
A High-Resolution Earth Observations and Machine Learning-Based Approach to Forecast Waterborne Disease Risk in Post-Disaster Settings



Abstract
:1. Introduction
1.1. Impact of Disasters on Humans (Health, Economic, and Social)
1.2. Waterborne Disease after Natural Disasters
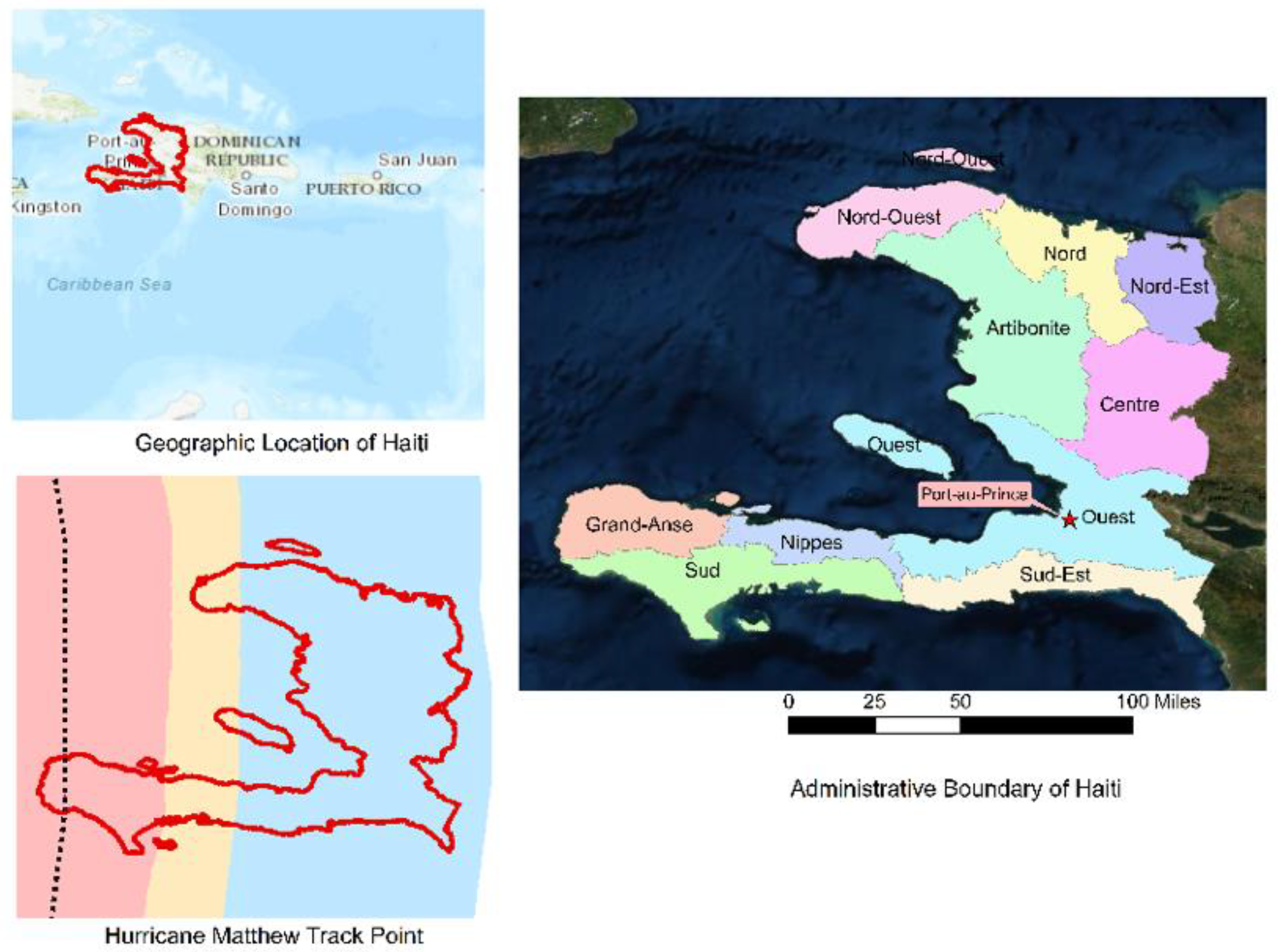
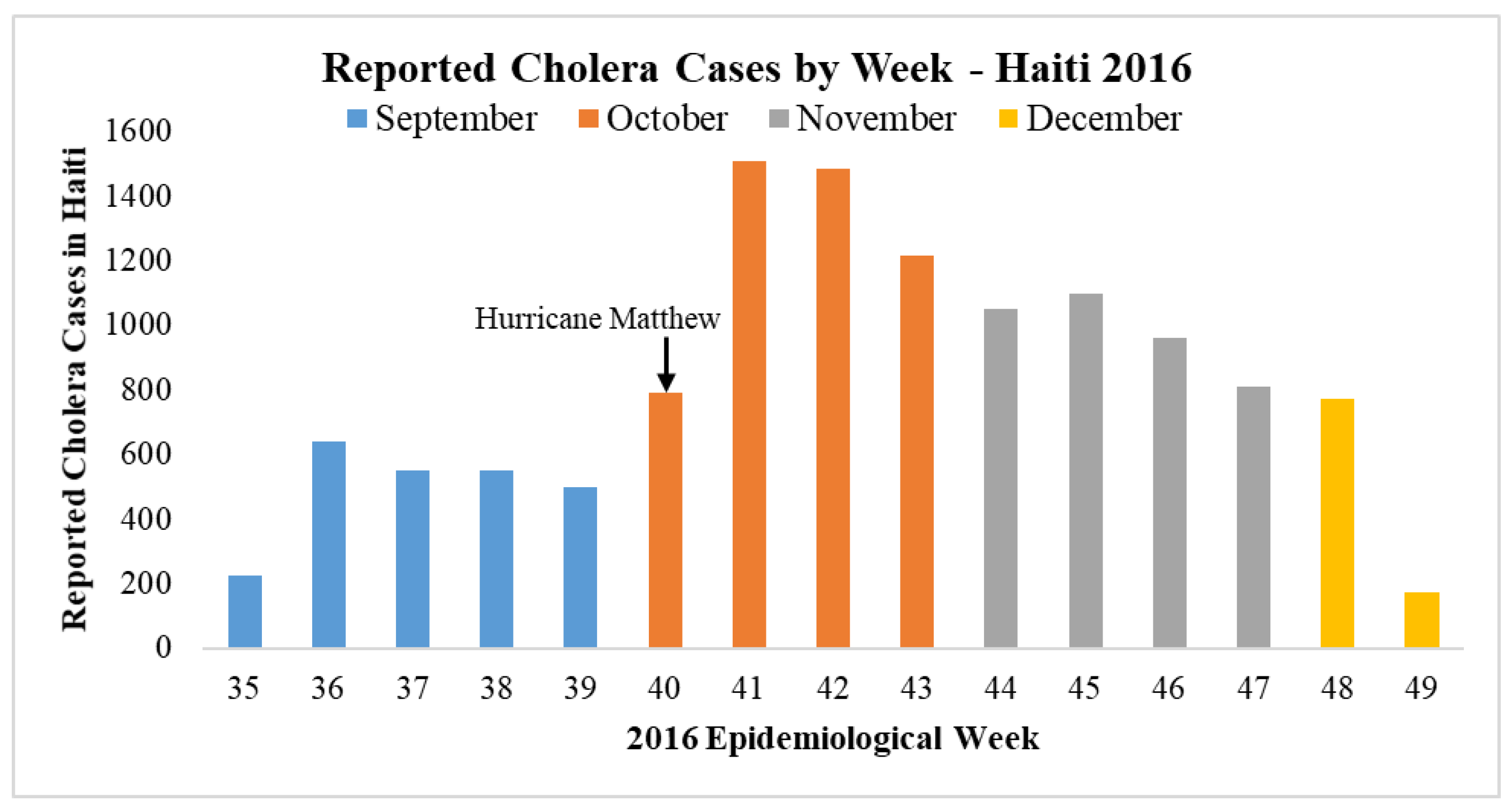
1.3. Cholera Outbreaks in Haiti
1.4. Research Questions and Objectives of the Paper
2. Materials and Methods
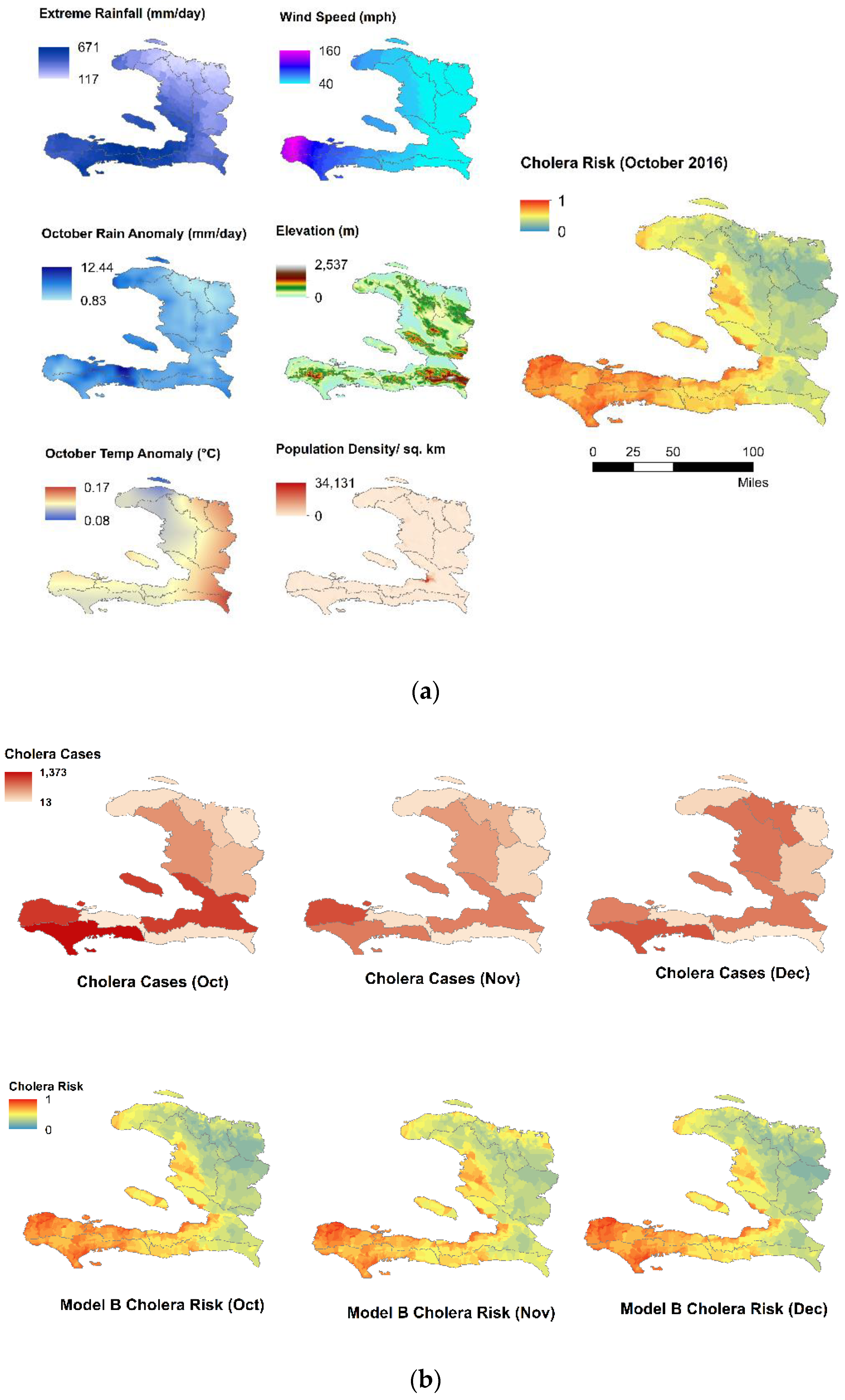
2.1. Data
2.1.1. Precipitation Anomaly
2.1.2. Temperature Anomaly
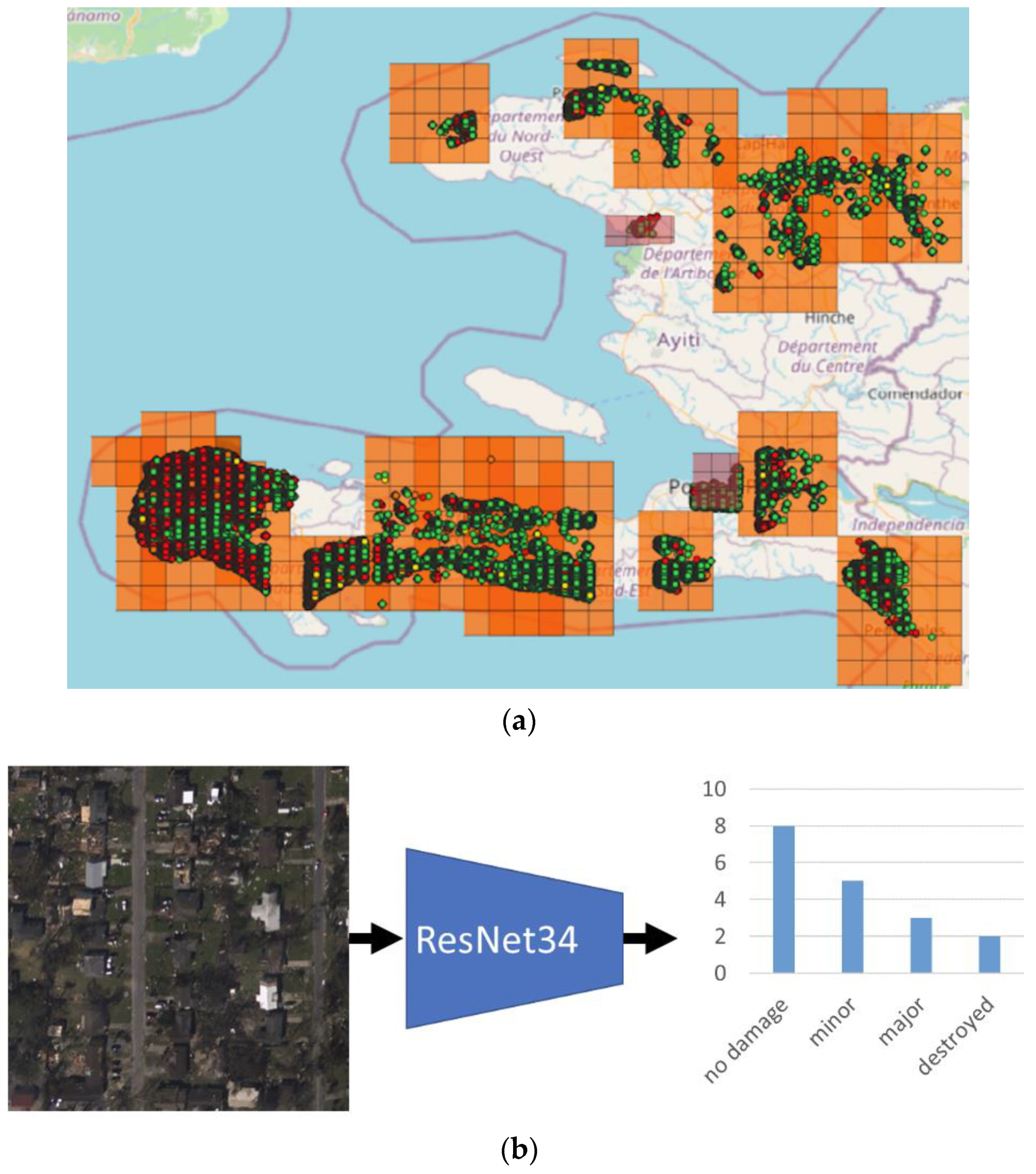
2.1.3. Humanitarian Assistance and Disaster Relief (HADR) Data
2.1.4. Cholera Data
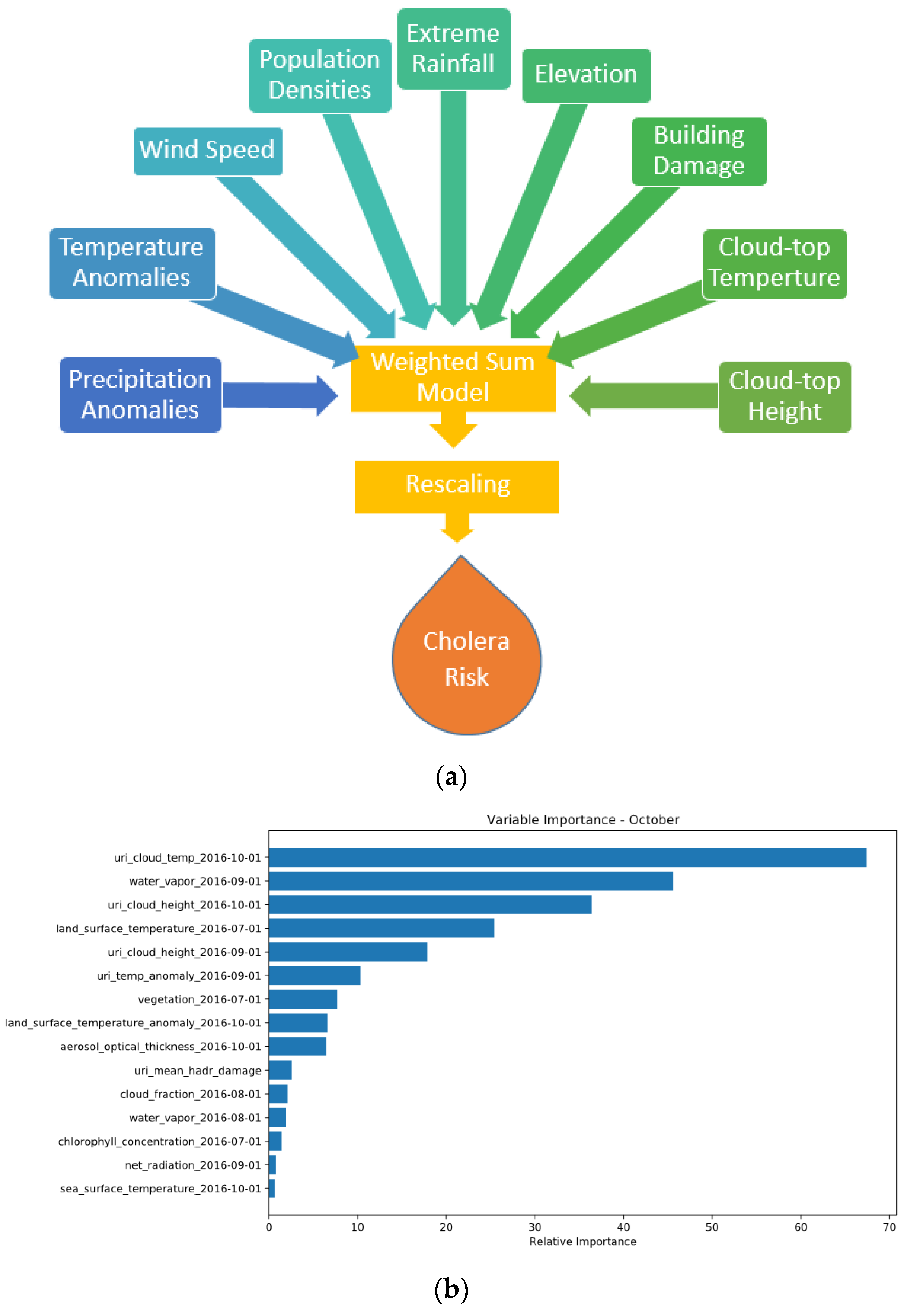
2.2. Models
Weighted Sum Models
- Feature Importance
3. Results
3.1. Correlation with Observed Cholera Cases
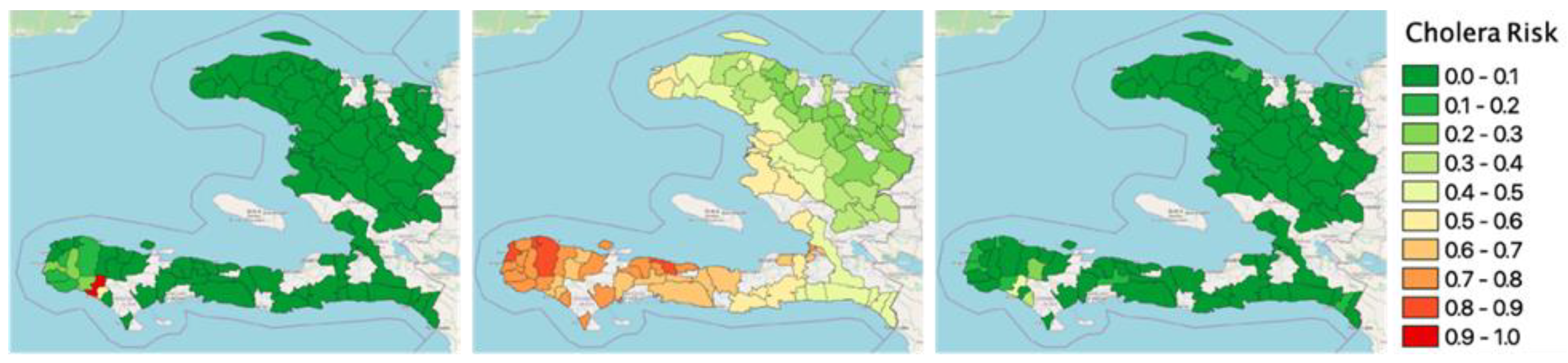
3.2. Understanding from the Variation of Model Outputs in Different Months
3.2.1. Model A
- September
- October
- November
- December
3.2.2. Model B
- September
- October
- November
- December
3.2.3. Model A Plus
- September
- October
- November
- December
3.2.4. Model B Plus
- September
- October
- November
- December
3.3. Improvement of Different Models from the Base Model A
3.4. Cholera Risk Prediction Improvement Offered by the Machine Learning Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mal, S.; Singh, R.B.; Huggel, C.; Grover, A. Introducing Linkages between Climate Change, Extreme Events, and Disaster Risk Reduction. In Climate Change, Extreme Events and Disaster Risk Reduction; Springer: New York, NY, USA, 2018; pp. 1–14. [Google Scholar]
- Trenberth, K.E.; Fasullo, J.T.; Shepherd, T.G. Attribution of climate extreme events. Nat. Clim. Chang. 2015, 5, 725–730. [Google Scholar] [CrossRef]
- Natural Disasters Are Increasing. The World’s Poorest Are Left to Fend for Themselves. Available online: https://www.vox.com/21571842/coronavirus-pandemic-climate-change-covid-19-natural-disaster-vaccine (accessed on 3 March 2022).
- Sawada, Y.; Takasaki, Y. Natural disaster, poverty, and development: An introduction. World Dev. 2017, 94, 2–15. [Google Scholar] [CrossRef]
- World Bank; United Nations. Natural Hazards, Unnatural Disasters: The Economics of Effective Prevention; The World Bank: Washington, DC, USA, 2011; Volume 48, ISBN 0821380508. [Google Scholar]
- Cash, R.A.; Halder, S.R.; Husain, M.; Islam, M.S.; Mallick, F.H.; May, M.A.; Rahman, M.; Rahman, M.A. Reducing the health effect of natural hazards in Bangladesh. Lancet 2013, 382, 2094–2103. [Google Scholar] [CrossRef] [Green Version]
- Charnley, G.E.C.; Kelman, I.; Gaythorpe, K.A.M.; Murray, K.A. Traits and risk factors of post-disaster infectious disease outbreaks: A systematic review. Sci. Rep. 2021, 11, 5616. [Google Scholar] [CrossRef] [PubMed]
- Hackbarth, M.; Pavkov, T.; Wetchler, J.; Flannery, M. Natural Disasters: An Assessment of Family Resiliency Following Hurricane Katrina. J. Marital Fam. Ther. 2012, 38, 340–351. [Google Scholar] [CrossRef]
- Freedy, J.R.; Shaw, D.L.; Jarrell, M.P.; Masters, C.R. Towards an understanding of the psychological impact of natural disasters: An application of the conservation resources stress model. J. Trauma. Stress 1992, 5, 441–454. [Google Scholar] [CrossRef]
- Kreimer, A. Social and economic impacts of natural disasters. Int. Geol. Rev. 2001, 43, 401–405. [Google Scholar] [CrossRef]
- Chigudu, S. The politics of cholera, crisis and citizenship in urban Zimbabwe: “People were dying like flies”. Afr. Aff. 2019, 118, 413–434. [Google Scholar] [CrossRef]
- Colwell, R. Cholera and climate: A demonstrated relationship. Trans. Am. Clin. Climatol. Assoc. 2009, 120, 119–128. [Google Scholar]
- Ali, M.; Emch, M.; Donnay, J.P.; Yunus, M.; Sack, R.B. Identifying environmental risk factors for endemic cholera: A raster GIS approach. Health Place 2002, 8, 201–210. [Google Scholar] [CrossRef]
- Ali, M.; Emch, M.; Donnay, J.P.; Yunus, M.; Sack, R.B. The spatial epidemiology of cholera in an endemic area of Bangladesh. Soc. Sci. Med. 2002, 55, 1015–1024. [Google Scholar] [CrossRef]
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; Faruque, A.S.G.; Hayashi, T.; Sack, D.A. Association between climate variability and hospital visits for non-cholera diarrhoea in Bangladesh: Effects and vulnerable groups. Int. J. Epidemiol. 2007, 36, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Penrose, K.; De Castro, M.C.; Werema, J.; Ryan, E.T. Informal urban settlements and cholera risk in Dar es Salaam, Tanzania. PLoS Negl. Trop. Dis. 2010, 4, e631. [Google Scholar] [CrossRef]
- Rajendran, K.; Sumi, A.; Bhattachariya, M.K.; Manna, B.; Sur, D.; Kobayashi, N.; Ramamurthy, T. Influence of relative humidity in Vibrio cholerae infection: A time series model. Indian J. Med. Res. 2011, 133, 138–145. [Google Scholar] [PubMed]
- Reiner, R.C.; King, A.A.; Emch, M.; Yunus, M.; Faruque, A.S.G.; Pascual, M. Highly localized sensitivity to climate forcing drives endemic cholera in a megacity. Proc. Natl. Acad. Sci. USA 2012, 109, 2033–2036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talavera, A.; Pérez, E.M. Is cholera disease associated with poverty? J. Infect. Dev. Ctries. 2009, 3, 408–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akanda, A.S.; Aziz, A.; Jutla, A.; Huq, A.; Alam, M.; Asham, G.U.; Colwell, R.R. Satellites and cell phones form a cholera early-warning system. Eos Trans. Am. Geophys. Union 2018, 99. [Google Scholar] [CrossRef]
- Ali, M.; Nelson, A.R.; Lopez, A.L.; Sack, D.A. Updated global burden of cholera in endemic countries. PLoS Negl. Trop. Dis. 2015, 9, e0003832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parry, M.L.; Canziani, O.; Palutikof, J.; Van der Linden, P.; Hanson, C. Climate Change 2007-Impacts, Adaptation and Vulnerability: Working Group II Contribution to the Fourth Assessment Report of the IPCC; Cambridge University Press: Cambridge, UK, 2007; Volume 4, ISBN 0521880106. [Google Scholar]
- Liu, Z.D.; Li, J.; Zhang, Y.; Ding, G.Y.; Xu, X.; Gao, L.; Liu, X.N.; Liu, Q.Y.; Jiang, B.F. Distributed lag effects and vulnerable groups of floods on bacillary dysentery in Huaihua, China. Sci. Rep. 2016, 6, 29456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flooding and Communicable Diseases Fact Sheet. Available online: https://www.who.int/hac/techguidance/ems/FloodingandCommunicableDiseasesfactsheet.pdf (accessed on 3 March 2022).
- Fewtrell, L.; Kay, D.; Watkins, J.; Davies, C.; Francis, C. The microbiology of urban UK floodwaters and a quantitative microbial risk assessment of flooding and gastrointestinal illness. J. Flood Risk Manag. 2011, 4, 77–87. [Google Scholar] [CrossRef]
- Levy, K.; Woster, A.P.; Goldstein, R.S.; Carlton, E.J. Untangling the Impacts of Climate Change on Waterborne Diseases: A Systematic Review of Relationships between Diarrheal Diseases and Temperature, Rainfall, Flooding, and Drought. Environ. Sci. Technol. 2016, 50, 4905–4922. [Google Scholar] [CrossRef] [Green Version]
- World Water Development Report 2018. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000261424 (accessed on 3 March 2022).
- Nusrat, F.; Akanda, A.S.; Johnson, K.; Khan, A.I.; Islam, M.T.; Rashid, M.M.; Qadri, F. Understanding the Water Access and Waterborne diseases vulnerability of women in the context of gender biased social norms. In Proceedings of the AGU Fall Meeting 2021, New Orleans, LA, USA, 13–17 December 2021. [Google Scholar]
- Effler, P.; Isaäcson, M.; Arntzen, L.; Heenan, R.; Canter, P.; Barrett, T.; Lee, L.; Mambo, C.; Levine, W.; Zaidi, A.; et al. Factors contributing to the emergence of Escherichia coli O157 in Africa. Emerg. Infect. Dis. 2001, 7, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Moors, E.; Singh, T.; Siderius, C.; Balakrishnan, S.; Mishra, A. Climate change and waterborne diarrhoea in northern India: Impacts and adaptation strategies. Sci. Total Environ. 2013, 468–469, S139–S151. [Google Scholar] [CrossRef]
- Rieckmann, A.; Tamason, C.C.; Gurley, E.S.; Rod, N.H.; Jensen, P.K.M. Exploring droughts and floods and their association with cholera outbreaks in sub-saharan africa: A register-based ecological study from 1990 to 2010. Am. J. Trop. Med. Hyg. 2018, 98, 1269–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senhorst, H.A.J.; Zwolsman, J.J.G. Climate change and effects on water quality: A first impression. Water Sci. Technol. 2005, 51, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Ahern, M.; Kovats, R.S.; Wilkinson, P.; Few, R.; Matthies, F. Global health impacts of floods: Epidemiologic evidence. Epidemiol. Rev. 2005, 27, 36–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shultz, J.M.; Russell, J.; Espinel, Z. Epidemiology of tropical cyclones: The dynamics of disaster, disease, and development. Epidemiol. Rev. 2005, 27, 21–35. [Google Scholar] [CrossRef] [Green Version]
- Watson, J.T.; Gayer, M.; Connolly, M.A. Epidemics after natural disasters. Emerg. Infect. Dis. 2007, 13, 1–5. [Google Scholar] [CrossRef]
- Bhunia, R.; Ghosh, S. Waterborne cholera outbreak following Cyclone Aila in Sundarban area of West Bengal, India, 2009. Trans. R. Soc. Trop. Med. Hyg. 2011, 105, 214–219. [Google Scholar] [CrossRef]
- Bhunia, R.; Ramakrishnan, R.; Hutin, Y.; Gupte, M.D. Cholera outbreak secondary to contaminated pipe water in an urban area, West Bengal, India, 2006. Indian J. Gastroenterol. 2009, 28, 62–64. [Google Scholar] [CrossRef]
- Sur, D.; Dutta, P.; Nair, G.B.; Bhattacharya, S.K. Severe cholera outbreak following floods in a northern district of West Bengal. Indian J. Med. Res. 2000, 112, 178–182. [Google Scholar] [PubMed]
- Taneja, N.; Kaur, J.; Sharma, K.; Singh, M.; Kalra, J.K.; Sharma, N.M.; Sharma, M. A recent outbreak of cholera due to Vibrio cholerae O1 Ogawa in & around Chandigarh, North India. Indian J. Med. Res. 2003, 117, 243–246. [Google Scholar]
- Akanda, A.S.; Jutla, A.S.; Alam, M.; De Magny, G.C.; Siddique, A.K.; Sack, R.B.; Huq, A.; Colwell, R.R.; Islam, S. Hydroclimatic influences on seasonal and spatial cholera transmission cycles: Implications for public health intervention in the Bengal Delta. Water Resour. Res. 2011, 47, W00H07. [Google Scholar] [CrossRef]
- Huq, A.; West, P.A.; Small, E.B.; Huq, M.I.; Colwell, R.R. Influence of water temperature, salinity, and pH on survival and growth of toxigenic Vibrio cholerae serovar O1 associated with live copepods in laboratory microcosms. Appl. Environ. Microbiol. 1984, 48, 420–424. [Google Scholar] [CrossRef] [Green Version]
- Cambaza, E.; Mongo, E.; Anapakala, E.; Nhambire, R.; Singo, J.; Machava, E. Outbreak of cholera due to cyclone kenneth in northern Mozambique, 2019. Int. J. Environ. Res. Public Health 2019, 16, 2925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- 2 Years Since Cyclone Idai and Mozambique Has Already Faced an Additional 3 Cyclones. Available online: https://reliefweb.int/report/mozambique/2-years-cyclone-idai-and-mozambique-has-already-faced-additional-3-cyclones (accessed on 3 March 2022).
- Cholera Is Spreading in Mozambique in the Wake of Cyclone Idai. Available online: https://www.vox.com/science-and-health/2019/3/29/18287342/mozambique-cyclone-idai-cholera-how-to-help (accessed on 3 March 2022).
- Chen, W.H.; Azman, A.S. Mitigating cholera in the aftermath of cyclone Idai. Am. J. Trop. Med. Hyg. 2019, 101, 960. [Google Scholar] [CrossRef]
- India: Cyclone Aila Situation Update, 30 June 2009. Available online: https://reliefweb.int/report/india/india-cyclone-aila-situation-update-30-jun-2009 (accessed on 3 March 2022).
- ECHO Factsheet–Haiti–April 2018. Available online: https://reliefweb.int/report/haiti/echo-factsheet-haiti-april-2018 (accessed on 3 January 2022).
- HAITI Humanitarian Situation Report #16. Available online: https://reliefweb.int/report/haiti/unicef-haiti-humanitarian-situation-report-hurricane-matthew-16-15-december-2016 (accessed on 2 January 2022).
- Organization United Nations Foundation. Agriculture Haiti: Hurricane Matthew SITUATION REPORT–22 November 2016. Available online: https://www.fao.org/emergencies/recursos/documentos/recursos-detalle/es/c/454208/ (accessed on 3 January 2022).
- Haiti: Hurricane Matthew-Situation Report No. 14 (21 October 2016). Available online: https://reliefweb.int/report/haiti/haiti-hurricane-matthew-situation-report-no-14-21-october-2016 (accessed on 3 March 2022).
- Haiti: Humanitarian Situation Report End of Yea-2018. Available online: https://reliefweb.int/report/haiti/haiti-humanitarian-situation-report-end-year-2018 (accessed on 4 January 2022).
- ECHO Factsheet–Haiti–(Last Updated 21/05/2019). Available online: https://reliefweb.int/report/haiti/echo-factsheet-haiti-last-updated-21052019 (accessed on 5 January 2022).
- Mozambique: Two Cyclones: Idai and Kenneth (As of 22 May 2019). Available online: https://reliefweb.int/report/mozambique/mozambique-two-cyclones-idai-and-kenneth-22-may-2019 (accessed on 3 March 2022).
- UNICEF Mozambique Cyclones Idai and Kenneth Situation Report #11 (1–10 June 2019). Available online: https://reliefweb.int/report/mozambique/unicef-mozambique-cyclones-idai-and-kenneth-situation-report-11-01-10-june-2019 (accessed on 16 December 2021).
- UNICEF Cyclone Idai Post-Impact Situation April 2019. Available online: https://reliefweb.int/report/mozambique/unicef-cyclone-idai-post-impact-situation-april-2019 (accessed on 1 March 2022).
- Mozambique Cyclone Idai Response: Situation Report #6 21–30 April 2019. Available online: https://reliefweb.int/report/mozambique/mozambique-cyclone-idai-response-situation-report-6-21-30-april-2019 (accessed on 19 December 2021).
- Barzilay, E.J.; Schaad, N.; Magloire, R.; Mung, K.S.; Boncy, J.; Dahourou, G.A.; Mintz, E.D.; Steenland, M.W.; Vertefeuille, J.F.; Tappero, J.W. Cholera Surveillance during the Haiti Epidemic—The First 2 Years. N. Engl. J. Med. 2013, 368, 599–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillaume, Y.; Ternier, R.; Vissieres, K.; Casseus, A.; Chery, M.J.; Ivers, L.C. Responding to cholera in Haiti: Implications for the national plan to eliminate cholera by 2022. J. Infect. Dis. 2018, 218, S167–S170. [Google Scholar] [CrossRef]
- Enserink, M. Cholera linked to U.N. forces, but questions remain. Science 2011, 332, 776–777. [Google Scholar] [CrossRef]
- Haiti Cholera Response December 2014. Available online: https://reliefweb.int/report/haiti/haiti-cholera-response-december-2014 (accessed on 29 November 2021).
- Haque, M.; Rollend, D.; Withee, S.; Christie, G.; Papusha, I.; Nikoukar, R.; Chen, M.; Nusrat, F.; Akanda, A.S. Continuum: A New Observing Strategies-Based Framework for Hyper-Local Situational Awareness. In Proceedings of the AGU Fall Meeting, Virtual Online, 1–17 December 2020. [Google Scholar]
- Khan, R.; Anwar, R.; Akanda, S.; McDonald, M.D.; Huq, A.; Jutla, A.; Colwell, R. Assessment of risk of cholera in Haiti following Hurricane Matthew. Am. J. Trop. Med. Hyg. 2017, 97, 896–903. [Google Scholar] [CrossRef]
- Nusrat, F.; Akanda, A.S.; Haque, M.; Rollend, D.; Christie, G. Waterborne Disease Outbreaks in the Post-Disaster Scenario: Can High-Resolution Earth Observations and Smallsat Imagery Enhance Cholera Forecasting? In Proceedings of the AGU Fall Meeting, Virtual Online, 1–17 December 2020. [Google Scholar]
- Haiti Faces Fresh Cholera Outbreak after Hurricane Matthew, Aid Agencies Fear. Available online: https://www.theguardian.com/world/2016/oct/14/haiti-cholera-hurricane-matthew-aid-agencies (accessed on 20 March 2022).
- NASA Global Maps. Available online: https://earthobservatory.nasa.gov/global-maps (accessed on 3 March 2022).
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; Volume 2016, pp. 770–778. [Google Scholar]
- Gupta, R.; Goodman, B.; Patel, N.; Hosfelt, R.; Sajeev, S.; Heim, E.; Doshi, J.; Lucas, K.; Choset, H.; Gaston, M. Creating XBD: A dataset for assessing building damage from satellite imagery. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition Workshops, Long Beach, CA, USA, 15–20 June 2019; Volume 2019, pp. 10–17. [Google Scholar]
- Digital Globe Open Data Program: Hurricane Matthew. Available online: https://www.digitalglobe.com/ecosystem/open-data/hurricane-matthew (accessed on 20 March 2022).
- Suspected Cholera Cases by Commune in Haiti Associated to Matthew Hurricane. Available online: http://ais.paho.org/phip/viz/ed_haiticoleracases.asp (accessed on 3 March 2022).
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. In Proceedings of the ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Campbell, A.M.; Racault, M.-F.; Goult, S.; Laurenson, A. Cholera risk: A machine learning approach applied to essential climate variables. Int. J. Environ. Res. Public Health 2020, 17, 9378. [Google Scholar] [CrossRef] [PubMed]
- Badkundri, R.; Valbuena, V.; Pinnamareddy, S.; Cantrell, B.; Standeven, J. Forecasting the 2017–2018 Yemen cholera outbreak with machine learning. arXiv 2019, arXiv:1902.06739 2019. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Natural Disasters | Country | People Impacted by Natural Disasters | Year | Cholera Related to Natural Disasters | House Damaged | Health Facility Damaged | ||
|---|---|---|---|---|---|---|---|---|
| Affected | Death | Cases | Fatalities | |||||
| Cyclone Aila | West Bengal, India | 6.8 million [46] | 138 [46] | 26 May 2009 | 1076 [36] (diarrhea: 85,000) [46] | 14 [36] (diarrhea: 28) [46] | 945,000 [46] | 30% of health sub-centers [46] |
| Hurricane Matthew | Haiti | 2.1 million [47] | 546 [47] | 4 October 2016 (after Matthew) | 8457 [48] | 100 [48] | 25,160 [49] | 36 [50] |
| 2017 | 13,747 [47] | 159 [47] | ||||||
| 2018 | 3786 [51] | 41 [51] | ||||||
| 2019 | 308 [52] | 3 [52] | ||||||
| Cyclone Kenneth | Mozambique | 374,000 [53] | 45 [53] | 25 April 2019 | 267 [54] | _ | 45,000 [53] | 19 [53] |
| Cyclone Idai | Mozambique | 1.85 million [55] | Over 602 [55] | 14 March 2019 | 6682 [56] | 8 | 240,000 [53] | 94 [53] |
| Model A | Model A Plus | Model B | Model B Plus |
|---|---|---|---|
| Precipitation Anomalies (mm/day) | Precipitation Anomalies (mm/day) | Precipitation Anomalies (mm/day) | Precipitation Anomalies (mm/day) |
| Temperature Anomalies (°C) | Temperature Anomalies (°C) | Temperature Anomalies (°C) | Temperature Anomalies (°C) |
| Population Densities (count per km2) | Population Densities (count per km2) | Population Densities (count per km2) | Population Densities (count per km2) |
| Wind Swath of Hurricane (miles) | Wind Speed Above Ground (m/s) | Wind Speed (miles/hour) | Wind Speed Above Ground (m/s) |
| Cloud Height (m) | Extreme Rainfall (mm/day) | Extreme Rainfall (mm/day) | |
| Cloud Temperature (k) | Elevation (m) | Elevation (m) | |
| Building Damage | Cloud Height (m) | ||
| Cloud Temperature (k) | |||
| Building Damage |
| Month | Total Cholera Cases |
|---|---|
| September | 2461 |
| October | 4998 |
| November | 3913 |
| December | 946 |
| Month | Model A | Model A Plus | Model B | Model B Plus | ML Model |
|---|---|---|---|---|---|
| September | −0.044 | −0.398 | −0.099 | −0.692 | 0.818 (0.0039) |
| October | 0.590 | 0.574 | 0.645 | 0.512 | 0.811 (0.0044) |
| November | 0.649 | 0.687 | 0.748 | 0.570 | 0.733 (0.0158) |
| December | 0.690 | 0.365 | 0.648 | 0.364 | 0.744 (0.0136) |
| Average (October–December) | 0.643 | 0.542 | 0.680 | 0.482 | 0.760 |
| Month | Improvement from Base Model A (%) | ||
|---|---|---|---|
| Model A Plus | Model B | Model B Plus | |
| October | −2.717 | 9.304 | −13.108 |
| November | 5.807 | 15.262 | −12.220 |
| December | −47.109 | −6.012 | −47.303 |
| Average (October–December) | −14.673 | 6.185 | −24.210 |
| Month | Correlation with Monthly Cholera Cases with Best Existing Model (Model B) Outputs | Correlation with Monthly Cholera Cases with ML Outputs | Improvement from Model B (%) |
|---|---|---|---|
| October | 0.645 | 0.811 | 25.81 |
| November | 0.748 | 0.733 | −2.00 |
| December | 0.648 | 0.744 | 14.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nusrat, F.; Haque, M.; Rollend, D.; Christie, G.; Akanda, A.S. A High-Resolution Earth Observations and Machine Learning-Based Approach to Forecast Waterborne Disease Risk in Post-Disaster Settings. Climate 2022, 10, 48. https://doi.org/10.3390/cli10040048
Nusrat F, Haque M, Rollend D, Christie G, Akanda AS. A High-Resolution Earth Observations and Machine Learning-Based Approach to Forecast Waterborne Disease Risk in Post-Disaster Settings. Climate. 2022; 10(4):48. https://doi.org/10.3390/cli10040048
Chicago/Turabian StyleNusrat, Farah, Musad Haque, Derek Rollend, Gordon Christie, and Ali S. Akanda. 2022. "A High-Resolution Earth Observations and Machine Learning-Based Approach to Forecast Waterborne Disease Risk in Post-Disaster Settings" Climate 10, no. 4: 48. https://doi.org/10.3390/cli10040048
APA StyleNusrat, F., Haque, M., Rollend, D., Christie, G., & Akanda, A. S. (2022). A High-Resolution Earth Observations and Machine Learning-Based Approach to Forecast Waterborne Disease Risk in Post-Disaster Settings. Climate, 10(4), 48. https://doi.org/10.3390/cli10040048