

The Impact of an Antimicrobial Stewardship Clinical Pharmacy Specialist on Antimicrobial Days of Therapy through Education Driven Policies, Procedures, and Interventions


Abstract
:1. Introduction
2. Materials and Methods
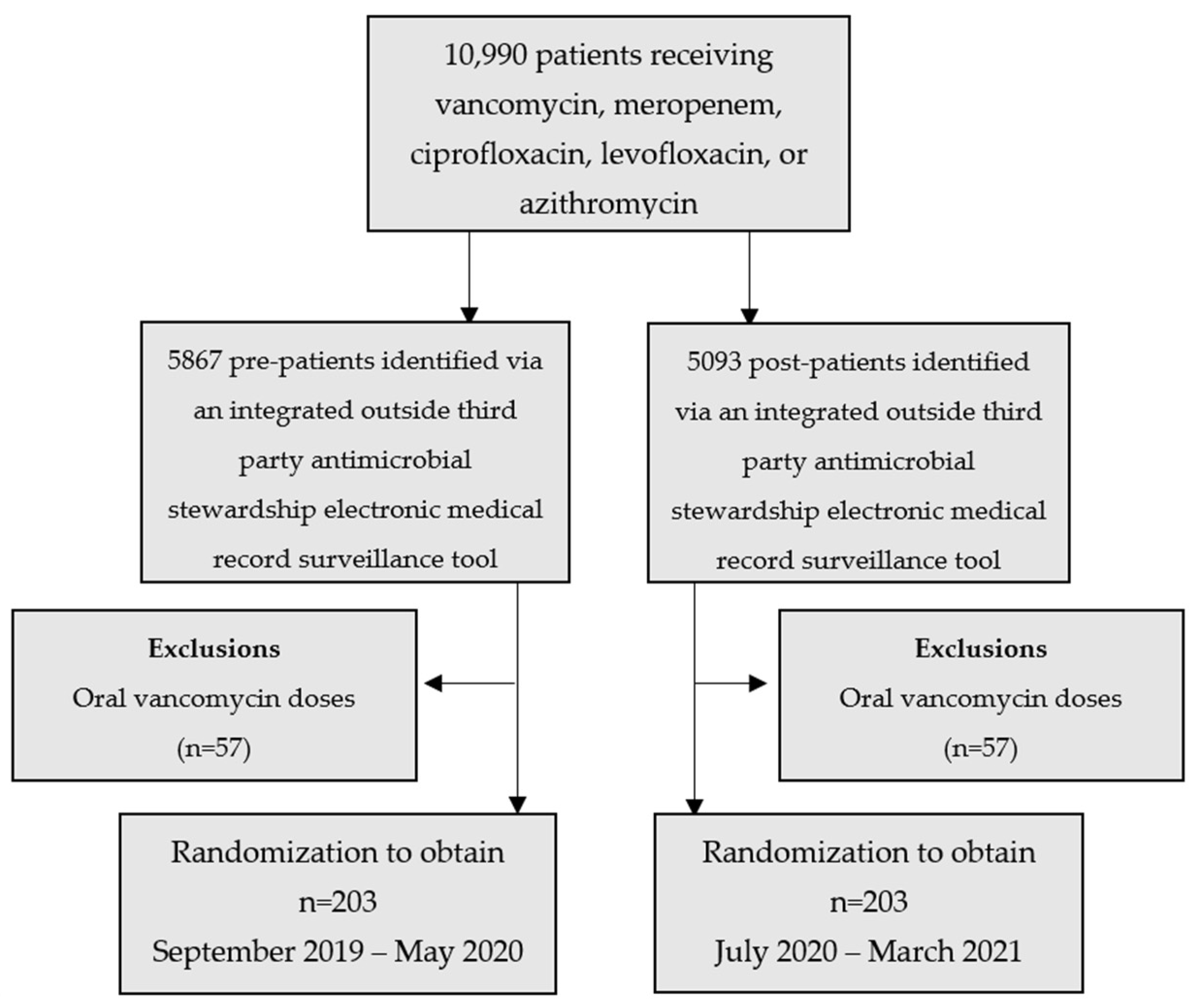
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horton, C.D.; Rawlins, M.D.M.; Manning, L.; Ingram, P.R. Non-adherence to antimicrobial stewardship prospective audit and feedback advice: Risk factors and clinical consequences. J. Infect. Chemother. 2019, 25, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Parente, D.M.; Morton, J. Role of the Pharmacist in Antimicrobial Stewardship. Med. Clin. N. Am. 2018, 102, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Chung, G.W.; Wu, J.E.; Yeo, C.L.; Chan, D.; Hsu, L.Y. Antimicrobial stewardship: A review of prospective audit and feedback systems and an objective evaluation of outcomes. Virulence 2013, 4, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Thabit, A.K.; Shea, K.M.; Guzman, O.E.; Garey, K.W. Antibiotic utilization within 18 community hospitals in the United States: A 5-year analysis. Pharmacoepidemiol. Drug Saf. 2021, 30, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Teshome, B.F.; Vouri, S.M.; Hampton, N.; Kollef, M.H.; Micek, S.T. Duration of Exposure to Antipseudomonal β-Lactam Antibiotics in the Critically Ill and Development of New Resistance. Pharmacotherapy 2019, 39, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Greene, M.H.; Nesbitt, W.J.; Nelson, G.E. Antimicrobial stewardship staffing: How much is enough? Infect. Control Hosp. Epidemiol. 2020, 41, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance: Key Facts. 2021. Available online: https://www.who.int/new-room/fact-sheets/detail/antibiotic-resistance (accessed on 13 May 2023).
- Talbot, G.H.; Bradley, J.; Edwards, J.E., Jr.; Gilbert, D.; Scheld, M.; Bartlett, J.G. Bad bugs need drugs: An update on the development pipeline from the Antimicrobial Availability Task Force of the Infectious Diseases Society of America. Clin. Infect. Dis. 2006, 42, 657–668. [Google Scholar] [CrossRef] [PubMed]
- DiDiodato, G.; McAthur, L. Transition from a dedicated to a non-dedicated, ward-based pharmacist antimicrobial stewardship programme model in a non-academic hospital and its impact on length of stay of patients admitted with pneumonia: A prospective observational study. BMJ Open Qual. 2017, 6, e000060. [Google Scholar] [CrossRef] [PubMed]
- Heil, E.L.; Kuti, J.L.; Bearden, D.T.; Gallagher, J.C. The essential role of pharmacists in antimicrobial stewardship. Infect. Control Hosp. Epidemiol. 2016, 37, 753–754. [Google Scholar] [CrossRef] [PubMed]
- Core Elements of Hospital Antibiotic Stewardship Programs. Centers for Disease Control and Prevention. CDC.gov. 2021. Available online: www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 13 May 2023).
- Ibrahim, O.M.; Polk, R.E. Antimicrobial use metrics and benchmarking to improve stewardship outcomes: Methodology, opportunities, and challenges. Infect. Dis. Clin. N. Am. 2014, 28, 195–214. [Google Scholar] [CrossRef] [PubMed]
- MedWatch: The FDA Safety Information and Adverse Event Reporting Program. Food and Drug Administration. Available online: https://www.fda.gov/safety/medwatch-fda-safety-information-andadverse-event-reporting-program (accessed on 13 May 2023).
- McGuinness, W.A.; Malachowa, N.; DeLeo, F.R. Vancomycin Resistance in Staphylococcus aureus. Yale J. Biol. Med. 2017, 90, 269–281. [Google Scholar] [PubMed]
- Codjoe, F.S.; Donkor, E.S. Carbapenem Resistance: A Review. Med. Sci. 2017, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Socan, M. Treatment of atypical pneumonia with azithromycin: Comparison of 5-day and a 3-day course. J. Chemother. 1998, 10, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Tanuma, K.; Iio, S.; Saito, J.; Komura, M.; Yamatani, A. Impact of a Pharmacist-Led Antimicrobial Stewardship Program on the Number of Days of Antimicrobial Therapy for Uncomplicated Gram-Negative Bacteremia in a Community Hospital. Cureus 2021, 13, e14635. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 6 June 2022).
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Vidal, C.; Sanjuan, G.; Moreno-García, E.; Puerta-Alcalde, P.; Garcia-Pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. COVID-19 Researchers Group. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Nicola, M.; O’Neill, N.; Sohrabi, C.; Khan, M.; Agha, M.; Agha, R. Evidence based management guideline for the COVID-19 pandemic—Review article. Int. J. Surg. 2020, 77, 206–216. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | Pre-Intervention n = 203 | Post-Intervention n = 203 | p-Value |
|---|---|---|---|
| Age, years | p = 0.0271 | ||
| Mean (SD) | 67 (18) | 62 (21) | |
| Length of stay, days | p = 0.05892 | ||
| Median (IQR) | 4.02 (2.19–7.55) | 4.28 (2.10–8.09) | |
| Male, n (%) | p = 0.04845 | ||
| Male | 104 (51) | 111 (55) | |
| Hospital Service, n (%) | p < 0.0001 | ||
| General medicine | 59 (29) | 45 (22) | |
| Oncology | 48 (24) | 37 (18) | |
| Surgical care | 11 (5) | 21 (10) | |
| Intermediate care | 11 (5) | 10 (5) | |
| Neurointensive care | 4 (2) | 5 (3) | |
| Allergies to antibiotics, n (%) | p = 0.0223 | ||
| No known drug allergies (NKDA) | 148 (73) | 169 (83) | |
| Allergies with no listed reaction | 46 (23) | 25 (12) | |
| Allergies with listed reactions | 9 (4) | 9 (4) | |
| Antibiotics, n (%) | p = 0.8459 | ||
| Vancomycin | 101 (50) | 99 (49) | |
| Azithromycin | 49 (24) | 55 (27) | |
| Ciprofloxacin | 23 (11) | 21 (10) | |
| Levofloxacin | 16 (8) | 16 (8) | |
| Meropenem | 13 (6) | 10 (5) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez, Y.G.; Tran, M.; Roduta, T.; Lam, S.; Price, T.; Stramel, S. The Impact of an Antimicrobial Stewardship Clinical Pharmacy Specialist on Antimicrobial Days of Therapy through Education Driven Policies, Procedures, and Interventions. Pharmacy 2023, 11, 137. https://doi.org/10.3390/pharmacy11050137
Martinez YG, Tran M, Roduta T, Lam S, Price T, Stramel S. The Impact of an Antimicrobial Stewardship Clinical Pharmacy Specialist on Antimicrobial Days of Therapy through Education Driven Policies, Procedures, and Interventions. Pharmacy. 2023; 11(5):137. https://doi.org/10.3390/pharmacy11050137
Chicago/Turabian StyleMartinez, Yolanda G., MaiCuc Tran, Thomas Roduta, Susan Lam, Todd Price, and Stefanie Stramel. 2023. "The Impact of an Antimicrobial Stewardship Clinical Pharmacy Specialist on Antimicrobial Days of Therapy through Education Driven Policies, Procedures, and Interventions" Pharmacy 11, no. 5: 137. https://doi.org/10.3390/pharmacy11050137
APA StyleMartinez, Y. G., Tran, M., Roduta, T., Lam, S., Price, T., & Stramel, S. (2023). The Impact of an Antimicrobial Stewardship Clinical Pharmacy Specialist on Antimicrobial Days of Therapy through Education Driven Policies, Procedures, and Interventions. Pharmacy, 11(5), 137. https://doi.org/10.3390/pharmacy11050137