


Inequity of Access: Scoping the Barriers to Assisted Reproductive Technologies



Abstract
:1. Introduction
2. Methods
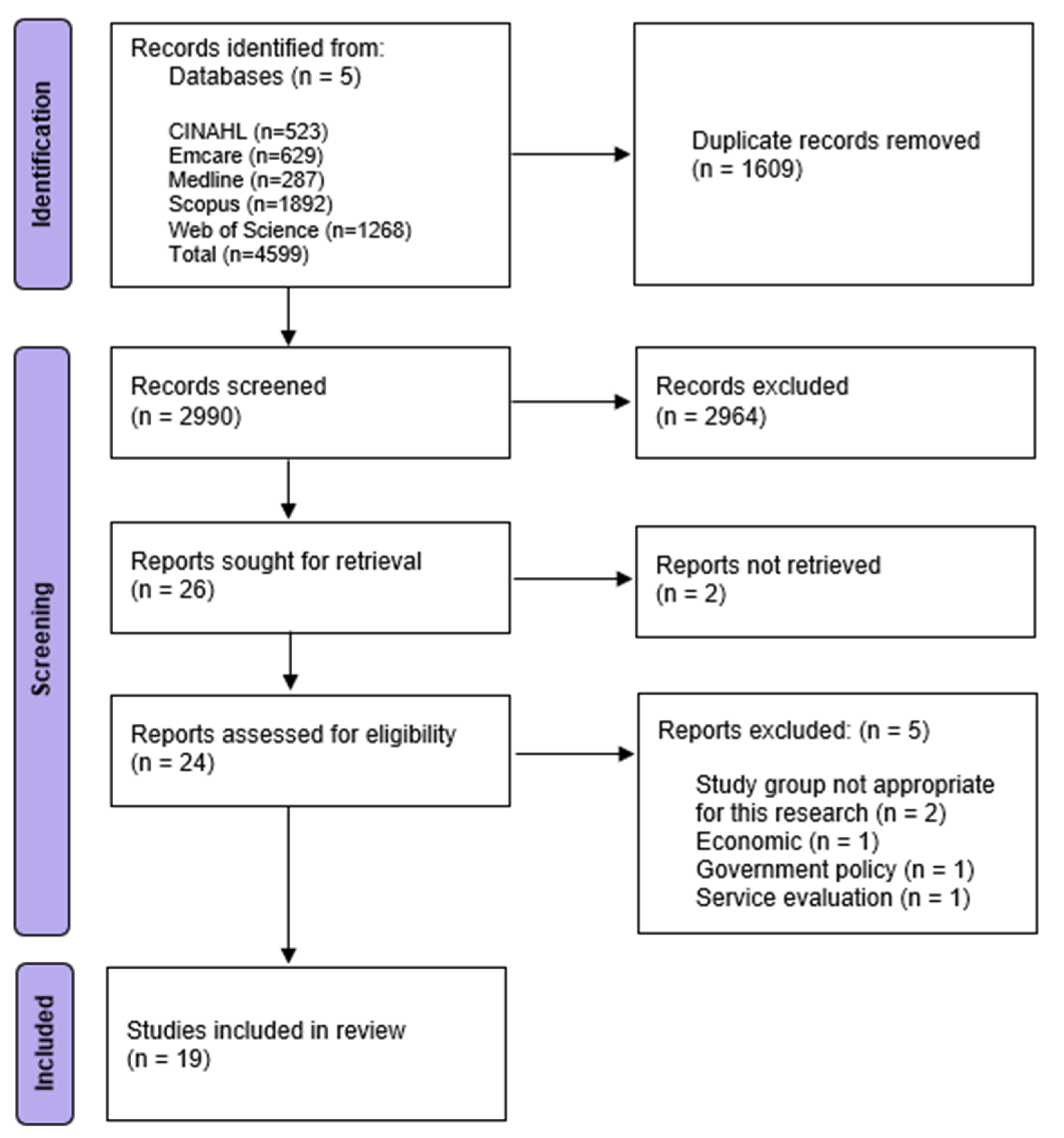
2.1. Literature Search
2.2. Selection of Relevant Studies
2.3. Review and Charting of Results

{kind=link}
| Author/Year/Country | Aim | Study Design | Key Outcome | Identified Barriers | Recommendations/ Implications |
|---|---|---|---|---|---|
| Barriers to Initiating ART | |||||
| Eisenberg ML, et al. [14] 2010 USA (Northern California) | To document the rate a cohort of infertility patients declined to pursue treatment and to determine reasons for this decision. | Mixed Methods Study Questionnaires followed by interviews of patients attending clinic for infertility 434 participants | Of 434 in cohort 13% did not pursue any infertility treatment. | Increased age Lower education Lower socioeconomic status Lower financial means Psychological (Depression) | Recommendation Introduce methods to detect and treat depression at initial infertility evaluation. |
| Hammoud AO, et al. [15] 2009 USA | To characterise the demographic correlation of IVF availability and utilisation. | Cross-sectional demographic analysis of public data Patients undergoing IVF | Lower availability of IVF physicians in USA vs. other developed countries. Lack of IVF insurance coverage correlated with low utilisation rates. | Geographic location (Country/State/ Less urbanisation) Lower education Lower financial means Health insurance coverage (lack of or limited) | |
| Herbert DL, et al. [10] 2010 Australia | To identify early users of fertility treatment (<34 years) and associations between various barriers. | Cross-sectional survey Infertile women from fertility clinics and community who had and had not used hormones/IVF as treatment 290 participants | Women (<34 years) living in major cities and having private health insurance is associated with early use of treatment for infertility at clinics. | Geographic location (outside major cities) Health insurance coverage (nil) | Implication Inequity of service for infertile women. |
| Yudin MH, et al. [16] 2010 Canada | To estimate the types of services available in fertility clinics in Canada for HIV positive individuals and couples. | Survey Registered fertility clinics in Canada clinics surveyed to assess availability of services for infertility OR viral transmission risk reduction in achieving pregnancy 28 clinics | Access to fertility investigation and treatment in Canada is limited and regionally dependent particularly for HIV positive patients. | Geographic location (distance from clinic) HIV positive status | Recommendation Develop strategies to increase access to appropriate service. |
| Blanchfield B, et al. [17] 2015 USA | To determine whether racial and/or sexual minority people receive help to become pregnant at the same rate as those not in these minority groups. | Demographic and socioeconomic analysis of public data (National Survey of Family Growth) Women aged 21–44 7463 participants | Heterosexual White women receive medical fertility assistance at nearly double the rates of non-White, sexual minority, or both. Differences in rates of help only partially mediated by insurance coverage and income. | Race/culture/ethnicity (non-white) Health insurance coverage (nil) Lower financial means (lower income) | Implication Sexual minority less likely to have insurance. |
| Chin HB, et al. [18] 2015 USA | To examine the persistence of a racial disparity in visiting a doctor for help getting pregnant. | Data analysis of cohort study Women aged 22–45 1073 participants | Black women were less likely to visit a doctor to get help to attain pregnancy After reporting infertility white women waited a year and black women 2 before accessing treatment. | Race / culture / ethnicity (Black women) Psychological (social stigmatisation around infertility and disappointing spouse) | Recommendation Development of online resources and encouragement of initiation of conversation with primary health care provider. |
| Harris K, et al. [19] 2016 Australia | To investigate disparities in access to assisted reproductive technology based on socio-economic status and geographic remoteness. | Data analysis of three datasets Women who accessed ART from 2009–2012 85,602 participants | Most disadvantaged/2nd most advantaged socio-economic status quintile had a 16%/6% reduction in access compared with the most advantaged quintile. Living in regional and remote areas had a 12% reduction in access. | Geographic location (remoteness) Lower socioeconomic status | Recommendation Change to public health policies to reduce inequity of access. |
| Chin HB, et al. [20] 2017 USA (Georgia) | To determine if there are any differences by place of residence in visiting a doctor for help getting pregnant. | Mixed methods study (Data analysis of cohort study and interviews) Women aged 22–45 1073 participants | Women visiting doctor for help getting pregnant ranged from 13% in small town/rural to 17% in suburban areas. Small town/rural and small metropolitan more likely to receive medications, less likely to receive testing alone or IVF. IVF 20% urbanised, 15.2% suburban, 12.5% small metropolitan, 0% small town/rural. | Geographic location (non-suburban location) Psychological (embarrassment / stigma) | Recommendation Increased communication from care providers to patients about reproductive goals and infertility care. |
| Dimitriadis I, et al. [21] 2017 USA. | To examine whether race affects: duration of infertility prior to seeking evaluation, diagnosis, treatment cycle characteristics, and outcomes. | Retrospective cohort data analysis Data examined from 5186 IUI cycles was retrospectively reviewed 1495 participants | Time to infertility-Asians and Hispanics compared to Caucasians waited significantly longer prior to seeking fertility evaluation. No effect of race on the average number of cycles required to achieve clinical pregnancy. | Race/culture/ethnicity (Asian and Hispanic) | |
| Janitz AE, et al. [22] 2019 USA | To assess racial differences in utilisation of infertility services (emphasis on American Indian, Alaskan natives). | Secondary analysis of cross-sectional data from survey (NSFG) Women aged 15–44 1824 participants | Disparities accessing and reduced service utilisation observed American Indian/Alaska Natives, Hispanic, and Black women compared to White. Asian/Pacific Islander similar prevalence of using services to Whites, except a lower prevalence seeking advice. | Race/culture/ethnicity (American Indian/Alaska Natives, Hispanic, and Black) | Recommendations Study to understand racial discrepancies in access and utilisation |
| Insogna IG, et al. [23] 2020 USA | To test the hypothesis that under-represented minority women, including Hispanic/Latina and African American or Black women, will be more likely to report greater socioeconomic and cultural barriers to infertility care compared with white women. | Cross-sectional survey Women aged 18–44 242 participants | No significant differences in education level, insurance type, socioeconomic barriers in access to care. Hispanic/Latina less likely to know if insurance covered infertility treatment. | Cost (out of pocket) Health insurance coverage (knowledge of insurance related to culture) | Recommendations Public health messaging and education around how to gain financial coverage. |
| Kyei JM, et al. [24] Ghana 2020 | To assess experiences of clients accessing ART services in Accra Ghana. | Qualitative study using Semi-structured interviews Men and women with infertility undergoing ART 12 women and 6 men | Five major challenges were identified at every phase of ART treatment: high cost, long distance to treatment centres, drug treatment challenges, disturbances in daily routine and work, anxiety around pregnancy outcome. | Geographic location (distance to treatment centres) Cost Psychological (Drug treatment challenges and anxiety around success of treatment) Multi-barrier (Change to routine) | Recommendations Counselling units to be added to centres, more insurance coverage. |
| Gilbert E, et al. [9] 2021 Australia (NT) | To explore health care provider (HCP) perspectives on the health burden of infertility among Aboriginal and Torres Strait Islander people, as well as factors that may affect access to infertility treatment for this group. | Qualitative study using semi-structured interviews Health care providers 12 participants– 8 doctors, 3 nurses, 1 aboriginal health practitioner | HCP perceive an underestimated health insurance in this patient population. Perceived barriers to accessing fertility care were reported. | Race/culture/ethnicity (Communication, language, fertility health literacy, shame and stigma, lack of culturally appropriate service) Geographic location (Distance from service) Psychological (shame and stigma) | Recommendations Increased patient education. Ongoing patient support Provision of culturally safe environment. |
| Koppen K, et al. [25] 2021 Germany | To examine the factors that assist and prevent individuals from seeking help for infertility and from using Medically Assisted Reproduction (MAR) in Germany. | Data analysis based on data from a longitudinal study Participants aged 25 or older who had tried to become pregnant or who were pregnant since previous interview 1446 participants | Utilisation of treatment was socially selective with married childless couples with a higher income rating the highest and younger couples with a less solid financial background, particularly those not married, appearing to face barriers to the use of medically assisted reproduction because of restrictive guidelines, corresponding legislation and limited insurance coverage. | Increased age Lower financial means Health insurance coverage (nil or limited) Marital status (not married) | |
| Barriers to continuing ART | |||||
| Bedrick BS, et al. [26] 2019 USA | To investigate factors involved with early IVF treatment discontinuation. | Secondary analysis of a retrospective cohort study Women undergoing IVF (first attempt) and did not achieve live birth 699 participants | Women without IVF insurance coverage had 3 times higher odds of treatment discontinuation. African American 3 times the odds of treatment discontinuation than White. Poor prognosis associated with greater likelihood discontinuing treatment. | Race / culture / ethnicity (African American) Health insurance coverage (nil) Confidence in fertility treatment (poor prognosis) | |
| Domar AD, et al. [27] 2010 USA | To determine the primary reason why insured patients, drop out of IVF treatment in the United States and to identify methods to decrease such behaviour. | Prospective patient survey Women age <40 with insurance for at least 3 cycles, did not conceive and did not return for third cycle 132 participants | Treatment termination was most commonly due to stress and psychological issues. | Geographic location (distance away from service) Psychological (stress, depression, relationship issues) Lower financial means Medication side effects | Recommendations Provide information on how to deal with psychological issues and immediate access to psychological services. |
| Domar AD, et al. [28] 2018 USA | To study the reason(s) why insured patients discontinue in vitro fertilisation (IVF) before achieving a live birth. | Cross-sectional survey study Women who have completed one IVF cycle but did not return within a year and no live birth 383 participants | Discontinuation was reported to be contributed to due to stress, financial burden or conceiving spontaneously. | Geographical location (distance from service) Lower financial means Health insurance coverage (lost) Psychological (stress) Medication side effects Confidence in fertility treatment (dissatisfaction / decreased confidence in provider) | Recommendations Investigate psychological interventions. |
| Maxwell E, et al. [8] 2018 Canada (Newfoundland) | To explore how barriers to accessing fertility services affect the treatment decisions made by fertility patients and service providers in Newfoundland and Labrador. | Qualitative study using semi-structured interviews ART patients and ART service providers 11 patients and eight service providers | Patients and providers make treatment choices to maximise likelihood of pregnancy success and increase accessibility (and costs) which can result in less effective care and sometimes potential risk to the patient. | Geographic location (isolation, number, and location of services available, partner separation) Cost Psychological (social stigma) | Recommendations Provide teleconsultations to make fertility care more accessible in rural and remote areas of the province. |
| Barriers to initiating and continuing ART | |||||
| Bennett LR, et al. [29] 2012 Indonesia | To improve understanding of infertility patients’ health seeking behaviour and patterns of access to infertility treatment in Indonesia, and to highlight possibilities for improving access. | Interviewer administered survey Female infertility treatment patients (from 3 Indonesian infertility clinics) 212 participants | Patients identified various barriers to accessing ART including: low confidence in fertility treatment; number and location of clinics; lack of well-established referral system; cost of treatment; fear of diagnosis of sterility; vaginal examination embarrassment. Women’s age of marriage and the timing of their initial presentation to gynaecologist were NOT found to be barriers to timely access to infertility care. | Geographic location (travel away from service) Cost Psychological (fear and embarrassment (shame)) Confidence in fertility centre (low) | Recommendations Increased patient education. Increased resources to reduce travel. Improve financial accessibility. Expansion of referral system. |
| Barrier | Initiating/Continuing | Number of Studies | Description of Barrier |
|---|---|---|---|
| Geographic location [8,9,10,15,16,19,20,24,28,29] | Initiating Continuing | 11 | Outside major cities Less urbanisation Geographic remoteness Embarrassment/shame with infertility related to geographic location Distance to service Travelling time and cost Inconvenience Away from emotional support Separation from partner Accessibility to IVF centre |
| Psychological [8,9,14,18,20,24,28,29] | Initiating Continuing | 9 | Depression Anxiety around success of treatment Social stigma Embarrassment/shame |
| Medication side effects [27,28] | Continuing | 2 | |
| Confidence in fertility treatment [26,28,29] | Continuing | 3 | Dissatisfaction with provider Confidence in provider |
| Race/culture/ethnicity [9,17,18,21,22,26] | Initiating | 6 | Non-white race Cultural relation to embarrassment/shame/stigma Communication and language Culturally appropriate service |
| Marital status [25] | Initiating | 1 | |
| HIV positive status [16] | Initiating | 1 | Safe conception |
| Socioeconomic status [14,19] | Initiating | 2 | |
| Health insurance coverage [10,14,15,17,25,27,28] | Initiating | 7 | Coverage by health insurance Classification of infertility as not a health condition but as a socially constructed need Knowledge of cover |
| Disposable income [14,15,17,25,27,28] | Initiating Continuing | 6 | Available funds Lower median income |
| Cost [8,23,24,29] | Initiating Continuing | 4 | |
| Lower education level [9,14,15] | Initiating | 3 | Formal education Health literacy |
| Increased age [14,25] | Initiating | 2 |
3. Results
3.1. Selected Studies
3.2. Barriers to ART
3.2.1. Geographical Location of Patient
3.2.2. Psychological Barriers
3.2.3. Minority Group Barriers
3.2.4. Financial Barriers
3.2.5. Education Level of Patient
3.2.6. Age Barriers
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Newman, J.E.P.R.; Chambers, G.M. Assisted Reproductive Technology in Australia and New Zealand 2019; National Perinatal Epidemiology and Statistics Unit, the University of New South Wales: Sydney, Australia, 2021. [Google Scholar]
- Mcguire, T.M. Fertility; Supporting the fertility treatment journey. AJP 2021, 102, 32–42. [Google Scholar] [CrossRef]
- Malina, A.; Pooley, J.A. Psychological consequences of IVF fertilization–Review of research. Ann. Agric. Environ. Med. 2017, 24, 554–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, L. Social and psychological consequences of infertility and assisted reproduction–what are the research priorities? Hum. Fertil. 2009, 12, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Beyene, R.T.; Kavalukas, S.L.; Barbul, A. Intra-abdominal adhesions: Anatomy, physiology, pathophysiology, and treatment. Curr. Probl. Surg. 2015, 52, 271–319. [Google Scholar] [CrossRef]
- Chambers, G.M.; Fauser, B. Access to ART treatment and gender equality. Reprod. Biomed. Online 2021, 42, 687–690. [Google Scholar] [CrossRef]
- Sol Olafsdottir, H.; Wikland, M.; Moller, A. Access to artificial reproduction technology in the Nordic countries in 2004. Acta Obs. Gynecol. Scand. 2009, 88, 301–307. [Google Scholar] [CrossRef]
- Maxwell, E.; Mathews, M.; Mulay, S. The Impact of Access Barriers on Fertility Treatment Decision Making: A Qualitative Study From the Perspectives of Patients and Service Providers. J. Obs. Gynaecol. Can. 2018, 40, 334–341. [Google Scholar] [CrossRef]
- Gilbert, E.; Walker, R.; Simon, D.; Derkenne, R.; Rumbold, A.; Campbell, S.; Boyle, J.A. "We are only looking at the tip of the iceberg in infertility": Perspectives of health providers about fertility issues and management among Aboriginal and Torres Strait Islander people. BMC Health Serv. Res. 2021, 21, 704. [Google Scholar] [CrossRef]
- Herbert, D.L.; Lucke, J.C.; Dobson, A.J. Early users of fertility treatment with hormones and IVF: Women who live in major cities and have private health insurance. Aust. N. Z. J. Public Health. 2010, 34, 629–634. [Google Scholar] [CrossRef]
- Di Trani, M.; Spoletini, R.; Renzi, A.; Greco, F.; Scaravelli, G. Psychologists’ representations about their professional functions within assisted reproductive multidisciplinary teams. Prof. Psychol. Res. Pract. 2021, 52, 299–307. [Google Scholar] [CrossRef]
- Holter, H.; Gejervall, A.L.; Borg, K.; Sandin-Bojö, A.K.; Wikland, M.; Wilde-Larsson, B.; Bergh, C. In vitro fertilization healthcare professionals generally underestimate patients’ satisfaction with quality of care. Acta Obs. Gynecol. Scand. 2017, 96, 302–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consolidated Framework for Implementation Research. Available online: https://cfirguide.org/ (accessed on 26 May 2022).
- Eisenberg, M.L.; Smith, J.F.; Millstein, S.G.; Nachtigall, R.D.; Adler, N.E.; Pasch, L.A.; Katz, P.P. Predictors of not pursuing infertility treatment after an infertility diagnosis: Examination of a prospective U.S. cohort. Fertil. Steril. 2010, 94, 2369–2371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammoud, A.O.; Gibson, M.; Stanford, J.; White, G.; Carrell, D.T.; Peterson, M. In vitro fertilization availability and utilization in the United States: A study of demographic, social, and economic factors. Fertil. Steril. 2009, 91, 1630–1635. [Google Scholar] [CrossRef]
- Yudin, M.H.; Shapiro, H.M.; Loutfy, M.R. Access to infertility services in Canada for HIV-positive individuals and couples: A cross-sectional study. Reprod. Health 2010, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanchfield, B.V.; Patterson, C.J. Racial and Sexual Minority Women’s Receipt of Medical Assistance to Become Pregnant. Health Psychol. 2015, 34, 571–579. [Google Scholar] [CrossRef]
- Chin, H.B.; Howards, P.P.; Kramer, M.R.; Mertens, A.C.; Spencer, J.B. Racial Disparities in Seeking Care for Help Getting Pregnant. Paediatr. Perinat. Epidemiol. 2015, 29, 416–425. [Google Scholar] [CrossRef] [Green Version]
- Harris, K.; Burley, H.; McLachlan, R.; Bowman, M.; Macaldowie, A.; Taylor, K.; Chapman, M.; Chambers, G.M. Socio-economic disparities in access to assisted reproductive technologies in Australia. Reprod. Biomed. Online 2016, 33, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Chin, H.B.; Kramer, M.R.; Mertens, A.C.; Spencer, J.B.; Howards, P.P. Differences in Women’s Use of Medical Help for Becoming Pregnant by the Level of Urbanization of County of Residence in Georgia. J. Rural Health 2017, 33, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Dimitriadis, I.; Batsis, M.; Petrozza, J.C.; Souter, I. Racial disparities in fertility care: An analysis of 4537 intrauterine insemination cycles. J. Racial Ethn. Health Disparities 2017, 4, 169–177. [Google Scholar] [CrossRef]
- Janitz, A.E.; Peck, J.D.; Craig, L.B. Racial/Ethnic Differences in the Utilization of Infertility Services: A Focus on American Indian/Alaska Natives. Matern. Child Health J. 2019, 23, 10–18. [Google Scholar] [CrossRef]
- Insogna, I.G.; Lanes, A.; Hariton, E.; Blake-Lamb, T.; Schilling, S.; Hornstein, M.D. Self-reported barriers to accessing infertility care: Patient perspectives from urban gynecology clinics. J. Assist. Reprod. Genet. 2020, 37, 3007–3014. [Google Scholar] [CrossRef] [PubMed]
- Kyei, J.M.; Manu, A.; Kotoh, A.M.; Meherali, S.; Ankomah, A. Challenges experienced by clients undergoing assisted reproductive technology in Ghana: An exploratory descriptive study. Int. J. Gynaecol. Obs. 2020, 149, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Köppen, K.; Trappe, H.; Schmitt, C. Who can take advantage of medically assisted reproduction in Germany? Reprod. Biomed. Soc. Online 2021, 13, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Bedrick, B.S.; Anderson, K.; Broughton, D.E.; Hamilton, B.; Jungheim, E.S. Factors associated with early in vitro fertilization treatment discontinuation. Fertil. Steril. 2019, 112, 105–111. [Google Scholar] [CrossRef]
- Domar, A.D.; Smith, K.; Conboy, L.; Iannone, M.; Alper, M. A prospective investigation into the reasons why insured United States patients drop out of in vitro fertilization treatment. Fertil. Steril. 2010, 94, 1457–1459. [Google Scholar] [CrossRef]
- Domar, A.D.; Rooney, K.; Hacker, M.R.; Sakkas, D.; Dodge, L.E. Burden of care is the primary reason why insured women terminate in vitro fertilization treatment. Fertil. Steril. 2018, 109, 1121–1126. [Google Scholar] [CrossRef]
- Bennett, L.R.; Wiweko, B.; Hinting, A.; Adnyana, I.B.; Pangestu, M. Indonesian infertility patients’ health seeking behaviour and patterns of access to biomedical infertility care: An interviewer administered survey conducted in three clinics. Reprod. Health 2012, 9, 24. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 2021, 372, n71. [Google Scholar] [CrossRef]
- Fleming, M.L.; Parker, E. Introduction to Public Health, 2nd ed.; Elsevier Health Sciences APAC: London, UK, 2012. [Google Scholar]
- Laird, P.; Chang, A.B.; Jacky, J.; Lane, M.; Schultz, A.; Walker, R. Conducting decolonizing research and practice with Australian First Nations to close the health gap. Health Res. Policy Syst. 2021, 19, 1–127. [Google Scholar] [CrossRef]
- Palinkas, L.A.; Spear, S.E.; Mendon, S.J.; Villamar, J.; Valente, T.; Chou, C.-P.; Landsverk, J.; Kellam, S.G.; Brown, C.H. Measuring sustainment of prevention programs and initiatives: A study protocol. Implement. Sci. IS 2016, 11, 95. [Google Scholar] [CrossRef]
- Sills, E.S.; Shurpyak, S.A.; Gorman, D.J.; Shkrobot, L.V.; Murray, G.U.; O’Connor, B.M.; Rapple, U.E.; Fogarty, A.O.; Svarkova, P.; Brickell, K.M. Fertility patients and their prescriptions: A two-year audit of patient-pharmacist interactions in a reproductive endocrinology practice. Int. Arch. Med. 2009, 2, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, M.N.; Wiemer, D. Therapeutic Management of Infertility A Pharmacist’s Perspective. US Pharm. 2015, 40, 52–58. [Google Scholar]
- Heredia, M.; Tenias, J.M.; Ruiz, R.; Sanchez, M.; Calleja, M.A.; Martinez, F. Pharmaceutical care for patients undergoing assisted reproduction techniques. Eur. J. Hosp. Pharm. 2012, 19, 289–292. [Google Scholar] [CrossRef]
- Chaudhary, S.; Ray, R.; Glass, B.D. “Treat us as a person”: A narrative inquiry of experiences and expectations of interactions with pharmacists and pharmacy staff among people who are transgender. Explor. Res. Clin. Soc. Pharm. 2022, 8, 100198. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, N.Z.; Brennan, L.; Abrons, J.P.; Chahine, E.B. An Introduction to Cultural Sensitivity and Global Pharmacy Engagement. Am. J. Pharm. Educ. 2019, 83, 7221. [Google Scholar] [CrossRef]
- Kaya, Y.; Kizilkaya Beji, N.; Aydin, Y.; Hassa, H. The effect of health-promoting lifestyle education on the treatment of unexplained female infertility. Eur. J. Obs. Gynecol. Reprod. Biol. 2016, 207, 109–114. [Google Scholar] [CrossRef]
- Anderson, C. Health promotion in community pharmacy: The UK situation. Patient Educ. Couns. 2000, 39, 285–291. [Google Scholar] [CrossRef]
- Benrimoj, S.I.; Frommer, M.S. Community pharmacy in Australia. Aust. Health Rev. 2004, 28, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.; Cairns, A.; Glass, B. Role Theory: A Framework to Explore Health Professional Perceptions of Expanding Rural Community Pharmacists’ Role. Pharmacy 2020, 8, 161. [Google Scholar] [CrossRef]
- Miller, P.; Newby, D.; Walkom, E.; Schneider, J.; Li, S.C. Depression screening in adults by pharmacists in the community: A systematic review. Int. J. Pharm. Pract. 2020, 28, 428–440. [Google Scholar] [CrossRef]
- El-Den, S.; Collins, J.C.; Chen, T.F.; O’Reilly, C.L. Pharmacists’ roles in mental healthcare: Past, present and future. Pharm. Pract. 2021, 19, 2545. [Google Scholar] [CrossRef] [PubMed]
- Allinson, R. Specialty pharmaceuticals: Infertility: A specialty pharmacy success story. Pharm. Times, 2010. Available online: https://www.pharmacytimes.com/view/specialtypharmacyinfertility-0610(accessed on 1 December 2022).
- Ito, T.; Shimizu, K.; Ichida, Y.; Ishibashi, Y.; Akizuki, N.; Ogawa, A.; Fujimori, M.; Kaneko, N.; Ueda, I.; Nakayama, K.; et al. Usefulness of pharmacist-assisted screening and psychiatric referral program for outpatients with cancer undergoing chemotherapy. Psycho-Oncology 2011, 20, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Penn, C.; Watermeyer, J.; Evans, M. Why don’t patients take their drugs? The role of communication, context and culture in patient adherence and the work of the pharmacist in HIV/AIDS. Patient Educ. Couns. 2011, 83, 310–318. [Google Scholar] [CrossRef]
- Skellett, L. Cultural awareness and cultural safety. Aust. Pharm. 2012, 31, 382–384. [Google Scholar]
- Singh, L.G.; Accursi, M.; Black, K.K. Implementation and outcomes of a pharmacist-managed clinical video telehealth anticoagulation clinic. Am. J. Health-Syst. Pharm. 2015, 72, 70–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nye, A.M. A Clinical Pharmacist in Telehealth Team Care for Rural Patients with Diabetes. North Carol. Med. J. 2017, 78, 183–184. [Google Scholar] [CrossRef] [Green Version]
- Omboni, S.; Tenti, M.; Coronetti, C. Physician–pharmacist collaborative practice and telehealth may transform hypertension management. J. Hum. Hypertens. 2019, 33, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Segal, E.M.; Alwan, L.; Pitney, C.; Taketa, C.; Indorf, A.; Held, L.; Lee, K.S.; Son, M.; Chi, M.; Diamantides, E.; et al. Establishing clinical pharmacist telehealth services during the COVID-19 pandemic. Am. J. Health-Syst. Pharm. 2020, 77, 1403–1408. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mackay, A.; Taylor, S.; Glass, B. Inequity of Access: Scoping the Barriers to Assisted Reproductive Technologies. Pharmacy 2023, 11, 17. https://doi.org/10.3390/pharmacy11010017
Mackay A, Taylor S, Glass B. Inequity of Access: Scoping the Barriers to Assisted Reproductive Technologies. Pharmacy. 2023; 11(1):17. https://doi.org/10.3390/pharmacy11010017
Chicago/Turabian StyleMackay, Amanda, Selina Taylor, and Beverley Glass. 2023. "Inequity of Access: Scoping the Barriers to Assisted Reproductive Technologies" Pharmacy 11, no. 1: 17. https://doi.org/10.3390/pharmacy11010017
APA StyleMackay, A., Taylor, S., & Glass, B. (2023). Inequity of Access: Scoping the Barriers to Assisted Reproductive Technologies. Pharmacy, 11(1), 17. https://doi.org/10.3390/pharmacy11010017