
Medicinal Plants for Rich People vs. Medicinal Plants for Poor People: A Case Study from the Peruvian Andes





Abstract
:1. Introduction
2. Results
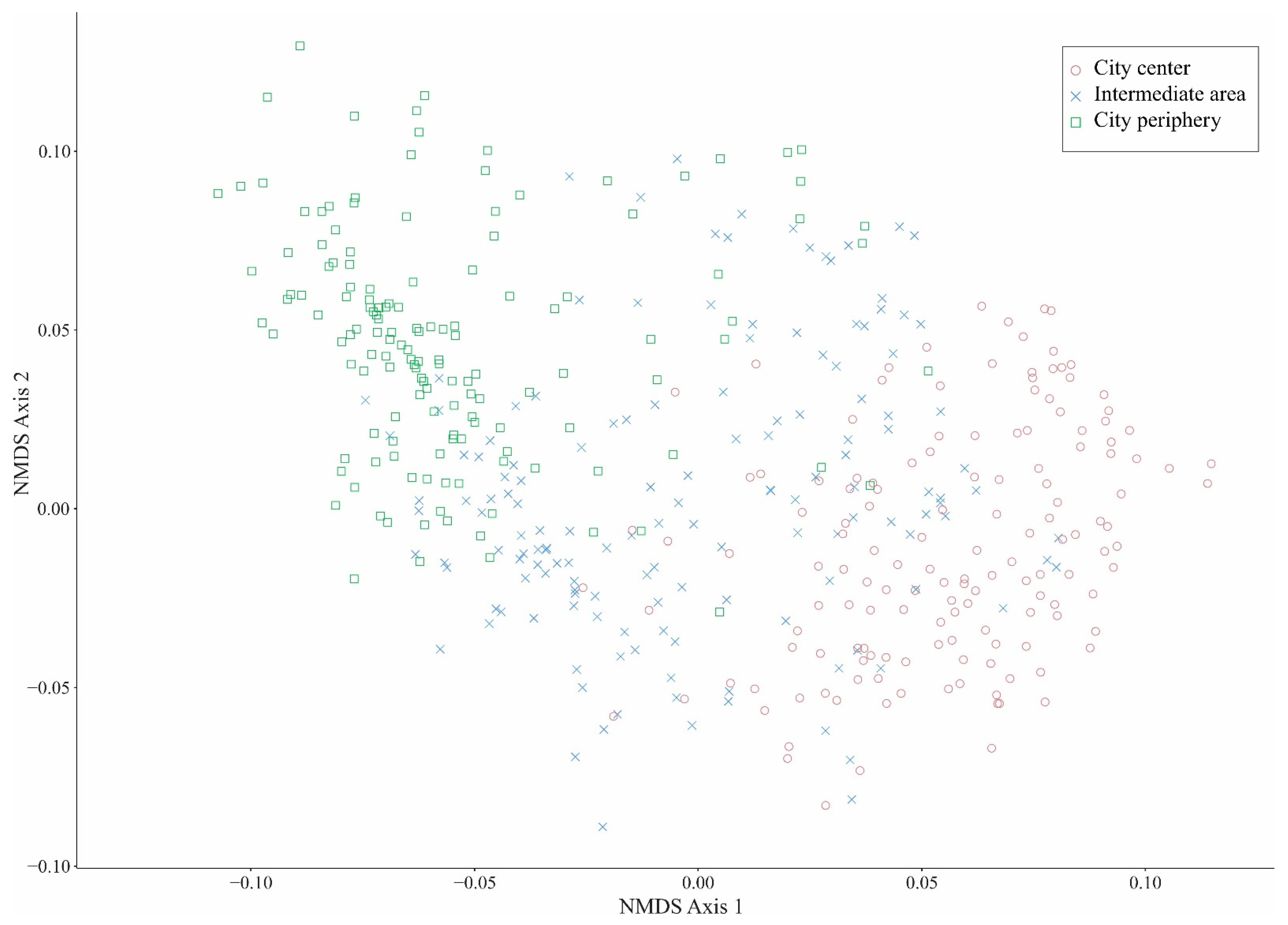
2.1. Distribution of TK of Medicinal Plants across City Areas
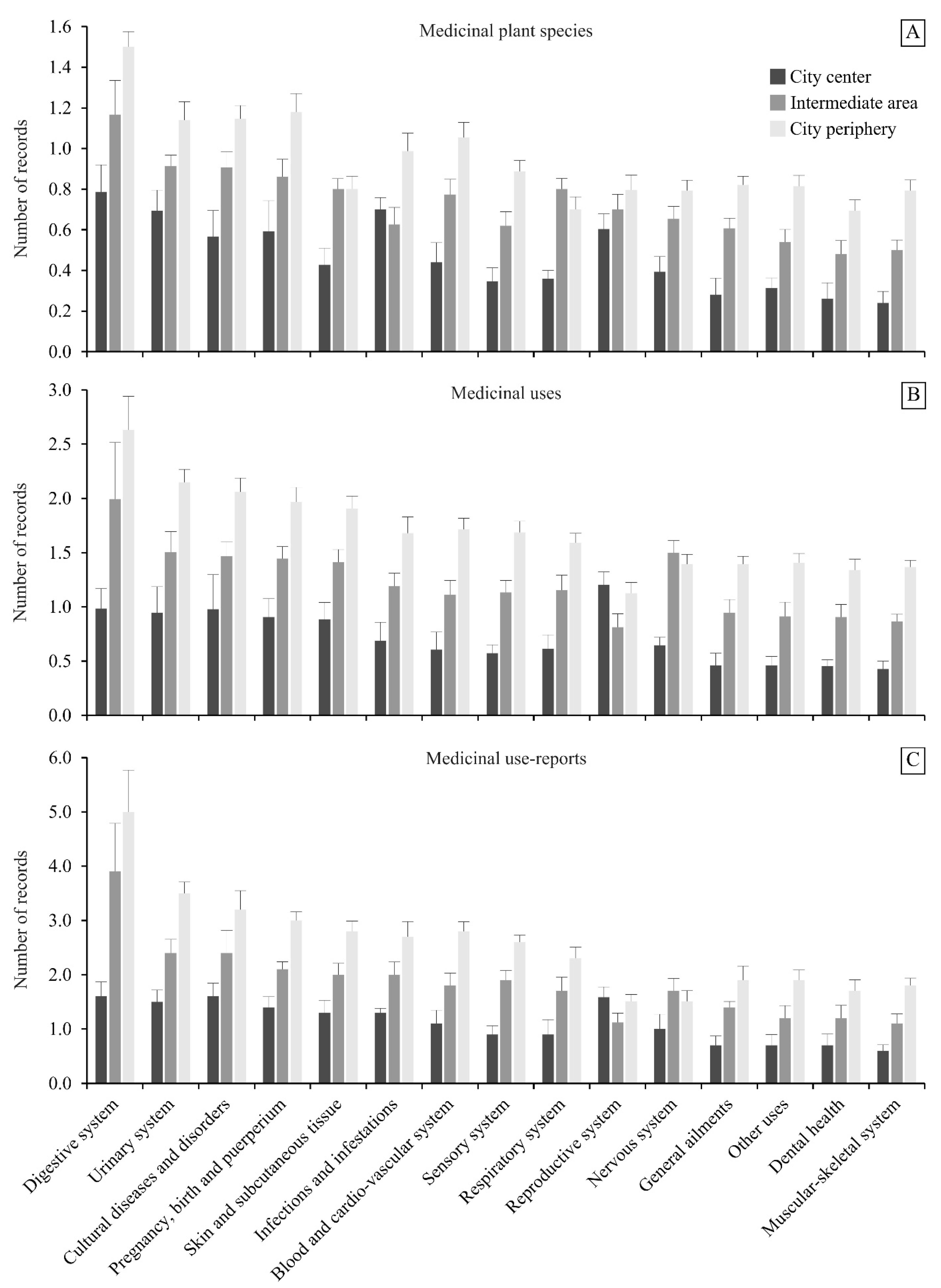
2.2. Comparison of the Most Used Medicinal Species and Medical Indications across the City Areas
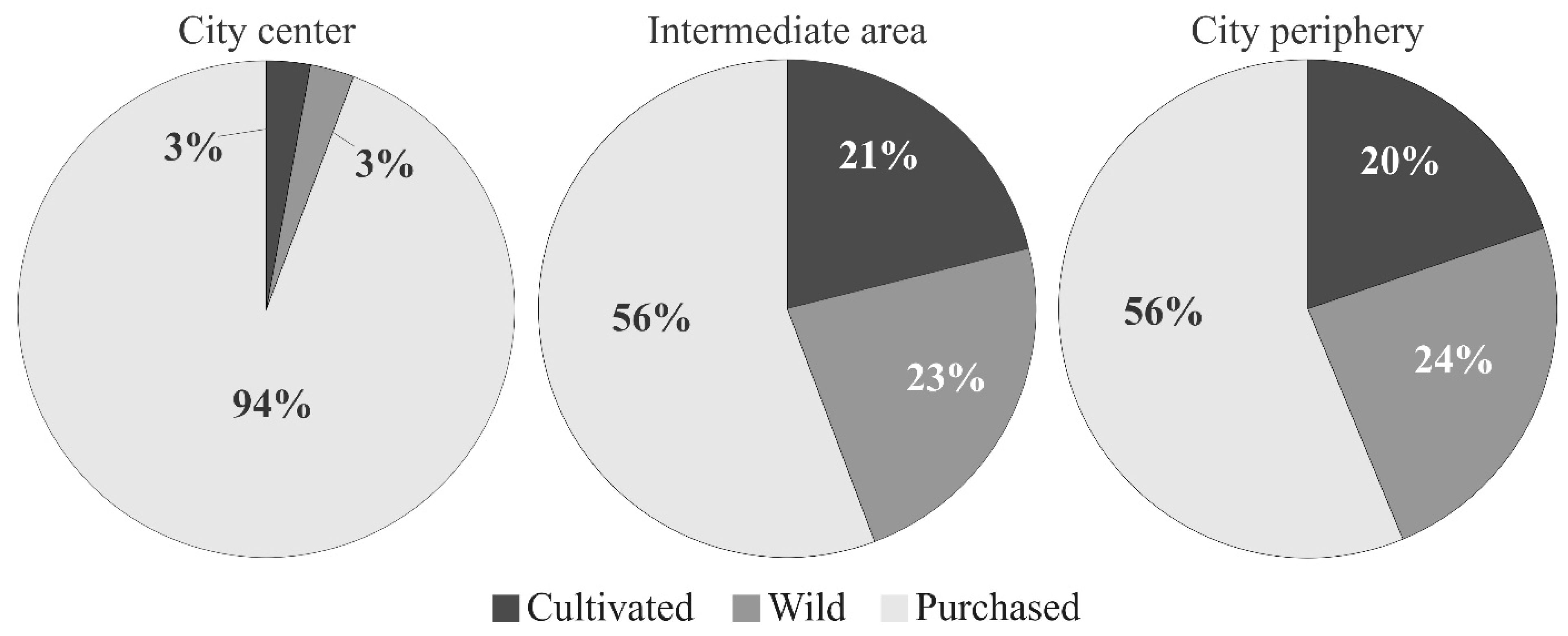
2.3. Acquisition of Medicinal Plant Species across the Three City Areas
3. Discussion
3.1. Distribution of the TK of Medicinal Plants in Chachapoyas
3.2. Cultural Significance of Medicinal Plants in Chachapoyas
3.3. Different Modes of Acquisition of Medicinal Plants in Chachapoyas
4. Materials and Methods
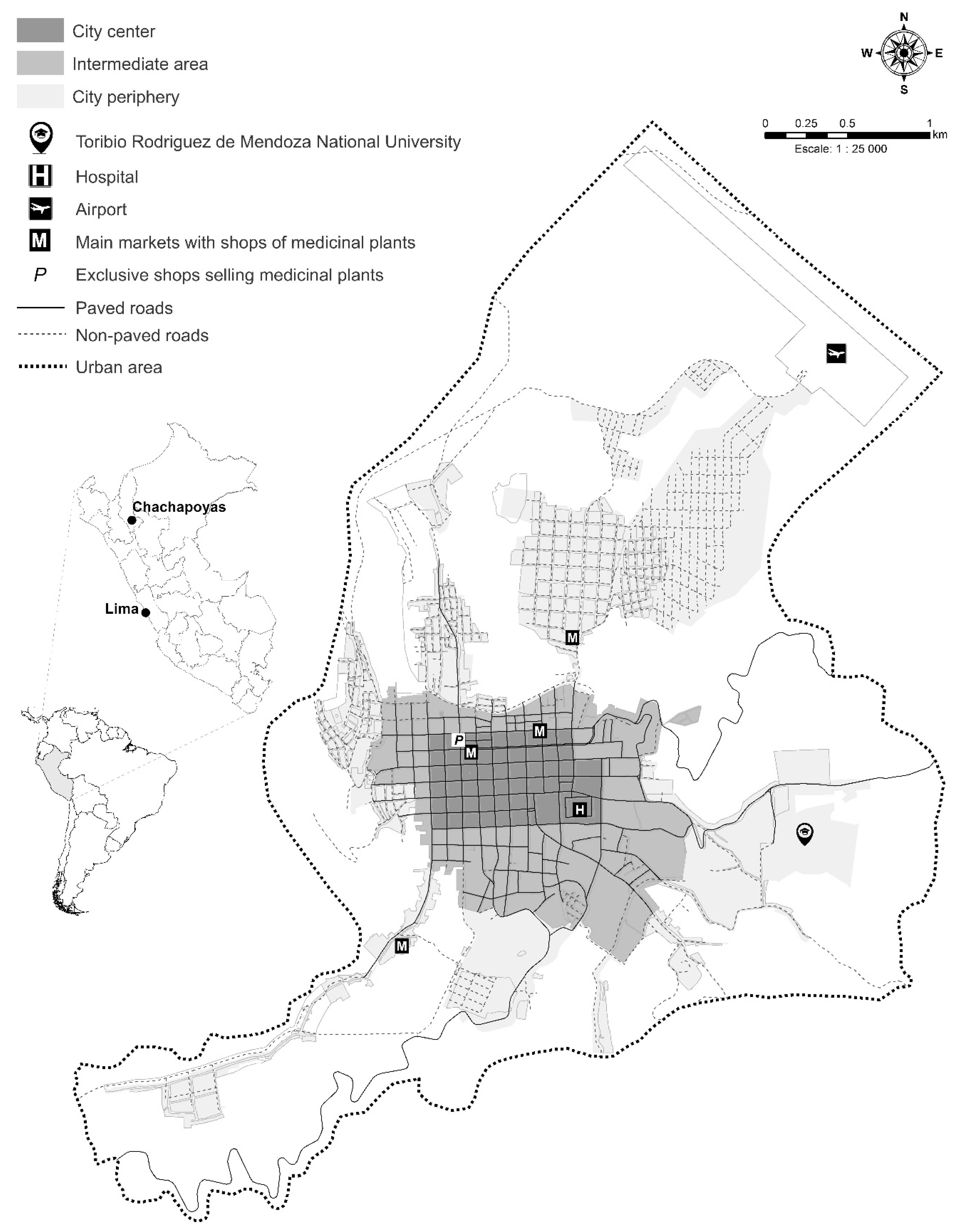
4.1. Study Area and City Areas
4.2. Data Collection
4.3. Data Analysis
4.4. Ethics Statement
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wekesa, B.W.; Steyn, G.S.; Otieno, F.F. A review of physical and socio-economic characteristics and intervention approaches of informal settlements. Habitat Int. 2011, 35, 238–245. [Google Scholar] [CrossRef]
- Williamson, J.G. Migration and city growth during industrial revolutions. In Urban Agglomeration and Economic Growth; Giersch, H., Ed.; Springer: Berlin, Germany, 1995; pp. 79–104. [Google Scholar]
- Konteh, F.H. Urban sanitation and health in the developing world: Reminiscing the nineteenth century industrial nations. Health Place 2009, 15, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Perz, S.G. Migrant characteristics and land-use/land-cover change in the Pan-Amazon Basin: A comparative analysis of Brazil, Bolivia, Ecuador and Perú. In The Social Ecology of Tropical Forests: Migration, Population and Frontiers; De Jong, W., Tuck-Po, L., Ken-ichi, A., Eds.; Kyoto University Press: Kyoto, Japan, 2006; pp. 25–53. [Google Scholar]
- Parry, L.; Day, B.; Amaral, S.; Peres, C.A. Drivers of rural exodus from Amazonian headwaters. Popul. Environ. 2010, 32, 137–176. [Google Scholar] [CrossRef]
- Sakay, C.; Sanoni, P.; Deng, T.H. Rural to urban squatter settlements: The micro model of generational self-help housing in Lima-Peru. Procedia Eng. 2011, 21, 473–480. [Google Scholar] [CrossRef] [Green Version]
- Grau, H.R.; Aide, T.M. Are rural-urban migration and sustainable development compatible in mountain systems? Mt. Res. Dev. 2007, 27, 119–123. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zhou, W.; Ouyang, Z. Forty years of urban expansion in Beijing: What is the relative importance of physical, socioeconomic, and neighborhood factors? Appl. Geogr. 2013, 38, 1–10. [Google Scholar] [CrossRef]
- Muñoz-Carrera, Ó.M. Gentrificación, segregación y reestructuración social en Madrid. Rev. Direito Cid. 2014, 6, 180–207. [Google Scholar]
- Grabkowska, M.; Frankowski, J. Close to the city centre, close to the university. Are there symptoms of studentification in Gdańsk, Poland? In Bulletin of Geography. Socio-Economic Series; Szymańska, D., Chodkowska-Miszczuk, J., Eds.; Nicolaus Copernicus University: Torún, Perú, 2016; pp. 73–83. [Google Scholar]
- Aguilar, A.G.; Ward, P.M. Globalization, regional development, and mega-city expansion in Latin America: Analyzing Mexico City’s peri-urban hinterland. Cities 2003, 20, 3–21. [Google Scholar] [CrossRef]
- INEI (Instituto Nacional de Estadística e Informática). Encuesta Nacional de Hogares del Perú 2015 (ENAHO); INEI: Lima, Perú, 2015; pp. 1–107. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1369/libro.pdf (accessed on 6 May 2020).
- Pardo-de-Santayana, M.; Macía, M.J. Biodiversity: The benefits of traditional knowledge. Nature 2015, 518, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.C. Medicinal plants, conservation and livelihoods. Biodivers. Conserv. 2004, 13, 1477–1517. [Google Scholar] [CrossRef]
- Neulinger, K.; Vogl, C.R.; Alayón-Gamboa, J.A. Plant species and their uses in homegardens of migrant Maya and Mestizo smallholder farmers in Calakmul, Campeche, Mexico. J. Ethnobiol. 2013, 33, 105–124. [Google Scholar] [CrossRef]
- Gaoue, O.G.; Coe, M.A.; Bond, M.; Hart, G.; Seyler, B.C.; McMillen, H. Theories and major hypotheses in ethnobotany. Econ. Bot. 2017, 71, 269–287. [Google Scholar] [CrossRef]
- Ceuterick, M.; Vandebroek, I.; Torry, B.; Pieroni, A. Cross-cultural adaptation in urban ethnobotany: The Colombian folk pharmacopoeia in London. J. Ethnopharmacol. 2008, 120, 342–359. [Google Scholar] [CrossRef] [PubMed]
- Vandebroek, I.; Balick, M.J. Globalization and loss of plant knowledge: Challenging the paradigm. PLoS ONE 2012, 7, e37643. [Google Scholar] [CrossRef]
- Ladio, A.H.; Acosta, M. Urban medicinal plant use: Do migrant and non-migrant populations have similar hybridisation processes? J. Ethnopharmacol. 2019, 234, 290–305. [Google Scholar] [CrossRef] [PubMed]
- Vandebroek, I. The dual intracultural and intercultural relationship between medicinal plant knowledge and consensus. Econ. Bot. 2010, 64, 303–317. [Google Scholar] [CrossRef]
- Corroto, F.; Torres, O.A.G.; Macía, M.J. Different patterns in medicinal plant use along an elevational gradient in northern Peruvian Andes. J. Ethnopharmacol. 2019, 239, 111924. [Google Scholar] [CrossRef] [PubMed]
- Godoy, R.; Reyes-García, V.; Byron, E.; Leonard, W.R.; Vadez, V. The effect of market economies on the well-being of indigenous peoples and on their use of renewable natural resources. Annu. Rev. Anthropol. 2005, 34, 121–138. [Google Scholar] [CrossRef] [Green Version]
- Andriamparany, J.N.; Brinkmann, K.; Jeannoda, V.; Buerkert, A. Effects of socio-economic household characteristics on traditional knowledge and usage of wild yams and medicinal plants in the Mahafaly region of south-western Madagascar. J. Ethnobiol. Ethnomed. 2014, 10, 82. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Nicolás, M.; Vibrans, H.; Romero-Manzanares, A.; Saynes-Vásquez, A.; Luna-Cavazos, M.; Flores-Cruz, M.; Lira-Saade, R. Patterns of knowledge and use of medicinal plants in Santiago Camotlán, Oaxaca, Mexico. Econ. Bot. 2017, 71, 209–223. [Google Scholar] [CrossRef]
- Bussmann, R.W.; Sharon, D.; Vandebroek, I.; Jones, A.; Revene, Z. Health for sale: The medicinal plant markets in Trujillo and Chiclayo, Northern Peru. J. Ethnobiol. Ethnomed. 2007, 3, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bussmann, R.W.; Paniagua-Zambrana, N.; Chamorro, M.R.; Moreira, N.M.; Negri, M.L.R.C.; Olivera, J. Peril in the market-classification and dosage of species used as anti-diabetics in Lima, Peru. J. Ethnobiol. Ethnomed. 2013, 9, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macía, M.J.; García, E.; Vidaurre, P.J. An ethnobotanical survey of medicinal plants commercialized in the markets of La Paz and El Alto, Bolivia. J. Ethnopharmacol. 2005, 97, 337–350. [Google Scholar] [CrossRef]
- Quintero, S.E.G.; Bernal Lizarazú, M.C.; Morales Robayo, A.; Lobo, P.; Zuled, A.; Gamba Molano, L. Traditional use of medicinal plants in markets Bogotá, DC. Nova 2015, 13, 73–80. [Google Scholar]
- Tinitana, F.; Rios, M.; Romero-Benavides, J.C.; de la Cruz Rot, M.; Pardo-de-Santayana, M. Medicinal plants sold at traditional markets in southern Ecuador. J. Ethnobiol. Ethnomed. 2016, 12, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giraldo, D.; Baquero, E.; Bermúdez, A.; Oliveira-Miranda, M.A. Caracterización del comercio de plantas medicinales en los mercados populares de Caracas, Venezuela. Acta Botánica Venezuélica 2009, 32, 267–301. [Google Scholar]
- Gómez-Estrada, H.; Díaz-Castillo, F.; Franco-Ospina, L.; Mercado-Camargo, J.; Guzmán-Ledezma, J.; Medina, J.D.; Gaitán-Ibarra, R. Folk medicine in the northern coast of Colombia: An overview. J. Ethnobiol. Ethnomed. 2011, 7, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurrell, J.A.; Puentes, J.P.; Arenas, P.M. Medicinal plants with cholesterol-lowering effect marketed in the Buenos Aires-La Plata conurbation, Argentina: An urban Ethnobotany study. Ethnobiol. Conserv. 2015, 4, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Balick, M.J.; Kronenberg, F.; Ososki, A.L.; Reiff, M.; Fugh-Berman, A.; Roble, M.; Lohr, P.; Atha, D. Medicinal plants used by Latino healers for women’s health conditions in New York City. Econ. Bot. 2000, 54, 344–357. [Google Scholar] [CrossRef]
- Van Andel, T.; Westers, P. Why Surinamese migrants in the Netherlands continue to use medicinal herbs from their home country. J. Ethnopharmacol. 2010, 127, 694–701. [Google Scholar] [CrossRef]
- Ellena, R.; Quave, C.L.; Pieroni, A. Comparative medical ethnobotany of the Senegalese community living in Turin (Northwestern Italy) and in Adeane (Southern Senegal). Evid. Based Complementary Altern. Med. 2012, 30. [Google Scholar] [CrossRef] [Green Version]
- Shackleton, C.M.; Shackleton, S.E. Household wealth status and natural resource use in the Kat River valley, South Africa. Ecol. Econ. 2006, 57, 306–317. [Google Scholar] [CrossRef]
- Cocks, M.L.; Bangay, L.; Shackleton, C.M.; Wiersum, F.K. Rich man poor man-inter-household and community factors influencing the use of wild plant resources amongst rural households in South Africa. Int. J. Sustain. Dev. World Ecol. 2008, 15, 198–210. [Google Scholar] [CrossRef]
- Case, R.J.; Pauli, G.F.; Soejarto, D.D. Factors in maintaining indigenous knowledge among ethnic communities of Manus Island. Econ. Bot. 2005, 59, 356–365. [Google Scholar] [CrossRef]
- Almeida, C.D.F.C.B.; Ramos, M.A.; Amorim, E.L.C.; Albuquerque, U.P. A comparison of knowledge about medicinal plants for three rural communities in the semi-arid region of northeast of Brazil. J. Ethnopharmacol. 2009, 127, 674–684. [Google Scholar] [CrossRef]
- Arruda, H.L.S.; dos Santos, J.F.O.; Albuquerque, U.P.; Ramos, M.A. Influence of socioeconomic factors on the knowledge and consumption of firewood in the Atlantic Forest of northeast Brazil. Econ. Bot. 2019, 73, 1–12. [Google Scholar] [CrossRef]
- Inta, A.; Shengji, P.; Balslev, H.; Wangpakapattanawong, P.; Trisonthi, C. A comparative study on medicinal plants used in Akha’s traditional medicine in China and Thailand, cultural coherence or ecological divergence? J. Ethnopharmacol. 2008, 116, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Martínez, G.J.; Luján, M.C. Medicinal plants used for traditional veterinary in the Sierras de Córdoba (Argentina): An ethnobotanical comparison with human medicinal uses. J. Ethnobiol. Ethnomed. 2011, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Hossan, S.; Agarwala, B.; Sarwar, S.; Karim, M.; Jahan, R.; Rahmatullah, M. Traditional use of medicinal plants in Bangladesh to treat urinary tract infections and sexually transmitted diseases. Ethnobot. Res. Appl. 2010, 8, 61–74. [Google Scholar] [CrossRef] [Green Version]
- Lyon, L.M.; Hardesty, L.H. Quantifying medicinal plant knowledge among non–specialist Antanosy villagers in southern Madagascar. Econ. Bot. 2012, 66, 1–11. [Google Scholar] [CrossRef]
- Ramet, A.; Benyei, P.; Parada, M.; Aceituno-Mata, L.; García-del-Amo, D.; Reyes-García, V. Grandparents’ proximity and children’s traditional medicinal plant knowledge: Insights from two schools in intermediate-rural Spain. J. Ethnobiol. 2018, 38, 187–204. [Google Scholar] [CrossRef]
- Vandebroek, I. Intercultural health and ethnobotany: How to improve healthcare for underserved and minority communities? J. Ethnopharmacol. 2013, 148, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Rai, P.K.; Lalramnghinglova, H. Ethnomedicinal plant resources of Mizoram, India: Implication of traditional knowledge in health care system. Ethnobot. Leafl. 2010, 14, 274–305. [Google Scholar]
- Campos, J.L.A.; de Lima Araújo, E.; Gaoue, O.G.; Albuquerque, U.P. Socioeconomic factors and cultural changes explain the knowledge and use of Ouricuri Palm (Syagrus coronata) by the Fulni ô indigenous people of Northeast Brazil. Econ. Bot. 2019, 73, 187–199. [Google Scholar] [CrossRef]
- Brown, K. The use of medicinal plants in Rio de Janeiro’s urban periphery: An analysis of communities’ engagements with policies. J. Ethnobiol. 2016, 36, 861–880. [Google Scholar] [CrossRef]
- Hammond, G.B.; Fernández, I.D.; Villegas, L.F.; Vaisberg, A.J. A survey of traditional medicinal plants from the Callejón de Huaylas, Department of Ancash, Perú. J. Ethnopharmacol. 1998, 61, 17–30. [Google Scholar] [CrossRef]
- De la Cruz, H.; Vilcapoma, G.; Zevallos, P.A. Ethnobotanical study of medicinal plants used by the Andean people of Canta, Lima, Peru. J. Ethnopharmacol. 2007, 111, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Tello-Cerón, G.; Flores Pimentel, M.; Gómez Galarza, V. Uso de las plantas medicinales del distrito de Quero, Jauja, región Junín, Perú. Ecol. Apl. 2019, 18, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Signorini, M.A.; Piredda, M.; Bruschi, P. Plants and traditional knowledge: An ethnobotanical investigation on Monte Ortobene (Nuoro, Sardinia). J. Ethnobiol. Ethnomed. 2009, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrió, E.; Vallès, J. Ethnobotany of medicinal plants used in eastern Mallorca (Balearic Islands, Mediterranean Sea). J. Ethnopharmacol. 2012, 141, 1021–1040. [Google Scholar] [CrossRef]
- Brandt, R.; Mathez-Stiefel, S.L.; Lachmuth, S.; Hensen, I.; Rist, S. Knowledge and valuation of Andean agroforestry species: The role of sex, age, and migration among members of a rural community in Bolivia. J. Ethnobiol. Ethnomed. 2013, 9, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González, J.A.; García-Barriuso, M.; Amich, F. Ethnobotanical study of medicinal plants traditionally used in the Arribes del Duero, western Spain. J. Ethnopharmacol. 2010, 131, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Urso, V.; Signorini, M.A.; Tonini, M.; Bruschi, P. Wild medicinal and food plants used by communities living in Mopane woodlands of southern Angola: Results of an ethnobotanical field investigation. J. Ethnopharmacol. 2016, 177, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Bulut, G.; Haznedaroğlu, M.Z.; Doğan, A.; Koyu, H.; Tuzlac, E. An ethnobotanical study of medicinal plants in Acipayam (Denizli-Turkey). J. Herb. Med. 2017, 10, 64–81. [Google Scholar] [CrossRef]
- Gonzales, M.; Malpartida, S.B.; Santiago, H.B.; Jullian, V.; Bourdy, G. Hot and cold: Medicinal plant uses in Quechua speaking communities in the high Andes (Callejón de Huaylas, Ancash, Perú). J. Ethnopharmacol. 2014, 155, 1093–1117. [Google Scholar] [CrossRef]
- Hersch-Martínez, P. Commercialization of wild medicinal plants from southwest Puebla, Mexico. Econ. Bot. 1995, 49, 197–206. [Google Scholar] [CrossRef]
- Van Andel, T.; Myren, B.; Van Onselen, S. Ghana’s herbal market. J. Ethnopharmacol. 2012, 140, 368–378. [Google Scholar] [CrossRef]
- Castillo-Vera, H.; Cochachin, E.; Albán, J. Plantas comercializadas por herbolarios en el mercado del distrito de Cajabamba (Cajamarca, Perú). Boletín Latinoam. Caribe Plantas Med. Aromáticas 2017, 16, 303–318. [Google Scholar]
- Sõukand, R.; Hrynevich, Y.; Vasilyeva, I.; Prakofjewa, J.; Vnukovich, Y.; Paciupa, J.; Hlushko, A.; Knureva, Y.; Litvinava, Y.; Vyskvarka, S.; et al. Multi-functionality of the few: Current and past uses of wild plants for food and healing in Liubań region, Belarus. J. Ethnobiol. Ethnomed. 2017, 13, 1–42. [Google Scholar] [CrossRef] [Green Version]
- Bussmann, R.W.; Sharon, D. Traditional medicinal plant use in Northern Peru: Tracking two thousand years of healing culture. J. Ethnobiol. Ethnomed. 2006, 2, 47. [Google Scholar] [CrossRef] [Green Version]
- Thomas, E.; Vandebroek, I.; Goetghebeur, P.; Sanca, S.; Arrázola, S.; Van Damme, P. The relationship between plant use and plant diversity in the Bolivian Andes, with special reference to medicinal plant use. Hum. Ecol. 2008, 36, 861–879. [Google Scholar] [CrossRef]
- Oblitas, G.; Hernández-Córdova, G.; Chiclla, A.; Antich-Barrientos, M.; Corihuamán-Cusitito, L.; Romaní, F. Empleo de plantas medicinales en usuarios de dos hospitales referenciales del Cusco, Perú. Rev. Peru. Med. Exp. Salud Pública 2013, 30, 64–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavender, A.P.; Albán, M. The use of magical plants by curanderos in the Ecuador highlands. J. Ethnobiol. Ethnomed. 2009, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luziatelli, G.; Sørensen, M.; Theilade, I.; Mølgaard, P. Asháninka medicinal plants: A case study from the native community of Bajo Quimiriki, Junín, Peru. J. Ethnobiol. Ethnomed. 2010, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandão, M.D.G.L.; Cosenza, G.P.; Pereira, F.L.; Vasconcelos, A.S.; Fagg, C.W. Changes in the trade in native medicinal plants in Brazilian public markets. Environmental monitoring and assessment. Environ. Monit. Assess. 2013, 185, 7013–7023. [Google Scholar] [CrossRef]
- Furlan, V.; Kujawska, M.; Hilgert, N.I.; Pochettino, M.L. To what extent are medicinal plants shared between country home gardens and urban ones? A case study from Misiones, Argentina. Pharm. Biol. 2016, 54, 1628–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SENAMHI (Servicio Nacional de Meteorología e Hidrología del Perú). Reporte Mensual de Meteorología y Climatología; Lima, Perú. 2017. Available online: http://www.senamhi.gob.pe/?p=descarga-datos-hidrometeorologicos/ (accessed on 12 June 2020).
- Rascón, J.; Angeles, W.G.; Oliva, M.; Huatangari, L.Q.; Gurbillón, M.A.B. Determinación de las épocas lluviosas y secas en la ciudad de Chachapoyas para el periodo de 2014–2018. Rev. De Climatol. 2020, 20, 15–28. [Google Scholar]
- Valqui, J.; Ziemendorff, M. Vestigios de una lengua originaria en el territorio de la cultura chachapoya. Letras 2016, 87, 5–32. [Google Scholar] [CrossRef]
- Corroto, F.; Gamarra, O.; Barboza, E. Multivariate assessment of water quality in the Utcubamba Basin (Peru). Tecnol. Cienc. Agua 2018, 9, 33–57. [Google Scholar] [CrossRef]
- Briceño, N.B.R.; Castillo, E.B.; Torres, O.A.G.; Oliva, M.; Tafur, D.L.; Gurbillón, M.Á.B.; Corroto, F.; Salas, R.; Rascón, J. Morphometric prioritization, fluvial classification, and hydrogeomorphological quality in high Andean livestock micro-watersheds in northern Peru. ISPRS Int. J. Geoinf. 2020, 9, 305–330. [Google Scholar] [CrossRef]
- INEI (Instituto Nacional de Estadística e Informática). Resultados Definitivos de los Censos Nacionales 2017; INEI: Lima, Perú, 2017; pp. 1–837. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1544/00TOMO_01.pdf (accessed on 23 February 2020).
- MPCh (Municipalidad Provincial de Chachapoyas). Plan de Desarrollo Urbano de la Ciudad de Chachapoyas. Volumen 1, Resumen Ejecutivo; Ministerio de Vivienda, Construcción y Saneamiento: Lima, Perú, 2013; pp. 1–30. Available online: https://docplayer.es/81432723-Resumen-ejecutivo-pdu-chachapoyas-plan-de-plan-de-desarrollo-urbano-de-la-ciudad-de-chachapoyas-resumen-ejecutivo.html (accessed on 12 January 2020).
- Sánchez-Aguilar, A. Migraciones Internas en el Perú. Misión en el Perú; Organización Internacional para las Migraciones: Lima, Perú, 2015; pp. 1–180. Available online: https://peru.iom.int/sites/default/files/Documentos/Migraciones_Internas.pdf (accessed on 7 June 2020).
- The Plant List—A Working List of all Known Plant Species. 2013. Available online: http://www.theplantlist.org. (accessed on 9 January 2020).
- Chase, M.W.; Christenhusz, M.J.M.; Fay, M.F.; Byng, J.W.; Judd, W.S.; Soltis, D.E.; Mabberley, D.J.; Sennikov, A.N.; Soltis, P.S.; Stevens, P.F. An update of the angiosperm phylogeny group classification for the orders and families of flowering plants: APG IV. Bot. J. Linn. Soc. 2016, 181, 1–20. [Google Scholar] [CrossRef] [Green Version]
- WONCA (World Organization of National Colleges, Academies and Academic Associations of General Practitioners/Family Physicians). ICPC-2-R: International Classification of Primary Care; Oxford University Press: Oxford, UK, 2005; pp. 1–208. ISBN 10:0198568576. [Google Scholar]
- Macía, M.J.; Armesilla, P.J.; Cámara-Leret, R.; Paniagua-Zambrana, N.; Villalba, S.; Balslev, H.L.; Pardo-de-Santayana, M. Palm uses in northwestern South America: A quantitative review. Bot. Rev. 2011, 77, 462–570. [Google Scholar] [CrossRef]
- Gruca, M.; Cámara-Leret, R.; Macía, M.J.; Balslev, H. New categories for traditional medicine in the economic botany data collection standard. J. Ethnopharmacol. 2014, 155, 1388–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Development Core Team. R: A Language and Environment for Statistical Computing. Version 3.6.3; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Tardío, J.; Pardo-de-Santayana, M. Cultural importance indices: A comparative analysis based on the useful wild plants of Southern Cantabria (Northern Spain). Econ. Bot. 2008, 62, 24–39. [Google Scholar] [CrossRef]
- SCBD (Secretariat of the Convention on Biological Diversity). Nagoya Protocol on Access to Genetic Resources and the Fair and Equitable Sharing of Benefits Arising from their Utilization to the Convention on Biological Diversity; Secretariat of the Convention on Biological Diversity: Montreal, QC, Canada, 2011; pp. 1–15. Available online: https://www.cbd.int/abs/doc/protocol/nagoya-protocol-en.pdf (accessed on 23 March 2020).
- SCBD (Secretariat of the Convention on Biological Diversity). Bonn Guidelines on Access to Genetic Resources and Fair and Equitable Sharing of the Benefits Arising out of Their Utilization; Secretariat of the Convention on Biological Diversity: Montreal, QC, Canada, 2002; pp. 1–26. Available online: https://www.cbd.int/doc/publications/cbd-bonn-gdls-en.pdf (accessed on 22 March 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Species | Family | Status | City Center | Intermediate Area | City Periphery | Whole City |
|---|---|---|---|---|---|---|
| Minthostachys mollis (Benth.) Griseb. (FC791) | Lamiaceae | Native | 0.40 | 0.75 | 0.92 | 0.69 |
| Matricaria recutita L. (FC752) | Compositae | Cultivated | 0.33 | 0.80 | 0.89 | 0.67 |
| Citrus limon (L.) Osbeck (FC888) | Rutaceae | Cultivated | 0.35 | 0.27 | 0.47 | 0.36 |
| Origanum vulgare L. (FC790) | Lamiaceae | Cultivated | 0.27 | 0.30 | 0.50 | 0.36 |
| Plantago major L. (FC861) | Plantaginaceae | Naturalized | 0.19 | 0.39 | 0.46 | 0.35 |
| Equisetum bogotense Kunth (FC775) | Equisetaceae | Native | 0.10 | 0.32 | 0.46 | 0.29 |
| Malus domestica Borkh. (FC878) | Rosaceae | Cultivated | 0.11 | 0.44 | 0.27 | 0.27 |
| Bixa orellana L. (FC717) | Bixaceae | Native | 0.24 | 0.23 | 0.30 | 0.26 |
| Ruta chalepensis L. (FC892) | Rutaceae | Cultivated | 0.22 | 0.17 | 0.35 | 0.25 |
| Zea mays L. (FC870) | Poaceae | Cultivated | 0.07 | 0.35 | 0.31 | 0.24 |
| Mentha spicata L. (FC788) | Lamiaceae | Cultivated | 0.17 | 0.22 | 0.32 | 0.24 |
| Aloe vera (L.) Burm. f. (FC923) | Xanthorrhoeaceae | Cultivated | 0.14 | 0.14 | 0.39 | 0.22 |
| Chenopodium ambrosioides L. (FC685) | Amaranthaceae | Naturalized | 0.13 | 0.24 | 0.29 | 0.22 |
| Piper acutifolium Ruiz & Pav. (FC860) | Piperaceae | Native | 0.09 | 0.24 | 0.33 | 0.22 |
| Erythroxylum coca Lam. (FC776) | Erythroxylaceae | Cultivated | 0.18 | 0.14 | 0.28 | 0.20 |
| Solanum lycopersicum L. (FC912) | Solanaceae | Cultivated | 0.11 | 0.14 | 0.27 | 0.17 |
| Capsicum pubescens Ruiz & Pav. (FC903) | Solanaceae | Cultivated | 0.07 | 0.21 | 0.23 | 0.17 |
| Brassica oleracea L. var. acephala DC. (FC720) | Brassicaceae | Cultivated | 0.15 | 0.18 | 0.16 | 0.16 |
| Eucalyptus globulus Labill. (FC842) | Myrtaceae | Cultivated | 0.06 | 0.16 | 0.27 | 0.16 |
| Tagetes filifolia Lag. (FC736) | Compositae | Native | 0.13 | 0.16 | 0.20 | 0.16 |
| Petroselinum crispus (Mill.) Fuss (FC701) | Apiaceae | Cultivated | 0.13 | 0.11 | 0.24 | 0.16 |
| Desmodium molliculum (Kunth) DC. (FC815) | Leguminosae | Native | 0.03 | 0.19 | 0.25 | 0.16 |
| Syzygium aromaticum (L.) Merr. & L.M. Perry (FC841) | Myrtaceae | Cultivated | 0.05 | 0.20 | 0.21 | 0.15 |
| Carica papaya L. (FC729) | Caricaceae | Cultivated | 0.06 | 0.26 | 0.12 | 0.15 |
| Musa acuminata Colla (FC839) | Musaceae | Cultivated | 0.04 | 0.27 | 0.13 | 0.15 |
| Cyclanthera pedata (L.) Schard. (FC768) | Cucurbitaceae | Native | 0.01 | 0.16 | 0.25 | 0.14 |
| Citrus aurantiifolia Risso (FC887) | Rutaceae | Cultivated | 0.04 | 0.14 | 0.22 | 0.13 |
| Apium graveolens L. (FC698) | Apiaceae | Cultivated | 0.07 | 0.12 | 0.20 | 0.13 |
| Daucus carota L. (FC704) | Apiaceae | Cultivated | 0.09 | 0.11 | 0.19 | 0.13 |
| Ullucus tuberosus Caldas (FC713) | Basellaceae | Native | 0.08 | 0.15 | 0.15 | 0.13 |
| Alternanthera mexicana Moq. (FC684) | Amaranthaceae | Native | 0.11 | 0.13 | 0.13 | 0.12 |
| Citrus aurantium L. var. sinensis L. (FC890) | Rutaceae | Cultivated | 0.06 | 0.19 | 0.11 | 0.12 |
| Spartium junceum L. (FC816) | Leguminosae | Naturalized | 0.03 | 0.09 | 0.23 | 0.12 |
| Medicago sativa L. (FC802) | Leguminosae | Cultivated | 0.11 | 0.06 | 0.17 | 0.11 |
| Passiflora edulis Sims. (FC853) | Passifloraceae | Cultivated | 0.09 | 0.12 | 0.13 | 0.11 |
| Phyllanthus niruri L. (FC856) | Phyllanthaceae | Native | 0.08 | 0.09 | 0.15 | 0.11 |
| Stachys arvensis (L.) L. (FC796) | Lamiaceae | Native | 0.03 | 0.13 | 0.16 | 0.11 |
| Solanum tuberosum L. (FC910) | Solanaceae | Naturalized | 0.05 | 0.06 | 0.20 | 0.10 |
| Valeriana adscendens Turcz. (FC727) | Caprifoliaceae | Native | 0.07 | 0.07 | 0.16 | 0.10 |
| Cucurbita maxima Duchesne (FC773) | Cucurbitaceae | Cultivated | 0.03 | 0.06 | 0.19 | 0.09 |
| Verbena litoralis Kunth (FC920) | Verbenaceae | Native | 0.07 | 0.10 | 0.11 | 0.09 |
| Croton perspeciosus Croizat (No voucher) | Euphorbiaceae | Native | 0.09 | 0.03 | 0.13 | 0.08 |
| Medicinal Uses | City Center | Intermediate | City Periphery | Whole City |
|---|---|---|---|---|
| Stomach cramps | 31 (2.8) | 161 (8.4) | 205 (7.4) | 397 (6.9) |
| Kidney disorder and diuretic | 49 (4.4) | 132 (6.9) | 211 (7.7) | 392 (6.8) |
| Diarrhea | 46 (4.1) | 81 (4.2) | 158 (5.7) | 285 (4.9) |
| Flu | 47 (4.2) | 95 (4.9) | 107 (3.9) | 249 (4.3) |
| Intestinal parasites | 55 (5.0) | 77 (4.0) | 111 (4.0) | 243 (4.2) |
| Tacsho | 43 (3.9) | 89 (4.6) | 106 (3.8) | 238 (4.1) |
| Visual disorders | 26 (2.3) | 85 (4.4) | 121 (4.4) | 232 (4.0) |
| Insomnia | 37 (3.3) | 77 (4.0) | 81 (2.9) | 195 (3.4) |
| Birth | 47 (4.2) | 59 (3.1) | 84 (3.0) | 190 (3.3) |
| Prostate disorders | 60 (5.4) | 50 (2.6) | 73 (2.6) | 183 (3.2) |
| Menstruation disorders | 82 (7.4) | 23 (1.2) | 56 (2.0) | 161 (2.8) |
| Wounds healing | 33 (3.0) | 61 (3.2) | 62 (2.2) | 156 (2.7) |
| Fever | 23 (2.1) | 59 (3.1) | 72 (2.6) | 154 (2.7) |
| Burns | 27 (2.4) | 49 (2.5) | 76 (2.8) | 152 (2.6) |
| Breastfeeding | 37 (3.3) | 48 (2.5) | 55 (2.0) | 140 (2.4) |
| Socio-Economic Factors | Variable Classification |
|---|---|
| Home ownership | (1) Own; (2) Rented |
| Property quality characteristics | (1) Well maintained; (2) With some defects |
| Construction materials of the property | (1) Only modern materials; (2) Modern and traditional materials |
| Water chlorination system | (1) Yes; (2) No |
| Sewage system | (1) Yes; (2) No |
| Mobile phone | (1) Yes; (2) No |
| Radio | (1) Yes; (2) No |
| Television | (1) Yes; (2) No |
| Paid TV channels | (1) Yes; (2) No |
| Internet access | (1) Yes; (2) No |
| Computer | (1) Yes; (2) No |
| Printer | (1) Yes; (2) No |
| Washing machine | (1) Yes; (2) No |
| Refrigerator | (1) Yes; (2) No |
| Microwave or oven | (1) Yes; (2) No |
| Water heater | (1) Yes; (2) No |
| Off-road vehicle | (1) Yes; (2) No |
| Conventional car | (1) Yes; (2) No |
| Motorbike | (1) Yes; (2) No |
| Bicycle | (1) Yes; (2) No |
| Cooking fuel | (1) Gas; (2) Wood |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corroto, F.; Rascón, J.; Barboza, E.; Macía, M.J. Medicinal Plants for Rich People vs. Medicinal Plants for Poor People: A Case Study from the Peruvian Andes. Plants 2021, 10, 1634. https://doi.org/10.3390/plants10081634
Corroto F, Rascón J, Barboza E, Macía MJ. Medicinal Plants for Rich People vs. Medicinal Plants for Poor People: A Case Study from the Peruvian Andes. Plants. 2021; 10(8):1634. https://doi.org/10.3390/plants10081634
Chicago/Turabian StyleCorroto, Fernando, Jesús Rascón, Elgar Barboza, and Manuel J. Macía. 2021. "Medicinal Plants for Rich People vs. Medicinal Plants for Poor People: A Case Study from the Peruvian Andes" Plants 10, no. 8: 1634. https://doi.org/10.3390/plants10081634
APA StyleCorroto, F., Rascón, J., Barboza, E., & Macía, M. J. (2021). Medicinal Plants for Rich People vs. Medicinal Plants for Poor People: A Case Study from the Peruvian Andes. Plants, 10(8), 1634. https://doi.org/10.3390/plants10081634