
The Effect of Genotyping on the Number of Pharmacotherapeutic Gene–Drug Interventions in Chronic Kidney Disease Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
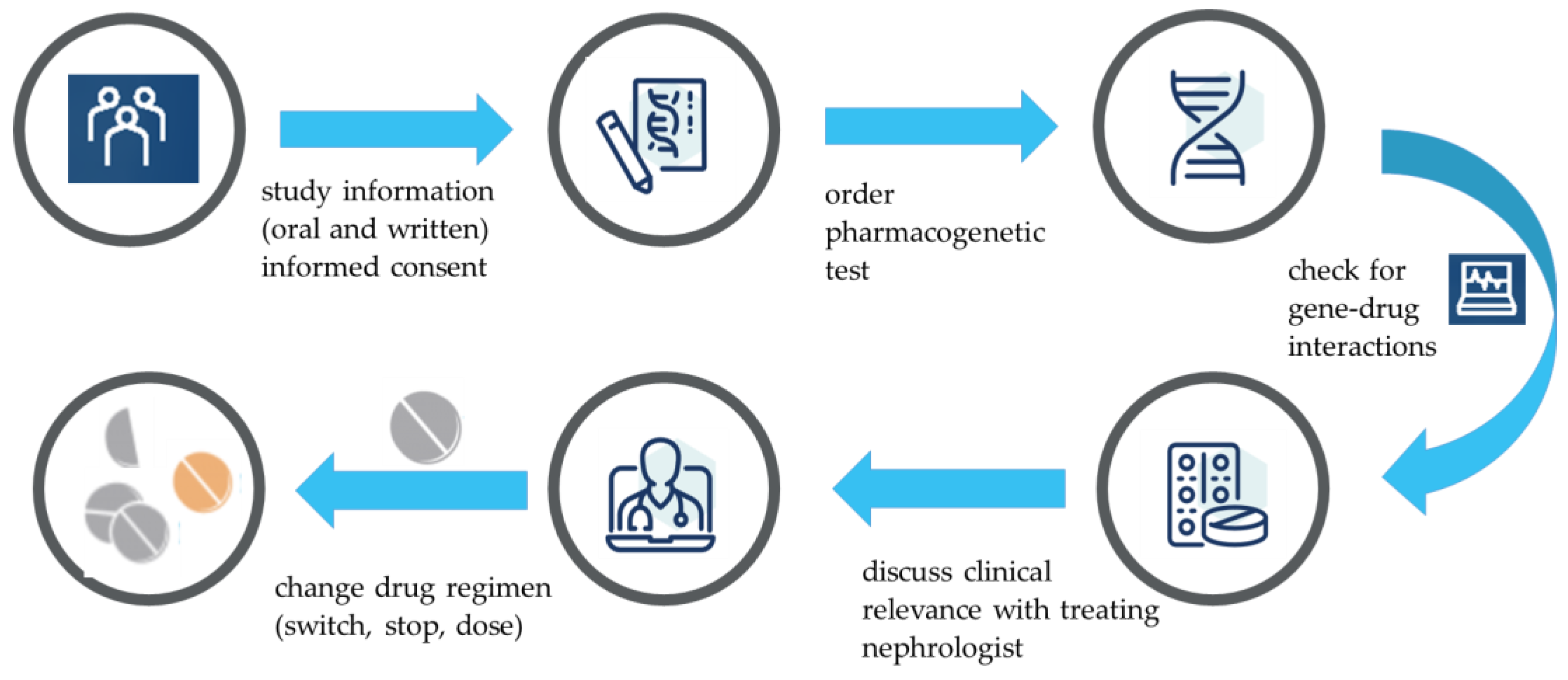
2.2. Study Procedure
2.3. Genotype Analysis
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Pharmacogenetic Testing
3.3. Gene–Drug Interactions and Pharmacotherapeutic Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burnier, M.; Pruijm, M.; Wuerzner, G.; Santschi, V. Drug Adherence in Chronic Kidney Diseases and Dialysis. Nephrol. Dial. Transplant. 2015, 30, 39–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joosten, H.; Drion, I.; Boogerd, K.J.; van der Pijl, E.V.; Slingerland, R.J.; Slaets, J.P.; Jansen, T.J.; Schwantje, O.; Gans, R.O.; Bilo, H.J. Optimising Drug Prescribing and Dispensing in Subjects at Risk for Drug Errors Due to Renal Impairment: Improving Drug Safety in Primary Healthcare by Low EGFR Alerts. BMJ Open 2013, 3, e002068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorks, M.; Herget-Rosenthal, S.; Schmiemann, G.; Hoffmann, F. Polypharmacy and Renal Failure in Nursing Home Residents: Results of the Inappropriate Medication in Patients with Renal Insufficiency in Nursing Homes (IMREN) Study. Drugs Aging 2016, 33, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Velenosi, T.J.; Urquhart, B.L. Pharmacokinetic Considerations in Chronic Kidney Disease and Patients Requiring Dialysis. Expert. Opin. Drug Metab Toxicol. 2014, 10, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- de Lara, D.V.; de Melo, D.O.; Kawakami, D.Y.; Goncalves, T.S.; Santos, P.C. Pharmacogenetic Testing-Guided Treatment for Oncology: An Overview of Reviews. Pharmacogenomics 2022, 23, 739–748. [Google Scholar] [CrossRef]
- Lara, D.V.; Melo, D.O.; Silva, R.A.M.; Santos, P.C.J.L. Pharmacogenetic Testing in Psychiatry and Neurology: An Overview of Reviews. Pharmacogenomics 2021, 22, 505–513. [Google Scholar] [CrossRef]
- Awdishu, L.; Joy, M.S. Role of Pharmacogenomics in Kidney Disease and Injury. Adv. Chronic. Kidney Dis. 2016, 23, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.T.; Andrews, L.M.; van Gelder, T.; Shi, Y.Y.; van Schaik, R.H.N.; Wang, L.L.; Hesselink, D.A. Pharmacogenetic Aspects of the Use of Tacrolimus in Renal Transplantation: Recent Developments and Ethnic Considerations. Expert. Opin. Drug Metab. Toxicol. 2016, 12, 555–565. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Lin, G.; Tan, L.; Li, J. Current Progress of Tacrolimus Dosing in Solid Organ Transplant Recipients: Pharmacogenetic Considerations. Biomed. Pharmacother. 2018, 102, 107–114. [Google Scholar] [CrossRef]
- Eadon, M.T.; Maddatu, J.; Moe, S.M.; Sinha, A.D.; Melo Ferreira, R.; Miller, B.W.; Sher, S.J.; Su, J.; Pratt, V.M.; Chapman, A.B.; et al. Pharmacogenomics of Hypertension in CKD: The CKD-PGX Study. Kidney360 2022, 3, 307–316. [Google Scholar] [CrossRef]
- KNMP: Dutch Pharmacogenetics Working Group. Available online: https://www.knmp.nl/dossiers/farmacogenetica (accessed on 27 December 2022).
- Ragia, G.; Petridis, I.; Tavridou, A.; Christakidis, D.; Manolopoulos, V.G. Presence of CYP2C9*3 allele increases risk for hypoglycemia in Type 2 diabetic patients treated with sulfonylureas. Pharmacogenomics 2009, 10, 1781–1787. [Google Scholar] [CrossRef] [PubMed]
- Matic, M.; Nijenhuis, M.; Soree, B.; de Boer-Veger, N.J.; Buunk, A.M.; Houwink, E.J.F.; Mulder, H.; Rongen, G.A.P.J.M.; Weide, J.V.; Wilffert, B.; et al. Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2D6 and opioids (codeine, tramadol and oxycodone). Eur. J. Hum. Genet. 2022, 10, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Collett, S.; Massmann, A.; Petry, N.J.; Van Heukelom, J.; Schultz, A.; Hellwig, T.; Baye, J.F. Metoprolol and CYP2D6: A Retrospective Cohort Study Evaluating Genotype-Based Outcomes. J. Pers. Med. 2023, 13, 416. [Google Scholar] [CrossRef] [PubMed]
- Verbelen, M.; Weale, M.E.; Lewis, C.M. Cost-Effectiveness of Pharmacogenetic-Guided Treatment: Are We There Yet? Pharmacogenom. J. 2017, 17, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Dowd, D.; Williams, G.; VanDorn, D.; Clarke, S.; Krause, D.S.; Botbyl, J.; Saklad, S.R. Predicting Drug-Drug and Drug-Gene Interactions in a Community Pharmacy Population. Am. J. Manag. Care 2022, 28, 566–571. [Google Scholar]
- Malki, M.A.; Pearson, E.R. Drug-Drug-Gene Interactions and Adverse Drug Reactions. Pharmacogenom. J. 2020, 20, 355–366. [Google Scholar] [CrossRef] [Green Version]
- Tannenbaum, C.; Sheehan, N.L. Understanding and Preventing Drug-Drug and Drug-Gene Interactions. Expert. Rev. Clin. Pharmacol. 2014, 7, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Ladda, M.A.; Goralski, K.B. The Effects of CKD on Cytochrome P450-Mediated Drug Metabolism. Adv. Chronic. Kidney Dis. 2016, 23, 67–75. [Google Scholar] [CrossRef]
- Liu, B.; Luo, F.; Luo, X.; Duan, S.; Gong, Z.; Peng, J. Metabolic Enzyme System and Transport Pathways in Chronic Kidney Diseases. Curr. Drug Metab. 2018, 19, 568–576. [Google Scholar] [CrossRef]
- Naud, J.; Dumayne, C.; Nolin, T.D.; Leblond, F.A.; Pichette, V. Drug Pharmacokinetics in Renal Failure: What’s New? Nephrol. Ther. 2015, 11, 144–151. [Google Scholar] [CrossRef]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.J.; Swen, J.J. Phenoconversion of Cytochrome P450 Metabolism: A Systematic Review. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef] [PubMed]
- Swen, J.J.; Nijenhuis, M.; van Rhenen, M.; de Boer-Veger, N.J.; Buunk, A.M.; Houwink, E.J.F.; Mulder, H.; Rongen, G.A.; van Schaik, R.H.N.; van der Weide, J.; et al. Pharmacogenetic Information in Clinical Guidelines: The European Perspective. Clin. Pharmacol. Ther. 2018, 103, 795–801. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n (%) |
|---|---|
| Gender | |
| male | 38 (62%) |
| female | 23 (38%) |
| Age, mean (range) | 73 (47–86) |
| Race (caucasian) | 61 (100%) |
| Smoking | |
| yes | 5 (8%) |
| no | 56 (92%) |
| eGFR (CKD-EPI mL/min), median (range) | 18 (9–30) |
| Number of drugs, median (range) | 12 (5–20) |
| Comorbidities | |
| hypertension | 41 (67%) |
| heartfailure | 41 (67%) |
| atrial fibrillation | 10 (16%) |
| diabetes | 22 (36%) |
| Drug | n | (%) |
|---|---|---|
| Colecalciferol | 57 | (93%) |
| Pantoprazole | 34 | (56%) |
| Metoprolol | 32 | (52%) |
| Acetylsalicylic acid | 26 | (43%) |
| Allopurinol | 23 | (38%) |
| Alfacalcidol | 20 | (33%) |
| Darbepoetin alfa | 20 | (33%) |
| Furosemide | 19 | (31%) |
| Simvastatin | 19 | (31%) |
| Amlodipine | 15 | (25%) |
| Folic acid | 14 | (23%) |
| Macrogol | 14 | (23%) |
| Acenocoumarol | 12 | (20%) |
| Acetaminophen | 12 | (20%) |
| Rosuvastatin | 12 | (20%) |
| Sodiumbicarbonate | 11 | (18%) |
| Atorvastatin | 10 | (16%) |
| Ferrofumarate | 10 | (16%) |
| Hydrochlorothiazide | 9 | (15%) |
| Lercanidipin | 9 | (15%) |
| Lisinopril | 9 | (15%) |
| Spironolacton | 9 | (15%) |
| Prednisolone | 8 | (13%) |
| Bisoprolol | 7 | (11%) |
| Bumetanide | 7 | (11%) |
| Clopidogrel | 7 | (11%) |
| Doxazosine | 7 | (11%) |
| Ezetimibe | 7 | (11%) |
| Linagliptin | 7 | (11%) |
| Perindopril | 7 | (11%) |
| n = 61 | PM | IM | NM | RM | UM | II |
|---|---|---|---|---|---|---|
| CYP1A2 | 0 | 2 | 25 | n.a. | 0 | 34 *1 |
| CYP2B6 | 3 | 24 | 34 | n.a. | 0 | n.a. |
| CYP2C19 | 3 | 19 | 25 | 12 | 2 | n.a. |
| CYP2C9 | 1 | 13 | 47 | n.a. | 0 | n.a. |
| CYP2D6 | 9 | 23 | 29 | n.a. | 0 | n.a. |
| CYP3A4 | 0 | 6 | 55 | n.a. | 0 | n.a. |
| CYP3A5 | 55 | 4 | 2 | n.a. | n.a. | n.a. |
| VKORC1 | 9 | 28 | 24 | n.a. | n.a. | n.a. |
| Subject | Intervention | CYP | Phenotype | Drug with Gene–Drug Interaction | Clinical Implication * |
|---|---|---|---|---|---|
| 6 | switch | CYP2C19 | IM | clopidogrel | less effect |
| 12 | switch | CYP2C9 | IM | gliclazide | side effect |
| dosage | VKORC1/CYP2C9 | PM/IM | acenocoumarol | side effect | |
| 17 | switch | VKORC1 | IM | fenprocoumon | side effect |
| 18 | dosage | CYP2D6 | IM | metoprolol | side effect |
| discontinuation | CYP2C19 | IM | pantoprazole | side effect | |
| 20 | switch | CYP2C19 | UM | pantoprazole | less effect |
| discontinuation | CYP2C19 | UM | amitriptylin | less effect | |
| 22 | switch | CYP3A4 | IM | simvastatin | side effect |
| 23 | discontinuation | CYP2C19 | IM | clopidogrel | less effect |
| discontinuation | CYP3A5 | IM | amiodarone | less effect | |
| 24 | dosage | CYP2D6 | IM | bisoprolol | side effect |
| 25 | switch | CYP3A4 | IM | simvastatin | side effect |
| dosage | CYP2D6 | IM | metoprolol | side effect | |
| 27 | dosage | CYP2D6 | IM | risperidone | side effect |
| 33 | dosage | CYP2D6 | IM | metoprolol | side effect |
| switch | CYP2C9 | PM | glimepiride | side effect | |
| 36 | dosage | CYP2D6 | IM | bisoprolol | side effect |
| 37 | discontinuation | CYP2D6 | PM | tramadol | less effect |
| 47 | dosage | CYP2C19 | IM | pantoprazole | side effect |
| 49 | dosage | CYP2D6 | IM | metoprolol | side effect |
| 51 | dosage | CYP2D6 | IM | metoprolol | side effect |
| 55 | switch | CYP3A4 | IM | simvastatin | side effect |
| 59 | discontinuation | CYP2D6 | PM | tramadol | less effect |
| 60 | switch | CYP2C19 | UM | pantoprazole | less effect |
| 61 | dosage | CYP2D6 | IM | metoprolol | side effect |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerskes, C.H.M.; van den Eijnde, C.J.M.E.; Aarnoudse, A.-J.L.H.J.; Grouls, R.J.E.; Deiman, B.A.L.M.; Deenen, M.J. The Effect of Genotyping on the Number of Pharmacotherapeutic Gene–Drug Interventions in Chronic Kidney Disease Patients. Pharmacy 2023, 11, 69. https://doi.org/10.3390/pharmacy11020069
Kerskes CHM, van den Eijnde CJME, Aarnoudse A-JLHJ, Grouls RJE, Deiman BALM, Deenen MJ. The Effect of Genotyping on the Number of Pharmacotherapeutic Gene–Drug Interventions in Chronic Kidney Disease Patients. Pharmacy. 2023; 11(2):69. https://doi.org/10.3390/pharmacy11020069
Chicago/Turabian StyleKerskes, Catharina H. M., Carien J. M. E. van den Eijnde, Albert-Jan L. H. J. Aarnoudse, René J. E. Grouls, Birgit A. L. M. Deiman, and Maarten J. Deenen. 2023. "The Effect of Genotyping on the Number of Pharmacotherapeutic Gene–Drug Interventions in Chronic Kidney Disease Patients" Pharmacy 11, no. 2: 69. https://doi.org/10.3390/pharmacy11020069
APA StyleKerskes, C. H. M., van den Eijnde, C. J. M. E., Aarnoudse, A. -J. L. H. J., Grouls, R. J. E., Deiman, B. A. L. M., & Deenen, M. J. (2023). The Effect of Genotyping on the Number of Pharmacotherapeutic Gene–Drug Interventions in Chronic Kidney Disease Patients. Pharmacy, 11(2), 69. https://doi.org/10.3390/pharmacy11020069