


Dances with Social Robots: A Pilot Study at Long-Term Care

Abstract
:1. Introduction
2. Related Works
2.1. Robot Dance for Older Adults
2.2. HRI Studies with Older Adults and Caregivers
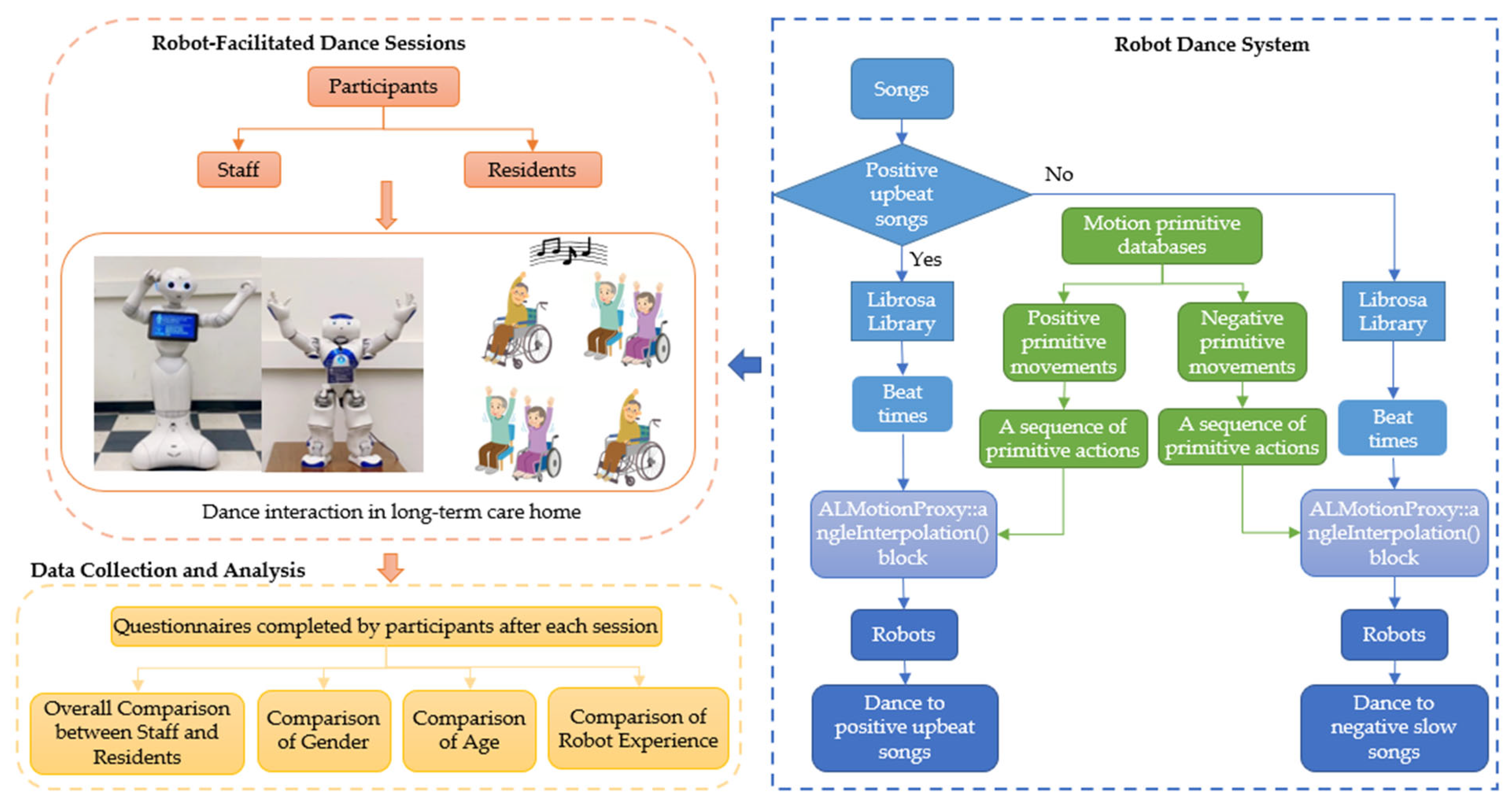
3. Robot Dance Pilot Study Methodology
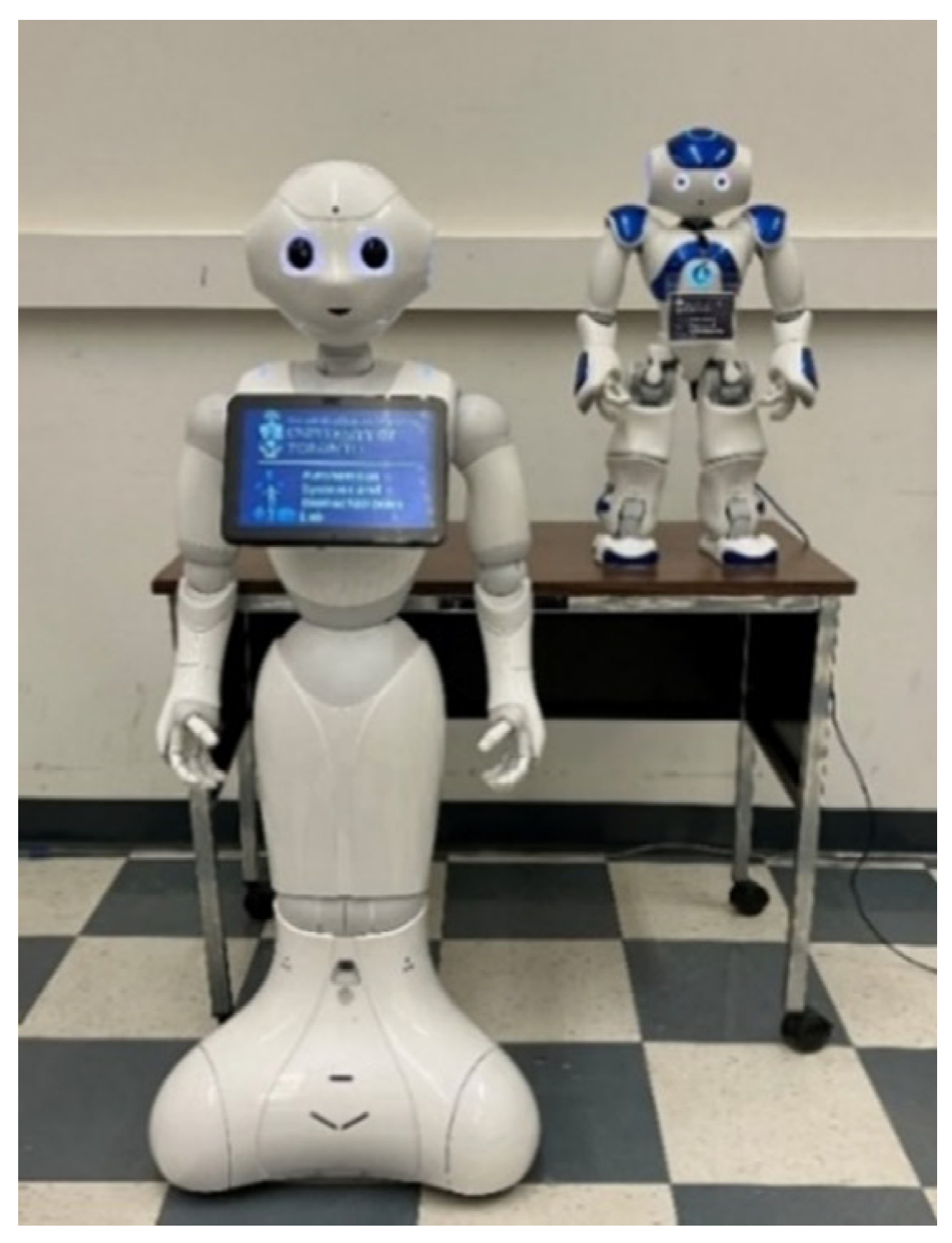
3.1. Robot Dance Design
3.2. Participants
3.3. Procedure
3.4. Measures
4. Results
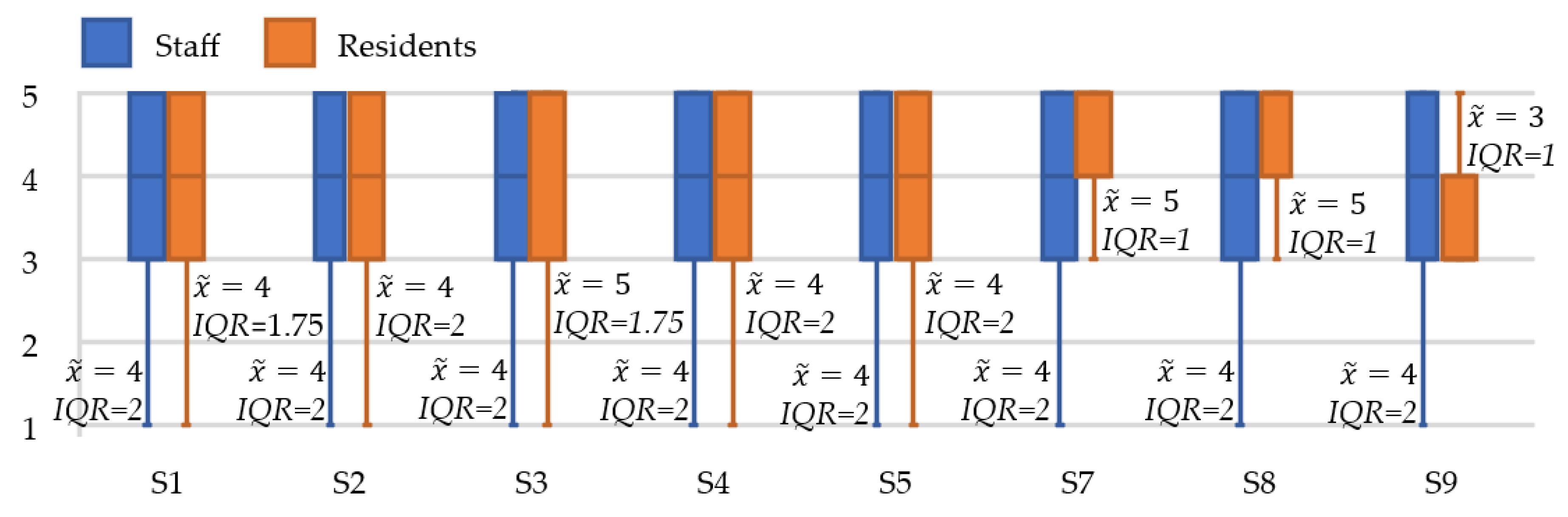
4.1. Staff and Resident Comparison
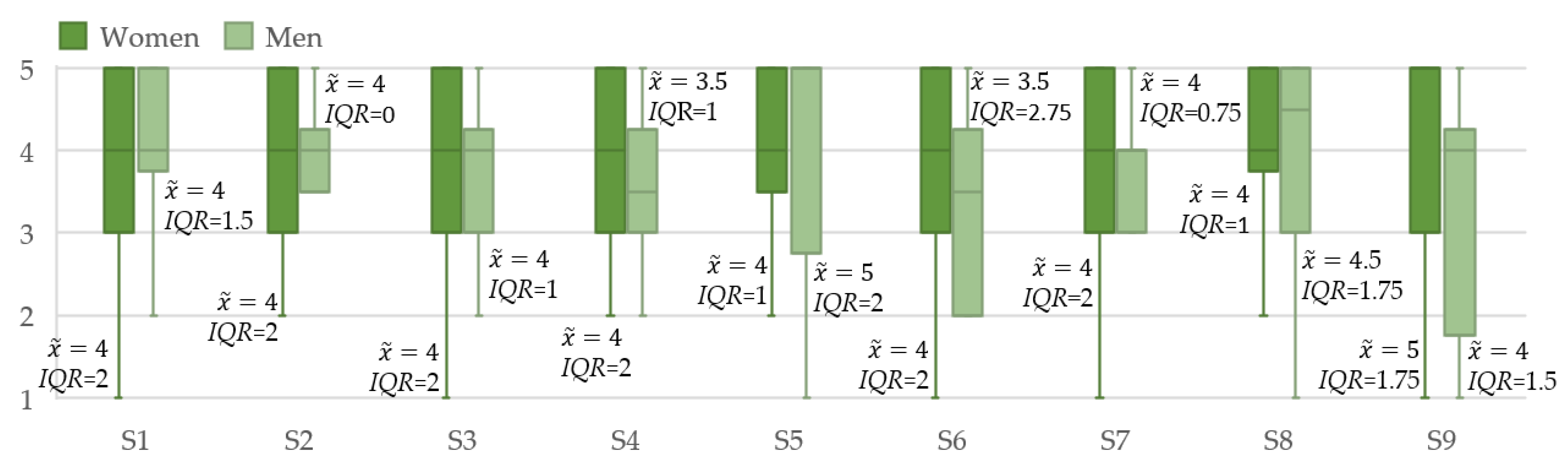
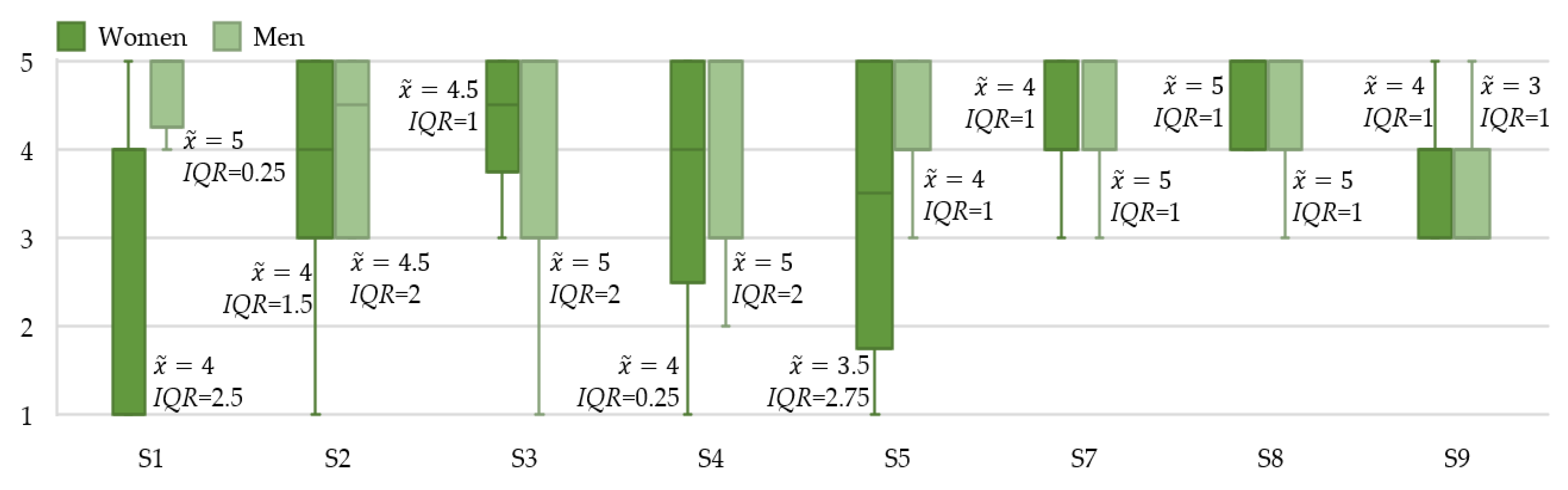
4.2. Gender
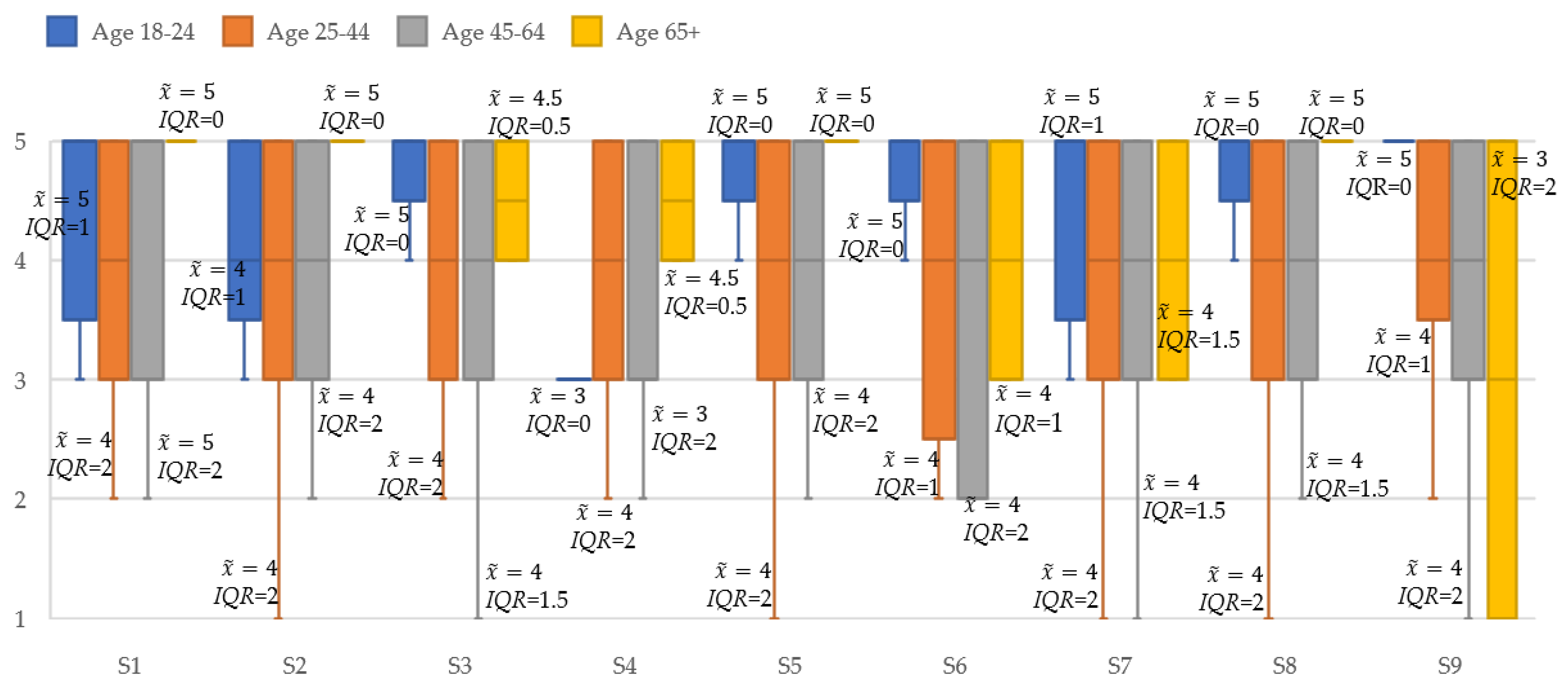
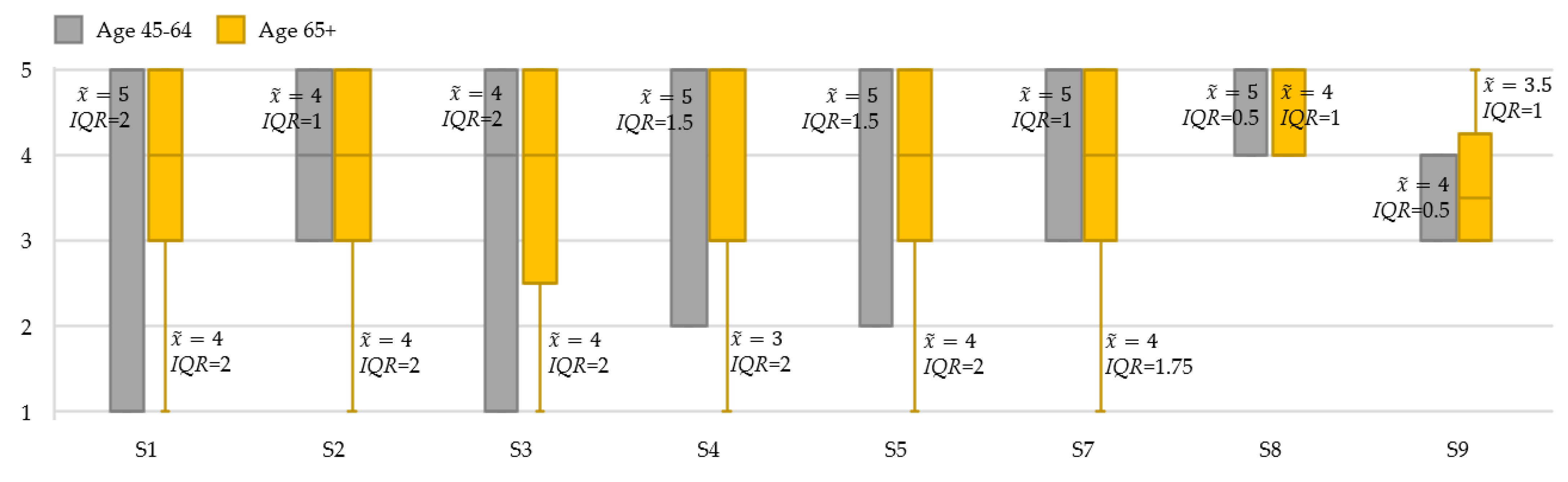
4.3. Age
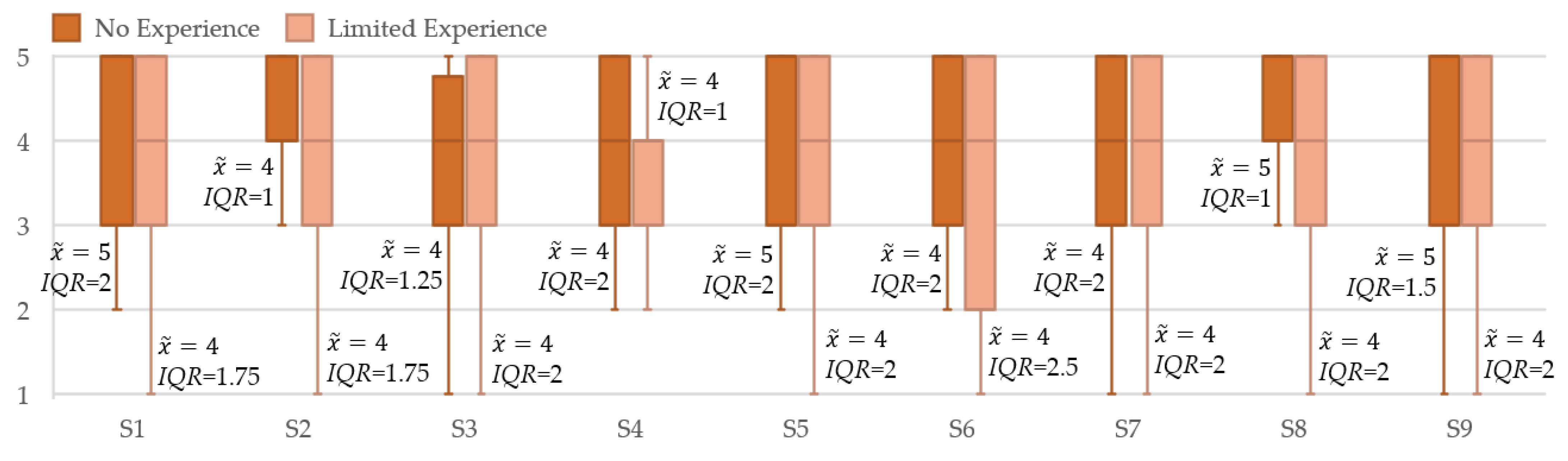
4.4. Prior Robot Experience
5. Discussions
5.1. Comparison of Staff and Residents
5.2. Gender
5.3. Age
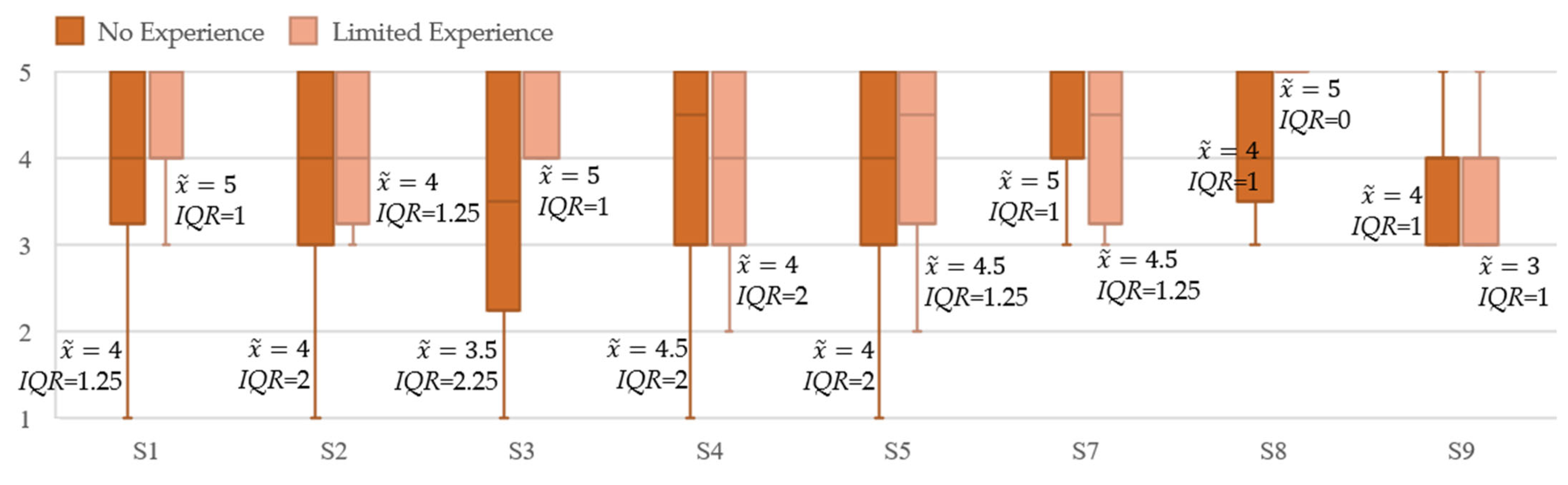
5.4. Prior Robot Experience
5.5. Robot Types
5.6. Comparisons to Previous Other HRI Studies
5.7. Study Considerations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strassel, J.K.; Cherkin, D.C.; Steuten, L.; Sherman, K.J.; Vrijhoef, H.J. A Systematic Review of the Evidence for the Effectiveness of Dance Therapy. Altern. Ther. Health Med. 2011, 17, 50–59. [Google Scholar] [PubMed]
- Coubard, O.A.; Duretz, S.; Lefebvre, V.; Lapalus, P.; Ferrufino, L. Practice of Contemporary Dance Improves Cognitive Flexibility in Aging. Front. Aging Neurosci. 2011, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Hwang, P.W.-N.; Braun, K.L. The Effectiveness of Dance Interventions to Improve Older Adults’ Health: A Systematic Literature Review. Altern. Ther. Health Med. 2015, 21, 64. [Google Scholar] [PubMed]
- Alpert, P.T. The Health Benefits of Dance. Home Health Care Manag. Pract. 2011, 23, 155–157. [Google Scholar] [CrossRef]
- Earhart, G.M. Dance as Therapy for Individuals with Parkinson Disease. Eur. J. Phys. Rehabil. Med. 2009, 45, 231. [Google Scholar]
- Hackney, M.E.; Earhart, G.M. Effects of Dance on Movement Control in Parkinson’s Disease: A Comparison of Argentine Tango and American Ballroom. J. Rehabil. Med. Off. J. UEMS Eur. Board Phys. Rehabil. Med. 2009, 41, 475. [Google Scholar] [CrossRef]
- Ho, R.T.; Fong, T.C.; Chan, W.C.; Kwan, J.S.; Chiu, P.K.; Yau, J.C.; Lam, L.C. Psychophysiological Effects of Dance Movement Therapy and Physical Exercise on Older Adults with Mild Dementia: A Randomized Controlled Trial. J. Gerontol. Ser. B 2020, 75, 560–570. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Hsieh, S.; Li, C.-W. Needs and Preferences of Middle-Aged and Older Adults in Taiwan for Companion Robots and Pets: Survey Study. J. Med. Internet Res. 2021, 23, e23471. [Google Scholar] [CrossRef]
- Sefcik, J.S.; Johnson, M.J.; Yim, M.; Lau, T.; Vivio, N.; Mucchiani, C.; Cacchione, P.Z. Stakeholders’ Perceptions Sought to Inform the Development of a Low-Cost Mobile Robot for Older Adults: A Qualitative Descriptive Study. Clin. Nurs. Res. 2018, 27, 61–80. [Google Scholar] [CrossRef]
- Kosuge, K.; Hayashi, T.; Hirata, Y.; Tobiyama, R. Dance partner robot-ms dancer. In Proceedings of the 2003 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS 2003) (Cat. No. 03CH37453), Las Vegas, NV, USA, 27–31 October 2003; IEEE: New York, NY, USA, 2003; Volume 4, pp. 3459–3464. [Google Scholar]
- Chen, T.L.; Bhattacharjee, T.; Beer, J.M.; Ting, L.H.; Hackney, M.E.; Rogers, W.A.; Kemp, C.C. Older Adults’ Acceptance of a Robot for Partner Dance-Based Exercise. PLoS ONE 2017, 12, e0182736. [Google Scholar] [CrossRef]
- Venture, G.; Indurkhya, B.; Izui, T. Dance with me! Child-robot interaction in the wild. In Proceedings of the International Conference on Social Robotics, Golden, CO, USA, 14–18 November 2020; Springer: Berlin/Heidelberg, Germany, 2017; pp. 375–382. [Google Scholar]
- Ros, R.; Baroni, I.; Demiris, Y. Adaptive Human–Robot Interaction in Sensorimotor Task Instruction: From Human to Robot Dance Tutors. Robot. Auton. Syst. 2014, 62, 707–720. [Google Scholar] [CrossRef] [Green Version]
- Lei, X.; Rau, P.-L.P. Effect of Robot Tutor’s Feedback Valence and Attributional Style on Learners. Int. J. Soc. Robot. 2021, 13, 1579–1597. [Google Scholar] [CrossRef]
- Pedell, S.; Constantin, K.; Muñoz, D.; Sterling, L. Designing meaningful, beneficial and positive human robot interactions with older adults for increased wellbeing during care activities. In Handbook of Artificial Intelligence in Healthcare; Springer: Berlin/Heidelberg, Germany, 2022; pp. 85–108. [Google Scholar]
- Javed, H.; Park, C.H. Promoting Social Engagement with a Multi-Role Dancing Robot for In-Home Autism Care. Front. Robot. AI 2022, 4, 161. [Google Scholar] [CrossRef]
- Sawami, K.; Kimura, M.; Kitamura, T.; Kawaguchi, M.; Furusumi, M.; Suishu, C.; Morisaki, N.; Hattori, S. Cognitive Ability and Psychological Effectiveness of Brain Training Dance Robot Therapy for Elderly People. OA J. Neuropsychiatry 2019, 1, 004. [Google Scholar] [CrossRef]
- Broadbent, E.; Stafford, R.; MacDonald, B. Acceptance of Healthcare Robots for the Older Population: Review and Future Directions. Int. J. Soc. Robot. 2009, 1, 319–330. [Google Scholar] [CrossRef]
- Papadopoulos, I.; Koulouglioti, C.; Lazzarino, R.; Ali, S. Enablers and Barriers to the Implementation of Socially Assistive Humanoid Robots in Health and Social Care: A Systematic Review. BMJ Open 2020, 10, e033096. [Google Scholar] [CrossRef] [PubMed]
- Persson, M.; Redmalm, D.; Iversen, C. Caregivers’ Use of Robots and Their Effect on Work Environment—A Scoping Review. J. Technol. Hum. Serv. 2021, 40, 251–277. [Google Scholar] [CrossRef]
- Franke, A.; Nass, E.; Piereth, A.-K.; Zettl, A.; Heidl, C. Implementation of Assistive Technologies and Robotics in Long-Term Care Facilities: A Three-Stage Assessment Based on Acceptance, Ethics, and Emotions. Front. Psychol. 2021, 12, 694297. [Google Scholar] [CrossRef]
- Yu, P.; Li, H.; Gagnon, M.-P. Health IT Acceptance Factors in Long-Term Care Facilities: A Cross-Sectional Survey. Int. J. Med. Inform. 2009, 78, 219–229. [Google Scholar] [CrossRef]
- Dijkers, M.P.; deBear, P.C.; Erlandson, R.F.; Kristy, K.; Geer, D.M.; Nichols, A. Patient and Staff Acceptance of Robotic Technology in Occupational Therapy: A Pilot Study. JRRD 1991, 28, 33. [Google Scholar] [CrossRef]
- Tuisku, O.; Pekkarinen, S.; Hennala, L.; Melkas, H. “Robots Do Not Replace a Nurse with a Beating Heart”: The Publicity around a Robotic Innovation in Elderly Care. Inf. Technol. People 2018, 32, 47–67. [Google Scholar] [CrossRef]
- Melkas, H.; Hennala, L.; Pekkarinen, S.; Kyrki, V. Impacts of Robot Implementation on Care Personnel and Clients in Elderly-Care Institutions. Int. J. Med. Inform. 2020, 134, 104041. [Google Scholar] [CrossRef]
- Broadbent, E.; Tamagawa, R.; Patience, A.; Knock, B.; Kerse, N.; Day, K.; MacDonald, B.A. Attitudes towards Health-Care Robots in a Retirement Village. Australas. J. Ageing 2012, 31, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Sabelli, A.M.; Kanda, T.; Hagita, N. A conversational robot in an elderly care center: An ethnographic study. In Proceedings of the 2011 6th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Lausanne, Switzerland, 6–9 March 2011; IEEE: New York, NY, USA, 2011; pp. 37–44. [Google Scholar]
- Hebesberger, D.; Koertner, T.; Gisinger, C.; Pripfl, J. A Long-Term Autonomous Robot at a Care Hospital: A Mixed Methods Study on Social Acceptance and Experiences of Staff and Older Adults. Int. J. Soc. Robot. 2017, 9, 417–429. [Google Scholar] [CrossRef]
- Bedaf, S.; Marti, P.; Amirabdollahian, F.; de Witte, L. A Multi-Perspective Evaluation of a Service Robot for Seniors: The Voice of Different Stakeholders. Disabil. Rehabil. Assist. Technol. 2018, 13, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Koceski, S.; Koceska, N. Evaluation of an Assistive Telepresence Robot for Elderly Healthcare. J. Med. Syst. 2016, 40, 121. [Google Scholar] [CrossRef]
- Potnuru, A.; Jafarzadeh, M.; Tadesse, Y. 3D printed dancing humanoid robot “buddy” for homecare. In Proceedings of the 2016 IEEE International Conference on Automation Science and Engineering (CASE), Fort Worth, TX, USA, 21–25 August 2016; IEEE: New York, NY, USA, 2016; pp. 733–738. [Google Scholar]
- Khosla, R.; Nguyen, K.; Chu, M.-T. Human Robot Engagement and Acceptability in Residential Aged Care. Int. J. Hum.–Comput. Interact. 2017, 33, 510–522. [Google Scholar] [CrossRef]
- Khosla, R.; Chu, M.-T.; Khaksar, S.M.S.; Nguyen, K.; Nishida, T. Engagement and Experience of Older People with Socially Assistive Robots in Home Care. Assist. Technol. 2021, 33, 57–71. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Benadduci, M.; Bonfigli, A.R.; Riccardi, G.R.; Melone, G.; La Forgia, A.; Macchiarulo, N.; Rossetti, L.; Marzorati, M.; Rizzo, G. Dancing With Parkinson’s Disease: The SI-ROBOTICS Study Protocol. Front. Public Health 2021, 9, 780098. [Google Scholar] [CrossRef]
- Back, I.; Kallio, J. Robot-Guided Exercise Program for the Rehabilitation of Older Nursing Home Residents. Ann. Long-Term Care 2013, 21, 6. [Google Scholar]
- Pepper-Technical Overview—Aldebaran 2.0.6.8 Documentation. Available online: http://doc.aldebaran.com/2-0/family/juliette_technical/index_juliette.html (accessed on 25 August 2022).
- NAO-Technical Overview—Aldebaran 2.0.6.8 Documentation. Available online: http://doc.aldebaran.com/2-0/family/robots/index_robots.html (accessed on 25 August 2022).
- De Meijer, M. The Contribution of General Features of Body Movement to the Attribution of Emotions. J. Nonverbal Behav. 1989, 13, 247–268. [Google Scholar] [CrossRef]
- McColl, D.; Nejat, G. Recognizing Emotional Body Language Displayed by a Human-Like Social Robot. Int. J. Soc. Robot. 2014, 6, 261–280. [Google Scholar] [CrossRef]
- Librosa. Librosa 0.9.1 Documentation. Available online: https://librosa.org/doc/latest/index.html (accessed on 10 March 2022).
- Ellis, D.P.W. Beat Tracking by Dynamic Programming. J. New Music. Res. 2007, 36, 51–60. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, G.; Wei, D.; Li, Q.; Yuan, G.; Wu, S.; Wang, G.; Zhao, X. Effects of Musical Tempo on Musicians’ and Non-Musicians’ Emotional Experience When Listening to Music. Front. Psychol. 2018, 9, 2118. [Google Scholar] [CrossRef]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef]
- Smarr, C.-A.; Mitzner, T.L.; Beer, J.M.; Prakash, A.; Chen, T.L.; Kemp, C.C.; Rogers, W.A. Domestic Robots for Older Adults: Attitudes, Preferences, and Potential. Int. J. Soc. Robot. 2014, 6, 229–247. [Google Scholar] [CrossRef]
- Heerink, M.; Kröse, B.; Wielinga, B.; Evers, V. Enjoyment intention to use and actual use of a conversational robot by elderly people. In Proceedings of the the 3rd ACM/IEEE International Conference on Human Robot Interaction, Amsterdam, The Netherlands, 12–15 March 2008; pp. 113–120. [Google Scholar]
- Bartneck, C.; Kulić, D.; Croft, E.; Zoghbi, S. Measurement Instruments for the Anthropomorphism, Animacy, Likeability, Perceived Intelligence, and Perceived Safety of Robots. Int. J. Soc. Robot. 2009, 1, 71–81. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Stone, A.; Shiffman, S.; Atienza, A.; Nebeling, L. The Science of Real-Time Data Capture: Self-Reports in Health Research; Oxford University Press: Oxford, UK, 2007; ISBN 0-19-534631-9. [Google Scholar]
- Rolstad, S.; Adler, J.; Rydén, A. Response Burden and Questionnaire Length: Is Shorter Better? A Review and Meta-Analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef]
- Kato, T.; Miura, T. The Impact of Questionnaire Length on the Accuracy Rate of Online Surveys. J. Mark. Anal. 2021, 9, 83–98. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a Test of Whether One of Two Random Variables Is Stochastically Larger than the Other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Costa, S.; Hausenblas, H.A.; Oliva, P.; Cuzzocrea, F.; Larcan, R. The Role of Age, Gender, Mood States and Exercise Frequency on Exercise Dependence. J. Behav. Addict. 2013, 2, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada. Canada Pension Plan—Overview. Available online: https://www.canada.ca/en/services/benefits/publicpensions/cpp.html (accessed on 30 June 2022).
- Gross, H.-M.; Schroeter, C.; Mueller, S.; Volkhardt, M.; Einhorn, E.; Bley, A.; Langner, T.; Merten, M.; Huijnen, C.; van den Heuvel, H.; et al. Further progress towards a home robot companion for people with mild cognitive impairment. In Proceedings of the 2012 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Seoul, Korea, 14–17 October 2012; pp. 637–644. [Google Scholar]
- Krakovski, M.; Kumar, S.; Givati, S.; Bardea, M.; Zafrani, O.; Nimrod, G.; Bar-Haim, S.; Edan, Y. “Gymmy”: Designing and Testing a Robot for Physical and Cognitive Training of Older Adults. Appl. Sci. 2021, 11, 6431. [Google Scholar] [CrossRef]
- Bishop, L.; van Maris, A.; Dogramadzi, S.; Zook, N. Social Robots: The Influence of Human and Robot Characteristics on Acceptance. Paladyn J. Behav. Robot. 2019, 10, 346–358. [Google Scholar] [CrossRef]
- Kuo, I.H.; Rabindran, J.M.; Broadbent, E.; Lee, Y.I.; Kerse, N.; Stafford, R.M.; MacDonald, B.A. Age and gender factors in user acceptance of healthcare robots. In Proceedings of the RO-MAN 2009—The 18th IEEE International Symposium on Robot and Human Interactive Communication, Toyama, Japan, 27 September–2 October 2009; IEEE: New York, NY, USA, 2009; pp. 214–219. [Google Scholar]
- Heerink, M. Exploring the influence of age, gender, education and computer experience on robot acceptance by older adults. In Proceedings of the 2011 6th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Lausanne, Switzerland, 8–11 March 2011; IEEE: New York, NY, USA, 2011; pp. 147–148. [Google Scholar]
- Sims-Gould, J.; McKay, H.A.; Feldman, F.; Scott, V.; Robinovitch, S.N. Autonomy, Choice, Patient-Centered Care, and Hip Protectors: The Experience of Residents and Staff in Long-Term Care. J. Appl. Gerontol. 2014, 33, 690–709. [Google Scholar] [CrossRef]
- Vichitkraivin, P.; Naenna, T. Factors of Healthcare Robot Adoption by Medical Staff in Thai Government Hospitals. Health Technol. 2021, 11, 139–151. [Google Scholar] [CrossRef]
- Hall, A.K.; Backonja, U.; Painter, I.; Cakmak, M.; Sung, M.; Lau, T.; Thompson, H.J.; Demiris, G. Acceptance and Perceived Usefulness of Robots to Assist with Activities of Daily Living and Healthcare Tasks. Assist. Technol. 2017, 31, 133–140. [Google Scholar] [CrossRef]
- Esposito, A.; Cuciniello, M.; Amorese, T.; Esposito, A.M.; Troncone, A.; Maldonato, M.N.; Vogel, C.; Bourbakis, N.; Cordasco, G. Seniors’ appreciation of humanoid robots. In Neural Approaches to Dynamics of Signal Exchanges; Springer: Berlin/Heidelberg, Germany, 2020; pp. 331–345. [Google Scholar]
- Zhumabekova, K.; Ismailova, A.; Kushkinbayev, D.; Sandygulova, A. Exploring the effects of robot gender on child-robot interaction. In Proceedings of the Companion of the 2018 ACM/IEEE International Conference on Human-Robot Interaction, New York, NY, USA, 1 March 2018; Association for Computing Machinery: New York, NY, USA, 2018; pp. 287–288. [Google Scholar]
- Schneider, S.; Kummert, F. Does the user’s evaluation of a socially assistive robot change based on presence and companionship type? In Proceedings of the Companion of the 2017 ACM/IEEE International Conference on Human-Robot Interaction, New York, NY, USA, 6 March 2017; Association for Computing Machinery: New York, NY, USA, 2017; pp. 277–278. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviations | Variables | ||
|---|---|---|---|
| HRI | human–robot interaction | D | The set of beat times in a song |
| TAM | technology acceptance model | ai | the ith primitive action |
| MWU | Mann-Whitney U | A | the sequence of primitive actions |
| KW | Kruskal-Wallis | T | the time trajectory |
| Si | the ith statement in the questionnaire | median value | |
| IQR | interquartile range | ||
| Min | minual value | ||
| Max | maximul value | ||
| U | the corresponding MWU statistic | ||
| H | the corresponding KW statistic | ||
| p | significance level | ||
| Reference | Robot Platform | Participants and Environment | Tasks and Functionalities | Methods | Findings |
|---|---|---|---|---|---|
| [25] | Zora robot | Care personnel and elderly clients in care homes and a geriatric rehabilitation hospital | Physical exercises, playing music, storytelling, dancing, interactive memory and playing guessing games | Focus group semi-structured interviews and interaction observations. | Staff expressed concerns regarding training on how to properly use the robot and the increased workload related to operating the robot. Residents found the robot funny, entertaining and interesting. |
| [27] | Robovie2 robot | Older adults and staff in an elderly care center | Greetings and engaging in conversations | Semi-structured interviews and interaction observations. | In general, staff had positive attitudes towards the robot. Older adults expressed willingness to interact with Robovie2. |
| [28] | SCITOS Robot | Older adults and employees in a care hospital | Autonomous navigation indoors, patrolling an area and greeting passersby. | Semi-structured interviews, interaction observations and questionnaires. | Staff had a moderate level acceptance of the robot, whereas older adults had higher acceptance. Staff also expressed concerns about the robot occupying their workspace and replacing them. |
| [29] | Care-O-bot 3 Robot | Older adults, informal cares and professional caregivers in a home-like testing environment | Package pick-ups and reminders for drinking water | Semi-structured interviews and questionaries | The robot was accepted more by the older adults than caregivers. Caregivers expressed concerns about the robot not being able to operate independently without supervision. |
| [30] | Assistive telepresence robot | Professional caregivers and elderly residents in a nursing home | Navigation indoors, vital sign measurements, video conferencing and reminders | Questionaries | Staff found vital sign measurements and reminders more useful than the older adults did. The older adults found video conferencing more useful than the staff did. |
| Robots | Main Features | ||||
|---|---|---|---|---|---|
| Height (m) | Mobile Base | Degrees-of-Freedom | Speakers | Microphones | |
| Salt (Pepper Robot by Softbank [36]) | 1.2 (human-size) | Omnidirectional wheeled base | 20 (Head: 2; Arm: 5 × 2; Hand: 1 × 2; Hip: 2; Knee: 1; Mobile base: 3) | ×2 on both sides of the head | ×4 on the head |
| Luke (Nao Robot by Softbank [37]) | 0.574 (toy-size) | Biped | 25 (Head: 2; Arm: 5 × 2; Hand: 1 × 2; Hip: 1; Leg: 5 × 2) | ×2 on both sides of the head | ×4 on the head |
| Examples | Positive Motion Primitives for Salt and Luke | ||
|---|---|---|---|
| 1 |  |  |  |
| 2 |  |  |  |
| 3 |  |  |  |
| 4 |  |  |  |
| Examples | Negative Motion Primitives for Salt and Luke | ||
| 1 |  |  |  |
| 2 |  |  |  |
| 3 |  |  |  |
| 4 |  |  |  |
| Statements | Median () | IQR | Min | Max | ||||
|---|---|---|---|---|---|---|---|---|
| Staff | Resident | Staff | Resident | Staff | Resident | Staff | Resident | |
| S1. It is useful to have a robot help with recreational activities. | 4 | 4 | 2 | 1.75 | 1 | 1 | 5 | 5 |
| S2. I think such robot-facilitated dance activities can enhance the wellbeing of residents. | 4 | 4 | 2 | 2 | 1 | 1 | 5 | 5 |
| S3. I think it will be easy for the residents to follow the robot during the dance sessions. | 4 | 5 | 2 | 1.75 | 1 | 1 | 5 | 5 |
| S4. It would be useful for the robot to automatically detect the residents’ emotions and pick appropriate music and dance movements to match their emotions. | 4 | 4 | 2 | 2 | 1 | 1 | 5 | 5 |
| S5. I think having a robot to facilitate the older adults to dance is a good idea. | 4 | 4 | 2 | 2 | 1 | 1 | 5 | 5 |
| S6. Using a robot would free up staff time to do other tasks. * | 4 | N/A | 2 | N/A | 1 | N/A | 5 | N/A |
| S7. I think having a robot facilitate the dance activity is safe. | 4 | 5 | 2 | 1 | 1 | 1 | 5 | 5 |
| S8. I think a robot will make the dancing activity fun. | 4 | 5 | 2 | 1 | 1 | 1 | 5 | 5 |
| S9. I would use a robot to conduct dance activities. | 4 | 3 | 2 | 1 | 1 | 1 | 5 | 5 |
| Statements | MWU Test | |
|---|---|---|
| U | p | |
| S1 | 680 | 0.816 |
| S2 | 698.5 | 0.752 |
| S3 | 559.5 | 0.127 |
| S4 | 634 | 0.55 |
| S5 | 705 | 0.865 |
| S7 | 585.5 | 0.129 |
| S8 | 602.5 | 0.171 |
| S9 | 938.5 | 0.019 |
| Statements | Staff | Residents | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Age | Experience | Gender | Age | Experience | |||||||
| U | p | H | p | U | p | U | p | H | p | U | p | |
| S1 | 185.5 | 0.91 | 2.61 | 0.456 | 230.5 | 0.109 | 18 | 0.04 | 0.24 | 0.624 | 93.5 | 0.219 |
| S2 | 220 | 0.46 | 2.818 | 0.421 | 225.5 | 0.09 | 60 | 0.74 | 0.004 | 0.947 | 83 | 0.81 |
| S3 | 212.5 | 0.573 | 5.784 | 0.123 | 338 | 0.541 | 55.5 | 0.771 | 0.044 | 0.834 | 102 | 0.089 |
| S4 | 214.5 | 0.449 | 5.978 | 0.113 | 258 | 0.44 | 44 | 0.314 | 0.316 | 0.574 | 73.5 | 0.932 |
| S5 | 181 | 0.929 | 3.992 | 0.262 | 249.5 | 0.312 | 46 | 0.381 | 0.181 | 0.671 | 84 | 0.514 |
| S6 | 223.5 | 0.251 | 4.585 | 0.205 | 226 | 0.198 | N/A | N/A | N/A | N/A | N/A | N/A |
| S7 | 234 | 0.274 | 0.686 | 0.876 | 264.5 | 0.373 | 45 | 0.211 | 0.223 | 0.637 | 73.5 | 0.81 |
| S8 | 193 | 0.95 | 3.839 | 0.279 | 243 | 0.175 | 60.5 | 0.74 | 0.691 | 0.406 | 110 | 0.087 |
| S9 | 250.5 | 0.126 | 4.853 | 0.183 | 251.5 | 0.329 | 74.5 | 0.608 | 0.039 | 0.843 | 71.5 | 0.728 |
| Statements | Gender | Age | Prior Robot Experience | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | 45–64 | 65+ | No Experience | Limited Experience | |||||||
| U | p | U | p | U | p | U | p | U | p | U | p | |
| S1 | 81.5 | 0.159 | 121.5 | 0.082 | 14 | 1 | 4 | 0.171 | 141 | 0.439 | 182 | 0.074 |
| S2 | 72 | 0.456 | 200 | 0.82 | 14.5 | 0.864 | 5 | 0.2 | 166 | 0.668 | 164.5 | 0.245 |
| S3 | 77.5 | 0.254 | 224 | 0.401 | 13 | 1 | 9 | 0.571 | 164.5 | 0.919 | 192 | 0.031 |
| S4 | 79 | 0.228 | 166.5 | 0.636 | 16.5 | 0.6 | 7 | 0.381 | 170 | 0.965 | 152.5 | 0.326 |
| S5 | 59.5 | 0.974 | 146 | 0.322 | 15.5 | 0.727 | 5 | 0.229 | 134.5 | 0.408 | 152 | 0.488 |
| S7 | 96 | 0.017 | 0.208 | 0.98 | 16.5 | 0.6 | 14.5 | 1 | 210 | 0.446 | 165 | 0.245 |
| S8 | 70.5 | 0.497 | 232 | 0.551 | 18 | 0.482 | 6 | 0.267 | 165 | 0.648 | 202 | 0.011 |
| S9 | 48 | 0.456 | 134 | 0.057 | 12 | 0.864 | 14.5 | 1 | 110.5 | 0.06 | 93.5 | 0.168 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Liang, N.; Effati, M.; Nejat, G. Dances with Social Robots: A Pilot Study at Long-Term Care. Robotics 2022, 11, 96. https://doi.org/10.3390/robotics11050096
Li Y, Liang N, Effati M, Nejat G. Dances with Social Robots: A Pilot Study at Long-Term Care. Robotics. 2022; 11(5):96. https://doi.org/10.3390/robotics11050096
Chicago/Turabian StyleLi, Yizhu, Nan Liang, Meysam Effati, and Goldie Nejat. 2022. "Dances with Social Robots: A Pilot Study at Long-Term Care" Robotics 11, no. 5: 96. https://doi.org/10.3390/robotics11050096
APA StyleLi, Y., Liang, N., Effati, M., & Nejat, G. (2022). Dances with Social Robots: A Pilot Study at Long-Term Care. Robotics, 11(5), 96. https://doi.org/10.3390/robotics11050096