Issues of Healthcare Planning and GIS: A Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Identifying the most important historical gaps related to health geomatics based on understanding the spatial relationship between health and place. This will contribute to defining the most important healthcare planning issues that health organizations, institutions and researchers have been dealing with using GIS technology.
- Discussing five independent issues related to healthcare planning, unlike most previous studies and research that focused on reviewing one or two major issues (e.g., epidemiological planning or health resources allocation).
- Presenting a largest possible number of useful GIS analytical approaches related to each discussed issue of healthcare planning. This will contribute to defining the gaps that need further investigation, analysis and visualization under each issue.
2. Methods
3. Results
3.1. Brief History of Health Geomatics and GIS
3.2. Overview of Healthcare Planning
3.3. Issues of Healthcare Planning and GIS Role
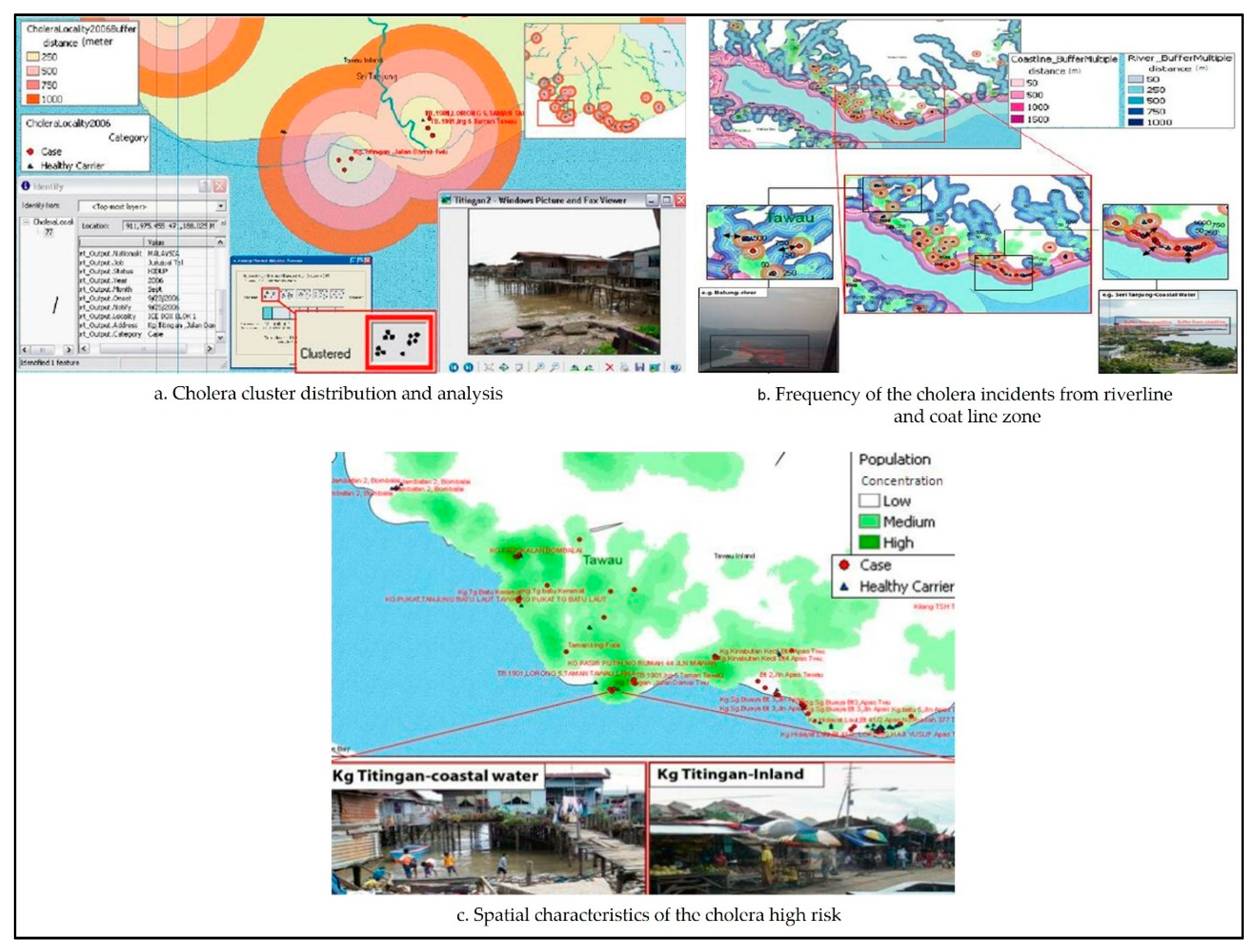
3.3.1. Epidemiological Planning and Disease Mapping
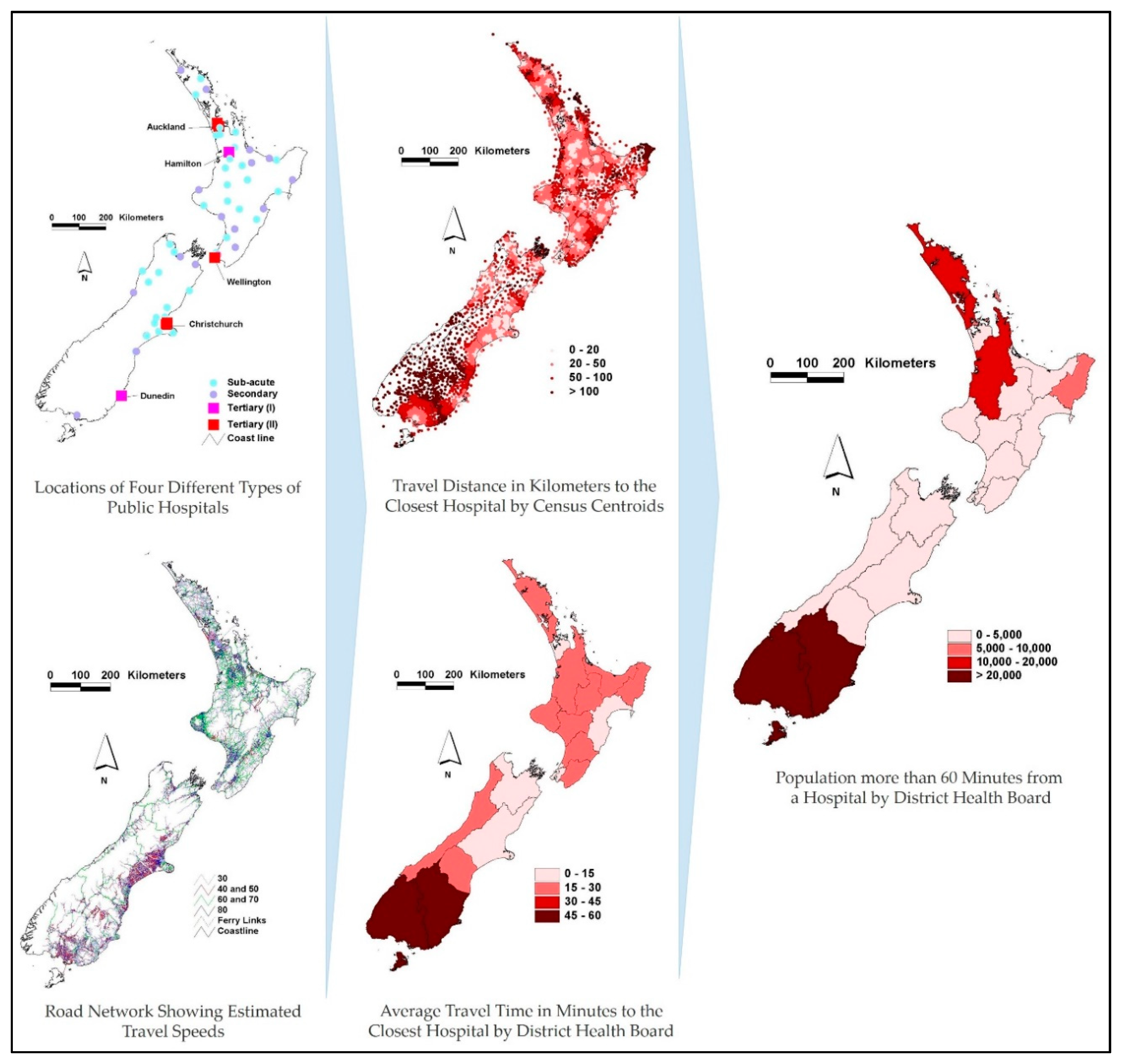
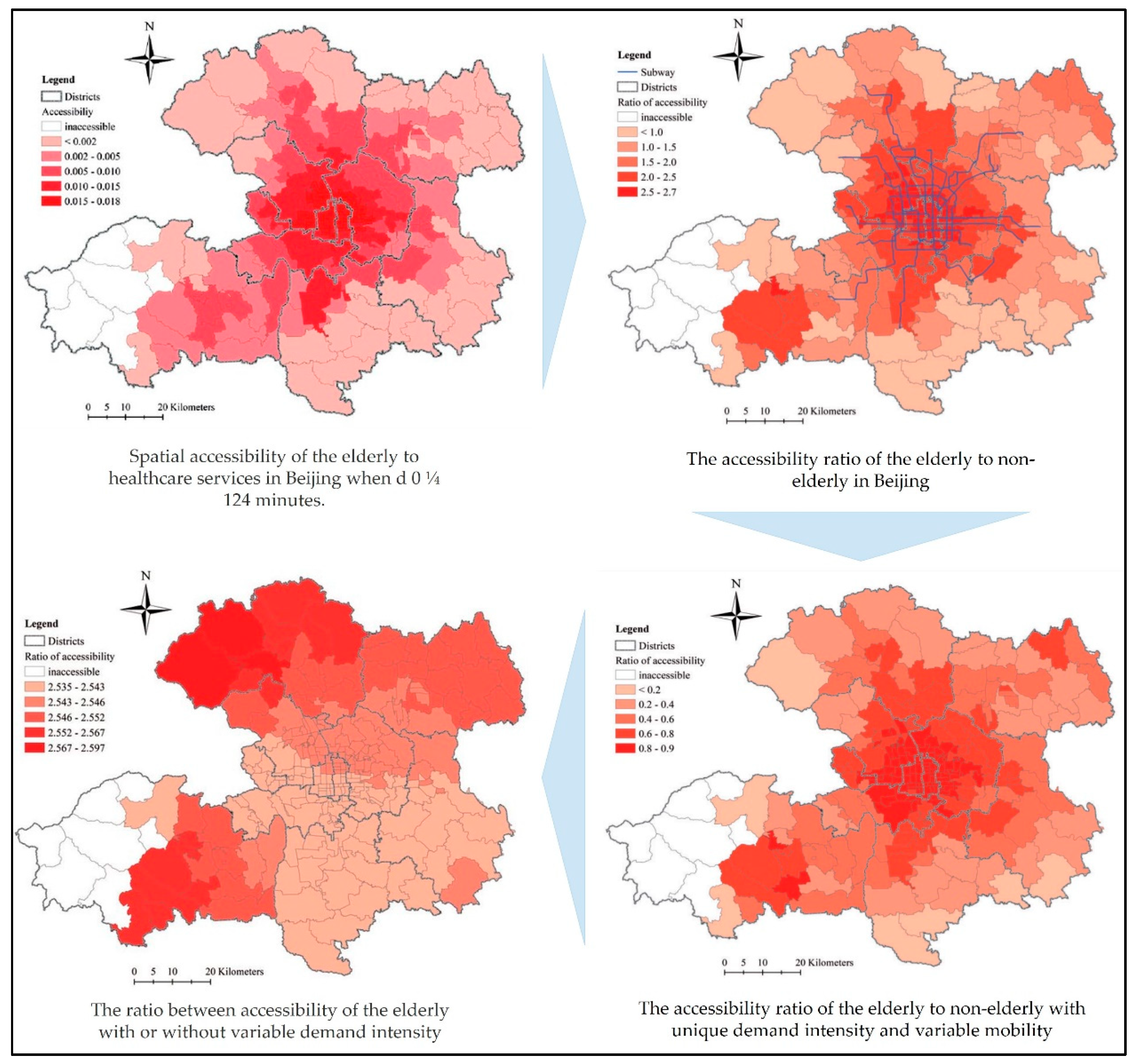
3.3.2. Accessibility and Utilization of Healthcare Services
3.3.3. Public Health and Information Management
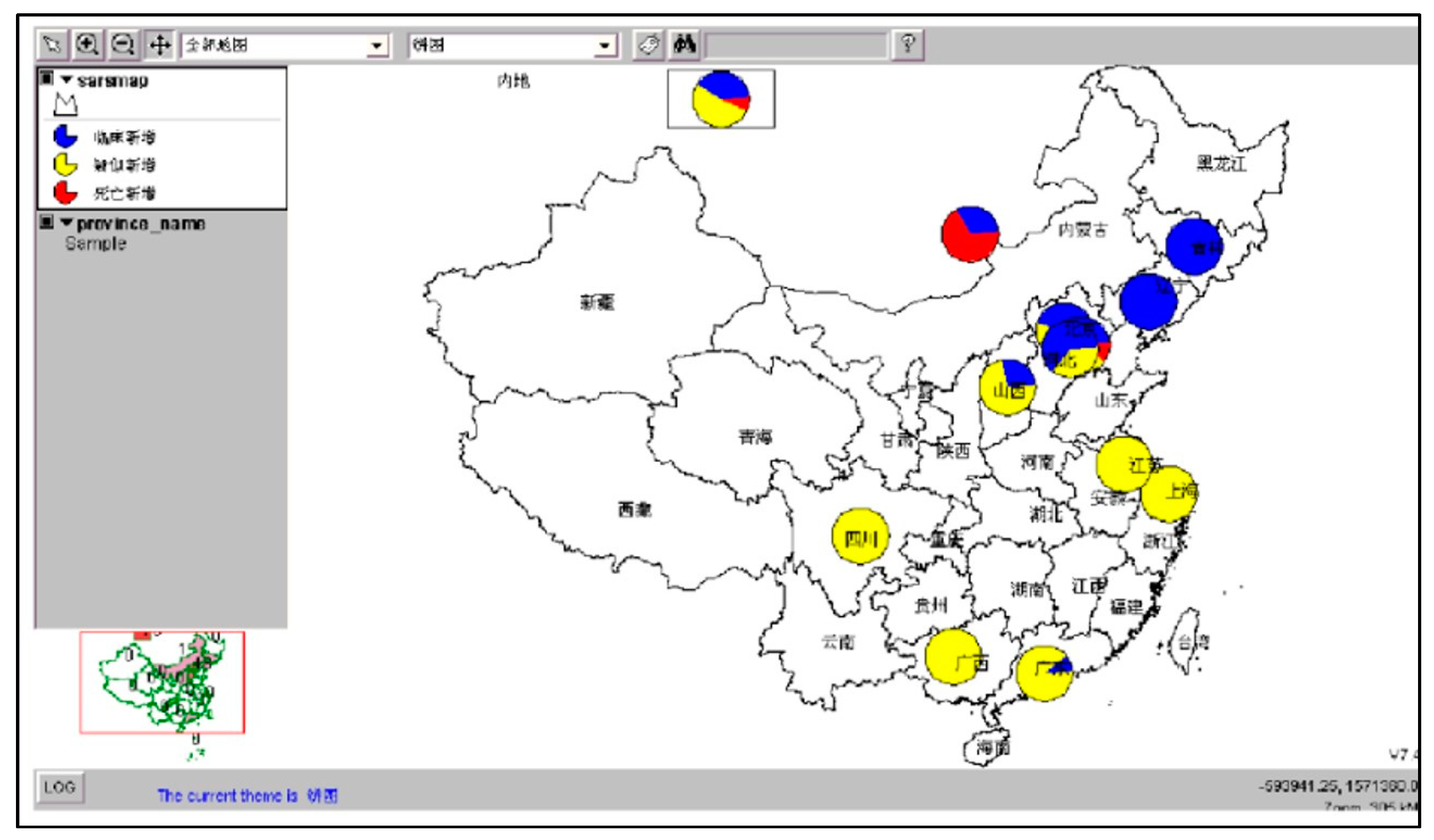
3.3.4. Public Health Surveillance
3.3.5. Location Allocation and Optimal Location Modelling
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Geraghty, E. Why Health is so Spatial. Available online: https://www.youtube.com/watch?v=3p7OFICg9Ak (accessed on 30 January 2020).
- Krieger, N. Place, Space, and Health: GIS and Epidemiology. Epidemiology 2003, 14, 384–385. [Google Scholar] [CrossRef]
- Pickle, L.W. Spatial Analysis of Disease. Cancer Treat. Res. 2002, 113, 113–150. [Google Scholar] [CrossRef] [PubMed]
- Gatrell, A.C.; Masser, I.; Salgé, F. GIS and Health; Informa UK Limited: London, UK, 1998; pp. 179–187. [Google Scholar]
- Curtis, S. Health and Inequality; SAGE Publications: Thousand Oaks, CA, USA, 2004. [Google Scholar]
- Yuan, M. Adding Time into Geographic Information System Databases. In The Handbook of Geographic Information Science; Wiley: Hoboken, NJ, USA, 2008; pp. 169–184. [Google Scholar]
- Koch, T. Mapping the Miasma: Air, Health, and Place in Early Medical Mapping. Cartogr. Perspect. 2005, 4–27, 4–27. [Google Scholar] [CrossRef]
- GisGeography. The Remarkable History of GIS. Available online: https://gisgeography.com/history-of-gis/ (accessed on 3 February 2020).
- ESRI. GIS for Public Health Today and Tomorrow. Available online: https://www.esri.com/news/arcuser/0499/umbrella.html (accessed on 3 February 2020).
- Koch, T. Disease Maps; The University of Chicago Press: Chicago, IL, USA, 2011; p. 247. [Google Scholar]
- D’Onofrio, A.; Mazzetta, C.; Robertson, C.; Smans, M.; Boyle, P.; Boniol, M. Maps and atlases of cancer mortality: A review of a useful tool to trigger new questions. Ecancermedicalscience 2016, 10, 670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yomralioglu, T.; Colak, E.H.; Aydinoglu, A.C. Geo-Relationship between Cancer Cases and the Environment by GIS: A Case Study of Trabzon in Turkey. Int. J. Environ. Res. Public Health 2009, 6, 3190–3204. [Google Scholar] [CrossRef] [Green Version]
- Altonen, B. Alfred Haviland—1875 (2ed. 1893)—Cancer in Great Britain. Public Health, Medicine and History. 2019. Available online: https://brianaltonenmph.com/gis/historical-disease-maps/alfred-haviland-1875-2ed-1893-disease-in-great-britain/ (accessed on 3 February 2020).
- Clarke, K.; McLafferty, S.L.; Tempalski, B. On epidemiology and geographic information systems: A review and discussion of future directions. Emerg. Infect. Dis. 1996, 2, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Croner, C. Public Health Geographic Information Systems (Gis) News and Information; 1994–1997. Center of Disease Control and Prevention. Available online: https://stacks.cdc.gov/view/cdc/13298 (accessed on 6 February 2020).
- CDC. Our History—Our Story. Available online: https://www.cdc.gov/about/history/index.html (accessed on 6 February 2020).
- World Health Organization. The Atlas of Heart Disease and Stroke. Available online: https://www.who.int/cardiovascular_diseases/resources/atlas/en/ (accessed on 17 February 2020).
- CDC. Heart Disease Death Rates, Total Population Ages 35+. Available online: https://www.cdc.gov/dhdsp/maps/national_maps/hd_all.htm (accessed on 8 February 2020).
- Musa, G.J.; Chiang, P.-H.; Sylk, T.; Bavley, R.; Keating, W.; Lakew, B.; Tsou, H.-C.; Hoven, C. Use of GIS Mapping as a Public Health Tool—From Cholera to Cancer. Health Serv. Insights 2013, 6, 111–116. [Google Scholar] [CrossRef]
- Farnia, P.; Aghajani, J.; Velayati, A. Impact of geographical information system on public health sciences. Biomed. Biotechnol. Res. J. 2017, 1, 94. [Google Scholar] [CrossRef]
- Briney, A. Overview of Public Health and GIS. Gislounge. Available online: https://www.gislounge.com/overview-public-health-gis/ (accessed on 8 February 2020).
- CESCR—Committee on Economic, Social and Cultural Rights. The Right to the Highest Attainable Standard of Health. United Nations Human Rights. Available online: https://www.refworld.org/pdfid/4538838d0.pdf (accessed on 26 May 2020).
- Sherif, A. Towards Spatial Justice in Urban Health Services Planning. Ph.D. Thesis, University of Utrecht, Utrecht, The Netherlands, 2007. [Google Scholar]
- Drissy, A. The Evolution of Health Expenditure in Algeria and its Effectiveness in the Reform of the Health System During the Period (2013–2004). Algerian J. Glob. Econ. Policies. 2015, 6, 137–145. [Google Scholar]
- Mokgalaka, H. Measuring Access to Primary Health Care: Use of a GIS-Based Accessibility Analysis. Semantic Scholar. Available online: https://pdfs.semanticscholar.org/5a16/14e0c2db094958a992a2b8a30c335b55d22b.pdf?_ga=2.240499466.883523912.1577652254-1188223766.1576187194 (accessed on 29 December 2019).
- Dallhammer, E.; Gaugitsch, R.; Neugebauer, W. Spatial Planning and Governance within EU Policies and Legislation and Their Relevance to the New Urban Agenda (p. 2); European Committee of the Regions: Bruxelles, Belgium, 2018; Available online: https://cor.europa.eu/en/engage/studies/Documents/Spatial-planning-new-urban-agenda.pdf (accessed on 26 May 2020).
- McLafferty, S.L. GIS and Health Care. Annu. Rev. Public Health 2003, 24, 25–42. [Google Scholar] [CrossRef]
- Kirby, R.S.; Delmelle, E.; Eberth, J.M. Advances in spatial epidemiology and geographic information systems. Ann. Epidemiol. 2016, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nicol, J. Geographic information systems within the national health service: The scope for implementation. Plan. Outlook 1991, 34, 37–42. [Google Scholar] [CrossRef]
- Murad, A. Using GIS for Planning Public General Hospitals at Jeddah City. J. King Abdulaziz Univ. Des. Sci. 2005, 3, 3–22. [Google Scholar] [CrossRef]
- Datta, D.; S G, R.K.; Mb, A.N.; Bapilus, L.; Anandan, S. Spatial Epidemiology: Geostatistical Tool for Disease Mapping. World J. Pharm. Res. 2017, 6523, 1771–1780. [Google Scholar] [CrossRef]
- Little, M.; Meade, M.; Florin, J.; Gesler, W. Medical Geography. Geogr. Rev. 1989, 79, 247. [Google Scholar] [CrossRef]
- Gatrell, A.; Senior, M. Health and health care application in Longley P, Goodchild M, Maguire D and Rhind D, Geographical Information System Principles and Application; John Wiley & Sons: Hoboken, NJ, USA; pp. 925–938.
- Cliff, A.D.; Haggett, P.; Ord, J.K. Spatial Aspects of Influenza Epidemics; Pion: London, UK, 1986. [Google Scholar]
- Gould, P.; Wallace, R. Spatial Structures and Scientific Paradoxes in the AIDS Pandemic. Geografiska Annaler 1994, 76, 105–116. [Google Scholar] [CrossRef]
- Braga, M.; Cislaghi, C.; Luppi, G.; Tasco, C. A Multipurpose. Interactive Mortality Atlas of Italy. In GIS and Health; Gatrell, A.C., Löytönen, M., Eds.; Taylor and Francis: London, UK, 1998; pp. 125–138. [Google Scholar]
- Brown, P.J.B.; Hirschfield, A.; Batey, P.W.J. Applications of geodemographic methods in the analysis of health condition incidence data. Pap. Reg. Sci. 1991, 70, 329–344. [Google Scholar] [CrossRef]
- Wrigley, N. Market-based systems of health-care provision, the NHS Bill, and geographical information systems. Environ. Plan. A. 1991, 23, 5–8. [Google Scholar]
- Johnson, G.D. Small area mapping of prostate cancer incidence in New York State (USA) using fully Bayesian hierarchical modelling. Int. J. Health Geogr. 2004, 3, 29. [Google Scholar] [CrossRef] [Green Version]
- Rasam, A.A.R.; Ghazali, R.; Noor, A.M.M.; Naim, W.M.; Hamid, J.R.A.; Bazlan, M.J.; Ahmad, N. Spatial epidemiological techniques in cholera mapping and analysis towards a local scale predictive modelling. In Proceedings of the IOP Conference Series: Earth and Environmental Science; IOP Publishing: Bristol, UK, 2014; Volume 18, p. 12095. [Google Scholar]
- Brown, B. 5 Benefits of Geographic Information Systems in Healthcare. Hitconsultant. Available online: https://hitconsultant.net/2015/10/29/5-benefits-of-geographic-information-systems-in-healthcare/#.Xe0UX-jXJPY (accessed on 8 December 2019).
- Sones, M. Reveal: Mapping and Tracking the Spread of Deadly Diseases. Available online: https://www.esri.com/about/newsroom/blog/reveal-mapping-and-tracking-the-spread-of-deadly-diseases/ (accessed on 18 December 2019).
- Fradelos, E.C.; Papathanasiou, I.V.; Mitsi, D.; Tsaras, K.; Kleisiaris, C.F.; Kourkouta, L. Health Based Geographic Information Systems (GIS) and their Applications. Acta Inform. Medica 2014, 22, 402–405. [Google Scholar] [CrossRef] [Green Version]
- WHO. World Bank and WHO: Half the World Lacks Access to Essential Health Services, 100 Million Still Pushed Into Extreme Poverty Because of Health Expenses. Available online: https://www.who.int/news-room/detail/13-12-2017-world-bank-and-who-half-the-world-lacks-access-to-essential-health-services-100-million-still-pushed-into-extreme-poverty-because-of-health-expenses (accessed on 21 December 2019).
- Bhatt, J.; Bathija, P. Ensuring Access to Quality Health Care in Vulnerable Communities. Acad. Med. 2018, 93, 1271–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, A.P.; Bentham, G. Emergency medical service accessibility and outcome from road traffic accidents. Public Health 1995, 109, 169–177. [Google Scholar] [CrossRef]
- Forbers, H.; Todd, P. Review of Cancer Services, Northwest Regional Health Authority, Urban Research and Policy Evaluation Regional Research Laboratory. University of Liverpool: Liverpool, UK, 1995. [Google Scholar]
- World Health Organization. Barriers and Facilitating Factors in Access to Health Services in the Republic of Moldova. Health Policy Paper; WHO: Moldova, 2012; pp. 4–22. Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/183510/e96775-final.pdf (accessed on 21 December 2019).
- Mohan, J.; Joseph, A.E.; Phillips, D.R. Accessibility and Utilization: Geographical Perspectives on Health Care Delivery. Trans. Inst. Br. Geogr. 1986, 11, 121. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.A.; Bhardwaj, S.M. Access to Healthcare: A Conceptual framework and its relevance to Health Care Planning. Eval. Health Prof. 1994, 17, 60–76. [Google Scholar] [CrossRef]
- Foley, R. Assessing the applicability of GIS in a health and social care setting: Planning services for informal carers in East Sussex, England. Soc. Sci. Med. 2002, 55, 79–96. [Google Scholar] [CrossRef] [Green Version]
- Teljeur, C.; Barry, J.; Kelly, A. The potential impact on travel times of closure and redistribution of A&E units in Ireland. Ir. Med J. 2004, 97, 6. [Google Scholar]
- Kumar, N. Changing geographic access to and locational efficiency of health services in two Indian districts between 1981 and 1996. Soc. Sci. Med. 2004, 58, 2045–2067. [Google Scholar] [CrossRef]
- Parker, E.B.; Campbell, J.L. Measuring access to primary medical care: Some examples of the use of geographical information systems. Health Place 1998, 4, 183–193. [Google Scholar] [CrossRef]
- Brabyn, L.; Skelly, C. Modeling population access to New Zealand public hospitals. Int. J. Health Geogr. 2002, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Murad, A. Using GIS for Determining Variations in Health Access in Jeddah City, Saudi Arabia. ISPRS Int. J. Geo-Inf. 2018, 7, 254. [Google Scholar] [CrossRef] [Green Version]
- Christie, S.; Fone, D. Equity of access to tertiary hospitals in Wales: A travel time analysis. J. Public Health Med. 2003, 25, 344–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokgalaka, H. GIS-Based Analysis of Spatial Accessibility: An Approach to Determine Public Primary Healthcare Demand in Metropolitan Areas. Master’s Thesis, University of Cape Town, Cape Town, South Africa, 2015. [Google Scholar]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanuganti, S.; Sarkar, A.; Singh, A.P. Quantifying Accessibility to Health Care Using Two-step Floating Catchment Area Method (2SFCA): A Case Study in Rajasthan. Transp. Res. Procedia 2016, 17, 391–399. [Google Scholar] [CrossRef]
- Tao, Z.; Cheng, Y. Modelling the spatial accessibility of the elderly to healthcare services in Beijing, China. Environ. Plan. B: Urban Anal. City Sci. 2018, 46, 1132–1147. [Google Scholar] [CrossRef]
- Ni, J.; Liang, M.; Lin, Y.; Wu, Y.; Wang, C. Multi-Mode Two-Step Floating Catchment Area (2SFCA) Method to Measure the Potential Spatial Accessibility of Healthcare Services. ISPRS Int. J. Geo-Inf. 2019, 8, 236. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.K. Role of GIS in Health Management Information System and Medical Plan: A Case Study of Gangtok area, Sikkim, India. Int. J. Environ. Geoinform. 2015, 2, 16–24. [Google Scholar] [CrossRef]
- Cockerham, W. International Encyclopedia of Public Health, 2nd ed.; Elsevier: Birmingham, UK, 2017; p. 414. [Google Scholar]
- Foley, R.; Charlton, M.; Fotheringham, S. GIS in Health and Social Care Planning. Available online: https://www.semanticscholar.org/ (accessed on 12 December 2019).
- Gong, H.; Simwanda, M.; Murayama, Y. An Internet-Based, IS Platform Providing Data for Visualization and Spatial Analysis of Urbanization in Major Asian and African Cities. ISPRS Int. J. Geo-Inf. 2017, 6, 257. [Google Scholar] [CrossRef] [Green Version]
- Singhasivanon, P.; Kidson, C.; Supavej, S. Mekong Malaria. Malaria, multi-drug resistance and economic development in the Greater Mekong sub-region of South-East Asia, incorporating geographical information systems databases. Southeast Asian J. Trop. Med. Public Health 1999, 30, 4. [Google Scholar]
- Pringle, D.; Johnson, H.; Cullen, C.; Boyle, E.; Doyle, D.; Brazil, J.; McKeown, P.; Staines, A.; Beaton, D.; McIntyre, M.; et al. Health Atlas Ireland: An Open-Source Mapping, Database and Statistical System; GeoComputation 2007; National University of Ireland: Maynooth, Ireland, 2008. [Google Scholar]
- Lu, X. A Framework of Web GIS Based Unified Public Health Information Visualization Platform. In Applications of Evolutionary Computation; Springer Science and Business Media LLC: Berlin, Germany, 2005; Volume 3482, pp. 256–265. [Google Scholar]
- Abdullahi, F.; Lawal, M.; Agushaka, J. Design and Implementation of A Web-Based Gis for Public Healthcare Decision Support System in Zaria Metropolis. Ijrras, 4(4), p. 1. Available online: https://core.ac.uk/download/pdf/25731372.pdf (accessed on 21 December 2019).
- Masimalai, P. GIS for rapid epidemiological mapping and health-care management with special reference to filariasis in India. Int. J. Med. Sci. Public Health 2015, 4, 1. [Google Scholar] [CrossRef]
- Moore, K.; Merritt, A.; Bobo, B.; Graham, A.; Kuhn, A. Kentucky Stroke Encounter Quality Improvement Project (SEQIP) Abstract 141: Using Geographic Information Systems (GIS) to Analyze Statewide Regional Data—A Feasibility Project from the Kentucky Stroke Encounter Quality Improvement Project (SEQIP). Circ. Cardiovasc. Qual. Outcomes 2019, 12, 1. [Google Scholar] [CrossRef]
- World Health Organization. Public Health Surveillance. Available online: https://www.who.int/topics/public_health_surveillance/en/ (accessed on 24 December 2019).
- Morens, D.M.; Fauci, A.S. Emerging Infectious Diseases: Threats to Human Health and Global Stability. PLoS Pathog. 2013, 9, e1003467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiafe, S.; Davenhall, B. Extending Disease Surveillance with GIS. ESRI. Available online: https://www.esri.com/news/arcuser/0405/disease_surveil1of2.html (accessed on 13 December 2019).
- Lee, L.M.; Teutsch, S.M.; Thacker, S.B.; Louis, M.E.S. Principles & Practice of Public Health Surveillance; Oxford University Press (OUP): Oxford, UK, 2010. [Google Scholar]
- Stallones, L.; Nuckols, J.R.; Berry, J.K. Surveillance around hazardous waste sites: GIS and reproductive outcomes. Environ. Res. 1992, 59, 81–92. [Google Scholar] [CrossRef]
- Law, D.; Wilfert, R. Infectious Disease Surveillance and Outbreak Investigation using GIS. Focus, Volume 5, p. 3. Available online: https://nciph.sph.unc.edu/focus/vol5/issue2/5-2Mapping_issue.pdf (accessed on 13 December 2019).
- ASTHO Organization Technologies for Vector-Borne Disease Surveillance. p. 3. Available online: https://astho.org/Programs/Environmental-Health/Natural-Environment/VBD-Tech-Surveillance-Scan/ (accessed on 13 December 2019).
- Kazmi, S.J.H.; Usery, E.L. Application of remote sensing and gis for the monitoring of diseases: A unique research agenda for geographers. Remote Sens. Rev. 2001, 20, 45–70. [Google Scholar] [CrossRef]
- Pam, D.D.; Omalu, I.C.J.; Akintola, A.A.; Dan, A.Y.; Kalesanwo, A.O.; Babagana, M.; Muhammad, S.A.; Ocha, I.M.; Adeniyi, K.A. The Role of GIS And Remote Sensing in the Control of Malaria. Online J Health Allied Scs. 2017, 16, 7. Available online: http://www.ojhas.org/issue63/2017-3-7.html (accessed on 26 May 2020).
- Kalluri, S.; Gilruth, P.; Rogers, D.; Szczur, M. Surveillance of Arthropod Vector-Borne Infectious Diseases Using Remote Sensing Techniques: A Review. PLoS Pathog. 2007, 3, e116. [Google Scholar] [CrossRef]
- Jeanne, I.; Chambers, L.E.; Kazazic, A.; Russell, T.L.; Bobogare, A.; Bugoro, H.; Otto, F.; Fafale, G.; Amjadali, A. Mapping a Plasmodium transmission spatial suitability index in Solomon Islands: A malaria monitoring and control tool. Malar. J. 2018, 17, 381. [Google Scholar] [CrossRef] [PubMed]
- Mandyata, C.B.; Olowski, L.K.; Mutale, W. Challenges of implementing the integrated disease surveillance and response strategy in Zambia: A health worker perspective. BMC Public Health 2017, 17, 746. [Google Scholar] [CrossRef] [Green Version]
- Rahman, S.-U.; Smith, D.K. Use of location-allocation models in health service development planning in developing nations. Eur. J. Oper. Res. 2000, 123, 437–452. [Google Scholar] [CrossRef]
- Afshari, Q.P.H.; Peng, H.A.A.Q. Challenges and Solutions for Location of Healthcare Facilities. Ind. Eng. Manag. 2014, 3. [Google Scholar] [CrossRef]
- Kotavaara, O.; Pohjosenperä, T.; Juga, J.; Rusanen, J. Accessibility in designing centralised warehousing: Case of health care logistics in Northern Finland. Appl. Geogr. 2017, 84, 83–92. [Google Scholar] [CrossRef]
- Abdelkarim, A. Integration of Location-Allocation and Accessibility Models in GIS to Improve Urban Planning for Health Services in Al-Madinah Al-Munawwarah, Saudi Arabia. J. Geogr. Inf. Syst. 2019, 11, 633–662. [Google Scholar] [CrossRef] [Green Version]
- Polo, G.; Acosta, C.M.; Ferreira, F.; Dias, R.A. Location-Allocation and Accessibility Models for Improving the Spatial Planning of Public Health Services. PLoS ONE 2015, 10, e0119190. [Google Scholar] [CrossRef] [PubMed] [Green Version]













© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khashoggi, B.F.; Murad, A. Issues of Healthcare Planning and GIS: A Review. ISPRS Int. J. Geo-Inf. 2020, 9, 352. https://doi.org/10.3390/ijgi9060352
Khashoggi BF, Murad A. Issues of Healthcare Planning and GIS: A Review. ISPRS International Journal of Geo-Information. 2020; 9(6):352. https://doi.org/10.3390/ijgi9060352
Chicago/Turabian StyleKhashoggi, Bandar Fuad, and Abdulkader Murad. 2020. "Issues of Healthcare Planning and GIS: A Review" ISPRS International Journal of Geo-Information 9, no. 6: 352. https://doi.org/10.3390/ijgi9060352
APA StyleKhashoggi, B. F., & Murad, A. (2020). Issues of Healthcare Planning and GIS: A Review. ISPRS International Journal of Geo-Information, 9(6), 352. https://doi.org/10.3390/ijgi9060352