, 138, 18–37. [Google Scholar]
- Beedham, W.; Sbai, M.; Allison, I.; Coary, R.; Shipway, D. Cannabinoids in the Older Person: A Literature Review. Geriatrics 2020, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Bryk, M.; Starowicz, K. Cannabinoid-based therapy as a future for joint degeneration. Focus on the role of CB2 receptor in the arthritis progression and pain: An updated review. Pharmacol. Rep. 2021, 73, 681–699. [Google Scholar] [CrossRef] [PubMed]
- Mangieri, R.A.; Piomelli, D. Enhancement of endocannabinoid signaling and the pharmacotherapy of depression. Pharmacol. Res. 2007, 56, 360–366. [Google Scholar] [CrossRef]
- Paredes-Ruiz, K.J.; Chavira-Ramos, K.; Orozco-Morales, M.; Karasu, C.; Tinkov, A.A.; Aschner, M.; Santamaría, A.; Colín-González, A.L. On the Biomedical Properties of Endocannabinoid Degradation and Reuptake Inhibitors: Pre-clinical and Clinical Evidence. Neurotox. Res. 2021, 39, 2072–2097. [Google Scholar] [CrossRef]
- Landa, L.; Jurica, J.; Sliva, J.; Pechackova, M.; Demlova, R. Medical cannabis in the treatment of cancer pain and spastic conditions and options of drug delivery in clinical practice. Biomed. Pap. 2018, 162, 18–25. [Google Scholar] [CrossRef]
- Trojan, V.; Landa, L.; Hrib, R.; Jurica, J.; Rychlickova, J.; Zvonicek, V.; Halamkova, L.; Halamek, J.; Demlova, R.; Belaskova, S.; et al. Assessment of Delta-9-Tetrahydrocannabinol (THC) in Saliva and Blood After Oral Administration of Medical Cannabis With Respect to its Effect on Driving Abilities. Physiol. Res. 2022, 71, 703–712. [Google Scholar] [CrossRef]
- Fisar, Z. Phytocannabinoids and endocannabinoids. Curr. Drug Abus. Rev. 2009, 2, 51–75. [Google Scholar] [CrossRef]
- Zendulka, O.; Dovrtělová, G.; Nosková, K.; Turjap, M.; Šulcová, A.; Hanuš, L.; Juřica, J. Cannabinoids and Cytochrome P450 Interactions. Curr. Drug Metab. 2016, 17, 206–226. [Google Scholar] [CrossRef] [PubMed]
- Mackie, K. Cannabinoid Receptors as Therapeutic Targets. Annu. Rev. Pharmacol. Toxicol. 2006, 46, 101–122. [Google Scholar] [CrossRef] [PubMed]
- Izzo, A.A.; Borrelli, F.; Capasso, R.; Di Marzo, V.; Mechoulam, R. Non-psychotropic plant cannabinoids: New therapeutic opportunities from an ancient herb. Trends Pharmacol. Sci. 2009, 30, 515–527, Erratum in: Trends Pharmacol. Sci. 2009, 30, 609. [Google Scholar] [CrossRef] [PubMed]
- Battista, N.; Di Tommaso, M.; Bari, M.; Maccarrone, M. The endocannabinoid system: An overview. Front. Behav. Neurosci. 2012, 6, 9. [Google Scholar] [CrossRef]
- Bilkei-Gorzo, A. The endocannabinoid system in normal and pathological brain ageing. Philos. Trans. R. Soc. B Biol. Sci. 2012, 367, 3326–3341. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Di Nisio, M.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015, 313, 2456–2473, Erratum in: JAMA 2015, 314, 520. Erratum in: JAMA 2015, 314, 837. Erratum in: JAMA 2015, 314, 2308. Erratum in: JAMA 2016, 315, 1522. [Google Scholar] [CrossRef] [PubMed]
- Sulcova, A. Pharmacodynamics of cannabinoids. Arch. Pharm. Pharm. Sci. 2019, 3, 1118. [Google Scholar] [CrossRef]
- Hodges, E.L.; Ashpole, N.M. Aging circadian rhythms and cannabinoids. Neurobiol. Aging 2019, 79, 110–118. [Google Scholar] [CrossRef]
- Komorowska-Müller, J.A.; Rana, T.; Olabiyi, B.F.; Zimmer, A.; Schmöle, A.-C. Cannabinoid Receptor 2 Alters Social Memory and Microglial Activity in an Age-Dependent Manner. Molecules 2021, 26, 5984. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, G.; Magnavacca, A.; Fumagalli, M.; Dell’agli, M.; Piazza, S.; Sangiovanni, E. Cannabis sativa and Skin Health: Dissecting the Role of Phytocannabinoids. Planta Medica 2021, 88, 492–506. [Google Scholar] [CrossRef]
- Ortega-Gutierrez, S. Therapeutic perspectives of inhibitors of endocannabinoid degradation. Curr. Drug Target CNS Neurol. Disord. 2005, 4, 697–707. [Google Scholar] [CrossRef]
- de Lago, E.; Fernández-Ruiz, J.; Ortega-Gutiérrez, S.; Cabranes, A.; Pryce, G.; Baker, D.; López-Rodríguez, M.; Ramos, J.A. UCM707, an inhibitor of the anandamide uptake, behaves as a symptom control agent in models of Huntington’s disease and multiple sclerosis, but fails to delay/arrest the progression of different motor-related disorders. Eur. Neuropsychopharmacol. 2006, 16, 7–18. [Google Scholar] [CrossRef] [PubMed]
- de Lago, E.; Ortega-Gutiérrez, S.; Ramos, J.A.; Rodríguez, M.L.L.; Fernández-Ruiz, J. Neurochemical effects of the endocannabinoid uptake inhibitor UCM707 in various rat brain regions. Life Sci. 2007, 80, 979–988. [Google Scholar] [CrossRef]
- Piomelli, D.; Tagne, A.M. Endocannabinoid-Based Therapies. Annu. Rev. Pharmacol. Toxicol. 2022, 62, 483–507. [Google Scholar] [CrossRef]
- Abrams, D.I. The therapeutic effects of Cannabis and cannabinoids: An update from the National Academies of Sciences, Engineering and Medicine report. Eur. J. Intern. Med. 2018, 49, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Benito, C.; Núñez, E.; Pazos, M.R.; Tolón, R.M.; Romero, J. The Endocannabinoid System and Alzheimer’s Disease. Mol. Neurobiol. 2007, 36, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Maccarrone, M.; Gasperi, V.; Catani, M.V.; Diep, T.A.; Dainese, E.; Hansen, H.S.; Avigliano, L. The Endocannabinoid System and Its Relevance for Nutrition. Annu. Rev. Nutr. 2010, 30, 423–440. [Google Scholar] [CrossRef] [PubMed]
- Dos Reis Rosa Franco, G.; Smid, S.; Viegas, C. Phytocannabinoids: General Aspects and Pharmacological Potential in Neurodegenerative Diseases. Curr. Neuropharmacol. 2021, 19, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://apps.who.int/iris/bitstream/handle/10665/279948/9789241210225-eng.pdf (accessed on 25 April 2023).
- Crippa, J.A.; Guimarães, F.S.; Campos, A.C.; Zuardi, A.W. Translational Investigation of the Therapeutic Potential of Cannabidiol (CBD): Toward a New Age. Front. Immunol. 2018, 9, 2009. [Google Scholar] [CrossRef] [PubMed]
- Batalla, A.; Janssen, H.; Gangadin, S.S.; Bossong, M.G. The Potential of Cannabidiol as a Treatment for Psychosis and Addiction: Who Benefits Most? A Systematic Review. J. Clin. Med. 2019, 8, 1058. [Google Scholar] [CrossRef] [PubMed]
- Abuhasira, R.; Schleider, L.B.-L.; Mechoulam, R.; Novack, V. Epidemiological characteristics, safety and efficacy of medical cannabis in the elderly. Eur. J. Intern. Med. 2018, 49, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Abuhasira, R.; Ron, A.; Sikorin, I.; Novack, V. Medical Cannabis for Older Patients—Treatment Protocol and Initial Results. J. Clin. Med. 2019, 8, 1819. [Google Scholar] [CrossRef] [PubMed]
- Solomon, H.V.; Greenstein, A.P.; DeLisi, L.E. Cannabis Use in Older Adults: A Perspective. Harv. Rev. Psychiatry 2021, 29, 225–233. [Google Scholar] [CrossRef]
- Morel, A.; Lebard, P.; Dereux, A.; Azuar, J.; Questel, F.; Bellivier, F.; Marie-Claire, C.; Fatséas, M.; Vorspan, F.; Bloch, V. Clinical Trials of Cannabidiol for Substance Use Disorders: Outcome Measures, Surrogate Endpoints, and Biomarkers. Front. Psychiatry 2021, 12565617. [Google Scholar] [CrossRef]
- Sulcova, A. Translational research on the effects of treatment with cannabidiol in addictions. Adiktologie 2021, 21, 161–165. [Google Scholar] [CrossRef]
- Taylor, L.; Crockett, J.; Tayo, B.; Checketts, D.; Sommerville, K. Abrupt withdrawal of cannabidiol (CBD): A randomized trial. Epilepsy Behav. 2020, 104, 106938. [Google Scholar] [CrossRef] [PubMed]
- Wall, M.E.; Brine, D.R.; Perez-Reyes, M. The Pharmacology of Marihuana; Braude, M.C., Szara, S., Eds.; Raven Press: New York, NY, USA, 1976; p. 93. [Google Scholar]
- Agurell, S.; Carlsson, S.; Lindgren, J.E.; Ohlsson, A.; Gillespie, H.; Hollister, L. Interactions of delta 1-tetrahydrocannabinol with cannabinol and cannabidiol following oral administration in man: Assay of cannabinol and cannabidiol by mass fragmentography. Experientia 1981, 37, 1090–1092. [Google Scholar] [CrossRef]
- Huestis, M.A. Human Cannabinoid Pharmacokinetics. Chem. Biodivers 2007, 4, 1770–1804. [Google Scholar] [CrossRef]
- Lucas, C.J.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [PubMed]
- Millar, S.A.; Stone, N.L.; Yates, A.S.; O’Sullivan, S.E. A Systematic Review on the Pharmacokinetics of Cannabidiol in Humans. Front. Pharmacol. 2018, 9, 1365. [Google Scholar] [CrossRef] [PubMed]
- Ohlsson, A.; Lindgren, J.-E.; Andersson, S.; Agurell, S.; Gillespie, H.; Hollister, L.E. Single-dose kinetics of deuterium-labelled cannabidiol in man after smoking and intravenous administration. J. Mass Spectrom. 1986, 13, 77–83. [Google Scholar] [CrossRef]
- Gaston, T.E.; Friedman, D. Pharmacology of cannabinoids in the treatment of epilepsy. Epilepsy Behav. 2017, 70, 313–318. [Google Scholar] [CrossRef]
- Consroe, P.; Laguna, J.; Allender, J.; Snider, S.; Stern, L.; Sandyk, R.; Kennedy, K.; Schram, K. Controlled clinical trial of cannabidiol in Huntington’s disease. Pharmacol. Biochem. Behav. 1991, 40, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Mielnik, C.A.; Lam, V.M.; Ross, R.A. CB1 allosteric modulators and their therapeutic potential in CNS disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 106, 110163. [Google Scholar] [CrossRef]
- Peng, J.; Fan, M.; An, C.; Ni, F.; Huang, W.; Luo, J. A narrative review of molecular mechanism and therapeutic effect of cannabidiol (CBD). Basic Clin. Pharmacol. Toxicol. 2022, 130, 439–456. [Google Scholar] [CrossRef]
- Laun, A.S.; Shrader, S.H.; Brown, K.J.; Song, Z.H. GPR3. GPR6, and GPR12 as novel molecular targets: Their biological functions and interaction with cannabidiol. Acta Pharmacol. Sin. 2019, 40, 300–308. [Google Scholar] [CrossRef]
- Mlost, J.; Bryk, M.; Starowicz, K. Cannabidiol for Pain Treatment: Focus on Pharmacology and Mechanism of Action. Int. J. Mol. Sci. 2020, 21, 8870. [Google Scholar] [CrossRef]
- Laprairie, R.B.; Bagher, A.M.; Kelly, M.E.; Denovan-Wright, E.M. Cannabidiol is a negative allosteric modulator of the cannabinoid CB1 receptor. Br. J. Pharmacol. 2015, 172, 4790–4805. [Google Scholar] [CrossRef]
- Morales, P.; Hurst, D.P.; Reggio, P.H. Molecular targets of the phytocannabinoids: A complex picture. Prog. Chem. Org. Nat. Prod. 2017, 103, 103–131. [Google Scholar] [CrossRef]
- Preedy, V.R. Handbook of Cannabis and Related Pathologies: Biology, Pharmacology, Diagnosis, and Treatment; Academic Press: Amsterdam, The Netherlands, 2017; 1143p. [Google Scholar]
- Ghovanloo, M.R.; Shuart, N.G.; Mezeyova, J.; Dean, R.A.; Ruben, P.C.; Goodchild, S.J. Inhibitory effects of cannabidiol on voltage-dependent sodium currents. J. Biol. Chem. 2018, 293, 16546–16558. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, M.; Onetti, Y.; Cortés-Montero, E.; Garzón, J.; Sánchez-Blázquez, P. Cannabidiol enhances morphine antinociception, diminishes NMDA-mediated seizures and reduces stroke damage via the sigma 1 receptor. Mol. Brain 2018, 11, 51. [Google Scholar] [CrossRef]
- Ma, H.; Xu, F.; Liu, C.; Seeram, N.P. A Network Pharmacology Approach to Identify Potential Molecular Targets for Cannabidiol’s Anti-Inflammatory Activity. Cannabis Cannabinoid Res. 2021, 6, 288–299. [Google Scholar] [CrossRef]
- Iffland, K.; Grotenhermen, F.; Reddon, H.; DeBeck, K.; Socias, M.-E.; Lake, S.; Dong, H.; Hayashi, K.; Milloy, M.-J.; Wright, M.; et al. An Update on Safety and Side Effects of Cannabidiol: A Review of Clinical Data and Relevant Animal Studies. Cannabis Cannabinoid Res. 2017, 2, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Cross, J.H.; Laux, L.; Marsh, E.; Miller, I.; Nabbout, R.; Scheffer, I.E.; Thiele, E.A.; Wright, S.; Cannabidiol in Dravet Syndrome Study Group. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N. Engl. J. Med. 2017, 376, 2011–2020. [Google Scholar] [CrossRef] [PubMed]
- Maa, E.; Figi, P. The case for medical marijuana in epilepsy. Epilepsia 2014, 55, 783–786. [Google Scholar] [CrossRef]
- Raucci, U.; Pietrafusa, N.; Paolino, M.C.; Di Nardo, G.; Villa, M.P.; Pavone, P.; Terrin, G.; Specchio, N.; Striano, P.; Parisi, P. Cannabidiol Treatment for Refractory Epilepsies in Pediatrics. Front. Pharmacol. 2020, 11, 586110. [Google Scholar] [CrossRef] [PubMed]
- Fong, S.L.; Kossoff, E.H. Cannabinoids as future treatment for epilepsy. Contemp. PEDS J. 2018, 35, 11–12. [Google Scholar]
- Pietrafusa, N.; Ferretti, A.; Trivisano, M.; de Palma, L.; Calabrese, C.; Pavia, G.C.; Tondo, I.; Cappelletti, S.; Vigevano, F.; Specchio, N. Purified Cannabidiol for Treatment of Refractory Epilepsies in Pediatric Patients with Developmental and Epileptic Encephalopathy. Pediatr. Drugs 2019, 21, 283–290. [Google Scholar] [CrossRef]
- Boyaji, S.; Merkow, J.; Elman, R.N.M.; Kaye, A.D.; Yong, R.J.; Urman, R.D. The Role of Cannabidiol (CBD) in Chronic Pain Management: An Assessment of Current Evidence. Curr. Pain Headache Rep. 2020, 24, 4. [Google Scholar] [CrossRef]
- Eskander, J.P.; Spall, J.; Spall, A.; Shah, R.V.; Kaye, A.D. Cannabidiol (CBD) as a treatment of acute and chronic back pain: A case series and literature review. J. Opioid Manag. 2020, 16, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.H.; Cullen, B.D.; Tang, M.; Fang, Y. The Effectiveness of Topical Cannabidiol Oil in Symptomatic Relief of Peripheral Neuropathy of the Lower Extremities. Curr. Pharm. Biotechnol. 2020, 21, 390–402. [Google Scholar] [CrossRef] [PubMed]
- Schneider, T.M.; Zurbriggen, L.; Dieterle, M.; Mauermann, E.M.; Frei, P.; Mercer-Chalmers-Bender, K.; Ruppen, W.M. Pain response to cannabidiol in induced acute nociceptive pain, allodynia, and hyperalgesia by using a model mimicking acute pain in healthy adults in a randomized trial (CANAB I). Pain 2022, 163, e62–e71. [Google Scholar] [CrossRef]
- Villanueva, M.R.B.; Joshaghani, N.; Villa, N.; Badla, O.; Goit, R.; Saddik, S.E.; Dawood, S.N.; Rabih, A.M.; Niaj, A.; Raman, A.; et al. Efficacy, Safety, and Regulation of Cannabidiol on Chronic Pain: A Systematic Review. Cureus 2022, 14, e26913. [Google Scholar] [CrossRef]
- Blake, A.; Wan, B.A.; Malek, L.; DeAngelis, C.; Diaz, P.; Lao, N.; Chow, E.; O’hearn, S. A selective review of medical cannabis in cancer pain management. Ann. Palliat. Med. 2017, 6, S215–S222. [Google Scholar] [CrossRef]
- Corroon, J.; Phillips, J.A. A Cross-Sectional Study of Cannabidiol Users. Cannabis Cannabinoid Res. 2018, 3, 152–161. [Google Scholar] [CrossRef]
- Laczkovics, C.; Kothgassner, O.D.; Felnhofer, A.; Klier, C.M. Cannabidiol treatment in an adolescent with multiple substance abuse, social anxiety and depression. Neuropsychiatrie 2020, 35, 31–34. [Google Scholar] [CrossRef]
- Berger, M.; Li, E.; Rice, S.; Davey, C.G.; Ratheesh, A.; Adams, S.; Jackson, H.; Hetrick, S.; Parker, A.; Spelman, T.; et al. Cannabidiol for Treatment-Resistant Anxiety Disorders in Young People: An Open-Label Trial. J. Clin. Psychiatry 2022, 83, 42111. [Google Scholar] [CrossRef] [PubMed]
- Fliegel, D.K.; Lichenstein, S.D. Systematic literature review of human studies assessing the efficacy of cannabidiol for social anxiety. Psychiatry Res. Commun. 2022, 2, 100074. [Google Scholar] [CrossRef] [PubMed]
- Zuardi, A.W. Cannabidiol: From an inactive cannabinoid to a drug with wide spectrum of action. Rev. Bras. Psiquiatr. 2008, 30, 271–280. [Google Scholar] [CrossRef] [PubMed]
- de Mello Schier, A.R.; de Oliveira Ribeiro, N.P.; Coutinho, D.S.; Machado, S.; Arias-Carrión, O.; Crippa, J.A.; Zuardi, A.W.; Nardi, A.E.; Silva, A.C. Antidepressant-like and anxiolytic-like effects of cannabidiol: A chemical compound of Cannabis sativa. CNS Neurol. Disord. Drug Targets. 2014, 13, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.; Shahinas, J. Dosage, Efficacy and Safety of Cannabidiol Administration in Adults: A Systematic Review of Human Trials. J. Clin. Med. Res. 2020, 12, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Irving, P.M.; Iqbal, T.; Nwokolo, C.; Subramanian, S.; Bloom, S.; Prasad, N.; Hart, A.; Murray, C.; Lindsay, J.O.; Taylor, A.; et al. A Randomized, Double-blind, Placebo-controlled, Parallel-group, Pilot Study of Cannabidiol-rich Botanical Extract in the Symptomatic Treatment of Ulcerative Colitis. Inflamm. Bowel Dis. 2018, 24, 714–724. [Google Scholar] [CrossRef] [PubMed]
- Bosnjak Kuharic, D.; Markovic, D.; Brkovic, T.; Jeric Kegalj, M.; Rubic, Z.; Vuica Vukasovic, A.; Jeroncic, A.; Puljak, L. Cannabinoids for the Treatment of Dementia. Cochrane Database Syst. Rev. 2021, 9, CD012820. [Google Scholar]
- Sales, A.J.; Fogaça, M.V.; Sartim, A.G.; Pereira, V.S.; Wegener, G.; Guimarães, F.S.; Joca, S.R.L. Cannabidiol Induces Rapid and Sustained Antidepressant-Like Effects Through Increased BDNF Signaling and Synaptogenesis in the Prefrontal Cortex. Mol. Neurobiol. 2018, 56, 1070–1081. [Google Scholar] [CrossRef]
- Ahmed, S.; Roth, R.M.; Stanciu, C.N.; Brunette, M.F. The Impact of THC and CBD in Schizophrenia: A Systematic Review. Front. Psychiatry 2021, 12, 694394. [Google Scholar] [CrossRef]
- Poleg, S.; Golubchik, P.; Offen, D.; Weizman, A. Cannabidiol as a suggested candidate for treatment of autism spectrum disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 89, 90–96. [Google Scholar] [CrossRef]
- Pedrazzi, J.F.C.; Ferreira, F.R.; Silva-Amaral, D.; Lima, D.A.; Hallak, J.E.C.; Zuardi, A.W.; Del-Bel, E.A.; Guimarães, F.S.; Costa, K.C.M.; Campos, A.C.; et al. Cannabidiol for the treatment of autism spectrum disorder: Hope or hype? Psychopharmacology 2022, 239, 2713–2734. [Google Scholar] [CrossRef]
- Kirkland, A.E.; Fadus, M.C.; Gruber, S.A.; Gray, K.M.; Wilens, T.E.; Squeglia, L.M. A scoping review of the use of cannabidiol in psychiatric disorders. Psychiatry Res. 2022, 308, 114347. [Google Scholar] [CrossRef]
- Khalsa, J.H.; Bunt, G.; Blum, K.; Maggirwar, S.B.; Galanter, M.; Potenza, M.N. Review: Cannabinoids as Medicinals. Curr. Addict. Rep. 2022, 9, 630–646. [Google Scholar] [CrossRef]
- Ahadi, S.; Zhou, W.; Schüssler-Fiorenza Rose, S.M.; Sailani, M.R.; Contrepois, K.; Avina, M.; Ashland, M.; Brunet, A.; Snyder, M. Personal aging markers and ageotypes revealed by deep longitudinal profiling. Nat. Med. 2020, 26, 83–90. [Google Scholar] [CrossRef]
- Dash, R.; Ali, C.; Jahan, I.; Munni, Y.A.; Mitra, S.; Hannan, A.; Timalsina, B.; Oktaviani, D.F.; Choi, H.J.; Moon, I.S. Emerging potential of cannabidiol in reversing proteinopathies. Ageing Res. Rev. 2020, 65, 101209. [Google Scholar] [CrossRef] [PubMed]
- Farr, S.A.; Goodland, M.N.; Niehoff, M.L.; Banerjee, S.; Young, B.J. Cannabidiol (CBD) improves cognition and decreases anxiety in the SAMP8 mouse model of Alzheimer’s. Alzheimer’s Dement. 2021, 17, e054428. [Google Scholar] [CrossRef]
- Kreilaus, F.; Przybyla, M.; Ittner, L.; Karl, T. Cannabidiol (CBD) treatment improves spatial memory in 14-month-old female TAU58/2 transgenic mice. Behav. Brain Res. 2022, 425, 113812. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, M.K.; Mondal, S.; Gangwar, M.; Jana, S. Effects of Cannabidiol Interactions withCYP2R1, CYP27B1, CYP24A1,and Vitamin D3Receptors on Spatial Memory, Pain, Inflammation, and Aging in Vitamin D3Deficiency Diet-Induced Rats. Cannabis Cannabinoid Res. 2022; ahead of print. [Google Scholar] [CrossRef]
- Jîtcă, G.; Ősz, B.E.; Vari, C.E.; Rusz, C.-M.; Tero-Vescan, A.; Pușcaș, A. Cannabidiol: Bridge between Antioxidant Effect, Cellular Protection, and Cognitive and Physical Performance. Antioxidants 2023, 12, 485. [Google Scholar] [CrossRef]
- Faria, D.d.P.; de Souza, L.E.; Duran, F.L.d.S.; Buchpiguel, C.A.; Britto, L.R.; Crippa, J.A.d.S.; Filho, G.B.; Real, C.C. Cannabidiol Treatment Improves Glucose Metabolism and Memory in Streptozotocin-Induced Alzheimer’s Disease Rat Model: A Proof-of-Concept Study. Int. J. Mol. Sci. 2022, 23, 1076. [Google Scholar] [CrossRef]
- Hassan, S.; Eldeeb, K.; Millns, P.J.; Bennett, A.J.; Alexander, S.P.H.; Kendall, D.A. Cannabidiol enhances microglial phagocytosis via transient receptor potential (TRP) channel activation. Br. J. Pharmacol. 2014, 171, 2426–2439. [Google Scholar] [CrossRef]
- Yang, S.; Du, Y.; Zhao, X.; Tang, Q.; Su, W.; Hu, Y.; Yu, P. Cannabidiol Enhances Microglial Beta-Amyloid Peptide Phagocytosis and Clearance via Vanilloid Family Type 2 Channel Activation. Int. J. Mol. Sci. 2022, 23, 5367. [Google Scholar] [CrossRef]
- Xiong, Y.; Lim, C.-S. Understanding the Modulatory Effects of Cannabidiol on Alzheimer’s Disease. Brain Sci. 2021, 11, 1211. [Google Scholar] [CrossRef]
- Hermush, V.; Ore, L.; Stern, N.; Mizrahi, N.; Fried, M.; Krivoshey, M.; Staghon, E.; Lederman, V.E.; Schleider, L.B.-L. Effects of rich cannabidiol oil on behavioral disturbances in patients with dementia: A placebo controlled randomized clinical trial. Front. Med. 2022, 9, 951889. [Google Scholar] [CrossRef] [PubMed]
- Alexandri, F.; Papadopoulou, L.; Tsolaki, A.; Papantoniou, G.; Athanasiadis, L.; Tsolaki, M. The Effect of Cannabidiol 3% on Neuropsychiatric Symptoms in Dementia—Six-Month Follow-Up. Clin. Gerontol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Bartschi, J.G.; Greenwood, L.-M.; Montgomery, A.; Dortants, L.; Weston-Green, K.; Huang, X.-F.; Pai, N.; Potter, J.; Schira, M.M.; Croft, R.; et al. Cannabidiol as a Treatment for Neurobiological, Behavioral, and Psychological Symptoms in Early-Stage Dementia: A Double-Blind, Placebo-Controlled Clinical Trial Protocol. Cannabis Cannabinoid Res. 2022, 8, 348–359. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Ookuma, S.; Nishida, E. Lifespan extension by suppression of autophagy genes in Caenorhabditis elegans. Genes Cells 2009, 14, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Braeckman, B.P.; Vanfleteren, J.R. Genetic control of longevity in C. Elegans. Exp. Gerontol. 2007, 42, 90–98. [Google Scholar] [CrossRef]
- Vrechi, T.A.M.; Leão, A.H.F.F.; Morais, I.B.M.; Abílio, V.C.; Zuardi, A.W.; Hallak, J.E.C.; Crippa, J.A.; Bincoletto, C.; Ureshino, R.P.; Smaili, S.S.; et al. Cannabidiol induces autophagy via ERK1/2 activation in neural cells. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Salminen, A.; Kaarniranta, K. SIRT1: Regulation of longevity via autophagy. Cell. Signal. 2009, 21, 1356–1360. [Google Scholar] [CrossRef]
- Wang, Z.; Zheng, P.; Chen, X.; Xie, Y.; Weston-Green, K.; Solowij, N.; Chew, Y.L.; Huang, X.-F. Cannabidiol induces autophagy and improves neuronal health associated with SIRT1 mediated longevity. GeroScience 2022, 44, 1505–1524. [Google Scholar] [CrossRef]
- Wang, Z.; Zheng, P.; Xie, Y.; Chen, X.; Solowij, N.; Green, K.; Chew, Y.L.; Huang, X.-F. Cannabidiol regulates CB1-pSTAT3 signaling for neurite outgrowth, prolongs lifespan, and improves health span in Caenorhabditis elegans of Aβ pathology models. FASEB J. 2021, 35, e21537. [Google Scholar] [CrossRef]
- Cannabidiol. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012; Updated 16 February 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/31643176/ (accessed on 16 March 2023).
- Leehey, M.A.; Liu, Y.; Hart, F.; Epstein, C.; Cook, M.; Sillau, S.; Klawitter, J.; Newman, H.; Sempio, C.; Forman, L.; et al. Safety and Tolerability of Cannabidiol in Parkinson Disease: An Open Label, Dose-Escalation Study. Cannabis Cannabinoid Res. 2020, 5, 326–336. [Google Scholar] [CrossRef]
- Lo, L.A.; Christiansen, A.; Eadie, L.; Strickland, J.C.; Kim, D.D.; Boivin, M.; Barr, A.M.; MacCallum, C.A. Cannabidiol-associated hepatotoxicity: A systematic review and meta-analysis. J. Intern. Med. 2023, 293, 724–752. [Google Scholar] [CrossRef] [PubMed]
- Rapin, L.; Gamaoun, R.; El Hage, C.; Arboleda, M.F.; Prosk, E. Cannabidiol use and effectiveness: Real-world evidence from a Canadian medical cannabis clinic. J. Cannabis Res. 2021, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trojan, V.; Landa, L.; Šulcová, A.; Slíva, J.; Hřib, R. The Main Therapeutic Applications of Cannabidiol (CBD) and Its Potential Effects on Aging with Respect to Alzheimer’s Disease. Biomolecules 2023, 13, 1446. https://doi.org/10.3390/biom13101446
Trojan V, Landa L, Šulcová A, Slíva J, Hřib R. The Main Therapeutic Applications of Cannabidiol (CBD) and Its Potential Effects on Aging with Respect to Alzheimer’s Disease. Biomolecules. 2023; 13(10):1446. https://doi.org/10.3390/biom13101446
Chicago/Turabian StyleTrojan, Václav, Leoš Landa, Alexandra Šulcová, Jiří Slíva, and Radovan Hřib. 2023. "The Main Therapeutic Applications of Cannabidiol (CBD) and Its Potential Effects on Aging with Respect to Alzheimer’s Disease" Biomolecules 13, no. 10: 1446. https://doi.org/10.3390/biom13101446
APA StyleTrojan, V., Landa, L., Šulcová, A., Slíva, J., & Hřib, R. (2023). The Main Therapeutic Applications of Cannabidiol (CBD) and Its Potential Effects on Aging with Respect to Alzheimer’s Disease. Biomolecules, 13(10), 1446. https://doi.org/10.3390/biom13101446