
Geospatial Technology: A Tool to Aid in the Elimination of Malaria in Bangladesh


Abstract
:1. Introduction

2. Materials and Methods
2.1. Study Area
2.2. Data Search
Box 1. Literature search for data on the use of geospatial technology to study malaria in Bangladesh.
- Period searched: through to June 2014
- Source: PubMed databases
- Search terms: (“Bangladesh”) AND (“malaria”)
- Articles found: 218
- Inclusion criterion: Referral to any article using GIS/RS/GPS to study malaria in Bangladesh

{kind=link}
| Geospatial Application | |||||||
|---|---|---|---|---|---|---|---|
| Study Area | Ref. # | Study Year | Sample Size | GIS | GPS | RS | Findings of the Study |
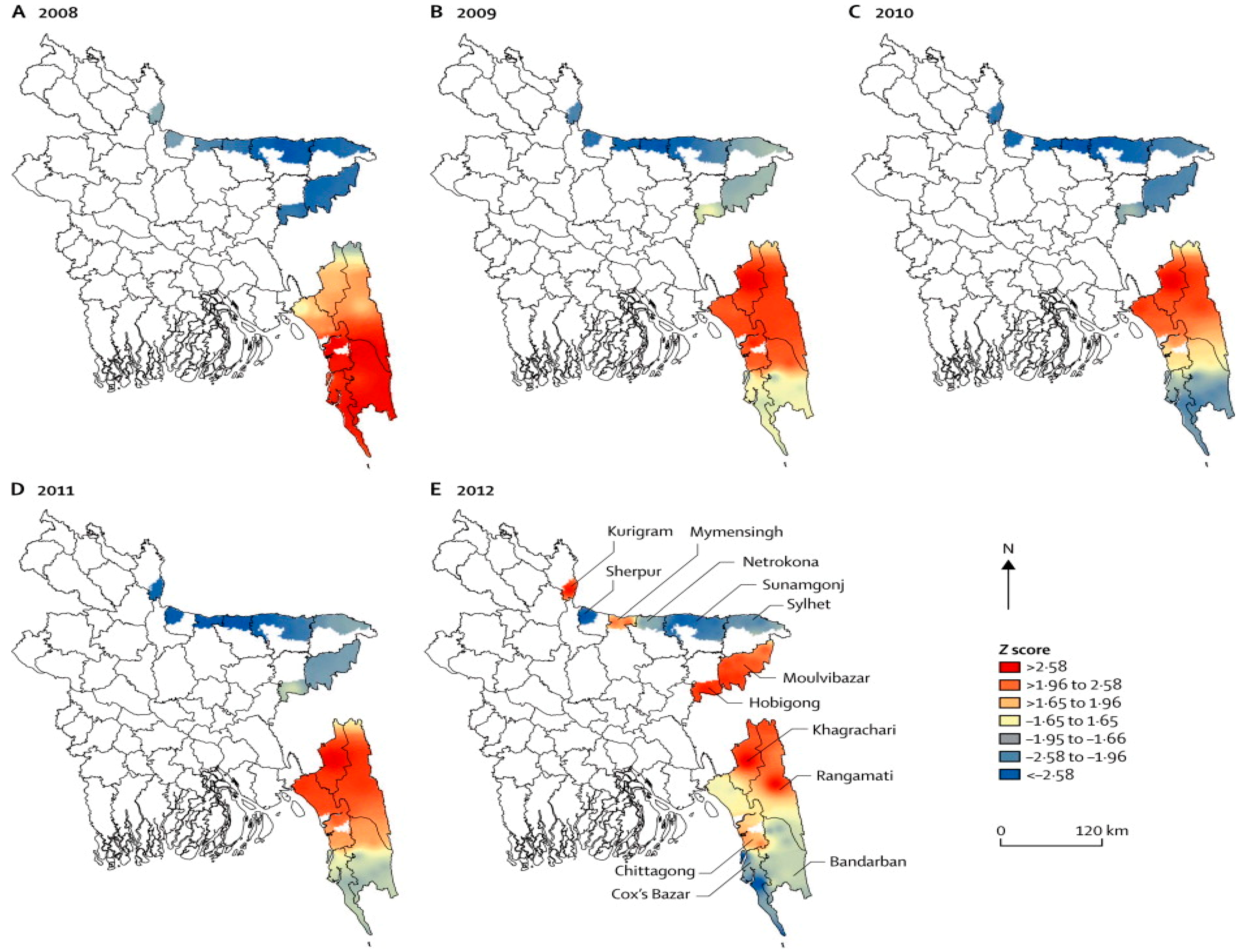
| 13 districts | [1] | 2008–2012 | - | √ | Malaria mapping of Bangladesh from 2008 to 2012 showing a decrease in the country’s prevalence rates (65%). | ||
| 13 districts | [2] | 2007 | - | √ | Findings reported statistically significant positive associations between the incidence of reported P. vivax and P. falciparum cases and rainfall and maximum temperature. | ||
| Rangamati | [4] | 2009 | 5322 | √ | √ | Housing materials, household densities, education levels, and proximity to the regional urban center, were found to be effective predictors of treatment-seeking preferences for malaria. | |
| 13 districts | [8] | 2007 | 9750 | √ | √ | √ | Bayesian modeling found statistically significant correlation between malaria prevalence and rainfall, temperature, and elevation as major factors influencing spatiotemporal patterns. |
| Khagrachari | [13] | 2007 | 750 | √ | √ | √ | Risk mapping used to predict areas of high and low malaria prevalence based on risk factors that included age and location of fragmented forests. |
| Khagrachari | [14] | 2007 | 750 | √ | √ | √ | Proximity (3 km) to water proved significant as a risk factor for malaria. |
| Rangamati | [15] | 2009 | 1400 | √ | √ | √ | Hot-spot clustering of cases with statistically significant risk factors between malaria positivity and ethnicity, forest cover, altitude, treatment preference, floor construction, and household density. |
| Rangamati | [16] | 2009–2010 | 1634 | √ | √ | √ | Identified malaria hotspots and with risk factors of low bed net ratio, home construction material, and high density of homes. |
| Rangamati | [17] | 2009 | 5322 | √ | √ | Mapping of treatment seeking behaviors showed place of preference for malaria treatment were government health facilities if it was located 2 km from government health facilities preferred drug vendors. | |
| Bandarban | [18] | 2010–2012 | 24,074 | √ | √ | Risk factors for malaria were higher among jhum cultivators than non-cultivators living in the same household. | |
| All Bangladesh | [19] | 1992–2001 | - | √ | VCI and TCI were strong predictors of malaria risk in Bangladesh. | ||
| Bandarban | [20] | 1992–2004 | - | √ | Estimated epidemic risks can be achieved using VHI and high summer TCI. | ||
| Bandarban | [21] | 2009–2010 | 20,563 | √ | √ | Mapping of symptomatic & asymptomatic cases with high clustering within CHT; 80% of cases occurred during the rainy season. | |
| Rangamati | [22] | 2009 | 1400 | √ | √ | Age, ethnicity, proximity to forest, household density, and elevation were significant risk factors for malaria with 44.12% households living in areas with ≥10% prevalence rates. | |
| 13 districts | [23] | 2007 | 9750 | √ | √ | Malaria risk mapping of CHT with unequal distribution of prevalence rates -Khagrachari (15.25%), Bandarban (10.97%), and Rangamati (7.42%). | |
| Bandarban | [24] | 2010–2013 | 1753 | √ | √ | Higher risk of P. falciparum infection in pregnant women than other adults with asymptomatic infections. | |
| Bandarban | [25] | 2009–2012 | 4782 | √ | √ | Cases were geographically limited to hotspots with 80% infections occurring in one third of the population; incidence rates were highly seasonal with 85.8% of cases during rainy season (May–October). | |
3. Results and Discussion
3.1. Results
3.2. Discussion
| Geospatial Technology | Recommended Applications |
|---|---|
| GIS | Create malaria risk map at the lowest administrative level and update malaria maps each month. |
| GPS | Locate hospitals, health facilities, clinics, and households to create malaria information systems for improved mapping of risk areas. |
| Mobile Telecommunication Systems | Target interventions using surveillance data, satellite imagery, and mobile phone call records to improve coordination of services. |
| Spatiotemporal Cluster Detection | Analyze malaria cases in each month, detect spatio-temporal clustering, and locate hotspots. |
| Geostatistics | Detect spatial auto-correlation, prediction, and modeling for cost effective interventions. |
| Ecological Niche Models | Prepare malaria vector distribution maps, ecological suitability, predict vector distribution maps to locate vector-breeding areas and determine the indoor residual spraying strategies. |
| Bayesian methods | Interpolate, predict, and develop models using multiple malaria risk factors. |
| Spatially Explicit Mathematical Models | Create hierarchical models, hierarchical linear regression models, and mixed linear regressions to predict current and future malaria risk scenarios. |
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Haque, U.; Overgaard, H.J.; Clements, A.C.; Norris, D.E.; Islam, N.; Karim, J.; Roy, S.; Haque, W.; Kabir, M.; Smith, D.L.; et al. Malaria burden and control in Bangladesh and prospects for elimination: An epidemiological and economic assessment. Lancet Glob. Health 2014, 2, e98–e105. [Google Scholar] [CrossRef] [PubMed]
- Reid, H.L.; Haque, U.; Roy, S.; Islam, N.; Clements, A.C. Characterizing the spatial and temporal variation of malaria incidence in Bangladesh, 2007. Malar. J. 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- National Malaria Control Program About NMCP in Bangladesh. Available online: http://www.Nmcp.Info/nmcp.Aspx (accessed on 9 June 2014).
- Haque, U.; Hashizume, M.; Sunahara, T.; Hossain, S.; Ahmed, S.M.; Haque, R.; Yamamoto, T.; Glass, G.E. Progress and challenges to control malaria in a remote area of Chittagong hill tracts, Bangladesh. Malar. J. 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- What is a GIS? Available online: http://www.Volusia.Org/gis/whatsgis.Htm (accessed on 11 September 2014).
- GPS. Available online: http://www.Gps.Gov/systems/gps/ (accessed on 28 May 2014).
- Bautista, C.T.; Chan, A.S.; Ryan, J.R.; Calampa, C.; Roper, M.H.; Hightower, A.W.; Magill, A.J. Epidemiology and spatial analysis of malaria in the northern Peruvian Amazon. Am. J. Trop. Med. Hyg. 2006, 75, 1216–1222. [Google Scholar] [PubMed]
- Reid, H.; Haque, U.; Clements, A.C.A.; Tatem, A.J.; Vallely, A.; Ahmed, S.M.; Islam, A.; Haque, R. Mapping malaria risk in Bangladesh using bayesian geostatistical models. Am. J. Trop. Med. Hyg. 2010, 83, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.S.; Chakma, S.; Khan, W.A.; Glass, G.E.; Mohon, A.N.; Elahi, R.; Norris, L.C.; Podder, M.P.; Ahmed, S.; Haque, R.; et al. Diversity of anopheline species and their plasmodium infection status in rural Bandarban, Bangladesh. Parasit. Vector 2012, 5. [Google Scholar] [CrossRef]
- Khan, A.Q.; Talibi, S.A. Epidemiological assessment of malaria transmission in an endemic area of East Pakistan and the significance of congenital immunity. Bull. World Health Organ. 1972, 46, 783–792. [Google Scholar] [PubMed]
- Elias, M.; Dewan, R.; Ahmed, R. Vectors of malaria in Bangladesh. J. Prev. Soc. Med. 1982, 1, 20–28. [Google Scholar]
- Alam, M.; Khan, M.; Chaudhury, N.; Deloer, S.; Nazib, F.; Bangali, A.; Haque, R. Prevalence of anopheline species and their plasmodium infection status in epidemic-prone border areas of Bangladesh. Malar. J. 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Magalhaes, R.J.S.; Reid, H.L.; Clements, A.C.A.; Ahmed, S.M.; Islam, A.; Yamamoto, T.; Haque, R.; Glass, G.E. Spatial prediction of malaria prevalence in an endemic area of Bangladesh. Malar. J. 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Huda, M.; Hossain, A.; Ahmed, S.M.; Moniruzzaman, M.; Haque, R. Spatial malaria epidemiology in Bangladeshi highlands. Malar. J. 2009, 8. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Sunahara, T.; Hashizume, M.; Shields, T.; Yamamoto, T.; Haque, R.; Glass, G.E. Malaria prevalence, risk factors and spatial distribution in a hilly forest area of Bangladesh. PLoS One 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Glass, G.E.; Bomblies, A.; Hashizume, M.; Mitra, D.; Noman, N.; Haque, W.; Kabir, M.M.; Yamamoto, T.; Overgaard, H.J. Risk factors associated with clinical malaria episodes in Bangladesh: A longitudinal study. Am. J. Trop. Med. Hyg. 2013, 88, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Scott, L.M.; Hashizume, M.; Fisher, E.; Haque, R.; Yamamoto, T.; Glass, G.E. Modelling malaria treatment practices in Bangladesh using spatial statistics. Malar. J. 2012, 11. [Google Scholar] [CrossRef] [PubMed]
- Galagan, S.R.; Prue, C.S.; Khyang, J.; Khan, W.A.; Ahmed, S.; Ram, M.; Alam, M.S.; Haq, M.Z.; Akter, J.; Streatfield, P.K.; et al. The practice of jhum cultivation and its relationship to plasmodium falciparum infection in the Chittagong hill districts of Bangladesh. Am. J. Trop. Med. Hyg. 2014, 91, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Kogan, F.; Roytman, L. Short report: Analysis of malaria cases in Bangladesh with remote sensing data. Am. J. Trop. Med. Hyg. 2006, 74, 17–19. [Google Scholar] [PubMed]
- Rahman, A.; Krakauer, N.; Roytman, L.; Goldberg, M.; Kogan, F. Application of advanced very high resolution radiometer (AVHRR)-based vegetation health indices for estimation of malaria cases. Am. J. Trop. Med. Hyg. 2010, 82, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.A.; Sack, D.A.; Ahmed, S.; Prue, C.S.; Alam, M.S.; Haque, R.; Khyang, J.; Ram, M.; Akter, J.; Nyunt, M.M.; et al. Mapping hypoendemic, seasonal malaria in rural Bandarban, Bangladesh: A prospective surveillance. Malar. J. 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Soares Magalhaes, R.J.; Mitra, D.; Kolivras, K.N.; Schmidt, W.P.; Haque, R.; Glass, G.E. The role of age, ethnicity and environmental factors in modulating malaria risk in Rajasthali, Bangladesh. Malar. J. 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Ahmed, S.M.; Hossain, S.; Huda, M.; Hossain, A.; Alam, M.S.; Mondal, D.; Khan, W.A.; Khalequzzaman, M.; Haque, R. Malaria prevalence in endemic districts of Bangladesh. PLoS One 2009, 4, e6737. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.A.; Galagan, S.R.; Prue, C.S.; Khyang, J.; Ahmed, S.; Ram, M.; Alam, M.S.; Haq, M.Z.; Akter, J.; Glass, G.; et al. Asymptomatic plasmodium falciparum malaria in pregnant women in the Chittagong hill districts of Bangladesh. PLoS One 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Glass, G.; Alam, M.S.; Khan, W.A.; Sack, D.A.; Sullivan, D.J. Spatial clustering of malaria cases during low-transmission season in Kuhalong, Bangladesh. In Proceedings of the 13th Ascon Conference, Dhaka, Bangladesh, 28 March 2011.
- Clement, A.C.; Reid, H.; Kelly, G.; Hay, S. Further shrinking the malaria map: How can geospatial science help to achieve malaria elimination? Lancet Infect. Dis. 2013, 13, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Tatem, A.J.; Huang, Z.; Narib, C.; Kumar, U.; Kandula, D.; Pindolia, D.K.; Smith, D.L.; Cohen, J.M.; Graupe, B.; Uusiku, P.; et al. Integrating rapid risk mapping and mobile phone call record data for strategic malaria elimination planning. Malar. J. 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Prue, C.S.; Shannon, K.L.; Khyang, J.; Edwards, L.J.; Ahmed, S.; Ram, M.; Shields, T.; Hossain, M.S.; Glass, G.E.; Nyunt, M.M.; et al. Mobile phones improve case detection and management of malaria in rural Bangladesh. Malar. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Haque, U.; Glass, G.E.; Haque, W.; Islam, N.; Roy, S.; Karim, J.; Noedl, H. Antimalarial drug resistance in Bangladesh, 1996–2012. Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.S.; Chakma, S.; Al-Amin, H.M.; Elahi, R.; Mohon, A.N.; Khan, W.A.; Haque, R.; Glass, G.E.; Sack, D.A.; Sullivan, D.J.; et al. Role of artificial containers as breeding sites for anopheline mosquitoes in Malaria hypo endemic areas of rural Bandarban, Bangladesh: Evidence form a baseline survey. In Proceedings of the Astmh Conference 2012, Atlanta, GA, USA, 11–15 November 2012.
- Stoops, C.A.; Gionar, Y.R.; Shinta; Sismadi, P.; Rachmat, A.; Elyazar, I.F.; Sukowati, S. Remotely-sensed land use patterns and the presence of anopheles larvae (diptera: Culicidae) in Sukabumi, West Java, Indonesia. J. Vector. Ecol. 2008, 33, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Nmor, J.C.; Sunahara, T.; Goto, K.; Futami, K.; Sonye, G.; Akweywa, P.; Dida, G.; Minakawa, N. Topographic models for predicting malaria vector breeding habitats: Potential tools for vector control managers. Parasit. Vector 2013, 6. [Google Scholar] [CrossRef]
- Kamuliwo, M.; Chanda, E.; Haque, U.; Mwanza-Ingwe, M.; Sikaala, C.; Katebe-Sakala, C.; Mukonka, V.M.; Norris, D.E.; Smith, D.L.; Glass, G.E.; et al. The changing burden of malaria and association with vector control interventions in Zambia using district-level surveillance data, 2006–2011. Malar. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Mukonka, V.M.; Chanda, E.; Haque, U.; Kamuliwo, M.; Mushinge, G.; Chileshe, J.; Chibwe, K.A.; Norris, D.E.; Mulenga, M.; Chaponda, M.; et al. High burden of malaria following scale-up of control interventions in Nchelenge district, Luapula province, Zambia. Malar. J. 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Chanda, E.; Mukonka, V.M.; Kamuliwo, M.; Macdonald, M.B.; Haque, U. Operational scale entomological intervention for malaria control: Strategies, achievements and challenges in Zambia. Malar. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Chanda, E.; Govere, J.M.; Macdonald, M.B.; Lako, R.L.; Haque, U.; Baba, S.P.; Mnzava, A. Integrated vector management: A critical strategy for combating vector-borne diseases in South Sudan. Malar. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Simon, C.; Moakofhi, K.; Mosweunyane, T.; Jibril, H.B.; Nkomo, B.; Motlaleng, M.; Ntebela, D.S.; Chanda, E.; Haque, U. Malaria control in Botswana, 2008–2012: The path towards elimination. Malar. J. 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Galagan, S.; Scobie, H.; Khyang, J.; Prue, C.S.; Khan, W.A.; Ram, M.; Alam, M.S.; Haq, M.Z.; Akter, J.; et al. Malaria hotspots drive hypoendemic transmission in the Chittagong hill districts of Bangladesh. PLoS One 2013, 8. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirk, K.E.; Haq, M.Z.; Alam, M.S.; Haque, U. Geospatial Technology: A Tool to Aid in the Elimination of Malaria in Bangladesh. ISPRS Int. J. Geo-Inf. 2015, 4, 47-58. https://doi.org/10.3390/ijgi4010047
Kirk KE, Haq MZ, Alam MS, Haque U. Geospatial Technology: A Tool to Aid in the Elimination of Malaria in Bangladesh. ISPRS International Journal of Geo-Information. 2015; 4(1):47-58. https://doi.org/10.3390/ijgi4010047
Chicago/Turabian StyleKirk, Karen E., M. Zahirul Haq, Mohammad Shafiul Alam, and Ubydul Haque. 2015. "Geospatial Technology: A Tool to Aid in the Elimination of Malaria in Bangladesh" ISPRS International Journal of Geo-Information 4, no. 1: 47-58. https://doi.org/10.3390/ijgi4010047
APA StyleKirk, K. E., Haq, M. Z., Alam, M. S., & Haque, U. (2015). Geospatial Technology: A Tool to Aid in the Elimination of Malaria in Bangladesh. ISPRS International Journal of Geo-Information, 4(1), 47-58. https://doi.org/10.3390/ijgi4010047