
Impact of Air Temperature on London Ambulance Call-Out Incidents and Response Times




Abstract
:1. Introduction
The presence of strong weather effects among different target groups indicates the possibility for the development of a short-term forecast system of daily ambulance demand using weather variables. The availability of such a forecast system would render more effective deployment of the ambulance services to meet unexpected increases in service demands.([18], p. 60)
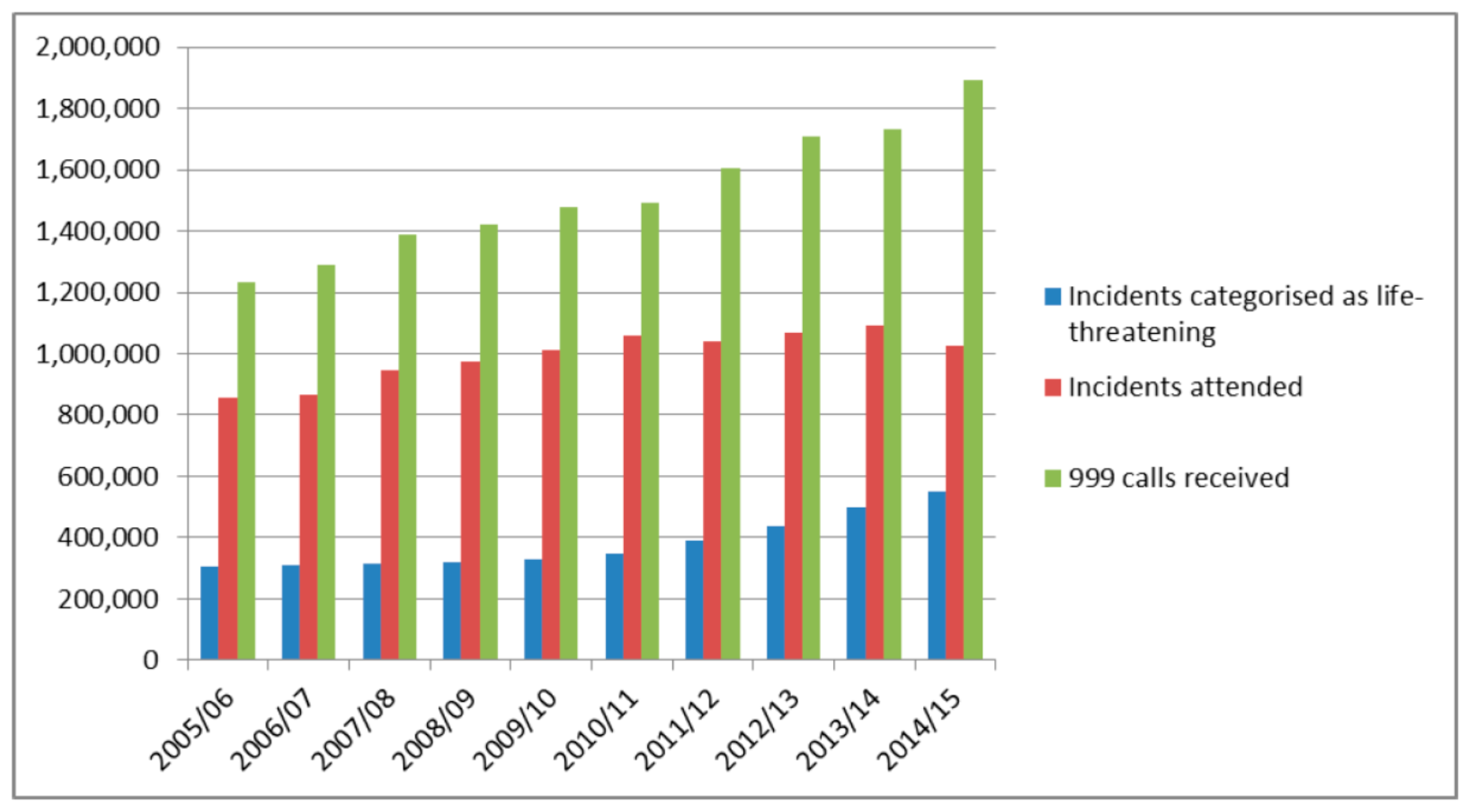
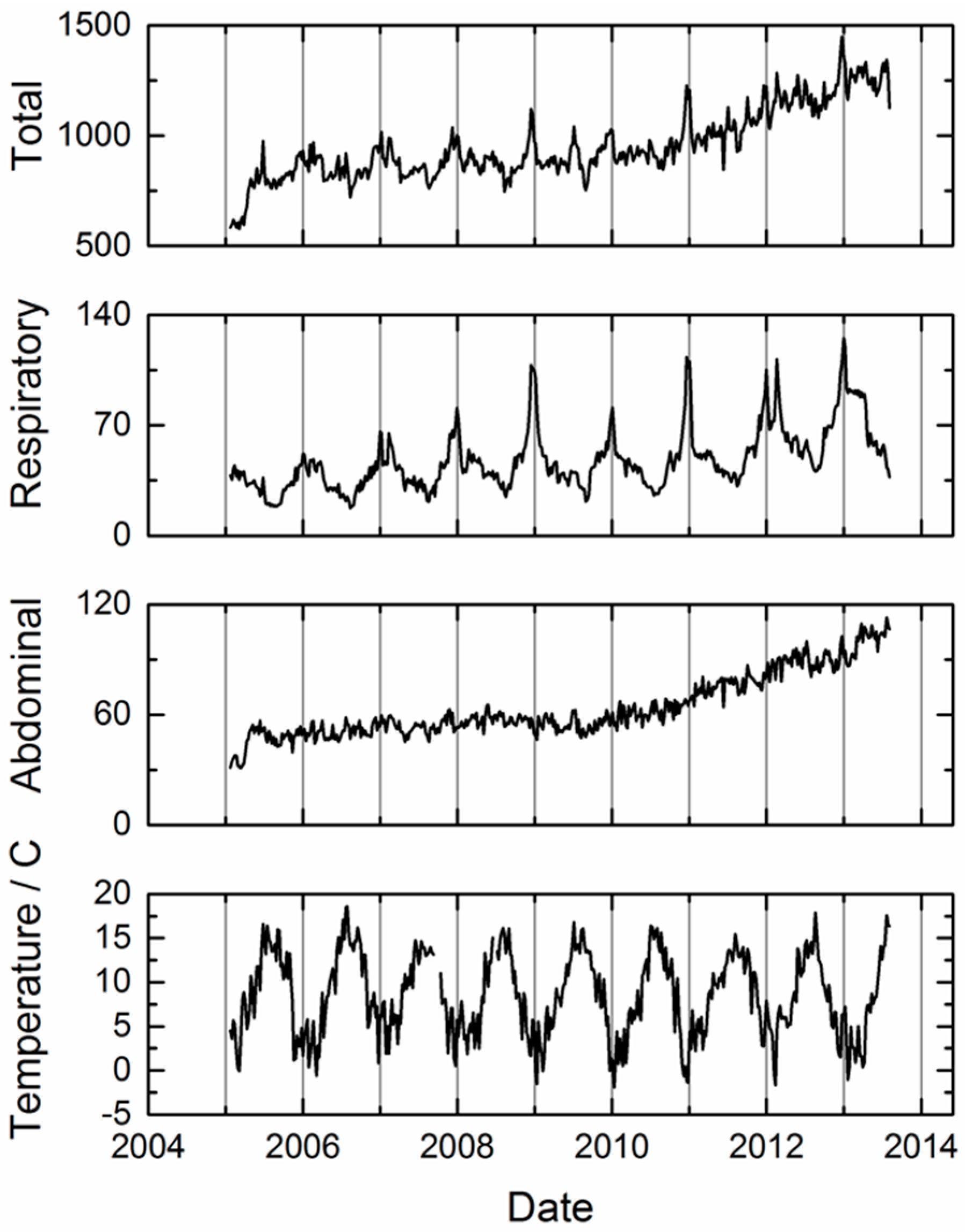
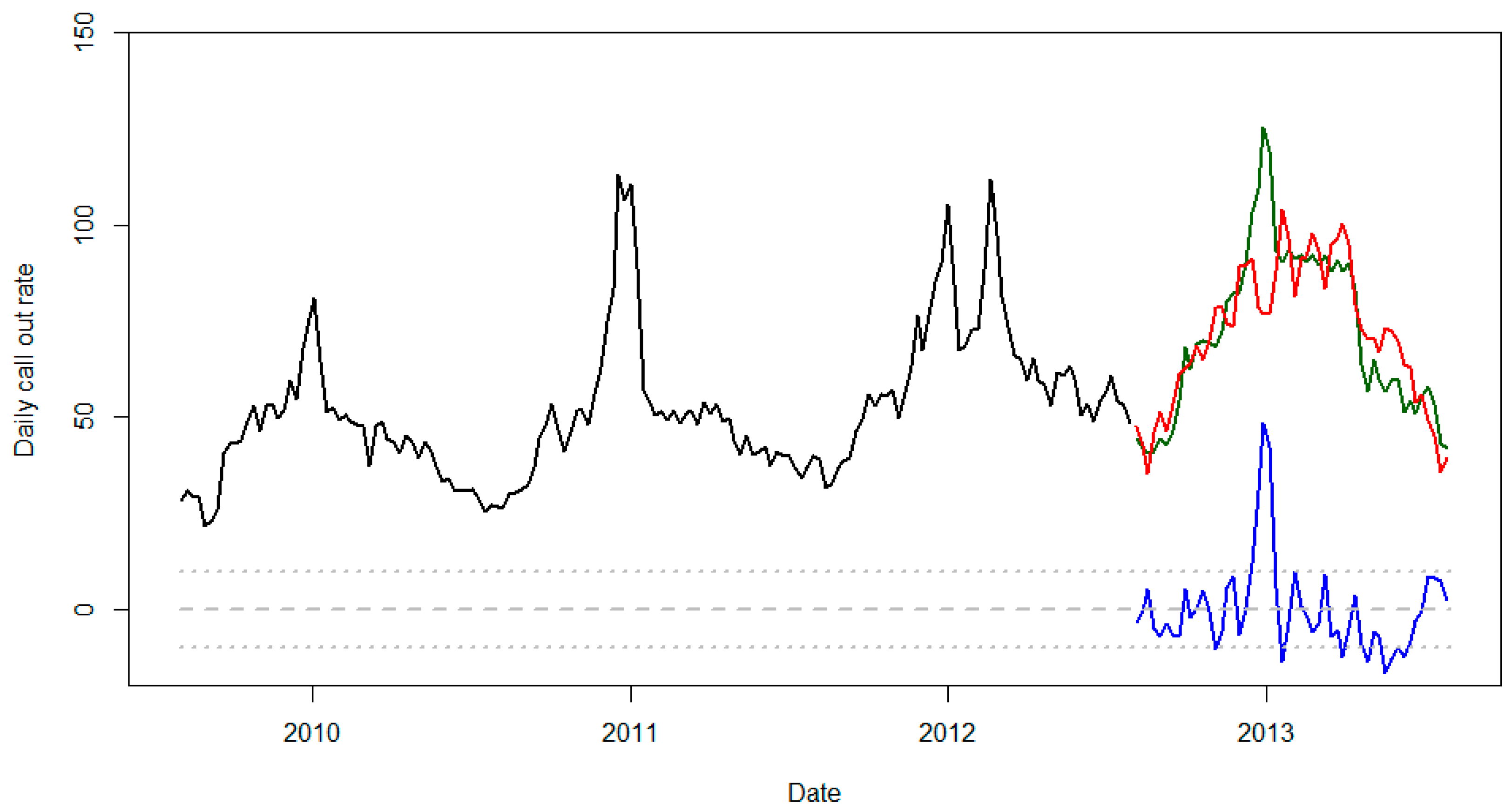
2. Methods: Long-Term Increase in Ambulance Usage
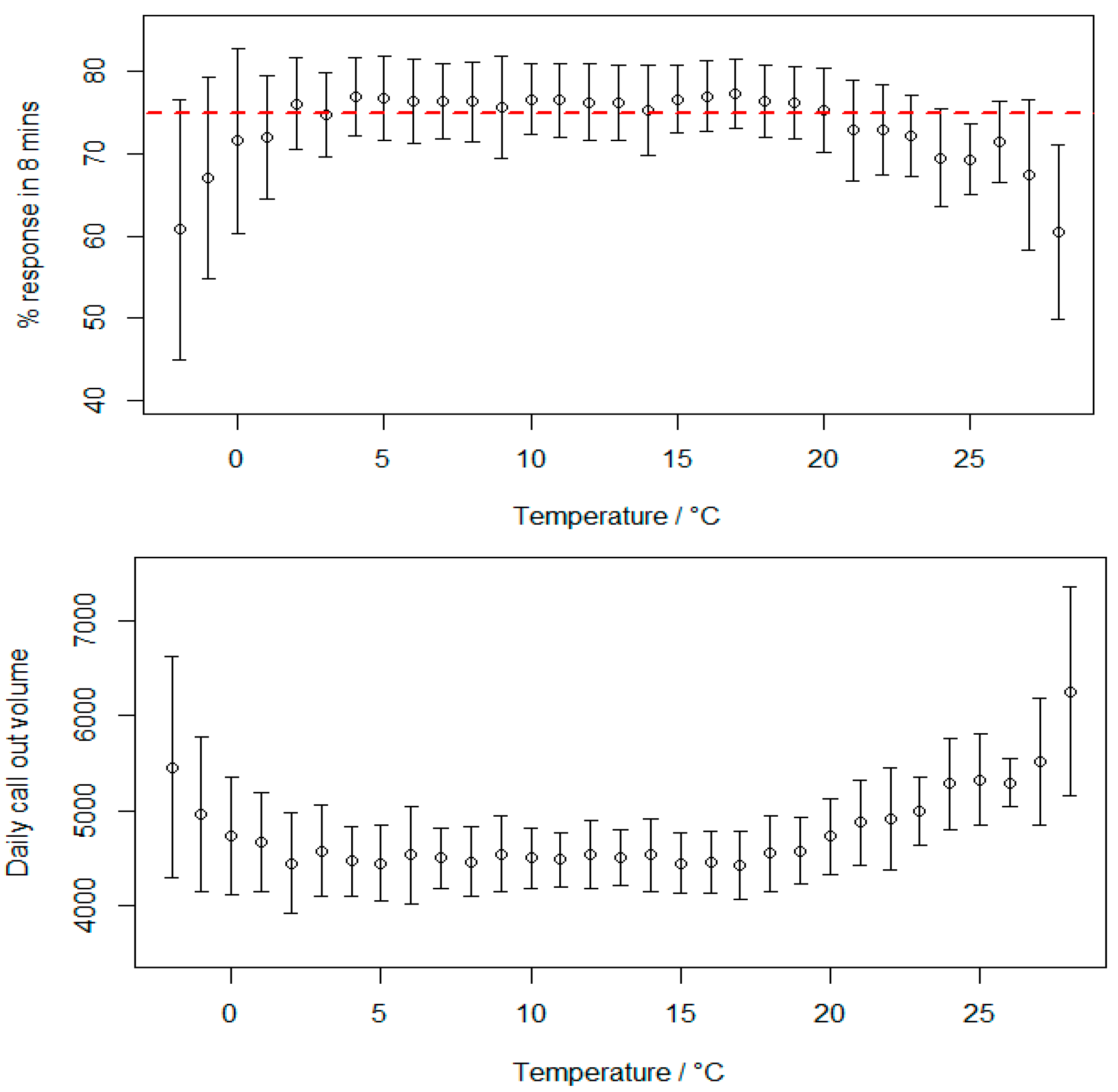
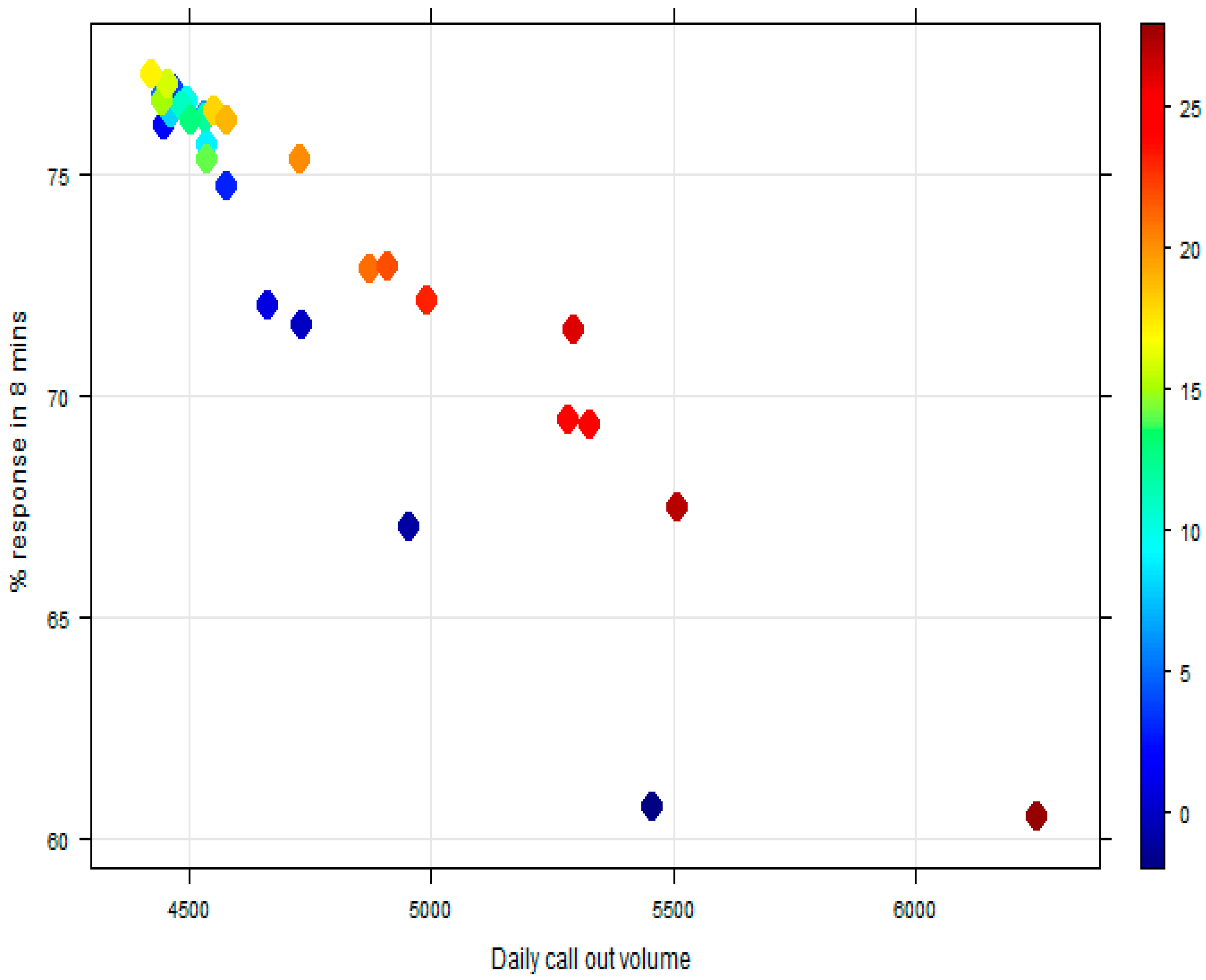
3. Results: The Effect of Air Temperature on Ambulance Response Times
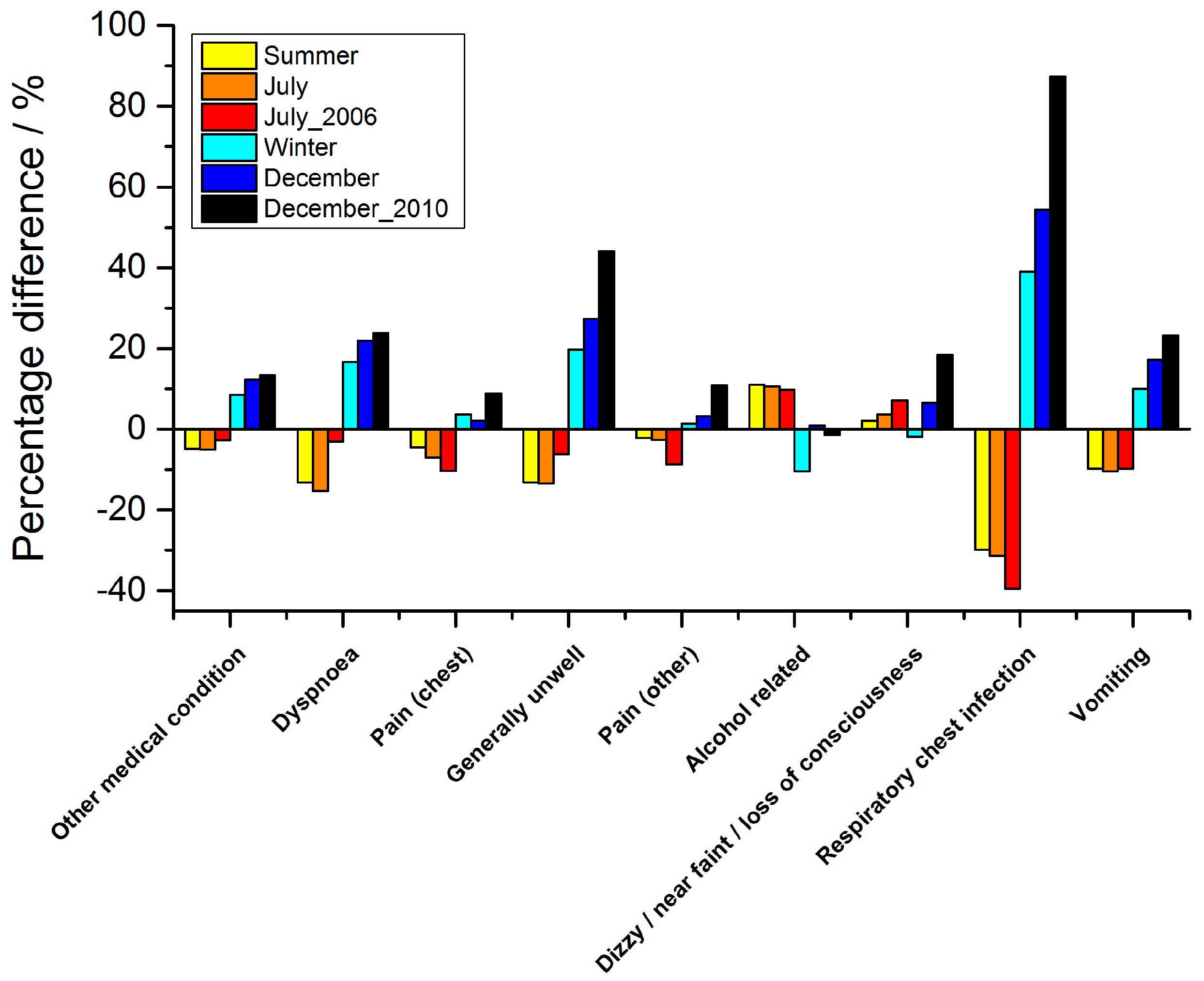
4. Discussion: Ambulance Illness Codes versus Air Temperature
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Health & Social Care Information Centre (HSCIC). Ambulance Services, England 2014-15; National Health Service: London, UK, 2015; pp. 1–75. [Google Scholar]
- Wu, O.; Briggs, A.; Kemp, T.; Gray, A.; MacIntyre, K.; Rowley, J.; Willett, K. Mobile phone use for contacting emergency services in life threatening circumstances. J. Emerg. Med. 2012, 42, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Heaviside, C. (Eds.) Health Effects of Climate Change in the UK; Health Protection Agency (Now Public Health England): Leeds, UK, 2012; pp. 1–238. [Google Scholar]
- Vardoulakis, S.; Dear, K.; Hajat, S.; Heaviside, C.; Eggen, B.; McMichael, A.J. Comparative assessment of the effects of climate change on heat and cold related mortality in the UK and Australia. Environ. Health Perspect. 2014, 122, 1285–1292. [Google Scholar] [PubMed]
- Hajat, S.; Vardoulakis, S.; Heaviside, C.; Eggen, B. Climate change effects on human health: Projections of temperature-related mortality for the UK during the 2020s, 2050s, and 2080s. J. Epidemiol. Community Health 2014, 68, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Tucker, G.R.; Hansen, A.L.; Williams, S.; Zhang, Y.; Bi, P. Impact of two recent extreme heat episodes on morbidity and mortality in Adelaide, South Australia: A case-series analysis. Environ. Health 2011, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.R.; Connell, D.; Tong, S. Exposure to hot and cold temperatures and ambulance attendances in Brisbane, Australia: A time series study. BMJ Open 2012, 2, e001074. [Google Scholar]
- Schaffer, A.; Muscatello, D.; Broome, R.; Corbett, S.; Smith, W. Emergency department visits, ambulance calls, and mortality associated with an exceptional heat wave in Sydney, Australia, 2011: A time-series analysis. Environ. Health 2012, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Dolney, T.J.; Sheridan, S.C. The relationship between extreme heat and ambulance response calls for the city of Toronto, Ontario, Canada. Environ. Res. 2006, 101, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Bassil, K.L.; Cole, D.C.; Moineddin, R.; Lou, W.; Craig, A.M.; Schwartz, B.; Rea, E. The relationship between temperature and ambulance response calls for heat related illness in Toronto, Ontario, 2005. J. Epidemiol. Community Health 2011, 65, 829–831. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Zauli Sajani, S.; Scotto, F.; Miglio, R.; Marchesi, S.; Lauriola, P. Emergency ambulance dispatches and apparent temperature: A time series analysis in Emilia-Romagna, Italy. Environ. Res. 2011, 111, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Petralli, M.; Morabito, M.; Cecchi, L.; Crisci, A.; Orlandini, S. Urban morbidity in summer: Ambulance dispatch data, periodicity and weather. Cent. Eur. J. Med. 2012, 7, 775–782. [Google Scholar] [CrossRef]
- Cerutti, B.; Tereanu, C.; Domenighetti, G.; Cantoni, E.; Gaia, M.; Bolgiani, I.; Lazzaro, M.; Cassis, I. Temperature related mortality and ambulance service interventions during the heat waves of 2003 in Ticino (Switzerland). Soz. Praventivmed. 2006, 51, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.; McGregor, G.; Analitis, A. Performance assessment of heat wave vulnerability index for Greater London, United Kingdom. Weather Clim. Soc. 2013, 6, 32–46. [Google Scholar] [CrossRef]
- Thornes, J.E. The Impact of Extreme Weather and Climate Change on Ambulance Incidents and Response Times in London; Pilot Report for the London Ambulance Service; Public Health England: Leeds, UK, 2014; pp. 1–30. [Google Scholar]
- Thornes, J.E. Predicting Demand through Climate Data. Ambulanc. Today 2013, 10, 39–41. [Google Scholar]
- Thornes, J.E.; Fisher, P.A.; Rayment-Bishop, T.; Smith, C. Ambulance Call-outs and Response Times in Birmingham and the Impact of Extreme Weather and Climate Change. Emerg. Med. J. 2014, 31, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.T.; Lai, P.C. Weather inference and daily demand for emergency ambulance services. Emerg. Med. J. 2012, 29, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, U.; Exner, T.; Wanka, E.R.; Bergemann, C.; Meyer-Arnek, J.; Hildenbrand, B.; Tufman, A.; Heumann, C.; Huber, R.M.; Bittner, M.; et al. Influence of air pressure, humidity, solar radiation, temperature, and wind speed on ambulatory visits due to chronic obstructive pulmonary disease in Bavaria, Germany. Int. J. Biometeorol. 2012, 56, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.H.; Canyon, D.V.; Buettner, P.G.; Mac Crawford, J.; Judd, J. Carbon footprint of Australian ambulance operations. Emerg. Med. Australas. 2012, 24, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Green Environmental Ambulance Network (GrEAN). Green Passport; Yorkshire Ambulance Service: Wakefield, UK, 2012. [Google Scholar]
- Chung, J.W.; Meltzer, D.O. Estimate of the carbon footprint of the US health care sector. JAMA 2009, 302, 1970–1972. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- British Atmospheric Data Centre. Available online: www.badc.nerc.ac.uk (accessed on 27 May 2015).
- Stedman, J.R. The Predicted number of air pollution related deaths in the UK during the August 2003 heatwave. Atmos. Environ. 2004, 38, 1087–1090. [Google Scholar] [CrossRef]
- Elliot, A.J.; Smith, S.; Dobney, A.; Thornes, J.E.; Smith, G.E.; Vardoulakis, S. Monitoring the effect of air pollution episodes on health care consultations and ambulance call-outs in England during March/April 2014: A retrospective observational analysis. Environ. Pollut. 2016, 214, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, H.L.; Heaviside, C.; Neal, L.S.; Agnew, P.; Thornes, J.E.; Vardoulakis, S. Mortality and emergency hospitalizations associated with atmospheric particulate matter episodes across the UK in spring 2014. Environ. Int. 2016, 97, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Sajani, S.Z.; Alessandrini, E.; Marchesi, S.; Lauriola, P. Are day-to-day variations of airbourne particles associated with emergency ambulance dispatches? Int. J. Occup. Environ. Health 2014, 20, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Bechtel, B.; Zakšek, K.; Oßenbrügge, J.; Kaveckis, G.; Böhner, J. Towards a satellite based monitoring of urban air temperatures. Sustain. Cities Soc. 2017. [Google Scholar] [CrossRef]
- See the Special Issue of Remote Sensing: The Application of Thermal Urban Remote Sensing to Understand and Monitor Urban Climates. Available online: https://www.mdpi.com/journal/remotesensing/special_issues/tirurbcli (accessed on 20 June 2017).
- Heaviside, C.; MacIntyre, H.; Vardoulakis, S. The Urban Heat Island: Implications for Health in a Changing Environment. Curr. Environ. Health Rep. 2017. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Cai, X.; Thornes, J.E. Birmingham’s air and surface urban heat islands associated with Lamb weather types and cloudless anticyclonic conditions. Prog. Phys. Geogr. 2014, 38, 431–447. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adelaide [6]: | Ambulance call-outs increased by 10% and by 16% in the 2008 and 2009 heat waves, respectively. Heat related dehydration appeared to promote acute renal failure. |
| Brisbane [7]: | Significant relationship between mean temperature and ambulance incidents (2000–2007) with a 1.17% increase in total incidents per 1 °C increase in temperature above a threshold of 22 °C (0 to 1 day lag). |
| Sydney [8]: | During the 2011 heat wave, all cause ambulance calls increased by 14% the additional calls mostly due to heat stroke, heat exhaustion and dehydration. |
| Toronto [9]: | Between 1999 and 2002, ambulance calls increased by 10% on oppressively hot days. GIS shows that the urban core experiences the greatest number of calls. |
| Toronto [10]: | For the summer of 2005, there were 201 ambulance response calls for heat related illness. On average, for every 1 °C increase in maximum temperature above average, there was a 29% increase in ambulance response calls for heat related illness. |
| Emilia-Romagna [11]: | For the summers of 2002–2006, for people over 35, the percentage change in ambulance dispatches associated with each 1 °C increase in the apparent mean temperature between 25 and 30 °C was 1.5% for non-traumatic diseases and 2.7% for respiratory diseases. Above 30 °C, cardiovascular diseases were positively associated especially for those aged over 75 with an increase of 12% in ambulance dispatches. |
| Florence [12]: | Ambulance and weather data for the summer of 2005 (13,354 calls) were examined. The overall number of calls rose in hotter conditions during the night: ‘oppressive night-time conditions might be more stressful than the maximum temperature’. A rise in alcohol-related diseases in hotter conditions relating to dehydration. |
| Ticino [13]: | Ambulance data from the 2003 heatwave showed that the number of incidents in June increased by 36% for the 65+ age group and 33% for the 75+ age group. |
| London [14]: | A heatwave vulnerability index (HVI) for London’s 4765 census units was developed for London that offers potential as an a priori spatial indicator of the number of heat related ambulance incidents. |
| London [15]: | For the London Ambulance Service, the daily percentage of CatA (Category A) (%CATA8) incidents responded to within the target of 8 min declines with increasing maximum daily air temperature. During hot weather for every 1 °C above 20 °C, the total number of incidents increases by 1% on average. |
| Brisbane [7]: | Cold weather effects were delayed and long lasting with a 1.30% increase in incidents for a decrease in temperature of 1 °C below the threshold of 22 °C (2–15 day lag). No harvesting was observed. |
| London [15]: | For December 2010, the coldest December for 100 years, the daily number of CatA incidents for the London Ambulance Service was nearly 20% higher than November 2010. |
| London [16]: | During cold weather for every 1 °C below 2 °C CatA performance declines by 1.5% on average. In cold weather, there are more incidents for flu, respiratory illnesses, fractures and head injuries. |
| Birmingham [17]: | Birmingham ambulance data was examined (2007–2011) and compared to air temperature data. Both hot and cold weather have an impact on response times (Target 75% of CatA incidents responded to in 8 min). In December 2010, the response rate fell below 50% for three days in a row with a mean response time of 15 min. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmood, M.A.; Thornes, J.E.; Pope, F.D.; Fisher, P.A.; Vardoulakis, S. Impact of Air Temperature on London Ambulance Call-Out Incidents and Response Times. Climate 2017, 5, 61. https://doi.org/10.3390/cli5030061
Mahmood MA, Thornes JE, Pope FD, Fisher PA, Vardoulakis S. Impact of Air Temperature on London Ambulance Call-Out Incidents and Response Times. Climate. 2017; 5(3):61. https://doi.org/10.3390/cli5030061
Chicago/Turabian StyleMahmood, Marliyyah A., John E. Thornes, Francis D. Pope, Paul A. Fisher, and Sotiris Vardoulakis. 2017. "Impact of Air Temperature on London Ambulance Call-Out Incidents and Response Times" Climate 5, no. 3: 61. https://doi.org/10.3390/cli5030061
APA StyleMahmood, M. A., Thornes, J. E., Pope, F. D., Fisher, P. A., & Vardoulakis, S. (2017). Impact of Air Temperature on London Ambulance Call-Out Incidents and Response Times. Climate, 5(3), 61. https://doi.org/10.3390/cli5030061