
Understanding the Risk Factors and Stressors Impacting Optimal Work Practices in New Zealand Pharmacies: A S.H.E.L.L Model Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Design
2.2. Ethics Approval
3. Results
3.1. Participant Demographics
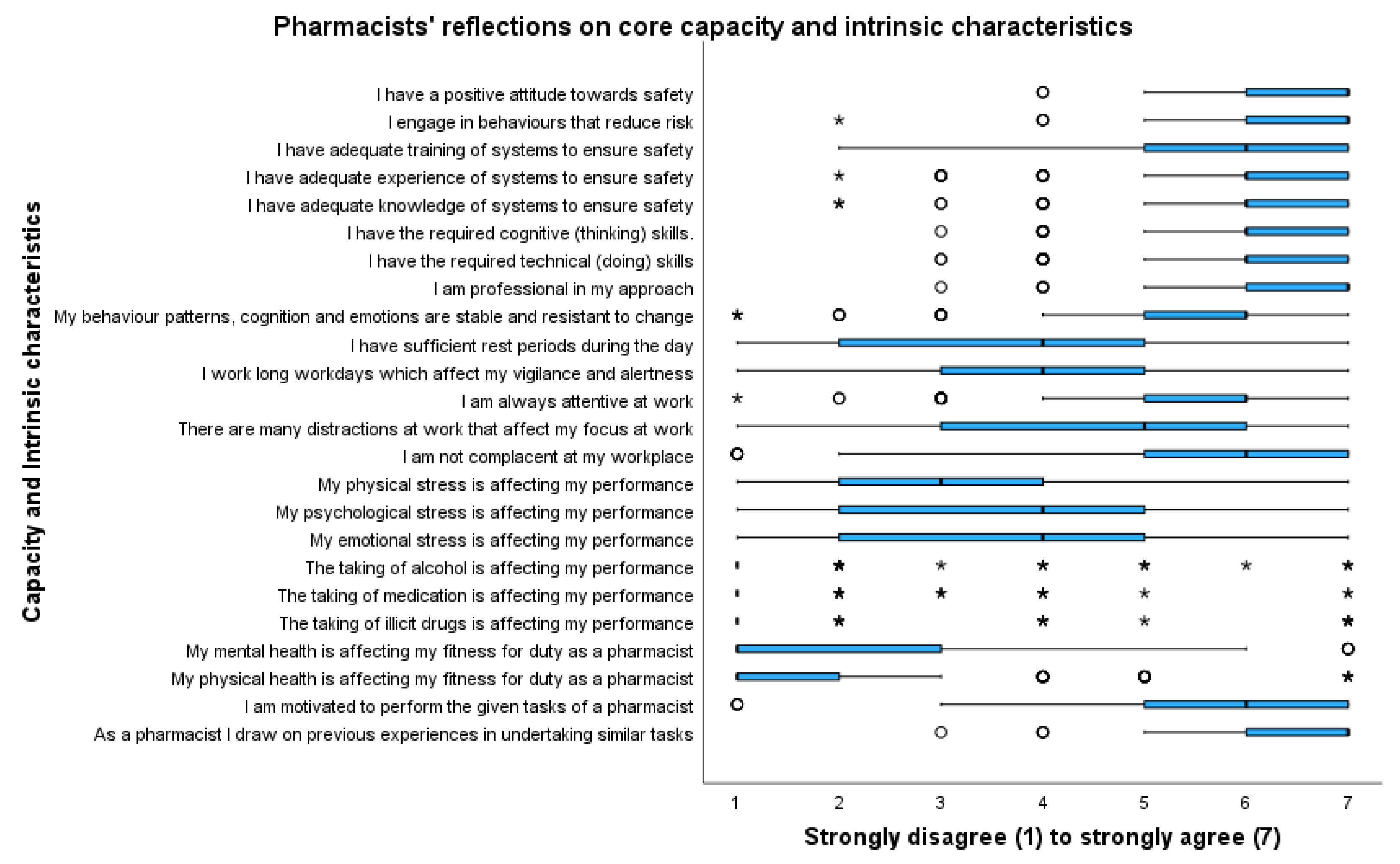
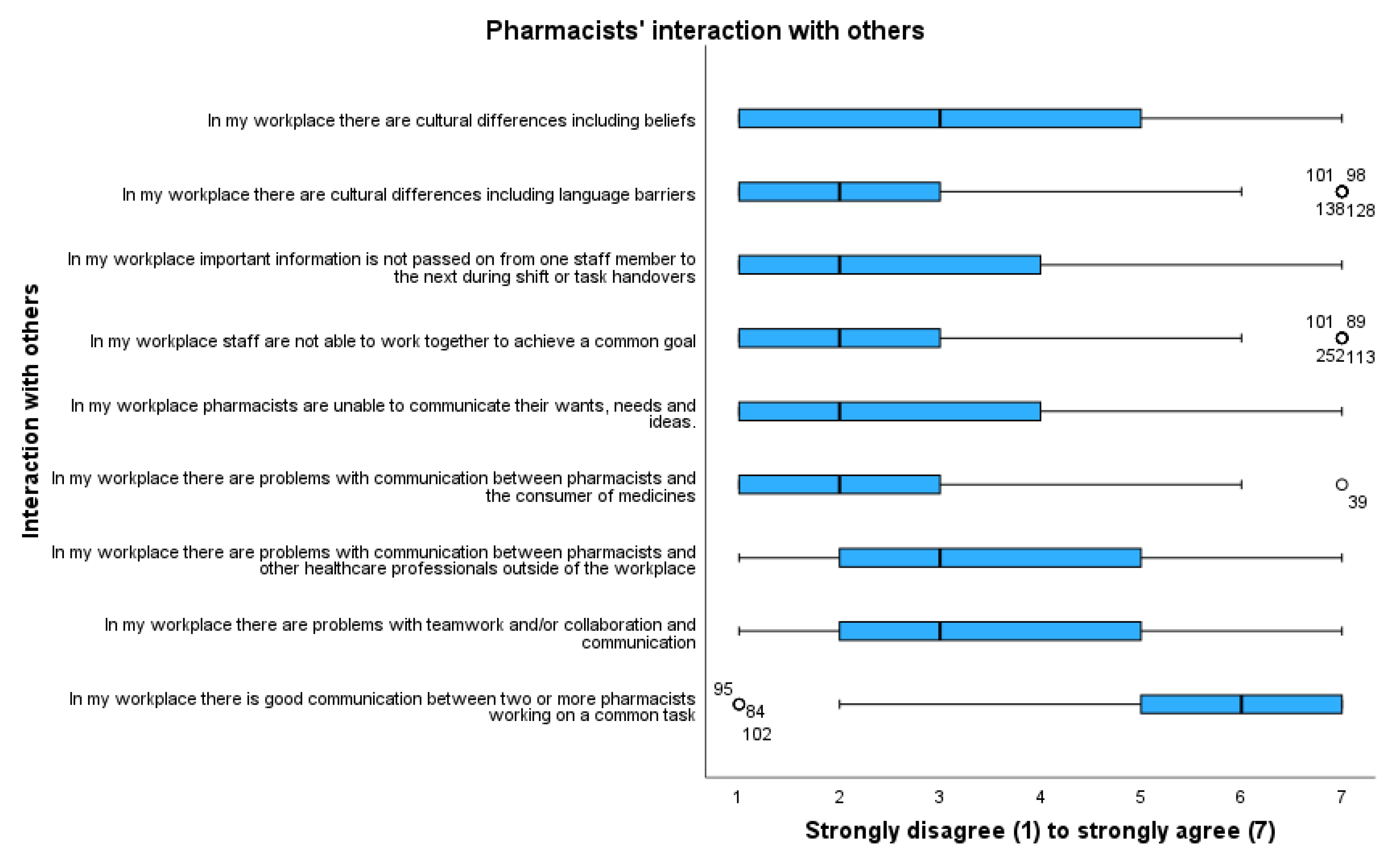
3.2. Quantitative Analysis
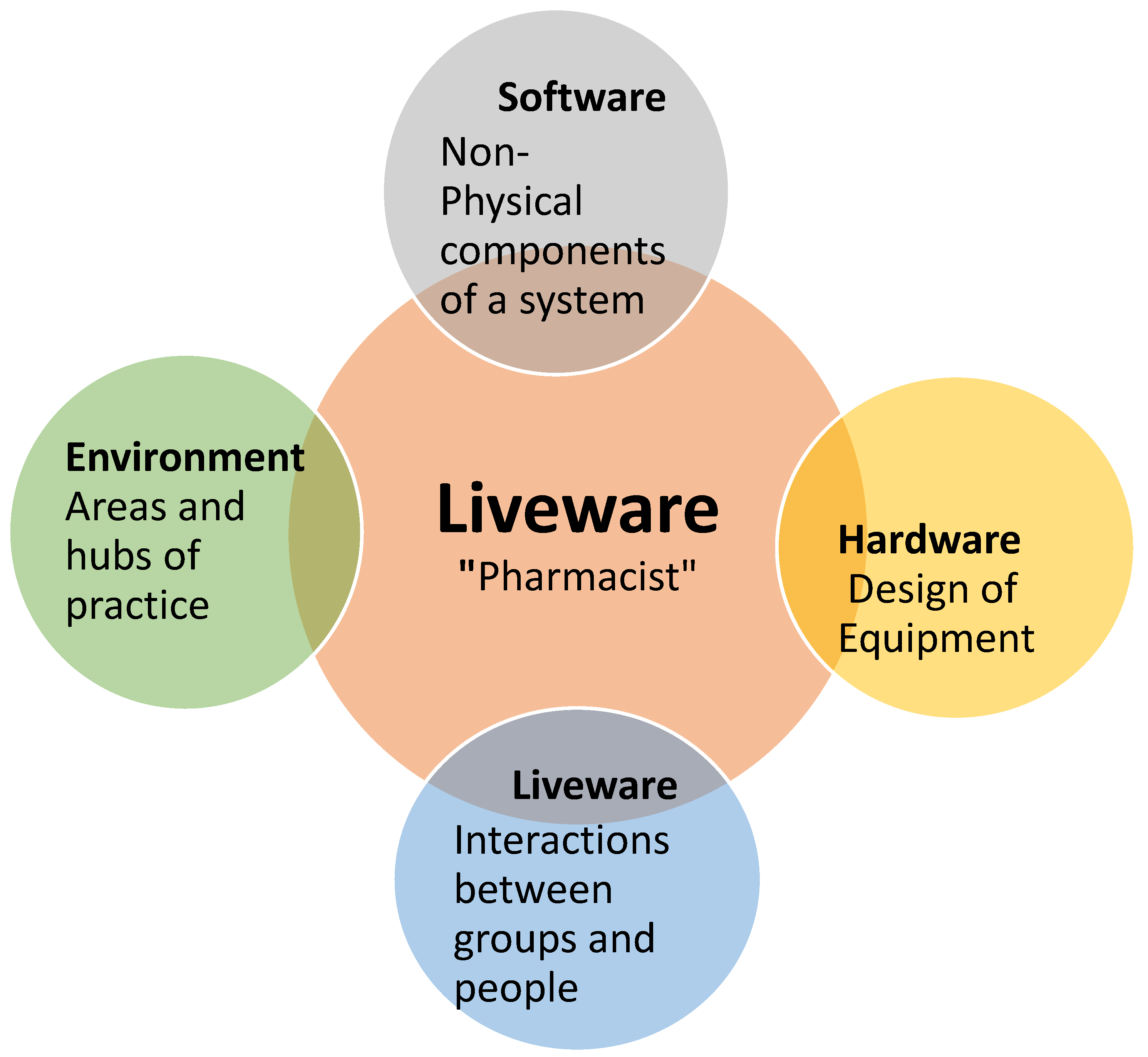
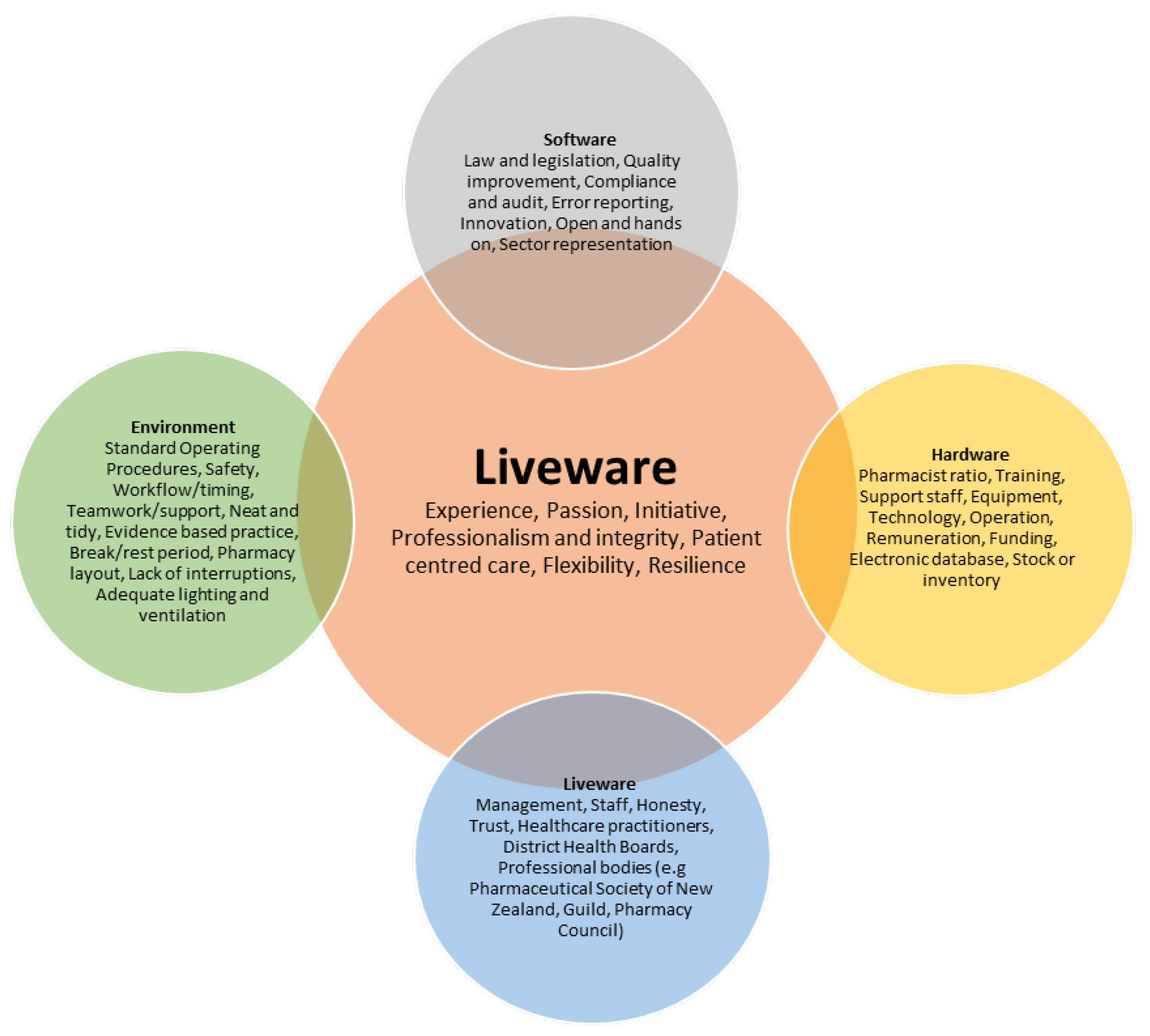
3.3. Summary of Factors That Affect Optimal Pharmacy Practice S.H.E.L.L Model
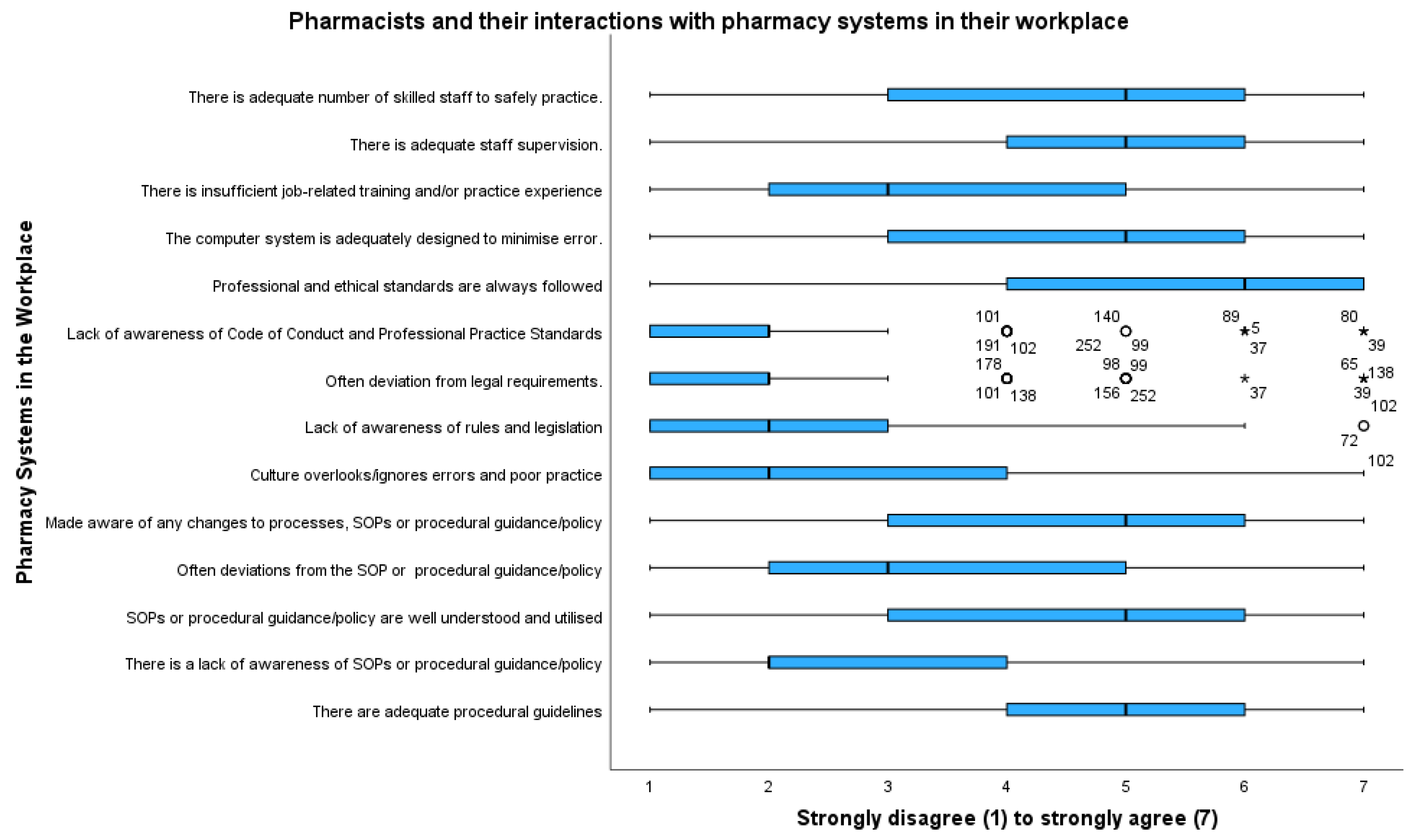
3.3.1. Liveware–Software: Pharmacist and Systems
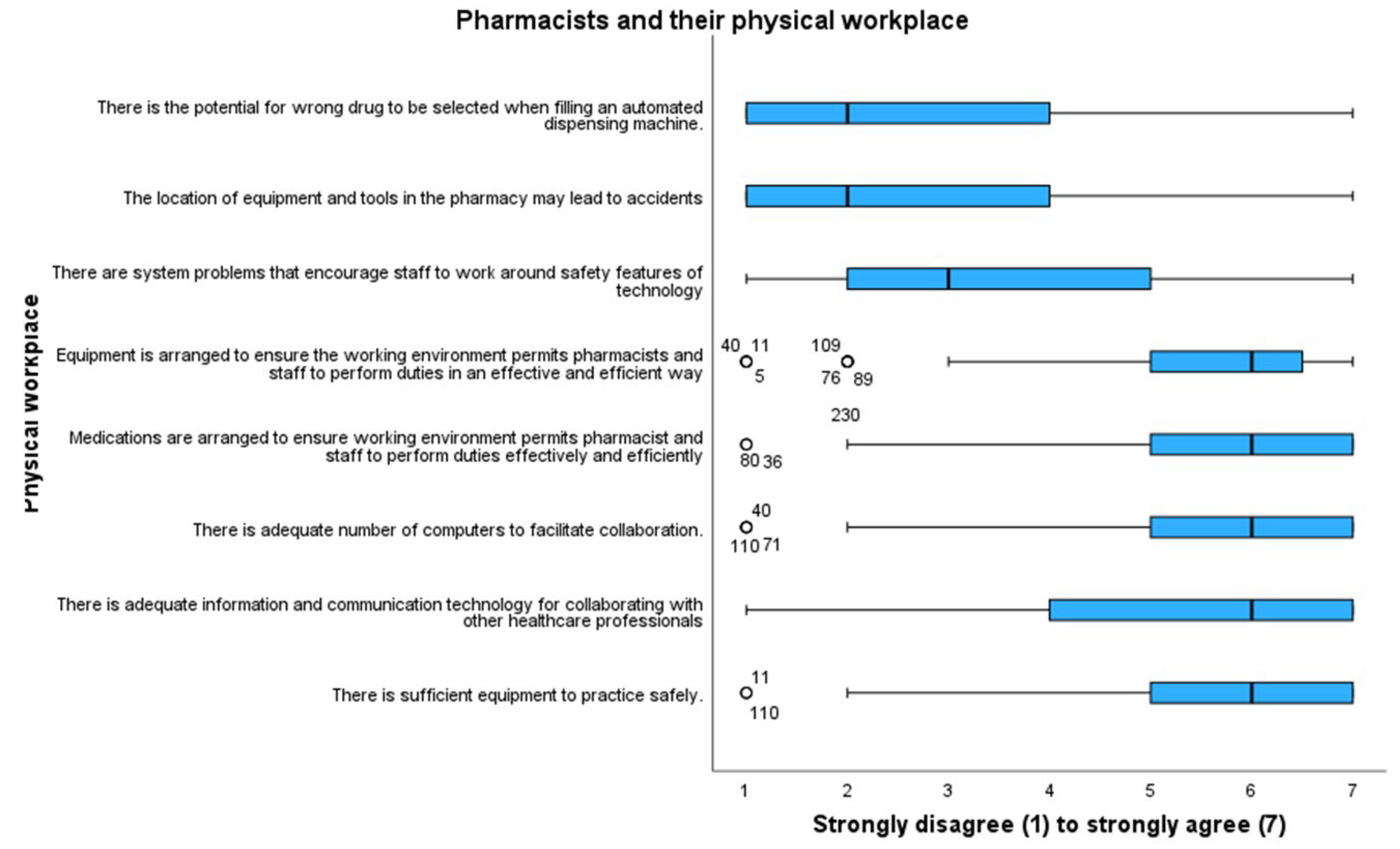
3.3.2. Liveware–Hardware (L–H): The Pharmacist and Their Physical Workplace
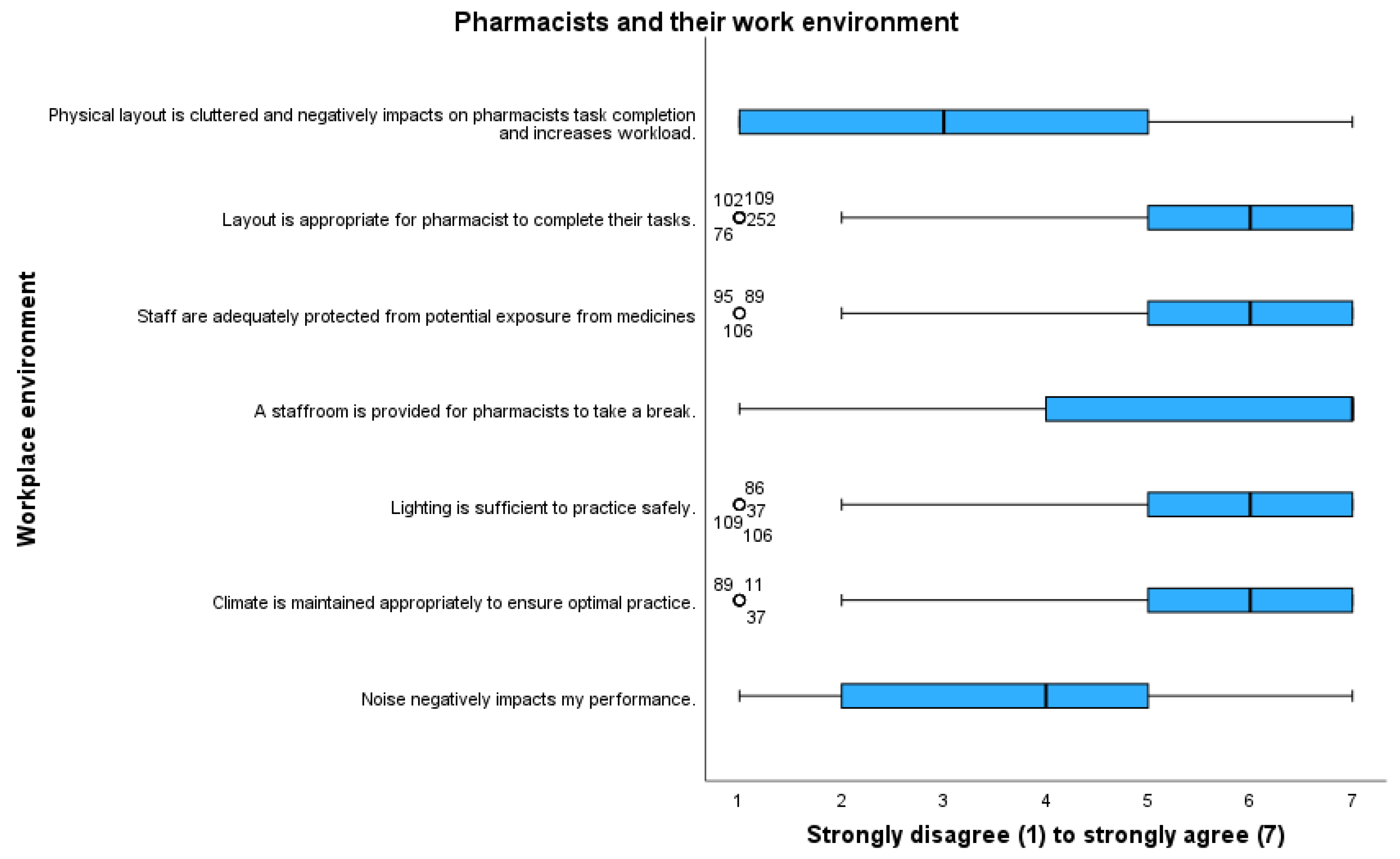
3.3.3. Liveware–Environment (L–E): Pharmacist and the Environment
3.3.4. Liveware (L): Pharmacist
3.3.5. Liveware–Liveware (L–L): Pharmacist and Others
4. Discussion
4.1. Participant Demographics
4.2. What do New Zealand Pharmacists Believe Are the Major Contributing Factors to Optimal Pharmacy Practice?
4.3. What Are the S.H.E.L.L. Factors That Affect New Zealand Pharmacy Practice?
4.4. Implications of Findings for Practice
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Croft, H.; Nesbitt, K.; Rasiah, R.; Levett-Jones, T.; Croft, C.G. Safe Dispensing in Community Pharmacies: Applying the Software, Hardware, Environment and Liveware (SHELL) Model. Pharm. J. 2017, 9. Available online: https://pharmaceutical-journalcom.ezproxy.auckland.ac.nz/article/research/safe-dispensing-in-community-pharmacies-applying-the-software-hardwareenvironment-and-liveware-S.H.E.L.L-model (accessed on 8 September 2021).
- Weir, N.M.; Newham, R.; Bennie, M. A literature review of human factors and ergonomics within the pharmacy dispensing process. Res. Soc. Adm. Pharm. 2020, 16, 637–645. [Google Scholar] [CrossRef]
- Kinsey, H.; Scahill, S.; Bye, L.; Harrison, J. Funding for change: New Zealand pharmacists’ views on, and experiences of, the community pharmacy services agreement. Int. J. Pharm. Pract. 2016, 24, 379–389. [Google Scholar] [CrossRef]
- McDonald, J.; Morris, C.; Pledger, M.; Dunn, P.; Fa’asalele Tanuvasa, A.; Smiler, K.; Cumming, J. A national survey of pharmacists and interns in Aotearoa New Zealand: Provision and views of extended services in community pharmacies. BMC Health Serv. Res. 2021, 21, 1147. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.C.; Parkin, R. The challenges of COVID-19 for community pharmacists and opportunities for the future. Ir. J. Psychol. Med. 2020, 37, 198–203. [Google Scholar] [CrossRef]
- Johnston, K.; O’Reilly, C.L.; Cooper, G.; Mitchell, I. The burden of COVID-19 on pharmacists. J. Am. Pharm. Assoc. 2021, 61, e61–e64. [Google Scholar] [CrossRef] [PubMed]
- Paudyal, V.; Cadogan, C.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Stewart, D. Provision of clinical pharmacy services during the COVID-19 pandemic: Experiences of pharmacists from 16 European countries. Res. Soc. Adm. Pharm. 2021, 17, 1507–1517. [Google Scholar] [CrossRef]
- Merks, P.; Jakubowska, M.; Drelich, E.; Świeczkowski, D.; Bogusz, J.; Bilmin, K.; Sola, K.F.; May, A.; Majchrowska, A.; Koziol, M.; et al. The legal extension of the role of pharmacists in light of the COVID-19 global pandemic. Res. Soc. Adm. Pharm. 2021, 17, 1807–1812. [Google Scholar] [CrossRef]
- Visacri, M.B.; Figueiredo, I.V.; Lima, T.d.M. Role of pharmacist during the COVID-19 pandemic: A scoping review. Res. Soc. Adm. Pharm. 2021, 17, 1799–1806. [Google Scholar] [CrossRef]
- Sridhar, S.B.; Rabbani, S.A. Pharmaceutical care services provided by pharmacists during COVID-19 pandemic: Perspectives from around the World. J. Pharm. Health Serv. Res. 2021, 12, 463–468. [Google Scholar] [CrossRef]
- Alqenae, F.A.; Steinke, D.; Keers, R.N. Prevalence and Nature of Medication Errors and Medication-Related Harm Following Discharge from Hospital to Community Settings: A Systematic Review. Drug Saf. 2020, 43, 517–537. [Google Scholar] [CrossRef] [PubMed]
- Naseralallah, L.M.; Hussain, T.A.; Jaam, M.; Pawluk, S.A. Impact of pharmacist interventions on medication errors in hospitalized pediatric patients: A systematic review and meta-analysis. Int. J. Clin. Pharm. 2020, 42, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Hignett, S.; Jones, E.L.; Miller, D.; Wolf, L.; Modi, C.; Shahzad, M.W.; Buckle, P.; Banerjee, J.; Catchpole, K. Human factors and ergonomics and quality improvement science: Integrating approaches for safety in healthcare. BMJ Qual. Saf. 2015, 24, 250. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Li, C.; Gao, X.; Liu, F.; Lin, P. Influence of the medication environment on the unsafe medication behaviour of nurses: A path analysis. J. Clin. Nurs. 2018, 27, 2993–3000. [Google Scholar] [CrossRef] [PubMed]
- Antunes, P.; Bandeira, R.; Carriço, L.; Zurita, G.; Baloian, N.; Vogt, R. Risk Assessment in Healthcare Collaborative Settings: A Case Study Using S.H.E.L.L. In Groupware: Design, Implementation, and Use; Briggs, R.O., Antunes, P., Vreede, G.-J.D., Read, A.S., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 65–73. [Google Scholar] [CrossRef]
- Lawton, R.; McEachan, R.R.C.; Giles, S.J.; Sirriyeh, R.; Watt, I.S.; Wright, J. Development of an evidence-based framework of factors contributing to patient safety incidents in hospital settings: A systematic review. BMJ Qual. Saf. 2012, 21, 369–380. [Google Scholar] [CrossRef]
- Wong, L.S.; Ram, S.; Scahill, S. Community Pharmacists’ Beliefs about Suboptimal Practice during the Times of COVID-19. Pharmacy 2022, 10, 140. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Workforce Demographics. Pharmacy Council NZ-Public Site. Retrieved. 2021. 1 January 2022. Available online: https://pharmacycouncil.org.nz/public/workforce-demographics/ (accessed on 1 January 2022).
- Sharif, S.; Fergus, S.; Guirguis, A.; Smeeton, N.; Schifano, F. Assessing prevalence, knowledge and use of cognitive enhancers among university students in the United Arab Emirates: A quantitative study. PLoS ONE 2022, 17, e0262704. [Google Scholar] [CrossRef]
- Reddy, A.; Abebe, E.; Rivera, A.J.; Stone, J.A.; Chui, M.A. Interruptions in Community Pharmacies: Frequency, Sources, and Mitigation Strategies. Res. Soc. Adm. Pharm. RSAP 2019, 15, 1243–1250. [Google Scholar] [CrossRef]
- Shao, S.-C.; Chan, Y.-Y.; Lin, S.-J.; Li, C.-Y.; Yang, Y.-H.K.; Chen, Y.-H.; Chen, H.-Y.; Lai, E.C.-C. Workload of pharmacists and the performance of pharmacy services. PLoS ONE 2020, 15, e0231482. [Google Scholar] [CrossRef]
- Abdel-Qader, D.H.; Al Meslamani, A.Z.; Lewis, P.J.; Hamadi, S. Incidence, nature, severity, and causes of dispensing errors in community pharmacies in Jordan. Int. J. Clin. Pharm. 2021, 43, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Abu Hagar, R.; El-Dahiyat, F.; El Refae, G. Risk management in community pharmacy practice in Abu Dhabi Region: A cross-sectional study. J. Pharm. Health Serv. Res. 2020, 11, 275–285. [Google Scholar] [CrossRef]
- Turner, S.; Wright, J.S.F. The Corporatization of Healthcare Organizations Internationally: A Scoping Review of Processes, Impacts, and Mediators; Public Administration: 2021. [CrossRef]
- The Pharmacy Council of New Zealand. Workplace Pressures in Pharmacy-Practical Advice for NZ Pharmacists, Pharmacy Staff and Employers; Pharmacy Council of New Zealand: Wellington, New Zealand, 2012. [Google Scholar]
- Badro, D.A.; Sacre, H.; Hallit, S.; Amhaz, A.; Salameh, P. Good pharmacy practice assessment among community pharmacies in Lebanon. Pharm. Pract. 2020, 18, 1745. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health-Manatū Hauora. Pharmacy Quality Audits Reporting Period 2021–2022 Q1: For July–September 2021; 2022.
- Ministry of Health-Manatū Hauora. Pharmacy Quality Audits Reporting Period 2021–2022 Q2: For October–November 2021; 2022.
- Holden, R.J.; Abebe, E.; Russ-Jara, A.L.; Chui, M.A. Human factors and ergonomics methods for pharmacy research and clinical practice. Res. Soc. Adm. Pharm. 2021, 17, 2019–2027. [Google Scholar] [CrossRef] [PubMed]
- Storm, F.A.; Chiappini, M.; Dei, C.; Piazza, C.; André, E.; Reißner, N.; Brdar, I.; Delle Fave, A.; Gebhard, P.; Malosio, M.; et al. Physical and mental well-being of cobot workers: A scoping review using the Software-Hardware-Environment-Liveware-Liveware-Organization model. Hum. Factors Ergon. Manuf. Serv. Ind. 2022, 32, 419–435. [Google Scholar] [CrossRef]
- Chionis, D.; Karanikas, N. Risk Perception and Risk Communication from a Systems Perspective: A Study on Safety Behavioural Intervention Frameworks and Functions. Syst. Pract. Action Res. 2022, 35, 711–746. [Google Scholar] [CrossRef]
- Bush, J.; Langley, C.A.; Wilson, K.A. The corporatization of community pharmacy: Implications for service provision, the public health function, and pharmacy’s claims to professional status in the United Kingdom. Res. Soc. Adm. Pharm. 2009, 5, 305–318. [Google Scholar] [CrossRef]
- Yong, F.R.; Hor, S.-Y.; Bajorek, B.V. Australian community pharmacy service provision factors, stresses and strains: A qualitative study. Explor. Res. Clin. Soc. Pharm. 2023, 9, 100247. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Total |
|---|---|
| n (n%) | |
| Age | |
| 20–25 years | 22 (8.5) |
| 26–30 years | 31 (11.9) |
| 31–35 years | 35 (13.5) |
| 36–40 years | 19 (7.3) |
| 41–45 years | 16 (6.2) |
| 46–50 years | 24 (9.2) |
| 51–55 years | 35 (13.5) |
| 56–60 years | 29 (11.2) |
| 61–65 years | 20 (7.7) |
| 65 and above | 9 (3.5) |
| Total | 240 (92.3) |
| Missing | 20 (0.66) |
| Gender | |
| Female | 172 (66.2) |
| Male | 68 (26.2) |
| Non-Binary | 0 (0) |
| Prefer not to say | 0 (0) |
| Total | 240 (92.3) |
| Missing | 20 (7.7) |
| Years in Practice | |
| 0–2 years | 28 (10.8) |
| 3–5 years | 20 (7.7) |
| 6–10 years | 33 (12.7) |
| 11–15 years | 24 (9.2) |
| 16–20 years | 16 (6.2) |
| 21–25 years | 17 (6.5) |
| 26–30 years | 31 (11.9) |
| 30 and above | 70 (26.9) |
| Total | 239 (91.9) |
| Missing | 21 (8.1) |
| Workplace | Total |
| Community Pharmacy Owner | 51 (19.6) |
| Community Pharmacy Manager | 26 (10) |
| Community Pharmacist | 85 (32.7) |
| Community Locum Pharmacist | 12 (4.6) |
| Academia | 3 (1.2) |
| Hospital | 36 (13.8) |
| Industry | 2 (0.8) |
| General Practitioner/Primary Health Organization | 10 (3.8) |
| Prescriber Pharm | 2 (0.8) |
| Other | 13 (5.0) |
| Total | 240 (92.3) |
| Missing | 20 (7.7) |
| Do You Think the Following Factors Affect Pharmacy Practice | Yes (%) | n | No (%) | n |
|---|---|---|---|---|
| Fatigue and lack of awareness, and inattention | 99.40% | 159 | 0.60% | 1 |
| Stress | 99.40% | 158 | 0.60% | 1 |
| Attitude towards safety | 98.70% | 157 | 1.30% | 2 |
| Knowledge | 97.50% | 156 | 2.50% | 4 |
| Distractions or interruptions | 97.50% | 157 | 2.50% | 4 |
| Lighting | 97.30% | 146 | 2.70% | 4 |
| Communication between pharmacists and pharmacy technicians/pharmacy assistants/senior supervisors/managers/other health professionals in the same workplace | 97.20% | 141 | 2.80% | 4 |
| Skills | 96.90% | 154 | 3.10% | 5 |
| Physical layout of the workplace | 96.70% | 147 | 3.30% | 5 |
| Complacency | 96.30% | 154 | 3.80% | 6 |
| Do You Think the Following Factors Affect Pharmacy Practice | Yes (%) | n | No (%) | n |
|---|---|---|---|---|
| Cultural differences | 70.50% | 98 | 29.50% | 41 |
| Staffroom | 73.10% | 98 | 26.90% | 36 |
| Professional and ethical requirements | 78.70% | 129 | 21.30% | 35 |
| Substance exposure | 79.70% | 98 | 20.30% | 25 |
| Changes to dispensing processes, SOPs, or procedural guidance/policy | 80.40% | 123 | 19.60% | 30 |
| Lack of assertiveness of members within the team | 84.60% | 121 | 15.40% | 22 |
| Lack of consistency in barcode scanning and not using barcode scanners as intended every time a medication is dispensed | 84.90% | 101 | 15.10% | 18 |
| Workplace norms | 85.70% | 138 | 14.30% | 23 |
| Alcohol, medication, drugs | 85.90% | 122 | 14.10% | 20 |
| Inadequate dispensing processes, dissemination, and enforcement of standard operating procedures (SOPs) or procedural guidance/policy | 86.50% | 134 | 13.50% | 21 |
| What Are the Factors Which You Would Associate with OPTIMAL Practice in Your Workplace? | |||
|---|---|---|---|
| Framework | Emerging Theme | Sub-Theme | Pharmacist Quote |
| Software | Leadership and Management | Practice within legislative boundaries Quality improvement Best practice compliance Representation and engagement | “Constant quality improvement of standards…regular identification and mitigation of errors, hands-on involvement from owner… A no-blame culture when errors are made… a focus on the “process” and not the “person” (Pharmacist 4) “Most important is the team culture, if a high standard of work is valued by the team and the leadership then this sets the tone of the workplace.” (Pharmacist 32) |
| Hardware | Resourcing | Adequate staffing Appropriate remuneration Training and Continuing education Adequate equipment Up to date Information Technology equipment | “Adequate staffing that allows time to complete our work to a high standard, keep abreast of best practice and reflect on how we can improve is vital.” (Pharmacist 32) “Resource management and skill/experience. Community pharmacy is an ad hoc on-call healthcare service provider with income that is derived predominantly from the supply and distribution of medication. An optimal workplace is one that delivers healthcare solutions to customers that meets the illness and wellness needs and expectations of those customers. The ad hoc nature of the service requires flexible resource allocation. That is, human, logistical and product resources need to be coordinated and re-leased in a way that enables effective and timely service provision to our customers. To provide that flexibility one needs a diverse resources and systems (including automation) that enable that release and an economy that enables the provision of those resources.” (Pharmacist 77) |
| Environment | Operating environment | Staff Safety Standard Operating Procedures Good workflow and design Teamwork and supportive culture Lighting Ventilation Order and tidiness No interruptions | “Having time to accurately dispense, having time to listen to patient’s needs, being able to access doctor’s (both private and public) patient notes to understand what they actually intend, having time to study at work, having time to take a break and sit down during a normal 9 h day.” (Pharmacist 37) “Robust standard operating procedures, good communication within team, physical premises are kept neat, organized and tidy premises is secure and staff are safe from hazards.” (Pharmacist 3). “Collegial support, moderately paced environment, having another pharmacist to double-check and verify prescriptions. Clear communication between colleagues and clear bench space to work with. Organized workspace also helps to optimize workflow and encourages good practice, e.g., placement of folders, caution and advisory labels.” (Pharmacist 47) |
| Liveware | Personnel | Experience Passion Professionalism and integrity Patient-centered care Flexibility in approach to dealings | “Quality staff who can work effectively at a high level independently, who are confident and competent within their role, who know the role and tasks they do within the team.” (Pharmacist 58) “Friendliness, informative, compassionate service, attention to detail and accuracy and ability to question if concerns arise over prescriptions, ensuring continually updating skills, knowledge and reviewing one’s own practice, enquiring nature and the desire to learn more about the patient, their health and relationships.” (Pharmacist 93) |
| Liveware-Liveware | Communication and relationships | Honesty Trust External engagement with organizations and professional bodies | “Enough support from colleagues and being able to effectively communicate with doctors regarding clinical issues.” (Pharmacist 43) “Good relationships—to work as a team—within the pharmacy and also with local healthcare providers-e.g., doctors, nurses, physio, hospital.” (Pharmacist 93) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, L.S.; Ram, S.; Scahill, S.L. Understanding the Risk Factors and Stressors Impacting Optimal Work Practices in New Zealand Pharmacies: A S.H.E.L.L Model Analysis. Pharmacy 2023, 11, 90. https://doi.org/10.3390/pharmacy11030090
Wong LS, Ram S, Scahill SL. Understanding the Risk Factors and Stressors Impacting Optimal Work Practices in New Zealand Pharmacies: A S.H.E.L.L Model Analysis. Pharmacy. 2023; 11(3):90. https://doi.org/10.3390/pharmacy11030090
Chicago/Turabian StyleWong, Lun Shen, Sanyogita (Sanya) Ram, and Shane L. Scahill. 2023. "Understanding the Risk Factors and Stressors Impacting Optimal Work Practices in New Zealand Pharmacies: A S.H.E.L.L Model Analysis" Pharmacy 11, no. 3: 90. https://doi.org/10.3390/pharmacy11030090
APA StyleWong, L. S., Ram, S., & Scahill, S. L. (2023). Understanding the Risk Factors and Stressors Impacting Optimal Work Practices in New Zealand Pharmacies: A S.H.E.L.L Model Analysis. Pharmacy, 11(3), 90. https://doi.org/10.3390/pharmacy11030090