1. Introduction
Global efforts to end the tuberculosis (TB) epidemic by 2030 (Sustainable Development Goal 3.3) through improved TB case detection and treatment have not been effective to significantly reduce the global burden of the TB epidemic. TB prevalence surveys have shown that only 61% of the estimated number of incident TB patients are detected and subsequently reported by national TB programs (NTPs) globally [
1]. This finding has led the global TB community to prioritize the development of interventions and monitoring tools to improve TB case detection in order to reach the SDG goal 3.3 to end the global TB epidemic by 2030 [
1,
2].
The main global indicator used to monitor progress in ending TB by 2030 is the TB incidence rate (number of new TB cases per 100,000 population per year). TB incidence rates are classified as a TIER 1 indicator by the UN SDG statistics division. This means that it is regarded to be: “conceptually clear, has an internationally established methodology and standards are available, and data are regularly produced by countries for at least 50 percent of countries and of the population in every region where the indicator is relevant…” [
2]. As TB incidence rates cannot be directly measured from routine surveillance data, indirect methods are commonly used and recommended to estimate national TB incidence rates. In countries where TB prevalence studies have been conducted, the gap between the reported rates of TB as compared to the actual burden can be estimated [
3]. Where recent TB prevalence results are not available, alternative methods utilizing TB case notification rates as a proxy to estimate TB incidence are used [
4,
5]. Case notification rates (CNR) are defined as the total number of people with TB who have been diagnosed with TB and are routinely reported to national health authorities per 100,000 population per year. TB notifications are routinely reported and monitored by National TB Programs (NTP). It is generally recognized that the number of TB patients reported to NTPs is highly influenced by the coverage of, and access to health services and the quality of clinical and diagnostic conduct. The ability of people with TB to access TB services and obtain a proper diagnosis is highly variable, as it depends on social, cultural, economic and programmatic factors which influence the coverage, cost and quality of TB services available to target populations [
6,
7,
8]. Therefore, estimating the gap between TB incidence and TB case notification is a key step to determine where people with TB are missed by health systems, as well as to estimate TB incidence, which is required to monitor progress towards the 2030 SDG target to end the global epidemic of TB.
Using information of TB risk, access to TB services and TB case detection is required to generate insight into where and why people with TB are “missed”, either because they are not diagnosed, or diagnosed but not reported within NTP surveillance systems. NTPs usually rely on nationally aggregated surveillance statistics to assess program performance and effectiveness, which are used to strategize future interventions. Using such a blanket approach to implement TB interventions ignores the existence of subnational variations in the TB epidemic and programmatic responses. A growing body of literature has now shown how targeted interventions can significantly improve the timely detection and treatment of TB [
8,
9,
10,
11,
12,
13]. The routine analysis of subnational data is expected to become a crucial step to identify and locate TB transmission hot spots and links these to geographic patterns of key populations at risk of TB, TB diagnostic and treatment service delivery [
14].
To plan and allocate resources efficiently and effectively, it is imperative for NTPs to integrate, map and analyze data from a variety of sources to inform locally tailored approaches. A robust and generally applicable data analysis framework is needed to evaluate the use of TB notification data to monitor progress towards SDG targets across various epidemic and programmatic contexts. In this paper, a new analytical framework was proposed to evaluate the effects of TB risk factors and program response on TB case detection and reporting. This framework was developed as part of a larger health system strengthening approach called: Mapping and Analysis for Tailored disease Control and Health system strengthening (MATCH) [
15]. Using a case study from Bangladesh, the MATCH analytical framework is applied to detect subnational variations in TB notification rates and to evaluate the effects of TB risks and program efforts to detect and report TB cases across the country. The outcomes are then used to assess the validity of using case notification data as a proxy for TB incidence accounting for the effects of access to healthcare, diagnostic performance and program quality.
2. Materials and Methods
2.1. MATCH Analytical Framework for TB
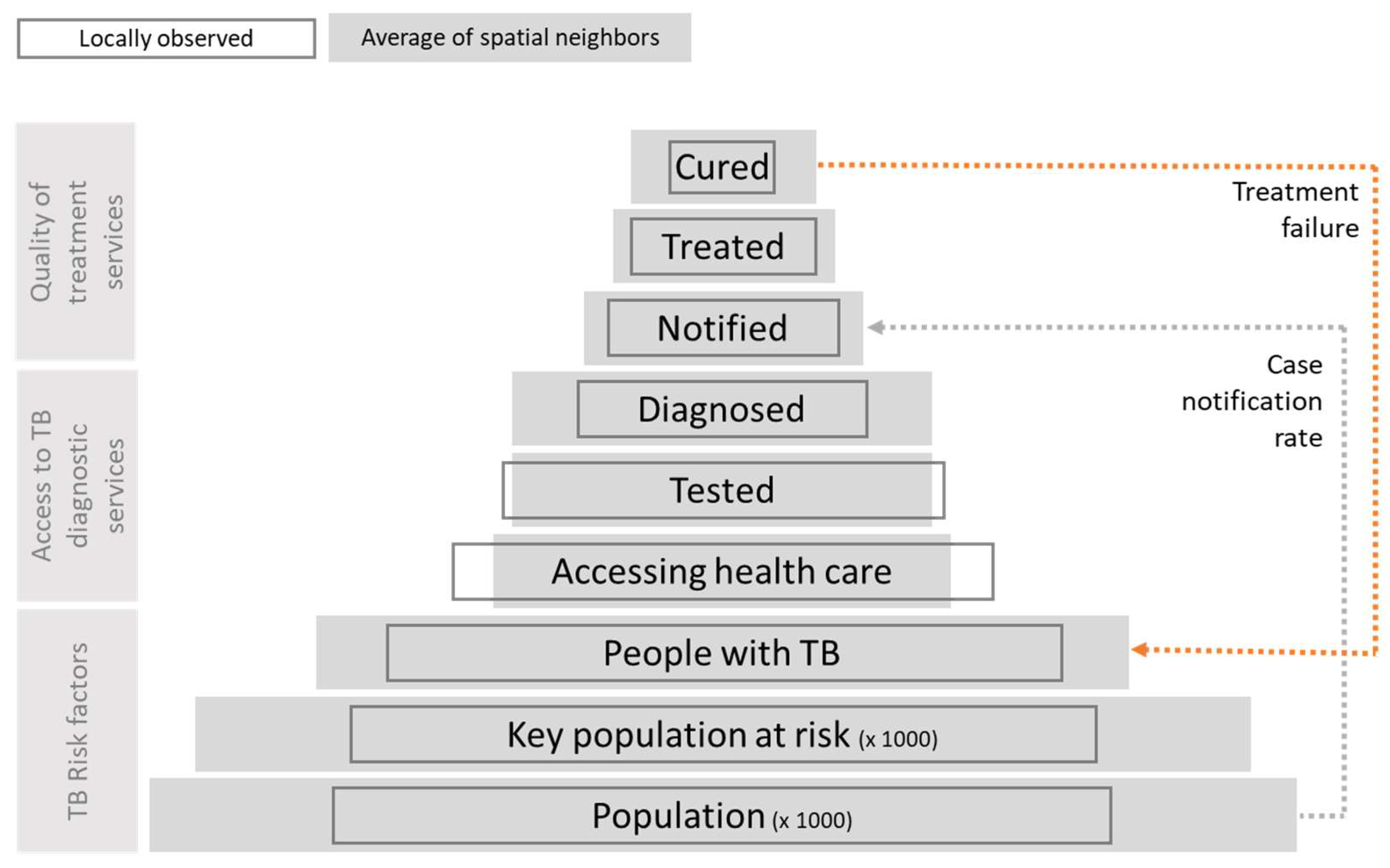
A common model used in the monitoring and evaluation of TB programs is the patient pathway pyramid as shown in
Figure 1. This model shows how the number of persons progressing along each stage of the pathway decreases from those at risk of TB, through diagnoses and treatment, to those being cured. The effectiveness of the program is then assessed by analyzing the proportions of drop-out along the pyramid, indicative of gaps in service delivery. The MATCH approach extends this model by assessing how progression along the pathway within a given subnational area correlates (or deviates), from its surroundings (
Figure 1 open and grey rectangles respectively). This conceptual extension distinguishes the MATCH framework from other TB monitoring and evaluation tools in three main aspects.
Firstly, it requires data analysis to be conducted using a set of adjacent subnational data, aggregated to the smallest available geographic unit available. Using subnational data allows one to visualize and quantify geographic variations in TB case notifications. These variations can be used to investigate spatial anomalies in which areas deviate from their surrounding areas, which then need to be investigated.
Secondly, data which are commonly not used by health programs, either due to limitations in accessing data, or due to interoperability issues such as incompatible units of reporting, are included in the analysis. The use of Geographic information System (GIS) and spatial data allow the integration of data collected across varying levels of aggregation and spatial delineation into a single unified spatial database.
Thirdly, subnational variations are explicitly quantified and accounted for by using spatial models to detect spatial patterns in the pathway. Therefore, it allows one to assess the geographic scale at which socio-economic, epidemiological and health system processes operate and interact. For example, small scale clusters of low TB case notifications might coincide with larger geographic clusters of good health system coverage. This might raise suspicion regarding the low numbers of TB patients being reported, possibly being caused by limited access to available services. Such findings provide insight in the effectiveness of health systems to detect and diagnose TB and provide important information for future planning.
To identify gaps in patient progression along the pathway of care, these principles were applied by simultaneously analyzing associations between locally observed case notification rates and proxies of TB risk, access to care and the quality of TB care services, explicitly accounting for spatial trends in these data.
2.2. Bangladesh Case Study Data
TB notification data, as well as the number of patients tested, treated, cured and retreated, reported by each of the 489 upazilas of Bangladesh (third level administrative units) to the NTP were collected for the year 2016. These data were complemented with socioeconomic data derived from the national census, Household Income and Expenditure survey (HIES) and laboratory data. All data were merged and joined with spatial polygon data of upazilas using a Geographic information System (GIS). All data obtained from different sources were integrated into one unified source database based on their common geographies (i.e., upazilas). An overview of the data used in this study is provided in
Table 1.
As routine surveillance data are likely to contain a certain amount of error, all data were validated by means of their internal consistency. Internal consistency [
16] was measured as the observed deviation of each observation from the overall mean of all observations. This showed that 12 out of the 489 upazilas (12/489 = 2.5%) reported case notification rates that were more than three standard deviations above the national mean of 125 cases per 100,000 population per year, which is usually indicative of reporting errors. The inclusion of outlying observations can potentially result in severe bias of parameter estimates of interest [
17]. Therefore, outlying values were substituted by imputing new values based on an unconditional random draw from a distribution with a mean and standard deviation equal to those of the remaining 477 upazilas included in the analysis [
18]. Five upazilas did not report TB patients to the NTP in 2016. These were omitted from the analysis, resulting in a final dataset including 484 upazilas.
Data were processed and stored in standardized thematic tables and stored in a PostgreSQL database. Data management and analyses were conducted using R language for statistical analysis (packages used: rgdal, spdep, reshape2, ncf) [
19]. Maps were made using QGIS 3.2 Geographic Information System [
20].
2.3. Data Analysis
To assess whether case notification rates across upazilas are spatially auto correlated and to locate clusters reporting high or low TB case notification rates, local indicators of spatial autocorrelation [
21] were calculated. A spatial correlogram was used to assess at which scale TB case notification rates are spatially clustered.
Next, the geographic pattern of TB case notification rates was compared to factors related to TB risk, access to health care and program performance. As subnational measures of TB prevalence were not available, poverty was used as an indicator of TB risk. The Bangladesh TB prevalence survey of 2007–2009 showed that TB incidence was significantly higher in people living in the lowest wealth quintile (incidence rate ratio (IRR): 1.73) [
22]. Other social and economic factors which are associated with an increased risk are often causally linked to poverty. Therefore, poverty was used as the key indicator of TB risk. Access to TB services was assessed using the TB testing rate, which was calculated as the total number of people tested for TB per 100,000 population. Finally, the retreatment rate was used to evaluate the effect of program performance on TB notifications. As the objective of the analysis was to simultaneously evaluate the effect of these factors on the drop-out of patients along the pathway, all variables were simultaneously entered into the model.
Simultaneous autoregressive models (SAR) [
23,
24], using a spatially correlated error structure, were used to analyze the combined effect of TB risk populations, access and program performance on TB case notification rates. Using a spatially explicit model allows the discernment of factors explaining variations in TB notification rates, while correcting for the lack of dependence between individual observations. This was of particular importance as a lack of independence between observations could result in type I errors when fitting regression models to the data [
25]. For example, the movement of patients commuting across upazilas from where they live to where they seek health care could lead to spatial diffusion of locally increased case notification rates, leading to biased results. Such processes are explicitly accounted for by using SAR models, as it prevents false significant associations between CNR and factors included in the model.
To assess the existence and magnitude of spatial autocorrelation (SAC) in the data, six different SAR models including the same covariates, but with varying spatial weight matrices (e.g., conceptualizations of the spatial surrounding areas) were fitted to the data: directly adjacent spatial neighbors; the five and 10 nearest neighbors; the neighbors within 20 and 15 km distances; and inverse travel distance weighted neighbors. Travel distances were based on smallest travel distance calculated along the primary and secondary road network in Bangladesh using the “Dijkstra” shortest distance algorithm calculated in postGIS [
26]. The best fitting model was identified based on the model with the lowest log likelihood. The effect of data imputation on the model fit was assessed by comparing Nagelkerke’s pseudo R-squared [
27] of a model fit to the data to that of the model fit using the imputed data. The final model fit was evaluated by means of diagnostic plots of observed and predicted values as well as residual plots.
To identify areas where TB under-detection and diagnosis are expected to occur, the best fitting model was used to predict the expected CNR based on the covariates (e.g., trend) and spatial dependencies (e.g., signal) in the data [
28]. Next, a standardized CNR, accounting for effects of poverty, testing and retreatment rate, was calculated by subtracting the predicted trend component from the observed CNR. The resulting prediction reflects the expected CNR when poverty, testing and retreatment would not affect case notification rates. Finally, the incidence rate ratio (IRR) of the observed divided by the predicted CNR were calculated for each upazila and mapped to identify areas which over- or under-reported TB.
3. Results
In 2016, a total of 220,273 cases of all forms of TB, consisting of 175,116 new and relapse cases of TB, were reported from 485 upazilas to the national TB program. Five upazilas (0.8%) did not report any cases and were omitted. The national case notification rate of 138/10,000 population varied greatly between upazilas [interquartile range: 73.3–145.2]. In total, 1641 patients who had previously started TB treatment were retreated in 2016, resulting in a national retreatment rate of 0.75% [interquartile range: 0.0–1.1%].
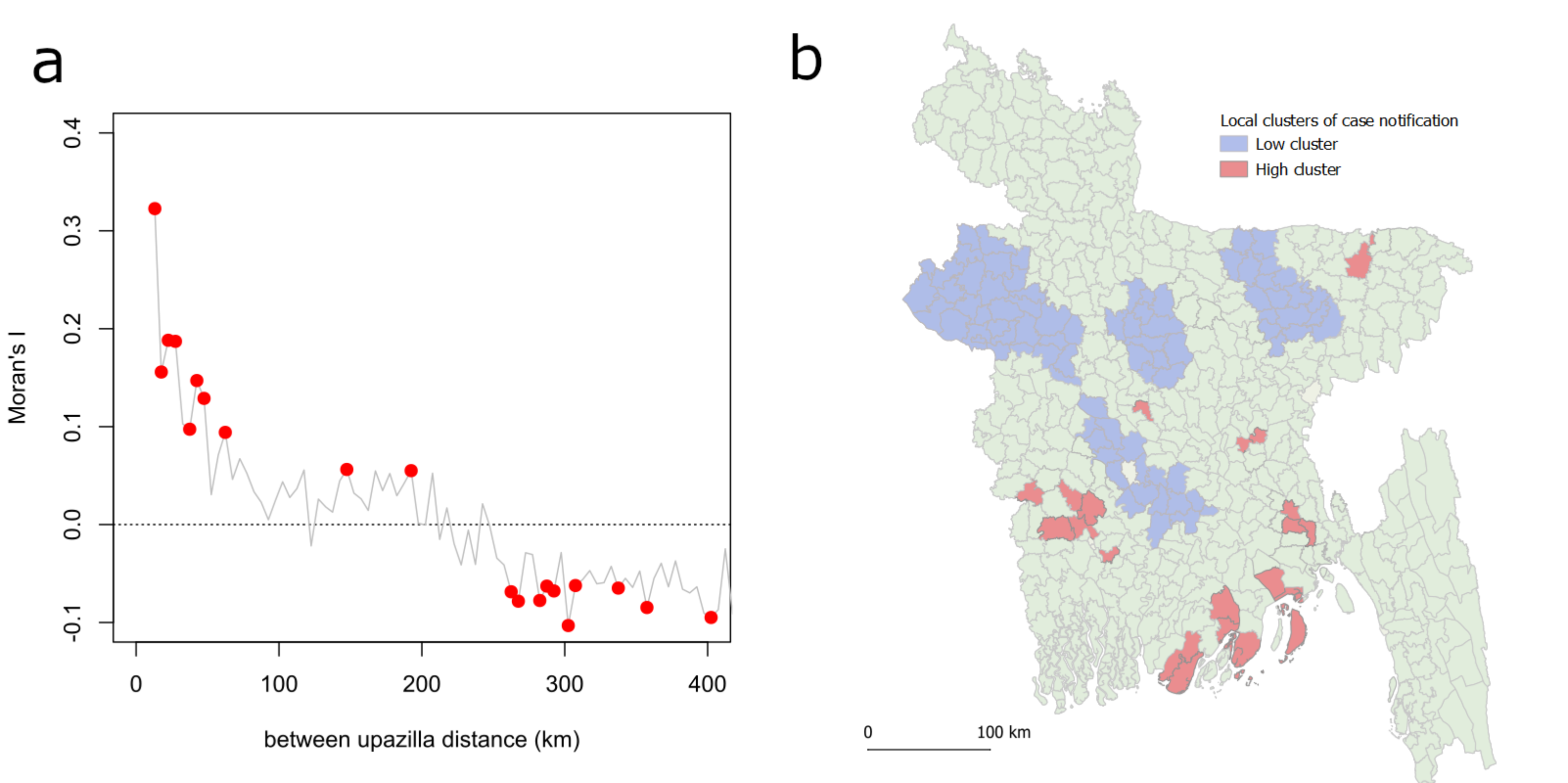
The spatial correlogram, testing for spatial autocorrelation over incremental distances, showed that significant autocorrelation of TB notification rates existed at scales of 5–70 km (Moran’s I range: 0.32–0.09,
p < 0.01;
Figure 2a). Local clusters of low case notification areas were identified across the central-west and central Bangladesh (
Figure 2b). Notably, clusters of consistently low CNR were found directly adjacent to areas that were consistently reporting a high CNR.
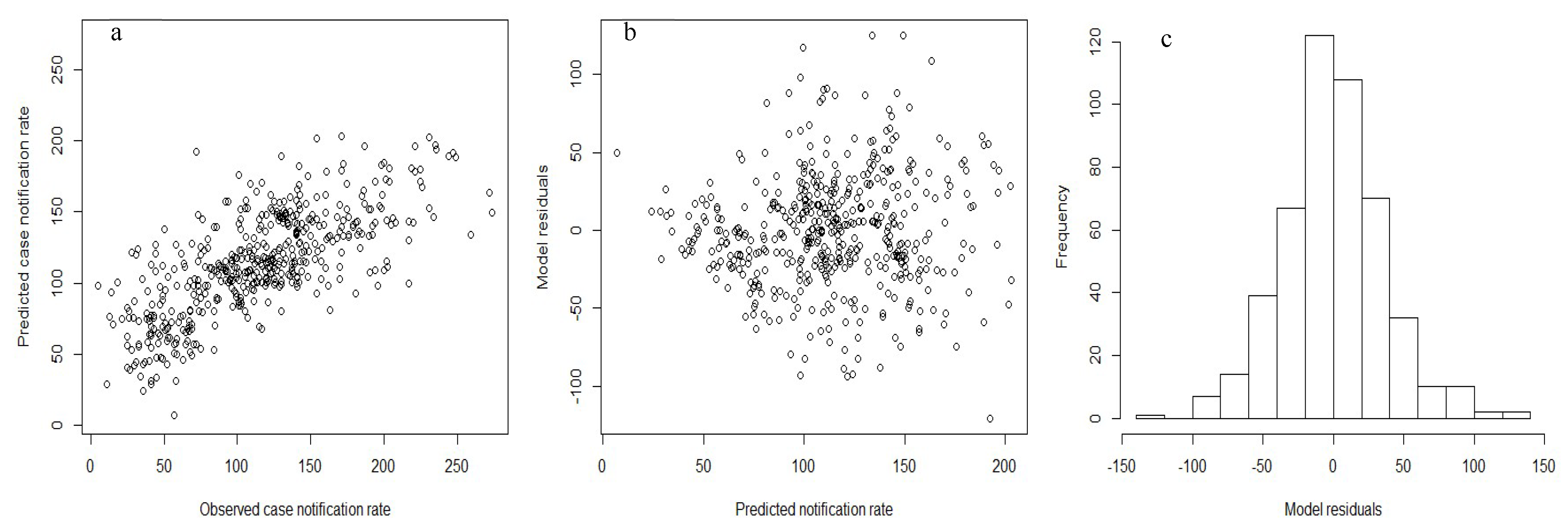
Table 2 shows the results of fitting models with different autocorrelation structures to the case notification rate data for 2016 in Bangladesh. Regardless of the spatial correlation structure used in the model, case notifications rates were found to be positively associated with the number of persons receiving bacteriological testing for TB and negatively correlated to the retreatment rate. In three models, negative correlations were found between CNR and poverty rates. Spatial models with autocorrelation structures corresponding to the ten nearest neighbors outperformed models which with correlation structures accounting for higher order levels of contiguity or distance based neighborhood models (Log-Likelihood = 2439;
Table 2). The best fitting model showed a good fit to the observed TB case notification rates (
Figure 3). The Nagelkerke’s pseudo R
2 of goodness of fit showed that the model based on the imputed data outperformed that of a model based on the raw data (Nagelkerke R
2: 0.50 versus 0.18, respectively).
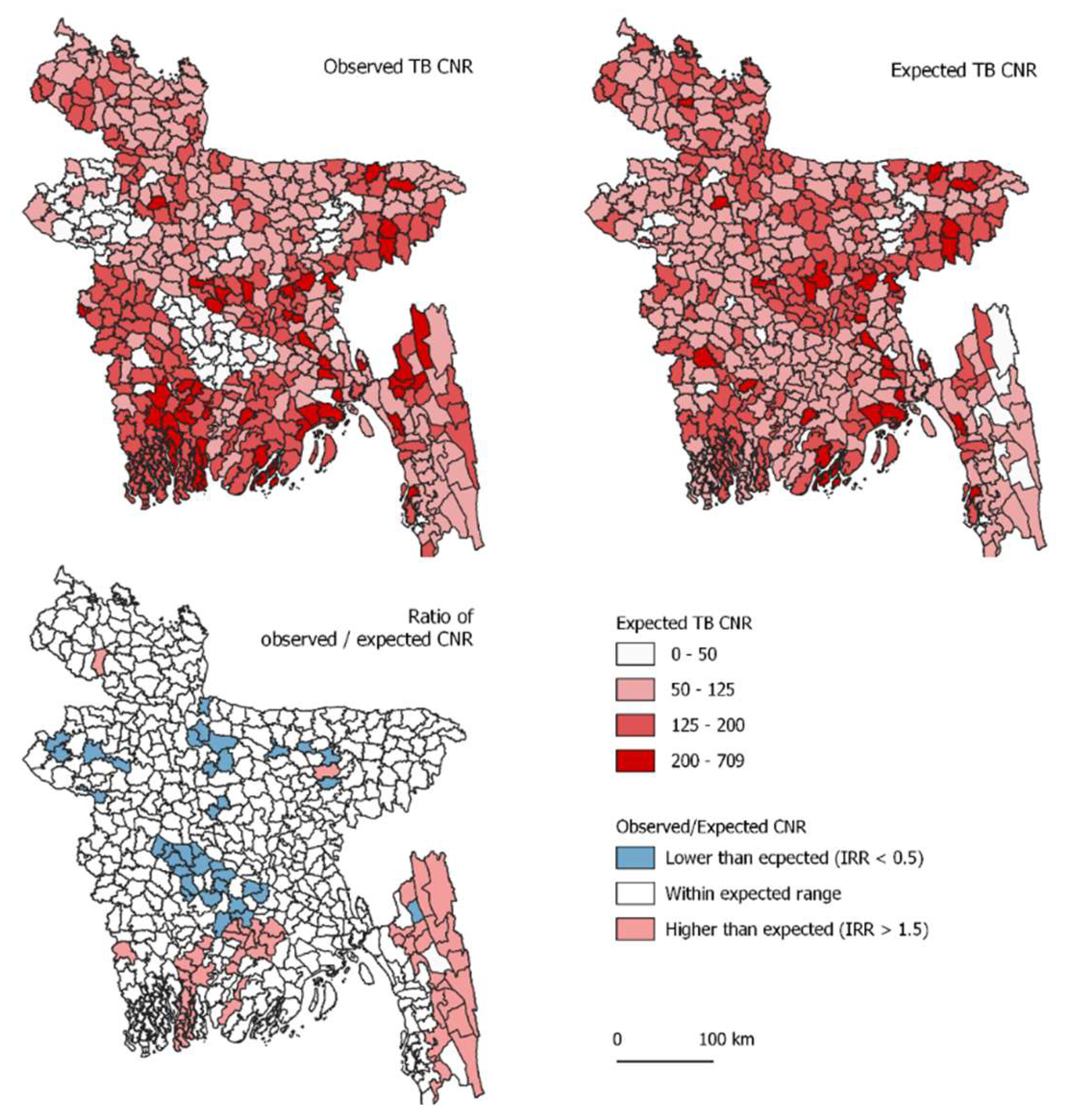
The best fitting model based on poverty (β = −8.7,
p = 0.04), testing rate (β =0.09,
p < 0.0001) and retreatment rate (β = −8.5,
p < 0.0001) was used to predict the expected case notification. The geographic pattern of the IRR map showed that low IRRs, indicative of TB under-detection and under notification, are expected to occur in the mid-central and northern central regions of Bangladesh (
Figure 4). Likewise, regions of high IRR were found in the southern and south-east of the country.
4. Discussion
The MATCH analytical framework was applied to analyze routinely collected, geographically disaggregated data in order to evaluate gaps in TB case detection and reporting in Bangladesh. The application of the MATCH framework allowed to assess the scale and strength of spatial trends in TB case notification rates at various spatial scales. The results of these analyses showed that TB notifications rates vary greatly across the country. Small clusters of geographically adjacent upazilas reporting similar TB rates were identified across the country. Accounting for spatial dependencies within clusters of geographically contiguous upazilas made it possible to assess the effects of TB risk and program delivery while taking into consideration the effect of the wider geographical surroundings. SAR modeling showed that significant spatial dependence in reported TB CNR existed between upazilas. These findings provide important insights regarding the location, scale and possible causes of TB under detection and underreporting. They provide valuable information required to target interventions, accounting for context specific factors causing the observed variations in TB case notifications.
Based on the model presented, TB case notifications were found to be negatively associated with poverty rates. This finding contrasts the results of the Bangladesh TB prevalence study in which TB was found to be most prevalent in the lowest quintile (IRR 1.74 (137.9/79.4) [
21]. However, poverty has been shown to be an important factor limiting access to healthcare [
29,
30]. Therefore, the negative association found between TB case notification rates and poverty is likely to be caused by the limitation of reaching TB diagnostic care and treatment rather than reduced risk of TB. Hence, the dual association of poverty with TB reporting in Bangladesh should be considered and underlines its importance for decision support as it is expected to both result in higher TB transmission but also to limit the detection of TB as a results of reduced financial access to TB services.
TB case notification rates were found to be significantly associated with both TB testing rates as well as TB retreatment rates. Although not surprising, this does suggest that the health system in Bangladesh might not be screening sufficient numbers of people presumptive for TB to detect new cases. Increasing the number of people screened and tested is expected to lead to an increase in TB case detection, with 8–10 more cases expected to be detected for every 1000 additional persons being bacteriologically tested for TB. Naturally, this relation is expected to decrease with increasing case detection success. Therefore, it is important that the additional value of screening and testing of people presumptive for TB is closely monitored to find the right balance between the amount of resources invested and the number of additional cases detected. In large areas where indiscriminate testing for TB does not result in increased TB case detection, alternative and more targeted TB screening and testing strategies should be considered.
The negative association between TB case notification rates and TB retreatment rate is used as a proxy to assess the overall success of the TB program to identify new TB cases. Treatment failure due to interrupted treatment, drug resistance or other causes could lead the patient to remain infected and re-enter the health system as a retreatment case. As retreatment is more likely in TB patients who do not adhere to treatment or due to deficiencies in the medication used, it can reveal limitations in the effectiveness of the NTP. As retreatment is independent of being reported, the retreatment rate is an important indicator of program performance. In a well-functioning TB program, TB retreatment rates are expected to represent a stable proportion of TB cases identified. High retreatment rates, caused by low treatment success, would be expected to result in continuous transmission, and consequently, in high rates of new TB. An inversed relation was found in this study. It is expected that the association between CNR and retreatment rates reflects a gap in the detection of new TB cases by programs.
The spatial pattern of standardized case notification rates, in which the effect of covariate factors was removed, differed considerably from the spatial pattern of the observed rates. The discrepancy between these patterns could be indicative of TB under detection and diagnosis and should be prioritized for targeted interventions. Since the model outputs are based on a conceptual generalization of the hypothesized relations between factors influencing effective TB case detection and reported TB notifications, expert opinions are required to verify the causative mechanism resulting in low notification rates.
The primary objective of this study was to validate the use of case notification rates as a proxy for TB incidence, accounting for the partial effect of TB risk and health system factors driving TB notification rates. Therefore, the absence of associations between TB notification rates and covariates of TB risk does not pose a limitation to the model. However, since the relation between poverty and TB burden was not found to reflect transmission risks, other factors affecting TB transmission, such as indoor living conditions and crowding [
31], are expected to complement the current findings to explain residual variation in CNR not accounted for in the model. These should be included in future models to further investigate how TB transmission risk and health system functions affect TB detection. Since the observed spatial pattern of TB notifications could not be fully attributed to the geographic patterns in the covariates included in the model, other epidemiological factors should still be further investigated to explain the observed pattern.
5. Conclusions
The reported TB case notification rates in Bangladesh showed considerable spatial heterogeneity and spatial clustering. TB case notifications showed unambiguous geographic patterns and were highly associated with factors influencing access to TB care, program coverage and performance. Accounting for these patterns enabled to identify areas where TB underreporting is likely to occur.
The MATCH analytical framework enabled to evaluate the use of TB notification rate as an indicator to monitor progress towards the SDG 3 indicator to end the global TB epidemic by 2030. More specifically, it enabled the identification of geographical anomalies in routine TB reporting which could be indicative of TB under detection and underreporting. The analysis of subnational data and integrating various independent data sources using GIS further enabled the identification and location of target areas where TB under-detection, diagnosis and reporting are expected to occur. Supervision missions should be targeting these areas to further verify these findings and to allocate resources more efficiently.
The fact that case notification rates were found to depend on programmatic testing efforts and performance underscores the recommendation that these should not be used as a proxy of TB incidence without further consideration of health system functioning. Careful consideration should be given to local heterogeneities in factors affecting TB case notifications when estimating TB burden (i.e., incidence). The MATCH analytical framework has provided a clear approach that will enable TB managers to plan and evaluate their activities and to identify potential gaps in patient pathways. When routinely applied to analyze subnational TB surveillance data, the methodology is expected to progressively provide new insights and generate evidence, which are required to end the TB epidemic by 2030.
Author Contributions
Conceptualization, E.R. and M.B.; Methodology, E.R.; Formal Analysis, E.R.; Resources, A.H.K. and P.K.M.; Data Curation, A.K. and M.v.G.; Writing—Original Draft Preparation, E.R.; Writing—Review & Editing, M.B. and C.M.; Supervision, L.B. and M.B.
Funding
This work was conducted with support of the knowledge investment fund of KIT Royal Tropical Institute
Acknowledgments
The authors would like to acknowledge The KIT Royal Tropical Institute for funding this research and the preparation on this paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. End TB Strategy; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- IAEG-SDGs. SDG Indicators. Available online: https://unstats.un.org/sdgs/iaeg-sdgs/tier-classification/ (accessed on 30 September 2018).
- Van Leth, F.; van der Werf, M.J.; Borgdorff, M.W. Prevalence of Tuberculous Infection and Incidence of Tuberculosis: A Re-Assessment of the Styblo Rule; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Glaziou, P.; Sismanidis, C.; Zignol, M.; Floyd, K. Methods Used by WHO to Estimate the Global Burden of TB Disease; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Alba, S.; Rood, E.; Bakker, M.I.; Straetemans, M.; Glaziou, P.; Sismanidis, C. Development and Validation of a Predictive Ecological Model for TB Prevalence. Int. J. Epidemiol. 2018, 47, 1645–1657. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.; Osberg, M.; Brown, J.; Durham, G.; Chin, D.P. Finding the Missing Patients with Tuberculosis: Lessons Learned From Patient-Pathway Analyses in 5 Countries. J. Infect. Dis. 2017, 216 (Suppl. 7), S686–S695. [Google Scholar] [CrossRef]
- Mhimbira, F.A.; Cuevas, L.E.; Dacombe, R.; Mkopi, A.; Sinclair, D. Interventions to Increase Tuberculosis Case Detection at Primary Healthcare or Community-Level Services. Cochrane Database Syst. Rev. 2017, 11, CD011432. [Google Scholar] [CrossRef] [PubMed]
- Rood, E.J.J.; Mergenthaler, C.; Bakker, M.I.; Redwood, L.; Mitchell, E.M.H. Using 15 DHS Surveys to Study Epidemiological Correlates of TB Courtesy Stigma and Health-Seeking Behaviour. Int. J. Tuberc. Lung Dis. 2017, 21, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.; Sahu, S.; Blok, L.; Bakker, M.I.; Stevens, R.; Ditiu, L. A Multi-Site Evaluation of Innovative Approaches to Increase Tuberculosis Case Notification: Summary Results. PLoS ONE 2014, 9, e94465. [Google Scholar] [CrossRef] [PubMed]
- Duc, L.V.; Vree, M.; Sy, D.N.; Co, N.V.; Borgdorff, M.W.; Cobelens, F.G.J. Steep Increases in Tuberculosis Notification among Young Men in the Industrialised Districts of Danang, Vietnam. Int. J. Tuberc. Lung Dis. 2007, 11, 567–570. [Google Scholar] [PubMed]
- Kranzer, K.; Afnan-Holmes, H.; Tomlin, K.; Golub, J.E.; Shapiro, A.E.; Schaap, A.; Corbett, E.L.; Lönnroth, K.; Glynn, J.R. The Benefits to Communities and Individuals of Screening for Active Tuberculosis Disease: A Systematic Review [State of the Art Series. Case Finding/Screening. Number 2 in the Series]. Int. J. Tuberc. Lung Dis. 2013, 17, 432–446. [Google Scholar] [CrossRef]
- Tulloch, O.; Theobald, S.; Morishita, F.; Datiko, D.G.; Asnake, G.; Tesema, T.; Jamal, H.; Markos, P.; Cuevas, L.E.; Yassin, M.A. Patient and Community Experiences of Tuberculosis Diagnosis and Care within a Community-Based Intervention in Ethiopia: A Qualitative Study. BMC Public Health 2015, 15, 187. [Google Scholar] [CrossRef]
- Datiko, D.G.; Yassin, M.A.; Theobald, S.J.; Blok, L.; Suvanand, S.; Creswell, J.; Cuevas, L.E. Health Extension Workers Improve Tuberculosis Case Finding and Treatment Outcome in Ethiopia: A Large-Scale Implementation Study. BMJ Glob. Heal. 2017, 2, e000390. [Google Scholar] [CrossRef]
- Oliwa, J.N.; Maina, J.; Ayieko, P.; Gathara, D.; Kathure, I.A.; Masini, E.; Van’t Hoog, A.H.; van Hensbroek, M.B.; English, M. Variability in Distribution and Use of Tuberculosis Diagnostic Tests in Kenya: A Cross-Sectional Survey. BMC Infect. Dis. 2018, 18, 328. [Google Scholar] [CrossRef]
- The MATCH Approach for Enhancing TB Care Coverage—Health. Available online: https://www.kit.nl/health/service/kit-match-approach-enhancing-tb-care-coverage/ (accessed on 30 September 2018).
- Fletcher, T. Quality Framework and Guidelines for OECD Statistical Activities. The Organisation for Economic Co-operationand Development. 2012. Available online: http://www.oecd.org (accessed on 28 December 2018).
- Ludbrook, J. Outlying Observations and Missing Values: How Should They Be Handeled? Clin. Exp. Pharmacol. Physiol 2008, 35, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Donders, A.R.T.; van der Heijden, G.J.M.G.; Stijnen, T.; Moons, K.G.M. Review: A Gentle Introduction to Imputation of Missing Values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2014. [Google Scholar]
- QGIS Geographic Information System; QGIS Development Team: Bonn, Germany, 2018.
- Anselin, L. Local Indicators of Spatial Association-LISA. Geogr. Anal. 2010, 27, 93–115. [Google Scholar] [CrossRef]
- ICDDR-B. National Tuberculosis Prevalence Survey, Bangladesh 2007–2009; ICDDR-B: Dhaka, Bangladesh, 2009. [Google Scholar]
- Besag, J. Spatial Interaction and the Statistical Analysis of Lattice Systems. J. R. Stat. Soc. Ser. B (Methodol.) 1974, 36, 192–236. [Google Scholar] [CrossRef]
- Kissling, W.D.; Carl, G. Spatial Autocorrelation and the Selection of Simultaneous Autoregressive Models. Glob. Ecol. Biogeogr. 2007, 17, 59–71. [Google Scholar] [CrossRef]
- Dormann, C.F.; McPherson, J.M.; Araújo, M.B.; Bivand, R.; Bolliger, J.; Carl, G.; Davies, R.G.; Hirzel, A.; Jetz, W.; Daniel Kissling, W.; et al. Methods to Account for Spatial Autocorrelation in the Analysis of Species Distributional Data: A Review. Ecography 2007, 30, 609–628. [Google Scholar] [CrossRef]
- Corti, P.; Mather, S.V.; Kraft, T.J.; Park, B. PostGIS Cookbook; Packt Publishing: Birmingham, UK, 2014. [Google Scholar]
- Nagelkerke, N.J.D. A Note on a General Definition of the Coefficient of Determination. Biometrika 1991, 78, 691–692. [Google Scholar] [CrossRef]
- Goulard, M.; Laurent, T.; Thomas-Agnan, C. About Predictions in Spatial Autoregressive Models: Optimal and Almost Optimal Strategies. Spat. Econ. Anal. 2017, 12, 304–325. [Google Scholar] [CrossRef]
- Asres, A.; Jerene, D.; Deressa, W. Pre- and Post-Diagnosis Costs of Tuberculosis to Patients on Directly Observed Treatment Short Course in Districts of Southwestern Ethiopia: A Longitudinal Study. J. Health. Popul. Nutr. 2018, 37, 15. [Google Scholar] [CrossRef] [PubMed]
- Barter, D.M.; Agboola, S.O.; Murray, M.B.; Bärnighausen, T. Tuberculosis and Poverty: The Contribution of Patient Costs in Sub-Saharan Africa—A Systematic Review. BMC Public Health 2012, 12, 980. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.W. Linking TB and the Environment: An Overlooked Mitigation Strategy. Environ. Health Perspect. 2008, 116, A478–A485. [Google Scholar] [CrossRef] [PubMed]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}