Co-Morbidities as Predictors of Airflow Limitation among Smokers in England



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Questionnaire
2.3. Data Analysis
2.4. Ethical Consideration
3. Results
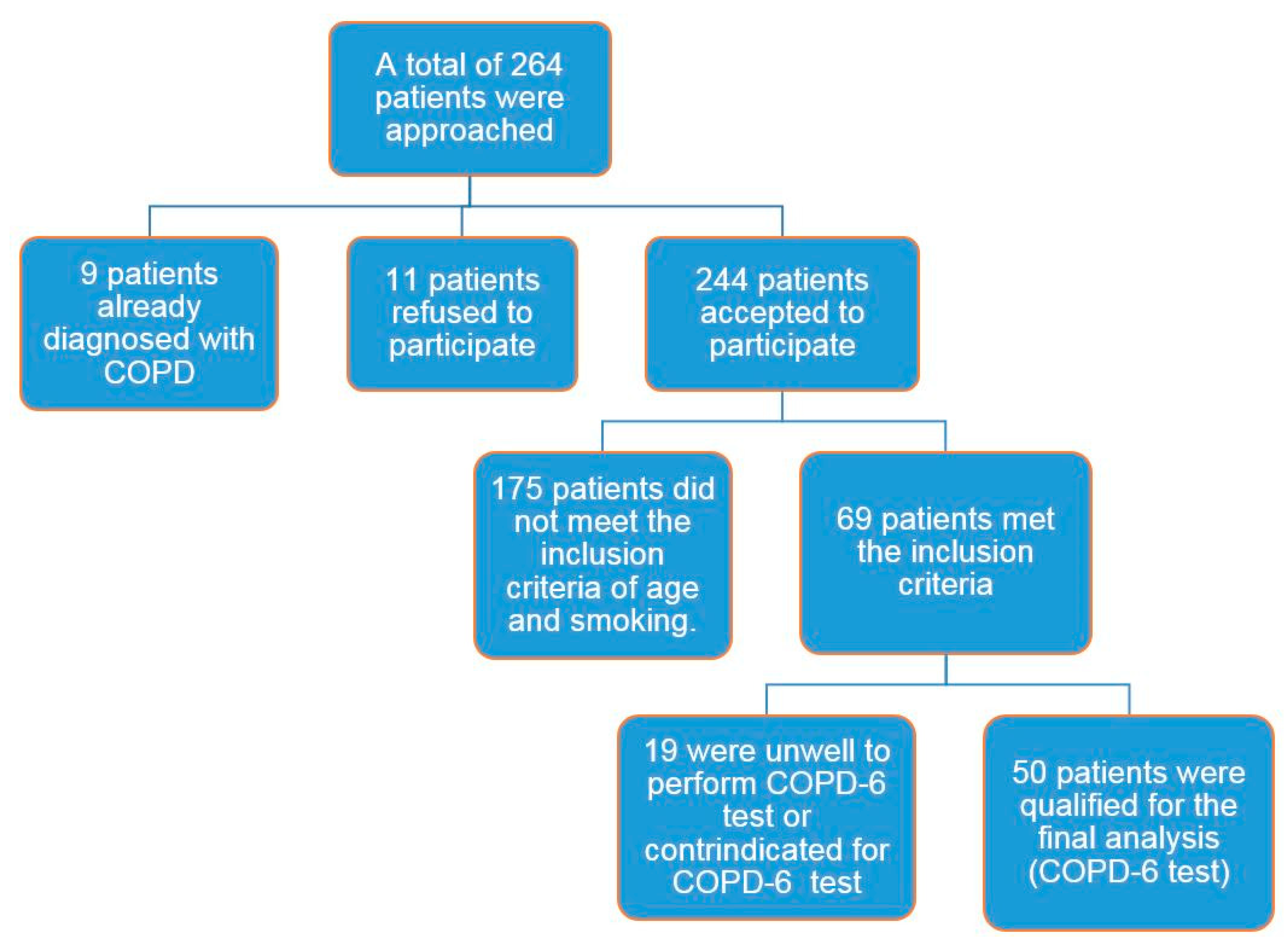
3.1. Participants’ Characteristics
3.2. COPD-6 Screening
3.3. Predictive Factors of Airflow Limitation
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A. Study Questionnaire
| Name: | |
| Date Of Birth: | |
| Age: | |
| Phone number: | |
| Ward: |
| Height: | |
| MRC: | 1/2/3/4/5 |
| Smoking status: | Y/N |
| Pack years: |
| Current or suspected respiratory infection | Y/N |
| Any antibiotics/prednisolone within the last 6 weeks | Y/N |
| Aneurysm (not treated) | Y/N |
| Unwell today, i.e., nausea, vomiting or pain | Y/N |
| Uncontrolled blood pressure | Y/N |
| Communication problems, i.e., dementia | Y/N |
| Ear problems, i.e., ear infection | Y/N |
| Eye problems, i.e., glaucoma | Y/N |
| Pregnancy | Y/N |
| Collapsed lung | Y/N |
| Haemoptysis of unknown cause | Y/N |
| Myocardial infarction or unstable heart condition | Y/N |
| Abdominal, chest, ear or eye surgery | Y/N |
| PE or Blood clot on the lung | Y/N |
| Stroke | Y/N |
| FEV1 | FEV1% Pred | FEV6 | FEV6% Pred | Ratio | |
| Effort 1 | |||||
| Effort 2 | |||||
| Effort 3 |
References
- Hesso, I.; Gebara, S.N.; Kayyali, R. Impact of community pharmacists in COPD management: Inhalation technique and medication adherence. Respir. Med. 2016, 118, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Depatment of Health (DH). An Outcomes Strategy for Chronic Obstructive Pulmonary Disease (COPD) and Asthma in England; Depatment of Health & Social Care: London, UK, 2011.
- Celli, B.R.; MacNee, W. ATS/ERS task force: Standards for the diagnosis and treatment of patients with COPD: A summary of the ATS/ERS position paper. Eur. Respir. J. 2004, 23, 932–946. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Global Srategy for the Diagnosis Management and Prevention of Chronic Obstructive Pulmonary Disease, Updated 2015. Available online: http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf (accessed on 7 January 2018).
- Kayyali, R.; Odeh, B.; Frerichs, I.; Davies, N.; Perantoni, E.; D’arcy, S. COPD care delivery pathways in five European Union countries: Mapping and health care professionals’ perceptions. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2831. [Google Scholar] [CrossRef] [PubMed]
- Löfdahl, C. COPD and co-morbidities, with special emphasis on cardiovascular conditions. Clin. Respir. J. 2008, 2, 59–63. [Google Scholar] [CrossRef] [PubMed]
- MacNee, W. Systemic inflammatory biomarkers and co-morbidities of chronic obstructive pulmonary disease. Ann. Med. 2013, 45, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, H.; Watz, H. Systemic inflammation in chronic obstructive pulmonary disease and asthma: Relation with comorbidities. Proc. Am. Thorac. Soc. 2009, 6, 648–651. [Google Scholar] [CrossRef] [PubMed]
- COPD Strategy Group. Chronic Obstructive Pulmonary Disease (COPD) Strategy 2010–2015. Available online: www.cress.bics.nhs.uk/EasySiteWeb/GatewayLink.aspx?alId=1907 (accessed on 17 January 2018).
- NICE. Chronic Obstructive Pulmonary Disease—Casting Report—Implementing NICE Guidelines; NICE: London, UK, 2011. [Google Scholar]
- Stenton, C. The MRC breathlessness scale. Occup. Med. (Lond.) 2008, 58, 226–227. [Google Scholar] [CrossRef] [PubMed]
- Rosa, F.W.; Perez-Padilla, R.; Camelier, A.; Nascimento, O.A.; Menezes, A.M.B.; Jardim, J.R. Efficacy of the FEV1/FEV6 ratio compared to the FEV1/FVC ratio for the diagnosis of airway obstruction in subjects aged 40 years or over. Braz. J. Med. Biol. Res. 2007, 40, 1615–1621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ching, S.; Pang, Y.; Price, D.; Cheong, A.; Lee, P.; Irmi, I. Detection of airflow limitation using a handheld spirometer in a primary care setting. Respirology 2014, 19, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Fathima, M.; Naik-Panvelkar, P.; Saini, B.; Armour, C. The role of community pharmacists in screening and subsequent management of chronic respiratory diseases: A systematic review. Pharm. Pract. (Granada) 2013, 11, 228–245. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.; Twigg, M.; Thornley, T. Chronic obstructive pulmonary disease case finding by community pharmacists: A potential cost-effective public health intervention. Int. J. Pharm. Pract. 2015, 23, 83–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calverley, P.M.; Nordyke, R.J.; Halbert, R.; Isonaka, S.; Nonikov, D. Development of a population-based screening questionnaire for COPD. COPD J. Chronic Obstr. Pulm. Dis. 2005, 2, 225–232. [Google Scholar] [CrossRef]


{kind=link}
| Variables | No Airflow Limitation (n = 29) | Have Airflow Limitation (n = 21) | P-Values |
|---|---|---|---|
| Age, years (median) | 53 | 56 | |
| Age ≥ 60, n (%) | 8 (28%) | 9 (43%) | 0.336 |
| Age < 60, n (%) | 21 (72%) | 12 (57%) | |
| Female gender, n (%) | 19 (66%) | 11 (52%) | 0.371 |
| Male gender, n (%) | 10 (34%) | 10 (48%) | |
| Smoking history, pack-years | - | - | |
| <20, n (%) | 16 (55%) | 5 (24%) | 0.029 |
| ≥20, n (%) | 13 (45%) | 16 (76%) | |
| Respiratory symptoms, n (%) MRC breathlessness grade ≥3 | 12 (41%) | 15 (71%) | 0.039 |
| Presence of co-morbidities, n (%) | 20 (69%) | 20 (95%) | 0.025 |
| Co-Morbidity | No Airflow Limitation (n = 29) | Have Airflow Limitation (n = 21) |
|---|---|---|
| Hypertension (HTN), n (%) | 4 (14%) | 9 (43%) |
| Cardiovascular diseases, n (%) | 3 (10%) | 5 (24%) |
| Hyperlipidaemia, n (%) | 7 (24%) | 4 (19%) |
| Depression, n (%) | 5 (17%) | 10 (48%) |
| Diabetes, n (%) | 4 (14%) | 4 (19%) |
| Osteoporosis, n (%) | 2 (7%) | 3 (14%) |
| Peripheral Vascular Disease (PVD), n (%) | 6 (21%) | 3 (14%) |
| Predictors of Airflow Limitation in Smokers (n = 50) | |
|---|---|
| Independent variables | Odds ratio (95% CI) |
| Age ≥ 60 | 1.97 (0.600–6.45) |
| Gender (male) | 1.72 (0.55–5.45) |
| Smoking history ≥ 20 pack-years | 3.94 (1.13–13.64) |
| Presence of respiratory symptoms | 3.54 (1.06–11.77) |
| Presence of co-morbidities | 9 (1.04–77.81) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kayyali, R.; Hassan, Y.; Hesso, I.; Siva, R. Co-Morbidities as Predictors of Airflow Limitation among Smokers in England. Pharmacy 2018, 6, 45. https://doi.org/10.3390/pharmacy6020045
Kayyali R, Hassan Y, Hesso I, Siva R. Co-Morbidities as Predictors of Airflow Limitation among Smokers in England. Pharmacy. 2018; 6(2):45. https://doi.org/10.3390/pharmacy6020045
Chicago/Turabian StyleKayyali, Reem, Yusur Hassan, Iman Hesso, and Roshan Siva. 2018. "Co-Morbidities as Predictors of Airflow Limitation among Smokers in England" Pharmacy 6, no. 2: 45. https://doi.org/10.3390/pharmacy6020045
APA StyleKayyali, R., Hassan, Y., Hesso, I., & Siva, R. (2018). Co-Morbidities as Predictors of Airflow Limitation among Smokers in England. Pharmacy, 6(2), 45. https://doi.org/10.3390/pharmacy6020045