1. Introduction
Pharmacokinetics encompasses multiple complex concepts and skills taught in the Doctor of Pharmacy (Pharm.D.) curricula. The Accreditation Council for Pharmacy Education’s 2016 standards require education on clinical pharmacokinetics, noting learners’ need to calculate appropriate doses and adjust therapy for safety and outcomes [
1]. Variation exists in how clinical pharmacokinetics is taught across colleges of pharmacy, suggesting that process improvements are possible [
2]. Additionally, there can be multiple reasonable therapeutic options, yet course work involving a mathematical calculation often directs students to a single correct answer. Team-based learning (TBL) is one educational method which can promote discussion, critical thinking, and timely feedback to engage learners in complex decision-making skills.
The main goal of TBL is to scaffold student learning in a manner requiring the application of taught material to address real-world issues through critical thinking [
3]. TBL may improve transferable skills through peer learning and academic performance [
4,
5,
6,
7]. TBL includes four core components: assignment design, group assignment, accountability, and feedback [
8]. TBL assignments require the same problem to be provided to all groups. Learner accountability is often tracked through an Individual Readiness Assurance Test (IRAT) followed by a Team Readiness Assurance Test (TRAT). Feedback for testing and TBL performance is provided in real time. High-quality TBL activities in pharmacy education should use authentic pharmacy challenges/situations regarding relevant pharmacy tasks, which encourage rich discussion and provide effective feedback to the groups [
9].
Pharmaceutical Skills courses provide students the opportunity to apply materials learned in other courses. In an effort to enhance pharmacokinetics learning, a vancomycin dosing TBL case series was added to a second-year Pharmaceutical Skills IV course (“Skills”), aligned with the simultaneously offered Clinical Pharmacokinetics/Pharmacodynamics II (“cPKPD”) course. Vancomycin dosing is a common clinical pharmacokinetics consultation. The primary course content for vancomycin dosing was provided in the cPKPD course in the Spring of the second year of the Pharm.D. curriculum at the time this learning activity was implemented. The vancomycin dosing content consisted of estimating renal function, estimating volume of distribution, estimating vancomycin elimination rate, determining initial vancomycin doses and regimens, monitoring the appropriate therapeutic drug, adjusting doses, and pulse dosing. In the cPKPD class, students received practice problems and clinical vignettes (more lengthy, multi-step clinical scenarios) during class (multiple per lecture hour), followed by a homework problem set for students to solve that was concurrent with the module content (provided at the start and due just prior to the exam day). Given this structure, the assigned homework was not graded prior to the exams. However, students were familiar with case-based questions before the Skills TBL activity. The report herein describes the TBL activity in Skills and the learning outcomes assessed in the cPKPD course.
2. Materials and Methods
The study objective was to assess the impact of a newly implemented TBL activity within the Skills course on student performance, between two class years, on related material on cPKPD exams. The University of South Florida Institutional Review Board waived review.
The TBL activity was developed collaboratively by the Skills and cPKPD course coordinators with feedback from a TBL expert [
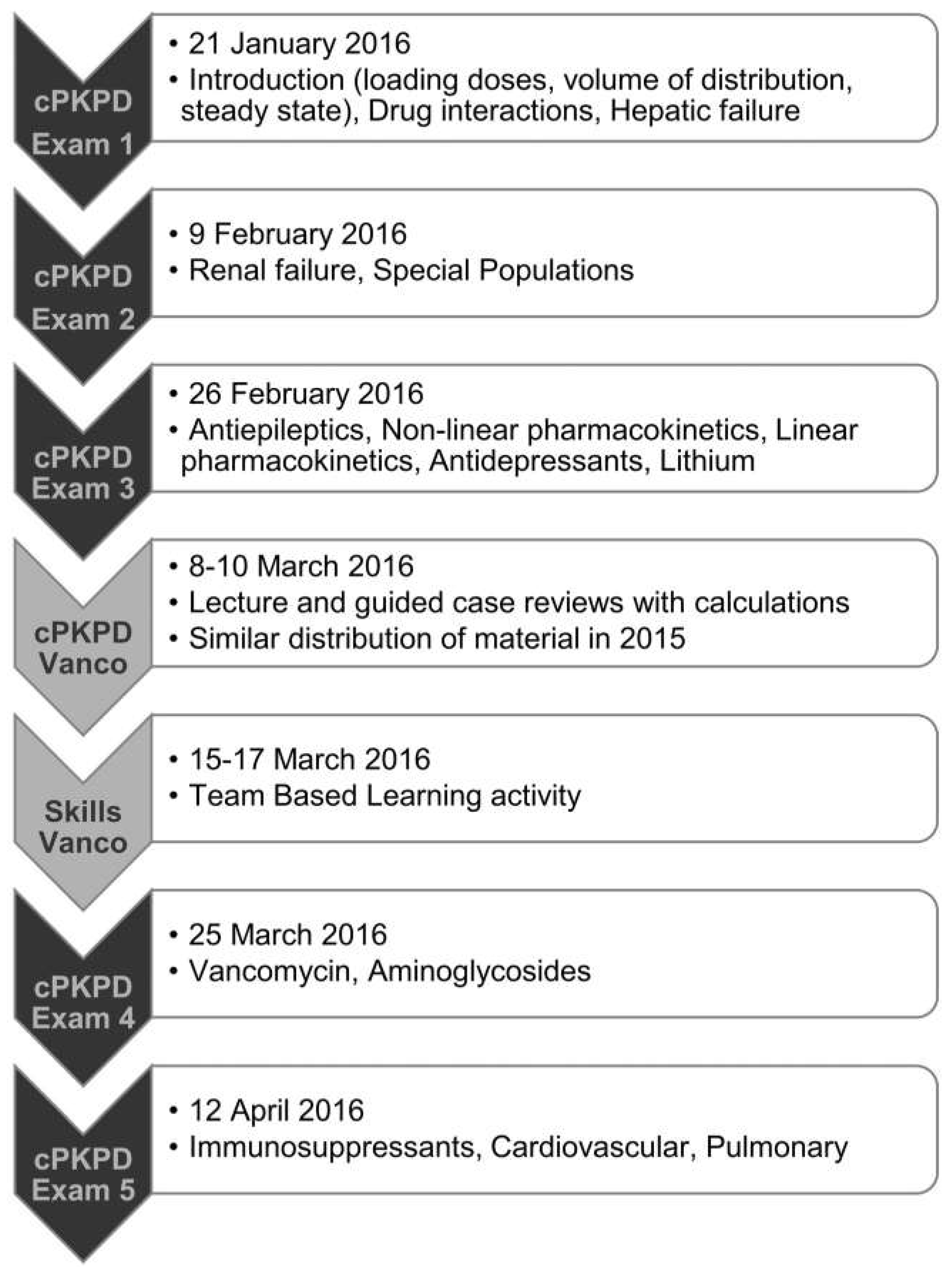
10]. The cPKPD course was a 3-credit hour course, with up to 6 h dedicated to teaching vancomycin content—at least 3 h of lecture, with up to 3 h of working problem sets with vancomycin dosing calculations and related clinical scenarios. The course activity sequence is shown in
Figure 1 with the cPKPD exam covering vancomycin occurring 8 or 10 days after the vancomycin TBL activity depending on which class section the students attended. It was the students’ first exposure to TBL as part of the standard Pharm.D. curriculum. The activity materials (
Appendix A,
Appendix B,
Appendix C,
Appendix D,
Appendix E and
Appendix F) are from 2020, minimally modified from the 2016 materials. Changes address typographical errors, clarity in language, and removal of discussion regarding D-test and interpreting culture data. The TBL activity was designed to communicate the clinical relevance and importance of safe and effective vancomycin dosing and required learner accountability at each step (i.e., IRAT, TRAT, verbal defense).
For in-class, small-group work, 85 students worked with their assigned “class groups” which met Tuesday or Thursday. Groups included six to eight students. Two students were absent for the activity. Two students typically scheduled for Tuesday were granted permission to attend the Thursday session and were integrated into an existing group. The in-class TBL activity was led by the skills coordinator during a 2-h and 50-min class period in a large-group learning room. The cPKPD course coordinator attended class sessions to answer questions pertaining to alignment of course material and to relate it to the upcoming cPKPD exam.
The focus of the TBL activity was application of previously learned materials for patient assessment, critical thinking, and clinical decision-making. Calculations were required to complete the activities; however, the primary focus remained on interpretation of the calculated values (
Appendix D). A vancomycin dosing protocol was developed and provided to ensure groups used identical methods of dosing to create consistency in calculated values (e.g., all vancomycin doses ≤ 2 g administered over 2 h) to ensure the discussion was streamlined toward patient assessment and clinical decisions rather than calculations (
Appendix F).
The learning objectives of the TBL activity were for students to be able to 1) assess a patient case to determine the best application of estimated renal function, 2) select an appropriate initial vancomycin dose (regimen or one-time dose), and 3) establish a monitoring plan based on changing renal function to determine future dose. Prior to the in-class TBL activity, students completed a “pre-preparation quiz” (
Appendix A) to assess learned material from cPKPD. Students were assigned two readings to facilitate their preparation and a list of values to be able to calculate (
Appendix B).
At the beginning of class, students individually completed an IRAT (~10 min) and then completed the same assessment as a group, TRAT (~5 min) (
Appendix C). The skills coordinator led a quiz debrief and emphasized the purpose and organization of the TBL activity (~10 min). Next, the TBL activity moved into group participation on the case series (~2-h and 25-min) (
Appendix D). The TBL activity followed a pharmacokinetic consult for vancomycin in a single patient during an inpatient stay over five “patient case-days”. Groups reviewed the patient’s presentation, made assessments, and chose clinical action. For each patient case-day, groups had ~15–20 min to work up the case. During this time, groups decided on their preferred answer to each question. Groups were held accountable to their preferred answer by holding up a response card for the discussion question being addressed [
11]. When called on, groups verbally defended the reasoning for their answer. Following discussion, the instructor clarified, confirmed, and summarized the salient points relating back to the activity learning objectives. This process repeated for all questions for each case-day.
Following the activity, an anonymous survey was distributed (
Appendix E) assessing general opinions about the activity, not related to a specific learning outcome, and, therefore, it was not formally validated. The components of the TBL activity were graded for participation: pre-preparation quiz (20% of activity grade), IRAT (10% of activity grade), TRAT (20% of activity grade), TBL patient case activity (30% of activity grade), and end of activity survey (20% of activity grade).
Vancomycin dosing summative assessments occurred in cPKPD course exams. To avoid bias from retrospectively comparing raw exam scores on non-identical exams (2015 versus 2016), we compared percent of points possible earned by the class by topic between years. To complete this comparison between class years, the question topic and question type of every exam question on all cPKPD course exams for each course year were assessed. In both years, exams were composed of the same question types: multiple choice, true–false, fill in the blank, and essay. Then the percents of points possible earned by the class years were compared between years, by question topic. As such, the topic with the highest percent of points possible earned by an entire class year, on all associated questions, would be considered the easiest topic. Whereas the topic with the lowest percent of points possible earned by the entire class year would be considered the hardest topic. The primary outcome was change in topic performance by rank difficulty, to minimize potential confounding. Assessing student learning by question topic area assumes that, in general, harder topics remain harder and easier topics remain easier. This approach is less prone to bias compared to the assumptions required for comparing raw exam scores (i.e., that student ability and exam difficulty are the same year over year).
Students without exam data for all exams assessed during the study period were removed from the data set, as were questions on cPKPD exams with missing data or which were dropped from the exam score or had all responses accepted as correct. As a retrospective study, determination to exclude questions in the final grade (e.g., dropped questions) were not performed in a protocolized fashion, though course coordinators evaluated question quality and item performance. As such, all questions meeting the criteria above were included in the present analysis. Prior to the study results being reviewed by the cPKPD course coordinator, that course coordinator assessed the cPKPD course for changes in topic instructors, instruction methods, and content hours. Survey data were manually entered into REDCap electronic data capture tools hosted at the University of South Florida [
12,
13].
3. Results
The final data set for analysis included 101 students from year 1, with 4 excluded for missing exam data, and 84 students from year 2, with 1 excluded for missing exam data. Four of the five Pharmacokinetics exams were assessed. Exam 1 was excluded from both years due to missing data. Over four exams in year 1, 149 questions were assessed. Eighteen questions were excluded for not being scored. Across all topics in year 1, a total of 291.8 points were possible on the assessed questions. Over four exams in year 2, 130 questions were assessed. One question was excluded for not being scored. Across all topics in year 2, a total of 332.18 points were possible on the assessed questions. Two students in year 2 did not participate in the TBL activity. One student’s exams scores were included in the analysis. One student was excluded for incomplete exam data. The only major change identified in the cPKPD course was a change in the instructor teaching theophylline and digoxin content (
Table 1).
The mean ± standard deviation score on the pre-preparation quiz before the TBL activity was 3.9 ± 1.06 (5 possible points, 78%). The mean IRAT performance was 5.5 ± 1.88 (10 points possible, 55%). Questions with relatively lower performance (<50% correct) on IRAT were calculation-based (questions 2, 6, 7, 8) rather than conceptual knowledge-based. One exception was that 37% of students answered question 10 correctly, which regarded a pre-reading topic addressing when to proactively change a vancomycin regimen before obtaining a first trough. The IRAT score did not differ between class days (mean ± standard deviation; day-one 5.45 ± 1.92, day-two 5.56 ± 1.90; p = 0.80). The mean TRAT score on the only attempt was 10 out of 10 points.
Overall, the data demonstrate a year-over-year decrease in raw exam scores. By topic, the largest single improvement in rank topic performance was warfarin (
Table 2). However, this was matched with a decline in warfarin interaction performance. A large improvement in the rank topic performance was observed in heparin, followed by vancomycin. Neither heparin nor vancomycin showed a meaningful absolute increase in the percent of points possible earned on the raw exam scores (both <1% absolute increase). Therefore, their change in rank is related to the maintenance of the percent of points possible earned, and their relative rank improvement related to the number of topics with a year-over-year decrease in percent of points possible earned. When restricting the analysis to topics with at least eight questions in each year (
Table 3), the trend of decreased raw exam scores remained. Similarly, heparin and vancomycin remained the topics with the largest rank improvement. Notably, while vancomycin demonstrated a maintenance in the percent of points possible earned year over year, there was a large decrease in aminoglycoside’s percent of points possible earned year over year. No discernable trend was identified by Bloom’s taxonomy or question type.
Both increases and decreases in the proportion of recall-based questions co-occurred with increases and decreases in topic performance. Similarly, both increase and decreases in the proportion of multiple-choice questions co-occurred with increases and decreases in topic performance (Data not shown). Survey data demonstrated a positive view on the group dynamics and interdependence (
Table 4). The majority of students either strongly agreed or agreed that their abilities improved regarding applying pharmacokinetic concepts, understanding of renally cleared medications, how renal function and volume of distribution affects vancomycin dosing, and linear pharmacokinetics.
4. Discussion
Overall, this study suggests moderately improved learning with an aligned TBL activity between the Skills course and the cPKPD course. While raw scores did not improve, the a priori analysis method accounted for this by comparing topic performance between years. In support of our conclusion of improved vancomycin learning with the vancomycin dosing activity, there was a notable decline in aminoglycoside performance, while vancomycin performance was maintained. The decrease in aminoglycoside performance is in line with the general decline in raw exam scores year over year. Potential reasons aminoglycosides did not see a corollary benefit related to the enhanced education on vancomycin may be due to 1) no additional aminoglycoside practice problems, 2) the multiple different dosing strategies with aminoglycosides (e.g., Hartford nomogram), and 3) the dose adjustments with aminoglycosides versus vancomycin in the presence of renal dysfunction being dissimilar.
Overall, the activity reinforced the pharmacokinetic skills taught in cPKPD. The alignment between courses and use of TBL seemed to support student learning and abilities in a complex, variable topic. This is an important application opportunity, as safe and effective pharmacokinetic dosing cannot rely on rote memorization and requires experience and application to support learners’ abilities, skills, and confidence. Importantly, the results of the present study are in line with prior assessments of including TBL in pharmacokinetic course work [
14,
15]. In addition to case-based questions, immediate feedback given after the TRAT and case discussions assesses students’ mastery of course outcomes, encourages deep learning and critical thinking skills, and is preferred by students [
15]. One eight-year retrospective review identified that increasing amounts of active learning increased student performance, despite the potential for decreased student evaluations [
14]. Similarly, another study identified that multiple strategies for including case-based learning resulted in improved exam scores compared to more traditional teaching methods [
15]. Additionally, the results being in line with prior research on active learning points to a strength of our study design—that being, that rank difficultly as an assessment of performance following a targeted intervention may be more able to identify differences (compared to raw exam score comparisons) in a pre–post retrospective study.
There are some limitations to the study and the interpretation of the results. While the score on the pre-preparation quiz (78%) suggests reasonable baseline knowledge following the cPKPD course work, the mean IRAT performance (55%) suggests a low level of preparation specific to the TBL activity, potentially relating to how points were earned (completion). However, the high performance on TRAT suggests the opportunity for peer teaching and activity readiness. Moreover, the enhanced learning observed regarding vancomycin is consistent with the study’s survey results and prior reports of enhanced student performance [
6,
7]. Additionally, the cohorts were not matched, and there was variation in the exam performance between class years. The data analysis strategy accounted for varying ability between cohorts, somewhat, and the differing ability between class years is not generally unexpected and, further, was in line with class metrics [
16]. The analysis strategy assumes that topic difficulty remains similar year over year. In support of this assumption, 50% of topics had a change in rank ≤ 2. Additionally, the analysis only included two class years, and, as such, inferential statistics were not possible. There were no controls over teaching methods between years, though content changes were minimal. Additionally, there were no controls on student workload, effort on other courses, or effort on outside activities. It is possible that the ratio of students in inpatient versus outpatient internship experiences changed year over year. However, we would not expect this to impact results. We do not anticipate interns in the second professional year at our local institutions to be involved in vancomycin dosing and monitoring. While the results do not form robust support for this TBL activity, the results could have been impacted by differences in the exams given between years. While the cPKPD exams were not identical between years, the formats were consistent, though variation in difficultly could have existed. There was a decrease in the number of exam questions covering vancomycin which could have impacted results by offering students differing chances to answer correctly. However, identical exams would not have eliminated the potential for bias as identical exams would be subject to the potential for students to communicate exam content between class years. One of the five exams was not analyzed. However, the excluded exam (exam 1) consisted primarily of general pharmacokinetic and pharmacodynamic topics and the associated introductory clinical considerations. Therefore, we expect its exclusion is less likely to affect the overall results than exclusion of a different exam would. Additionally, the end of unit exam performance is also an indirect measure of the value of a given activity. The students appeared to value the activity (
Table 4) which provides information on student perceptions of learning/engagement which are important for student processing of new information. However, Likert scales are highly subjective, and these results are secondary to the changes in test scores. Finally, the data of the present study pre-date the COVID-19 pandemic, and changing teaching methods and student populations may diminish replicability.



















{kind=link}