
Could Historical Mortality Data Predict Mortality Due to Unexpected Events?

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Construction of Mortality Models
2.2. Selection of the Appropriate Mortality Model
2.3. Selection of Mortality Data
3. Results
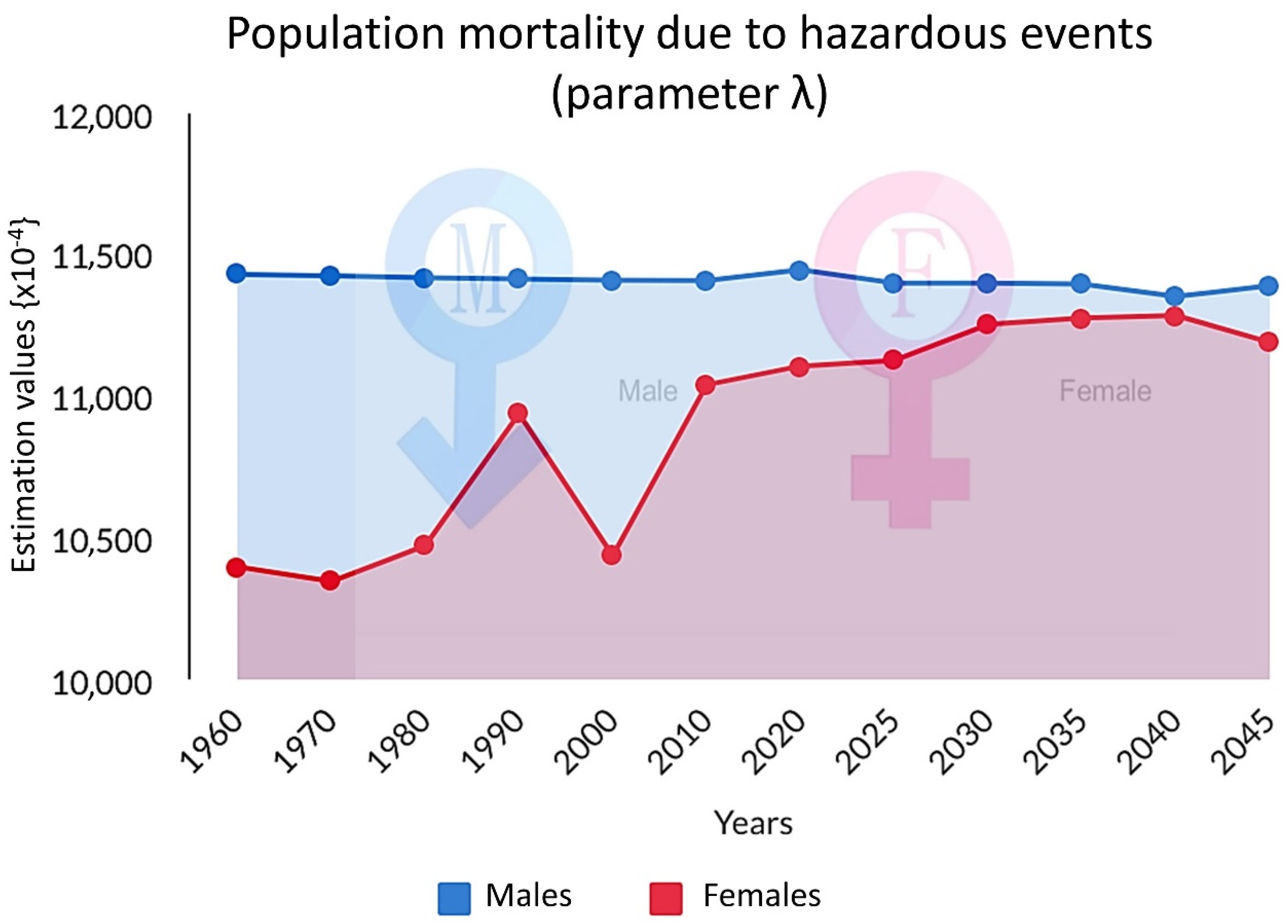
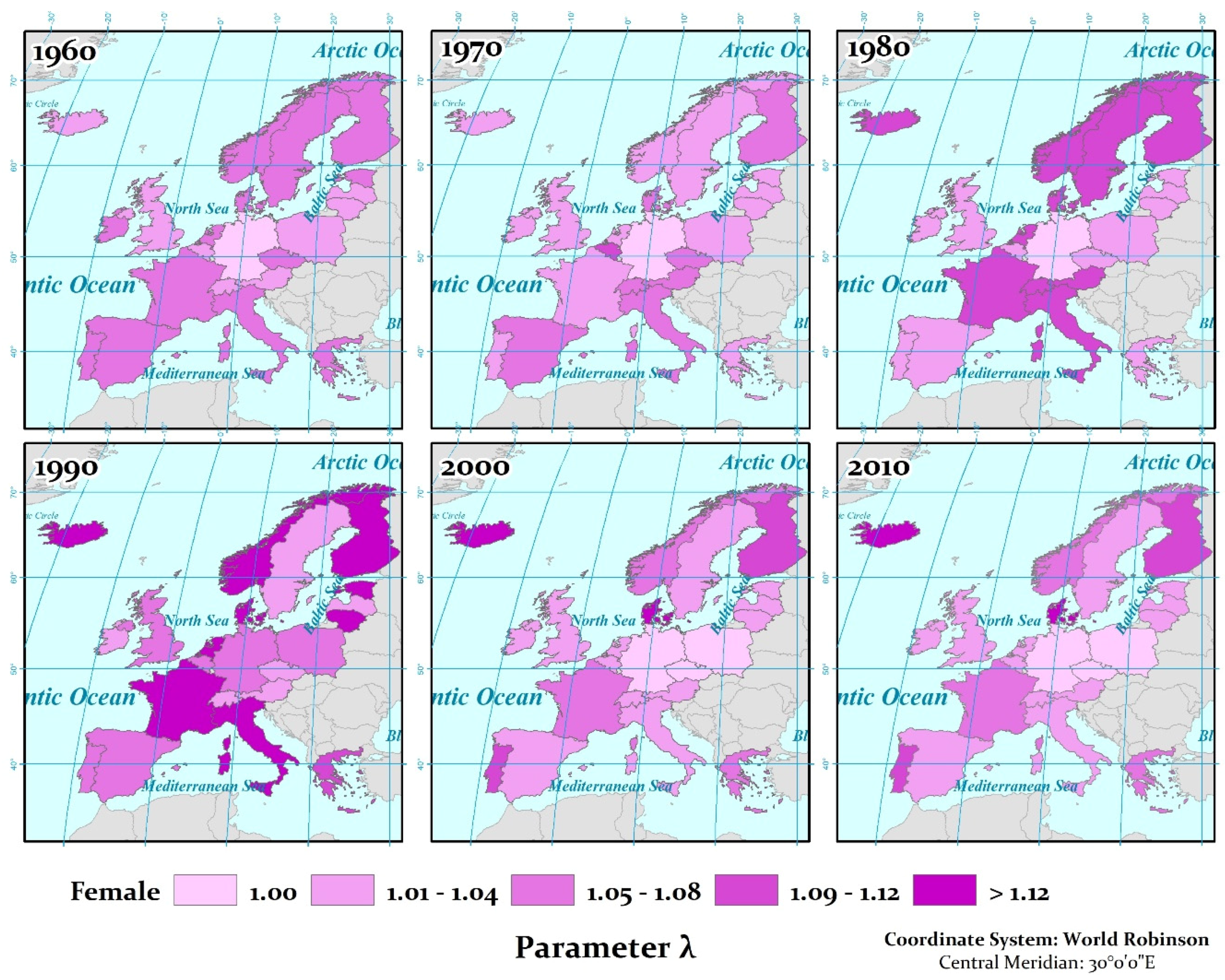
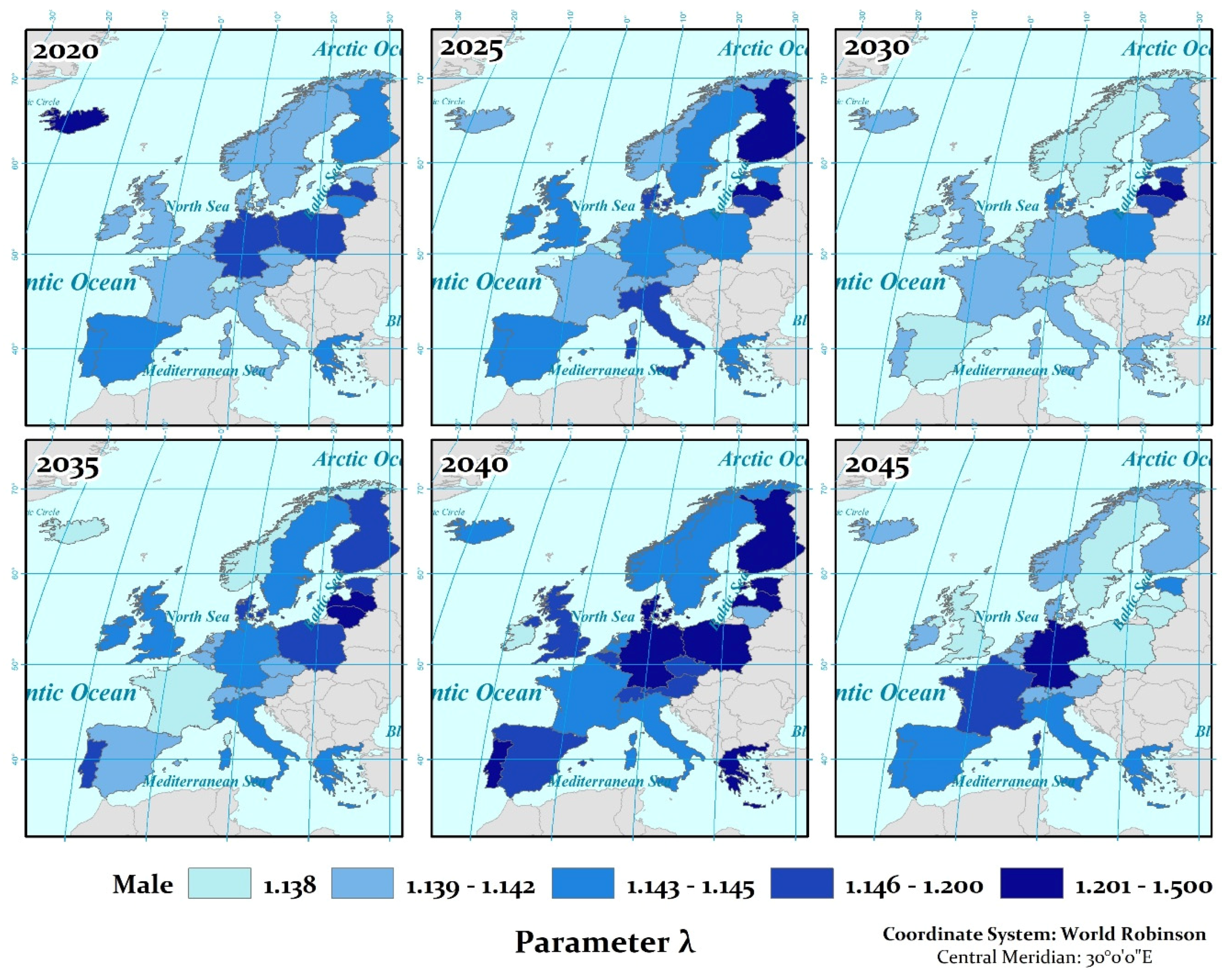
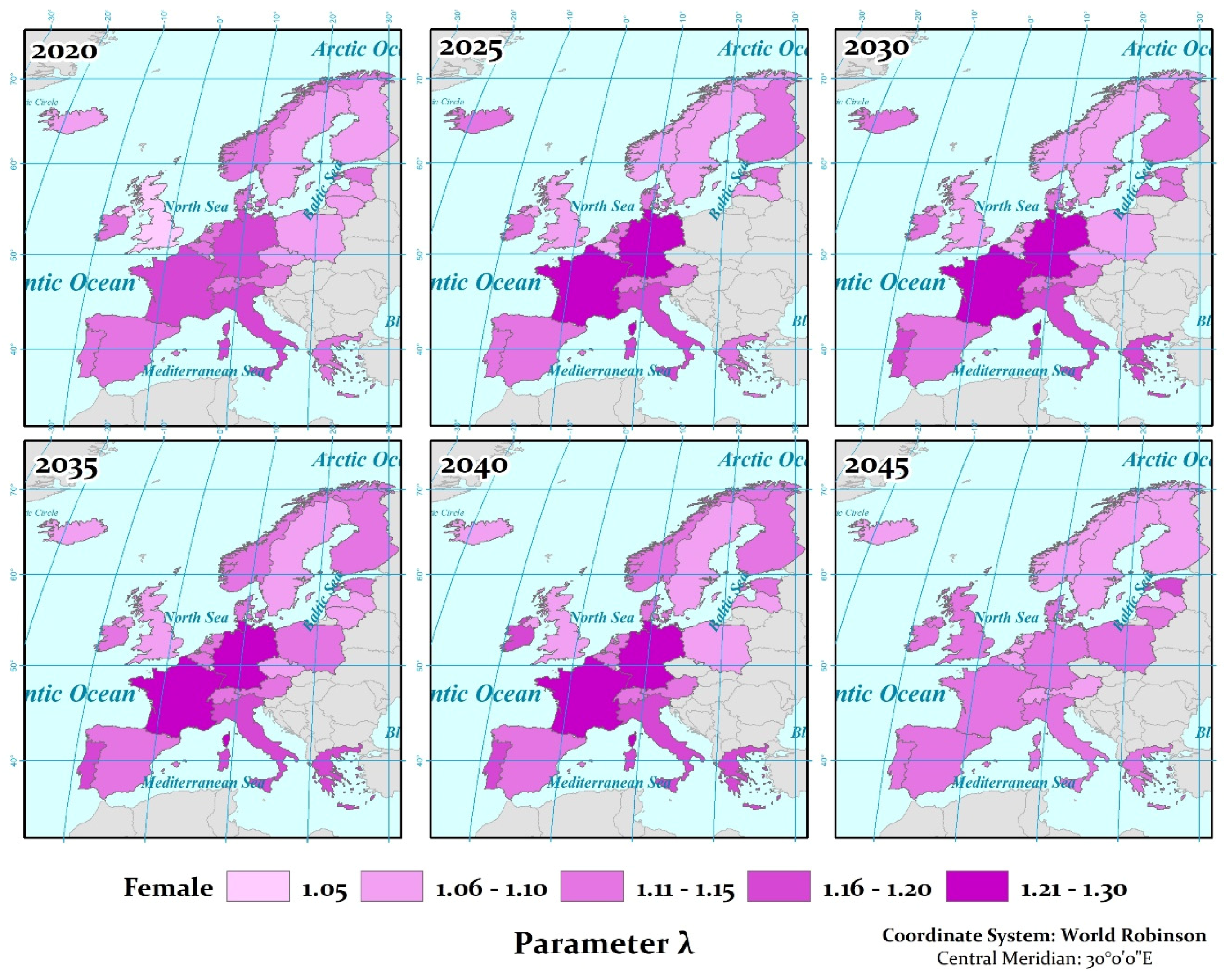
3.1. Non Age-Related Random Risk Factor for the Whole Population (Parameter λ)
3.2. Sensitivity Analysis of the Prediction Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Currie, I.D.; Durban, M.; Eilers, P.H. Smoothing and forecasting mortality rates. Stat. Model. 2004, 4, 279–298. [Google Scholar] [CrossRef]
- Gianquintieri, L.; Brovelli, M.A.; Pagliosa, A.; Dassi, G.; Brambilla, P.M.; Bonora, R.; Sechi, G.M.; Caiani, E.G. Mapping Spatiotemporal Diffusion of COVID-19 in Lombardy (Italy) on the Base of Emergency Medical Services Activities. ISPRS Int. J. Geo-Inf. 2020, 9, 639. [Google Scholar] [CrossRef]
- Huang, J.; Kwan, M.P.; Kan, Z.; Wong, M.S.; Kwok, C.Y.T.; Yu, X. Investigating the Relationship between the Built Environment and Relative Risk of COVID-19 in Hong Kong. ISPRS Int. J. Geo-Inf. 2020, 9, 624. [Google Scholar] [CrossRef]
- Niu, X.; Yue, Y.; Zhou, X.; Zhang, X. How Urban Factors Affect the Spatiotemporal Distribution of Infectious Diseases in Addition to Intercity Population Movement in China. ISPRS Int. J. Geo-Inf. 2020, 9, 615. [Google Scholar] [CrossRef]
- Antoniou, V.; Vassilakis, E.; Hatzaki, M. Is Crowdsourcing a Reliable Method for Mass Data Acquisition? The Case of COVID-19 Spread in Greece During Spring 2020. ISPRS Int. J. Geo-Inf. 2020, 9, 605. [Google Scholar] [CrossRef]
- Brito, P.L.; Kuffer, M.; Koeva, M.; Pedrassoli, J.C.; Wang, J.; Costa, F.; Freitas, A.D. The Spatial Dimension of COVID-19: The Potential of Earth Observation Data in Support of Slum Communities with Evidence from Brazil. ISPRS Int. J. Geo-Inf. 2020, 9, 557. [Google Scholar] [CrossRef]
- Liu, Y.; He, Z.; Zhou, X. Space-Time Variation and Spatial Differentiation of COVID-19 Confirmed Cases in Hubei Province Based on Extended GWR. ISPRS Int. J. Geo-Inf. 2020, 9, 536. [Google Scholar] [CrossRef]
- Peng, Z.; Wang, R.; Liu, L.; Wu, H. Exploring Urban Spatial Features of COVID-19 Transmission in Wuhan Based on Social Media Data. ISPRS Int. J. Geo-Inf. 2020, 9, 402. [Google Scholar] [CrossRef]
- Thakar, V. Unfolding Events in Space and Time: Geospatial Insights into COVID-19 Diffusion in Washington State during the Initial Stage of the Outbreak. ISPRS Int. J. Geo-Inf. 2020, 9, 382. [Google Scholar] [CrossRef]
- Wang, Z.; Yao, M.; Meng, C.; Claramunt, C. Risk Assessment of the Overseas Imported COVID-19 of Ocean-Going Ships Based on AIS and Infection Data. ISPRS Int. J. Geo-Inf. 2020, 9, 351. [Google Scholar] [CrossRef]
- Vatavali, F.; Gareiou, Z.; Kehagia, F.; Zervas, E. Impact of COVID-19 on Urban Everyday Life in Greece. Perceptions, Experiences and Practices of the Active Population. Sustainability 2020, 12, 9410. [Google Scholar] [CrossRef]
- Giannakis, E.; Hadjioannou, L.; Jimenez, C.; Papageorgiou, M.; Karonias, A.; Petrou, A. Economic Consequences of Coronavirus Disease (COVID-19) on Fisheries in the Eastern Mediterranean (Cyprus). Sustainability 2020, 12, 9406. [Google Scholar] [CrossRef]
- Telukdarie, A.; Munsamy, M.; Mohlala, P. Analysis of the Impact of COVID-19 on the Food and Beverages Manufacturing Sector. Sustainability 2020, 12, 9331. [Google Scholar] [CrossRef]
- Ballester, J.; Robine, J.M.; Herrmann, F.R.; Rodó, X. Effect of the Great Recession on regional mortality trends in Europe. Nat. Commun. 2019, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gompertz, B. XXIV. On the nature of the function expressive of the law of human mortality, and on a new mode of determining the value of life contingencies. In a letter to Francis Baily, Esq. FRS &c. Philos. Trans. R. Soc. Lond. 1825, 115, 513–583. [Google Scholar]
- Makeham, W.M. On the law of mortality and the construction of annuity tables. J. Inst. Actuar. 1860, 8, 301–310. [Google Scholar] [CrossRef] [Green Version]
- Andreopoulos, P.; Bersimis, G.F.; Tragaki, A.; Rovolis, A. Mortality modeling using probability distributions. APPLICATION in Greek mortality data. Commun. Stat. Theory Methods 2019, 48, 127–140. [Google Scholar] [CrossRef]
- European Statistical Authority (Eurostat), Population Data. Available online: https://ec.europa.eu/eurostat/ (accessed on 10 November 2020).
- HMD. Mortality and Population Data. Human Mortality Database. 2019. Available online: http://www.mortality.org/ (accessed on 10 November 2020).
- Gavrilov, L.A.; Gavrilova, N.S. The Biology of Life Span: A Quantitative Approach; Harwood Academic Publishers: Warsaw, Poland, 1991. [Google Scholar]
- London, D. Graduation, the Revision of Estimates; Actex Publications: Greenland, NH, USA, 1985. [Google Scholar]
- Haberman, S. Actuarial Methods, Encyclopedia of Biostatistics, 1st ed.; Armitage, P., Colton, T., Eds.; John Wiley & Sons: New York, NY, USA, 1998; pp. 37–49. [Google Scholar]
- Chalkias, C.; Papadopoulos, A.G.; Kalogeropoulos, K.; Tambalis, K.; Psarra, G.; Sidossis, L. Geographical heterogeneity of the relationship between childhood obesity and socio-environmental status: Empirical evidence from Athens, Greece. Appl. Geogr. 2013, 37, 34–43. [Google Scholar] [CrossRef]
- Myung, I.J. Tutorial on maximum likelihood estimation. J. Math. Psychol. 2003, 47, 90–100. [Google Scholar] [CrossRef]
- Amemiya, T. Advanced Econometrics; Harvard University Press: Cambridge, MA, USA, 1985. [Google Scholar]
- De Moivre, A. Annuities Upon Lives: Or, The Valuation of Annuities Upon Any Number of Lives; NewsBank Readex: Naples, FL, USA, 1725. [Google Scholar]
- Horiuchi, S.; Coale, A.J. Age patterns of mortality for older women: An analysis using the age-specific rate of mortality change with age. Math. Popul. Stud. 1990, 2, 245–267. [Google Scholar] [CrossRef]
- Elzhov, T.V.; Mullen, K.M.; Spiess, A.; Bolker, B. R interface to the Levenberg-Marquardt nonlinear least-squares algorithm found in MINPACK. Plus Support Bounds 2010, 1–2. [Google Scholar]
- Andreopoulos, P.; Polykretis, C.; Tragaki, A. Assessment and Mapping of Spatio-Temporal Variations in Human Mortality-Related Parameters at European Scale. ISPRS Int. J. Geo-Inf. 2020, 9, 547. [Google Scholar] [CrossRef]
- Jones, D.R. Mathematical Analysis of Mortality Dynamics; Technical Report; University of Liverpool: Liverpool, UK, 2013. [Google Scholar]
- Kim, D.; Saada, A. The social determinants of infant mortality and birth outcomes in Western developed nations: A cross-country systematic review. Int. J. Environ. Res. Public Health 2013, 10, 2296–2335. [Google Scholar] [CrossRef] [Green Version]
- Kalogeropoulos, K. The Geographical Aspect of the Geodata of the National Population Censuses. Mapping—Creation of Modern Spatial Data Infrastructures with the Use of Geoinformatics. Ph.D. Thesis, Department of Geography, Harokopio University, Athens, Greece, 2020. Available online: http://estia.hua.gr/browse/23211 (accessed on 27 April 2021).
- Lenart, P.; Kuruczova, D.; Joshi, P.K.; Bienertová-Vašků, J. Male mortality rates mirror mortality rates of older females. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zografos, K.; Balakrishnan, N. On families of beta-and generalized gamma-generated distributions and associated inference. Stat. Methodol. 2009, 6, 344–362. [Google Scholar] [CrossRef]
- Kalogirou, S.; Tsimbos, C.; Verropoulou, G.; Kotsifakis, G. Regional mortality differentials in Greece by selected causes of death: 2006–2008. J. Maps 2012, 8, 354–360. [Google Scholar] [CrossRef]
- Drevenstedt, G.L.; Crimmins, E.M.; Vasunilashorn, S.; Finch, C.E. The rise and fall of excess male infant mortality. Proc. Natl. Acad. Sci. USA 2008, 105, 5016–5021. [Google Scholar] [CrossRef] [Green Version]
- Organisation for Economic Co-Operation and Development (OECD). Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Wasserman, D.; Cheng, Q.I.; Jiang, G.X. Global suicide rates among young people aged 15–19. World Psychiatry 2005, 4, 114. [Google Scholar] [PubMed]
- Oksuzyan, A.; Juel, K.; Vaupel, J.W.; Christensen, K. Men: Good health and high mortality. Sex differences in health and aging. Aging Clin. Exp. Res. 2008, 20, 91–102. [Google Scholar] [CrossRef] [Green Version]
- Laliotis, I.; Ioannidis, J.P.; Stavropoulou, C. Total and cause-specific mortality before and after the onset of the Greek economic crisis: An interrupted time-series analysis. Lancet Public Health 2016, 1, e56–e65. [Google Scholar] [CrossRef] [Green Version]
- Lafaut, D.; Vandenheede, H.; Surkyn, J.; Coene, G. Counting the non-existing: Causes of death of undocumented migrants in Brussels-Capital Region (Belgium), 2005–2010. Arch. Public Health 2019, 77, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domnich, A.; Panatto, D.; Gasparini, R.; Amicizia, D. The “healthy immigrant” effect: Does it exist in Europe today? Ital. J. Public Health 2012, 9, e7532. [Google Scholar]
- Ugarte, M.D.; Goicoa, T.; Etxeberria, J.; Militino, A.F. Projections of cancer mortality risks using spatio-temporal P-spline models. Stat. Methods Med Res. 2012, 21, 545–560. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Range | Min | Max | Mean | Std. Deviation | ||
|---|---|---|---|---|---|---|
| 1960 | 0.2700 | 1.0000 | 1.2700 | 1.1445 | 0.0116 | 0.0542 |
| 1970 | 0.2900 | 1.0000 | 1.2900 | 1.1418 | 0.0140 | 0.0655 |
| 1980 | 0.4900 | 1.0000 | 1.4900 | 1.1418 | 0.0273 | 0.1281 |
| 1990 | 0.4700 | 1.0100 | 1.4800 | 1.1414 | 0.0243 | 0.1141 |
| 2000 | 0.0000 | 1.1400 | 1.1400 | 1.1400 | 0.0000 | 0.0000 |
| 2010 | 0.0000 | 1.1400 | 1.1400 | 1.1400 | 0.0000 | 0.0000 |
| 2015 | 0.0000 | 1.1400 | 1.1400 | 1.1400 | 0.0000 | 0.0000 |
| 2020 | 0.0800 | 1.1400 | 1.2200 | 1.1450 | 0.0036 | 0.0171 |
| 2025 | 0.0000 | 1.1400 | 1.1400 | 1.1400 | 0.0000 | 0.0000 |
| 2030 | 0.0100 | 1.1400 | 1.1500 | 1.1405 | 0.0005 | 0.0021 |
| 2035 | 0.0000 | 1.1400 | 1.1400 | 1.1400 | 0.0000 | 0.0000 |
| 2040 | 0.0300 | 1.1100 | 1.1400 | 1.1350 | 0.0017 | 0.0080 |
| 2045 | 0.3600 | 1.0200 | 1.3800 | 1.1391 | 0.0159 | 0.0746 |
| Range | Min | Max | Mean | Std. Deviation | ||
|---|---|---|---|---|---|---|
| 1960 | 0.0743 | 1.0000 | 1.0743 | 1.0391 | 0.0047 | 0.0221 |
| 1970 | 0.0876 | 1.0000 | 1.0876 | 1.0348 | 0.0054 | 0.0254 |
| 1980 | 0.1114 | 1.0000 | 1.1114 | 1.0525 | 0.0098 | 0.0460 |
| 1990 | 0.2364 | 1.0140 | 1.2504 | 1.0937 | 0.0147 | 0.0690 |
| 2000 | 0.1309 | 1.0000 | 1.1309 | 1.0446 | 0.0077 | 0.0361 |
| 2010 | 0.1897 | 1.0000 | 1.1897 | 1.1041 | 0.0103 | 0.0482 |
| 2015 | 0.1984 | 1.0095 | 1.2079 | 1.1001 | 0.0102 | 0.0479 |
| 2020 | 0.1459 | 1.0478 | 1.1937 | 1.1104 | 0.0075 | 0.0353 |
| 2025 | 0.2032 | 1.0101 | 1.2132 | 1.1105 | 0.0110 | 0.0518 |
| 2030 | 0.2122 | 1.0163 | 1.2285 | 1.1247 | 0.0109 | 0.0512 |
| 2035 | 0.1941 | 1.0516 | 1.2457 | 1.1265 | 0.0101 | 0.0474 |
| 2040 | 0.2438 | 1.0182 | 1.2620 | 1.1242 | 0.0121 | 0.0565 |
| 2045 | 0.1493 | 1.0104 | 1.1597 | 1.1185 | 0.0066 | 0.0309 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreopoulos, P.; Kalogeropoulos, K.; Tragaki, A.; Stathopoulos, N. Could Historical Mortality Data Predict Mortality Due to Unexpected Events? ISPRS Int. J. Geo-Inf. 2021, 10, 283. https://doi.org/10.3390/ijgi10050283
Andreopoulos P, Kalogeropoulos K, Tragaki A, Stathopoulos N. Could Historical Mortality Data Predict Mortality Due to Unexpected Events? ISPRS International Journal of Geo-Information. 2021; 10(5):283. https://doi.org/10.3390/ijgi10050283
Chicago/Turabian StyleAndreopoulos, Panagiotis, Kleomenis Kalogeropoulos, Alexandra Tragaki, and Nikolaos Stathopoulos. 2021. "Could Historical Mortality Data Predict Mortality Due to Unexpected Events?" ISPRS International Journal of Geo-Information 10, no. 5: 283. https://doi.org/10.3390/ijgi10050283
APA StyleAndreopoulos, P., Kalogeropoulos, K., Tragaki, A., & Stathopoulos, N. (2021). Could Historical Mortality Data Predict Mortality Due to Unexpected Events? ISPRS International Journal of Geo-Information, 10(5), 283. https://doi.org/10.3390/ijgi10050283