
Examining Routine Pediatric Vaccination Availability in Community Pharmacies in Washington State


Abstract
:1. Introduction
2. Materials and Methods
Design
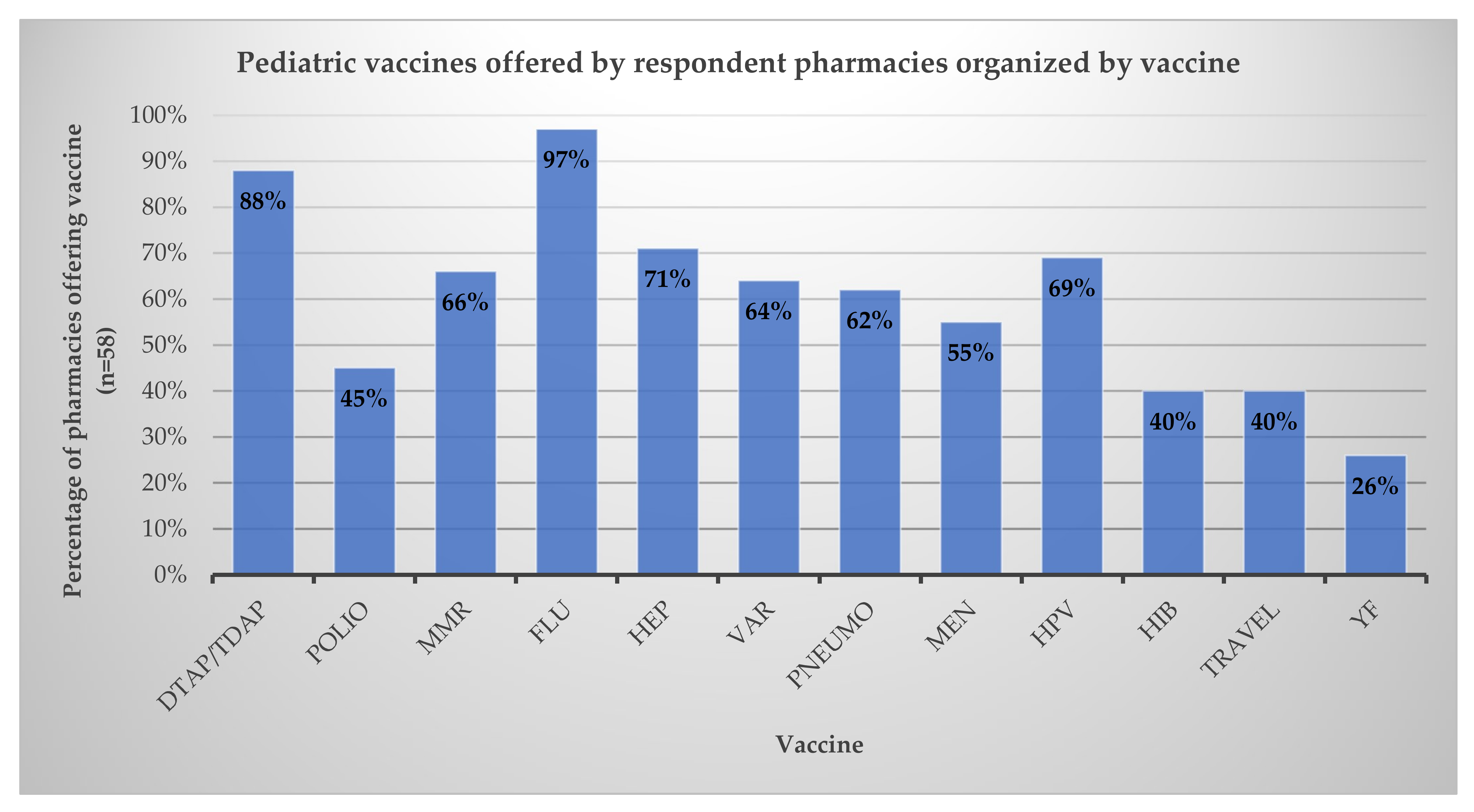
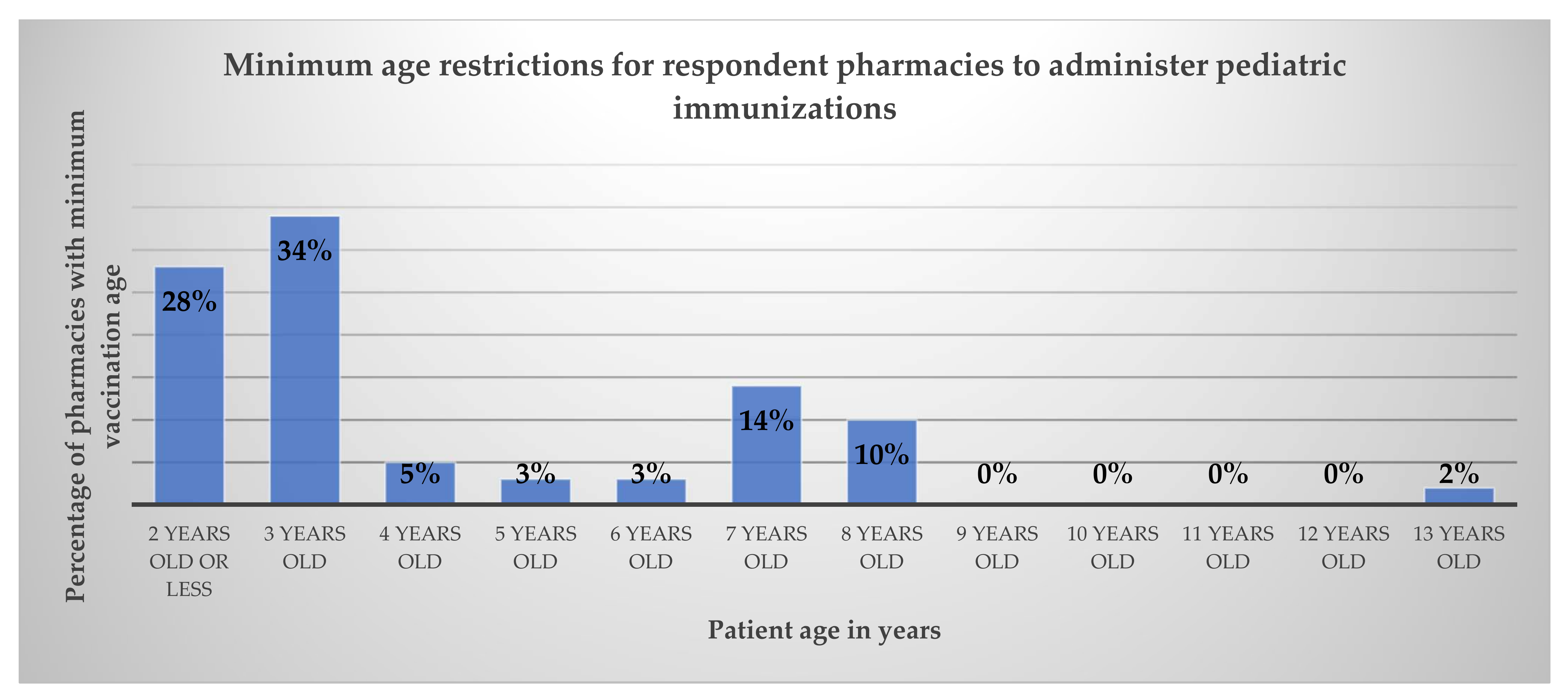
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Immunization and Infectious Diseases. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/immunization-and-infectious-diseases (accessed on 13 March 2022).
- Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 14 August 2022).
- Whitney, C.G.; Zhou, F.; Singleton, J.; Schuchat, A. Benefits from Immunization During the Vaccines for Children Program Era—United States, 1994–2013. MMWR 2014, 63, 352–355. [Google Scholar] [PubMed]
- Child and Adolescent Immunization Schedule. Available online: https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html#birth-15 (accessed on 29 September 2022).
- IID-8: State-Level Data Map. Available online: https://www.healthypeople.gov/2020/data/map/4722?year=2018 (accessed on 6 November 2021).
- 2020 Survey of America’s Physicians COVID-19 Impact Edition. Available online: https://physiciansfoundation.org/wp-content/uploads/2020/08/20-1278-Merritt-Hawkins-2020-Physicians-Foundation-Survey.6.pdf (accessed on 30 August 2022).
- 2021 Survey of America’s Physicians COVID-19 Impact Edition A Year Later. Available online: https://physiciansfoundation.org/wp-content/uploads/2021/08/2021-Survey-Of-Americas-Physicians-Covid-19-Impact-Edition-A-Year-Later.pdf (accessed on 2 March 2022).
- Santoli, J.M.; Lindley, M.C.; DeSilva, M.B.; Kharbanda, E.O.; Daley, M.F.; Galloway, L.; Gee, J.; Glover, M.; Herring, B.; Kang, Y.; et al. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration—United States, 2020. MMWR 2020, 69, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Patel Murthy, B.; Zell, E.; Kirtland, K.; Jones-Jack, N.; Harris, L.; Sprague, C.; Schultz, J.; Le, Q.; Bramer, C.A.; Kuramoto, S.; et al. Impact of the COVID-19 Pandemic on Administration of Selected Routine Childhood and Adolescent Vaccinations—10 U.S. Jurisdictions, March-September 2020. MMWR 2021, 70, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Kujawski, S.A.; Yao, L.; Wang, H.E.; Carias, C.; Chen, Y.T. Impact of the COVID-19 pandemic on pediatric and adolescent vaccinations and well child visits in the United States: A database analysis. Vaccine 2022, 40, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Third Amendment to Declaration Under the Public Readiness and Emergency Preparedness Act for Medical Countermeasures Against COVID–19. Available online: https://www.govinfo.gov/content/pkg/FR-2020-08-24/pdf/2020-18542.pdf (accessed on 30 August 2022).
- Public Readiness and Emergency Preparedness Act. Available online: https://www.phe.gov/Preparedness/legal/prepact/Pages/default.aspx (accessed on 10 April 2022).
- Pharmacist Immunization Authority. Available online: https://naspa.us/resource/pharmacist-authority-to-immunize/ (accessed on 6 November 2022).
- Vaccinations & Injections. Available online: https://www.cvs.com/minuteclinic/services/vaccinations-and-injections/N-d8Z3a3joZd5 (accessed on 13 March 2022).
- Immunizations. Available online: https://www.walgreens.com/pharmacy/immunization/immunization_index.jsp (accessed on 13 March 2022).
- The Little Clinic. Available online: http://www.kroger.com/i/coronavirus-update/the-little-clinic (accessed on 13 March 2022).
- Rite Aid Pharmacy. Available online: https://www.riteaid.com/pharmacy (accessed on 13 March 2022).
- COVID-19 Vaccination Federal Retail Pharmacy Partnership Program. Available online: https://www.cdc.gov/vaccines/covid-19/retail-pharmacy-program/index.html (accessed on 6 November 2021).
- COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 28 February 2022).
- Updated Pediatric COVID-19 Vaccination Operational Planning Guide—Information for the COVID-19 Vaccine for Children 6 Months–4 Years Old. Available online: https://www.cdc.gov/vaccines/covid-19/downloads/Pediatric-Planning-Guide.pdf (accessed on 28 February 2022).
- McKeirnan, K.C.; Frazier, K.R.; Nguyen, M.; MacLean, L.G. Training pharmacy technicians to administer immunizations. J. Am. Pharm. Assoc. 2018, 58, 174–178.e1. [Google Scholar] [CrossRef] [PubMed]
- McKeirnan, K.C.; McDonough, R.P. Transforming pharmacy practice: Advancing the role of technicians. Pharm. Today 2018, 24, 54–61. [Google Scholar] [CrossRef]
- HealthMap Vaccine Finder. Available online: https://vaccinefinder.org/ (accessed on 1 March 2022).
- DeSilva, M.B.; Haapala, J.; Vazquez-Benitez, G.; Daley, M.F.; Nordin, J.D.; Klein, N.P.; Henninger, M.L.; Williams, J.; Hambidge, S.J.; Jackson, M.L.; et al. Association of the COVID-19 Pandemic with Routine Childhood Vaccination Rates and Proportion Up to Date with Vaccinations Across 8 US Health Systems in the Vaccine Safety Datalink. JAMA Pediatr. 2021, 176, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Bramer, C.A.; Kimmins, L.M.; Swanson, R.; Kuo, J.; Vranesich, P.; Jacques-Carroll, L.A.; Shen, A.K. Decline in child vaccination coverage during the COVID-19 pandemic—Michigan Care Improvement Registry, May 2016–May 2020. Am. J. Transpl. 2020, 20, 1930–1931. [Google Scholar] [CrossRef] [PubMed]
- CDC Streamlines COVID-10 Guidance to Help the Public Better Protect Themselves and Understand Their Risk. Available online: https://www.cdc.gov/media/releases/2022/p0811-covid-guidance.html (accessed on 30 September 2022).
- Ackerson, B.K.; Sy, L.S.; Glenn, S.C.; Qian, L.; Park, C.H.; Riewerts, R.J.; Jacobsen, S.J. Pediatric Vaccination During the COVID-19 Pandemic. Pediatrics 2020, 148, e2020047092. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Item Number | Question |
|---|---|
| 1 | What is your role in your current pharmacy position? (pharmacist, intern, technician, assistant) |
| 2 | What gender do you most identify with? (male, female, other, prefer not to answer) |
| 3 | What is your age? |
| 4 | Are you a full-time or part-time employee at your pharmacy? |
| 5 | How long have you worked in pharmacy practice? |
| 6 | How long have you worked at this pharmacy? |
| 7 | How often does your pharmacy immunize pediatric patients? (daily, weekly, monthly, yearly, or not at all) |
| 8 | What is the minimum age for patients to receive immunizations at your pharmacy? (age in years) |
| 9 | Which diseases does your pharmacy offer vaccines against for pediatric patients? (ACIP-recommended vaccines for pediatric patients) |
| 10 | Are there any pediatric vaccines requested by your current patients that you do not offer? (ACIP-recommended vaccines for pediatric patients) |
| Demographic | n (%) |
|---|---|
| Current pharmacy position | |
| Pharmacist | 40 (69%) |
| Pharmacy Intern | 8 (14%) |
| Pharmacy Technician | 10 (17%) |
| Pharmacy Assistant | 0 (0%) |
| Gender | |
| Male | 17 (29%) |
| Female | 41 (71%) |
| Prefer not to answer | 0 (0%) |
| Employment status | |
| Full time | 42 (72%) |
| Part time | 16 (28%) |
| Age and Experience | |
| Average age | 35.8 years (range 22 to 65 years) |
| Average years in practice | 11.7 years (range <1 to 50 years) |
| Average years employed at this pharmacy | 6.6 years (range <1 to 50 years) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKeirnan, K.C.; Motzner, M.S.; Kherghehpoush, S. Examining Routine Pediatric Vaccination Availability in Community Pharmacies in Washington State. Pharmacy 2022, 10, 156. https://doi.org/10.3390/pharmacy10060156
McKeirnan KC, Motzner MS, Kherghehpoush S. Examining Routine Pediatric Vaccination Availability in Community Pharmacies in Washington State. Pharmacy. 2022; 10(6):156. https://doi.org/10.3390/pharmacy10060156
Chicago/Turabian StyleMcKeirnan, Kimberly Caye, Madison Shea Motzner, and Sorosh Kherghehpoush. 2022. "Examining Routine Pediatric Vaccination Availability in Community Pharmacies in Washington State" Pharmacy 10, no. 6: 156. https://doi.org/10.3390/pharmacy10060156
APA StyleMcKeirnan, K. C., Motzner, M. S., & Kherghehpoush, S. (2022). Examining Routine Pediatric Vaccination Availability in Community Pharmacies in Washington State. Pharmacy, 10(6), 156. https://doi.org/10.3390/pharmacy10060156