
Analysis of Continuing Airworthiness Occurrences under the Prism of a Learning Framework


Abstract
:
1. Introduction
2. Safety Reporting Background
2.1. International and European Regulatory Context
2.2. Learning from Incidents: Underpinning Theory
3. A Model Supporting Learning from Incidents
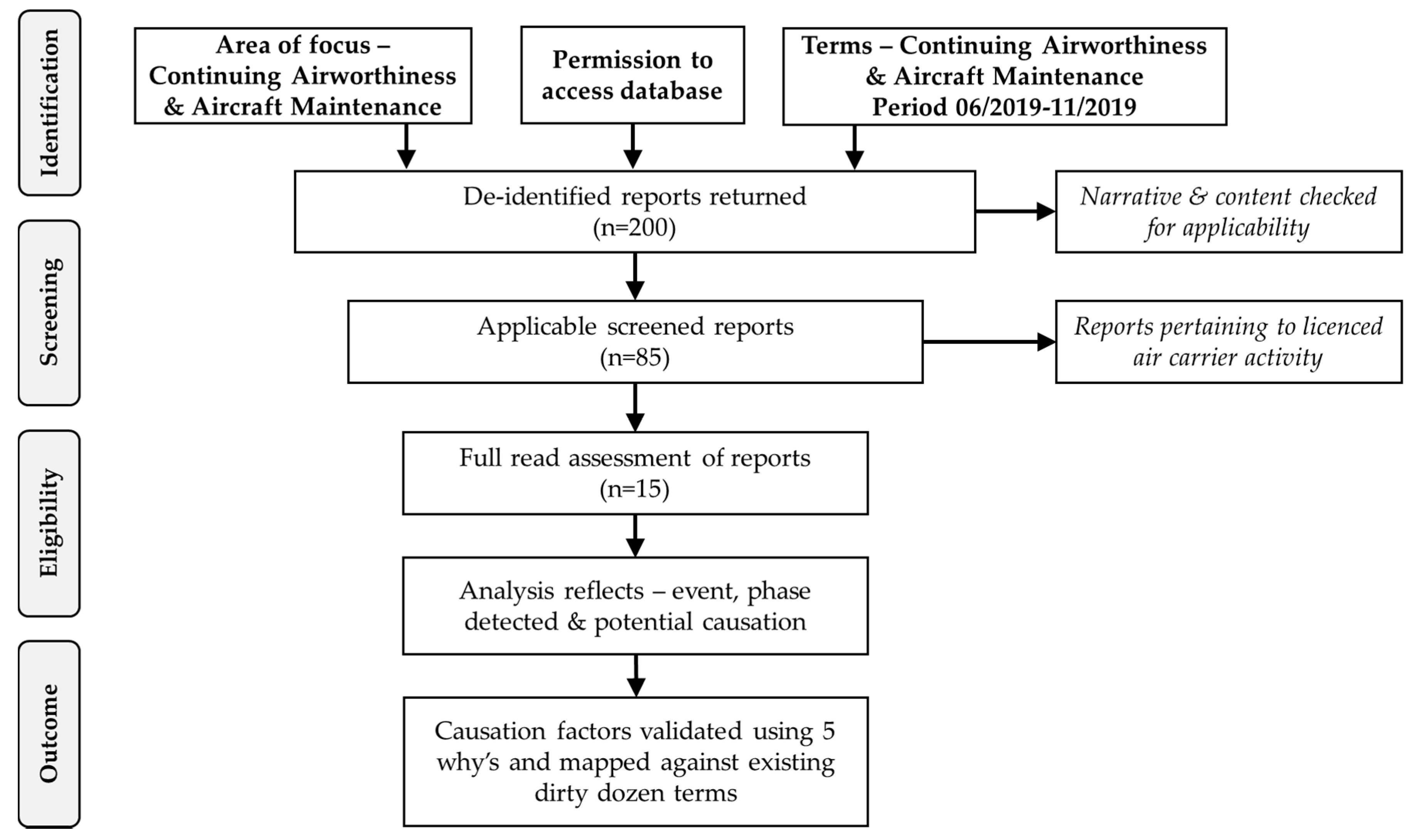
3.1. Model Design and Description
3.2. Model Implementation
3.3. Model Validation: Report Causal Elements
4. Results
- Lack of knowledge features as a primary element in 13 (87%) of 15 occurrences. This can be closely related to the competence required to perform the task as it relates to aircraft maintenance and continuing airworthiness management activities which are defined as comprising of ‘knowledge, skills and attitude/ability’ [4]. As a secondary potential contributing element, it relates to only 1 (7%) of the 15 occurrences.
- Lack of awareness is highlighted as a primary potential causation factor in 9 (60%) of the 15 reviewed occurrences. This element can be closely related to competence, communication and teamwork. As a secondary contributing factor, lack of awareness was noted during the review in 5 (33%) of 15 reviewed occurrences.
- Lack of resources were recorded in 3 (20%) of 15 events. Adequate resources are required in order for an operator to adequately staff an organisation so that an aircraft can be maintained to the correct standard and when required. EU 1321/2014 [4] mandates that a manpower plan is maintained in support of ensuring adequate levels of staff are consistently available. As a secondary issue, lack of resources appeared as an issue in 5 (33%) of 15 cases. Ultimately, accountable managers are the key to ensuring sufficient resources are made available so that the organisational elements continue to remain compliant and effective in this respect.
- Norms accounted for 3 (20%) of 15 reports examined. Norms are often viewed as behaviours that are developed and accepted within a group. However, when the resulting behaviour requires a deviation from approved procedural function, the consequences are often unknown. Although such actions may offer short-term productivity gains, they may also introduce active and latent safety hazards. In the case of secondary causation, norms are associated with 8 (53%) of 15 assessed occurrences.
- Lack of communication was found to be evident in 3 (20%) of 15 occurrences in the study. Communication in aircraft maintenance and management activities is a vital element in the release of a safe product. Poor communication can amplify many other elements of the human factors leading to a deterioration in human performance, Chatzi [32], Chatzi et al. [33]. 2 (13%) of the 15 reviewed communication-related occurrences were recorded as contributing to secondary event causation.
- Complacency was revealed as a primary factor in the causation of 1 (7%) of 15 events studied. However, as a secondary contributing factor it accounted for 5 (33%) of 15 reports. Stress levels associated with a task can diminish performance if one becomes complacent. Its presence can contribute in concert with other elements capable of setting the scene for an unwelcome event.
- Stress as a primary factor appeared in 1 (7%) of the 15 reviewed events. However, it was associated with 2 (13%) of 15 reports as a secondary issue. Stress can be both a by-product and an enabler of other Dirty Dozen elements. Fatigue for example can be closely coupled to stress and displayed similar pattern in the study with 7% and 13% respectively of prevalence in the reports reviewed.
- Lack of assertiveness was evident as a primary and as a secondary causation factor in both cases and occurring at rate of 1 (7%) of 15 events under review. Distraction and lack of teamwork appeared in similar proportions in the review results.
5. Discussion
5.1. Acquiring, Processing and Storing Incident Data
5.2. Single, Double and Triple-Loop Learning
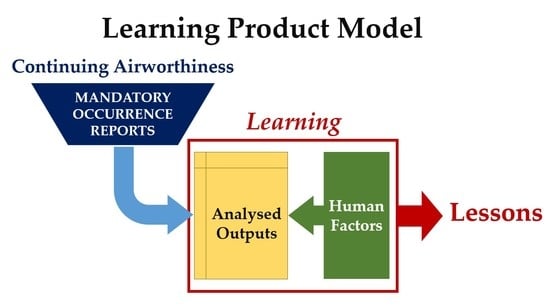
5.3. Learning Product
5.4. Effectiveness of Learning
5.5. Types of Knowledge
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silva, S.A.; Carvalho, H.; Oliveira, M.J.; Fialho, T.; Guedes Soares, C.; Jacinto, C. Organizational practices for learning with work accidents throughout their information cycle. Saf. Sci. 2017, 99, 102–114. [Google Scholar] [CrossRef]
- Akselsson, R.; Jacobsson, A.; Bötjesson, M.; Ek, Å.; Enander, A. Efficient and effective learning for safety from incidents. Work 2012, 41, 3216–3222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Document 32018R1139. Regulation (EU) 2018/1139 of the European Parliment and the Council of 4 July 2018 on common rules in trhe field of civil aviation and establishing a European Union Aviation Safety Agency, and amending Regulations (EC) No 2111/2005, (EC) No 1008/2008, (EU) No 996/2010, EU376/2014 and Directives 2014/30/EU of the European Parliment and the Council, and repealing Regulation (EC) No 216/2008 of the European Parliment and of the Council and Council Regulation (EEC) No 3922/91. In Official Journal of the European Union; European Commission: Brussels, Belgium, 2018; pp. 1–122. [Google Scholar]
- Document 32014R1321. Commission Regulation (EU) No 1321/2014 of 26 November 2014 on the continuing airworthiness of aircraft and aeronautical products, parts and appliances, and on the approval of organisations and personnel involved in these tasks. In Official Journal of the European Union; European Commission: Brussels, Belgium, 2014; pp. 1–194. [Google Scholar]
- Harvey, C.; Stanton, N.A. Safety in System-of-Systems: Ten key challenges. Saf. Sci. 2014, 70, 358–366. [Google Scholar] [CrossRef]
- Document 32014R0376. Regulation (EU) No 376/2014 of the European Parliament and of the Council of 3 April 2014 on the reporting, analysis and follow-up of occurrences in civil aviation, amending Regulation (EU) No 996/2010 of the European Parliament and of the Council and repealing Directive 2003/42/EC of the European Parliament and of the Council and Commission Regulations (EC) No 1321/2007 and (EC) No 1330/2007. In Official Journal of the European Union; European Commission: Brussels, Belgium, 2014; pp. 18–43. [Google Scholar]
- Transport Canada. Human Performance Factors for Elementary Work and Servicing; Canada, T., Ed.; Transport Canada: Ottawa, ON, Canada, 2003.
- FAA. 120-92B-Safety Management Systems for Aviation Service Providers; Federal Aviation Administration: Washington, WA, USA, 2015.
- ICAO. ICAO Annex 13 to the Convention on International Civil Aviation: Aircraft Accident and Incident Investigation. In Issue 10 Amendment 14; ICAO: Montreal, QC, Canada, 2010. [Google Scholar]
- ICAO. Convention on International Civil Aviation; Doc 7300; ICAO: Montreal, QC, Canada, 1944. [Google Scholar]
- ICAO. ICAO Accident/Incident Reporting Manual, 3rd ed.; ICAO: Montreal, QC, Canada, 2014. [Google Scholar]
- Boeing. Current Market Outlook 2015–2034; Boeing: Chicago, IL, USA, 2015. [Google Scholar]
- Leveson, N. A new accident model for engineering safer systems. Saf. Sci. 2004, 42, 237–270. [Google Scholar] [CrossRef] [Green Version]
- Deming, W. The New Econonics for Industry, Government, Education, 2nd ed.; MIT Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Bond, J. A Janus Approach to Safety. Process. Saf. Environ. Prot. 2002, 80, 9–15. [Google Scholar] [CrossRef]
- Drupsteen, L.; Guldenmund, F.W. What is Learning? A Review of the Safety Literature to Define Learning from Incidents, Accidents and Disasters. J. Contingencies Crisis Manag. 2014, 22, 81–96. [Google Scholar] [CrossRef]
- Hovden, J.; Størseth, F.; Tinmannsvik, R.K. Multilevel learning from accidents-Case studies in transport. Saf. Sci. 2011, 49, 98–105. [Google Scholar] [CrossRef]
- Jacobsson, A.; Ek, Å.; Akselsson, R. Method for evaluating learning from incidents using the idea of “level of learning”. J. Loss Prev. Process Ind. 2011, 24, 333–343. [Google Scholar] [CrossRef]
- Argyris, C.; Schön, D.A. Organizational Learning II: Theory, Method, and Practice; Addison-Wesley Publishing Company: Boston, MA, USA, 1996. [Google Scholar]
- Cooke, D.L. A system dynamics analysis of the Westray mine disaster. Syst. Dyn. Rev. 2003, 19, 139–166. [Google Scholar] [CrossRef]
- ED Decision 2020/002/R. Amending the Acceptable Means of Compliance and Guidance Material to Annex I (Part-M), Annex II (Part-145), Annex III (Part-66), Annex IV (Part-147) and Annex Va (Part-T) to as well as to the articles of Commission Regulation (EU) No 1321/2014, and issuing Acceptable Means of Compliance and Guidance Material to Annex Vb (Part-ML), Annex Vc (Part-CAMO) and Annex Vd (Part-CAO) to that Regulation. In Official Journal of the European Union; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- ICAO. Annex 19 to the Convention on International Civil Aviation Safety Management. In Safety Management; ICAO: Montreal, QC, Canada, 2013. [Google Scholar]
- Document 52011DC0670. Communication from the Commission to the Council and the European Parliament Setting up an Aviation Safety Management System for Europe. In Setting up an Aviation Safety Management System for Europe; European Commission: Brussels, Belgium, 2011. [Google Scholar]
- Cooke, D.L.; Rohleder, T.R. Learning from incidents: From normal accidents to high reliability. Syst. Dyn. Rev. 2006, 22, 213–239. [Google Scholar] [CrossRef]
- Drupsteen, L.; Groeneweg, J.; Zwetsloot, G.I. Critical steps in learning from incidents: Using learning potential in the process from reporting an incident to accident prevention. Int. J. Occup. Saf. Ergon. 2013, 19, 63–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paradies, M.; Busch, D. Root cause analysis at Savannah River plant (nuclear power station). In Proceedings of the Conference Record for 1988 IEEE Fourth Conference on Human Factors and Power Plants, Monterey, CA, USA, 5–9 June 1988; pp. 479–483. [Google Scholar]
- Card, A.J. The problem with ‘5 whys’. BMJ Qual. Saf. 2017, 26, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Ohno, T. Toyota Production System: Beyond Large-Scale Production; CRC Press: Boca Raton, FL, USA, 1988. [Google Scholar]
- Bloom, B.S. Taxonomy of Educational Objectives; Cognitive Domain; Edwards Bros: Ann Arbor, MI, USA, 1956; Volume 20, p. 24. [Google Scholar]
- Anderson, L.W.; Sosniak, L.A. Bloom’s Taxonomy; Chicago Press: Chicago, IL, USA, 1994. [Google Scholar]
- Chatzi, A.V. The Diagnosis of Communication and Trust in Aviation Maintenance (DiCTAM) Model. Aerospace 2019, 6, 120. [Google Scholar] [CrossRef] [Green Version]
- Chatzi, A.V.; Martin, W.; Bates, P.; Murray, P. The unexplored link between communication and trust in aviation maintenance practice. Aerospace 2019, 6, 66. [Google Scholar] [CrossRef] [Green Version]
- Garvin, D.A. Building a Learning Organization; Harvard Business Review July-August: Brighton, MA, USA, 1993; Volume 71. [Google Scholar]
- Lukic, D.; Littlejohn, A.; Margaryan, A. A framework for learning from incidents in the workplace. Saf. Sci. 2012, 50, 950–957. [Google Scholar] [CrossRef]
- Bateson, G. The Logical Categories of Learning and Communication. Steps to an Ecolology of Mind; Ballantine Books: New York, NY, USA, 1972; pp. 279–308. [Google Scholar]
- Lampel, J.; Shamsie, J.; Shapira, Z. Experiencing the improbable: Rare events and organizational learning. Organ. Sci. 2009, 20, 835–845. [Google Scholar] [CrossRef]
- McDonald, N.; Corrigan, S.; Daly, C.; Cromie, S. Safety management systems and safety culture in aircraft maintenance organisations. Saf. Sci. 2000, 34, 151–176. [Google Scholar] [CrossRef]
- Von Thaden, T.L.; Gibbons, A.M. The Safety Culture Indicator Scale Measurement System (SCISMS); National Technical Information Service Final Report; Office of Aviation Research and Development: Washington, DC, USA, 2008; pp. 1–57.
- Thorndike, E.L. Fundamental theorems in judging men. J. Appl. Psychol. 1918, 2, 67. [Google Scholar] [CrossRef]
- Reason, J.T. Managing the Risk of Organisational Accidents; Ashgate Publishing: Farnham, UK, 1997. [Google Scholar]
- ICAO. Safety Management Manual; Doc 9859; ICAO: Montreal, QC, Canada, 2013. [Google Scholar]
- Perrow, C. Normal Accidents Living with High-Risk Technologies. In With a New Afterword and a Postscript on the Y2K Problem; Perrow, C., Ed.; Princeton University Press: Princeton, NJ, USA, 1999. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Potential Causation Factors for Each Incident | Dirty Dozen ‘Taxonomy’ | ||
|---|---|---|---|
| Primary | Secondary | ||
| 1 | Incorrect tooling Competence for task Task sequencing | Lack of resources Lack of knowledge (Knowledge, skills, ability) Complacency Lack of awareness | Norms established Lack of communication Lack of assertiveness |
| 2 | Continuing Airworthiness Management Organisation (CAMO) management system competence Production pressure | Lack of knowledge (procedures & knowledge, skills, ability) Lack of communication Pressure | Lack of resources Stress Fatigue/Stress/Distraction |
| 3 | Inadequate aircraft maintenance programme (AMP) inspection task Product design | Norms established Lack of communication | Lack of awareness Lack of resources |
| 4 | Inadvertent damage Incorrect gauge of locking wire & locking technique | Distraction Lack of knowledge (Knowledge, skills, ability) Fatigue Lack of teamwork | Complacency Lack of awareness |
| 5 | CAMO work request incorrect Maintenance procedure not followed | Lack of knowledge (Knowledge, skills, ability) Pressure Lack of assertiveness | Norms established Lack of resources |
| 6 | Procedure design Production pressure Competence for task CAMO management system competence | Lack of knowledge Pressure Lack of awareness Lack of communication | Lack of resources Fatigue/Stress/Distraction Lack of supervision |
| 7 | Production pressure Competence for maintenance task | Pressure Lack of knowledge (Knowledge, skills, ability) | Fatigue/Stress/Distraction Lack of resources |
| 8 | Maintenance data availability Production pressure Competence for task | Lack of resources Lack of knowledge Pressure | Norms established Fatigue Lack of awareness |
| 9 | Procedure design Production pressure Supervision Competence for maintenance task | Lack of knowledge (Procedures) Pressure Lack of knowledge (Knowledge, skills, ability) | Lack of awareness Lack of communication Complacency Lack of assertiveness |
| 10 | Incorrect tooling Competence for maintenance task Task sequencing | Lack of knowledge Lack of awareness Lack of communication | Norms Lack of resources |
| 11 | Maintenance data Procedure design Production pressure Competence for maintenance task Post task leak-check | Lack of knowledge (Knowledge, skills, ability) Pressure Lack of awareness | Lack of teamwork Complacency Fatigue/Stress/Distraction Lack of resources |
| 12 | Production pressure Competence for maintenance task Maintenance data availability Supervision | Pressure Lack of knowledge Lack of teamwork | Fatigue/Stress/Distraction Lack of resources |
| 13 | Competence for maintenance task Production pressure | Lack of knowledge Pressure | Fatigue/Stress/Distraction |
| 14 | Culture Risk taking Competence Supervision | Norms established Lack of resources Lack of knowledge (Knowledge, skills, ability) | Lack of awareness Complacency Lack of communication |
| 15 | CAMO procedure competence Culture Supervision | Lack of knowledge (Knowledge, skills, ability) Norms Stress | Lack of awareness Lack of resources Pressure |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clare, J.; Kourousis, K.I. Analysis of Continuing Airworthiness Occurrences under the Prism of a Learning Framework. Aerospace 2021, 8, 41. https://doi.org/10.3390/aerospace8020041
Clare J, Kourousis KI. Analysis of Continuing Airworthiness Occurrences under the Prism of a Learning Framework. Aerospace. 2021; 8(2):41. https://doi.org/10.3390/aerospace8020041
Chicago/Turabian StyleClare, James, and Kyriakos I. Kourousis. 2021. "Analysis of Continuing Airworthiness Occurrences under the Prism of a Learning Framework" Aerospace 8, no. 2: 41. https://doi.org/10.3390/aerospace8020041
APA StyleClare, J., & Kourousis, K. I. (2021). Analysis of Continuing Airworthiness Occurrences under the Prism of a Learning Framework. Aerospace, 8(2), 41. https://doi.org/10.3390/aerospace8020041