The Use of Video Instructions in Patient Education Promoting Correct Technique for Dry Powder Inhalers: An Investigation on Inhaler-Naïve Individuals


Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Pilot
2.3. Study Population and Sample
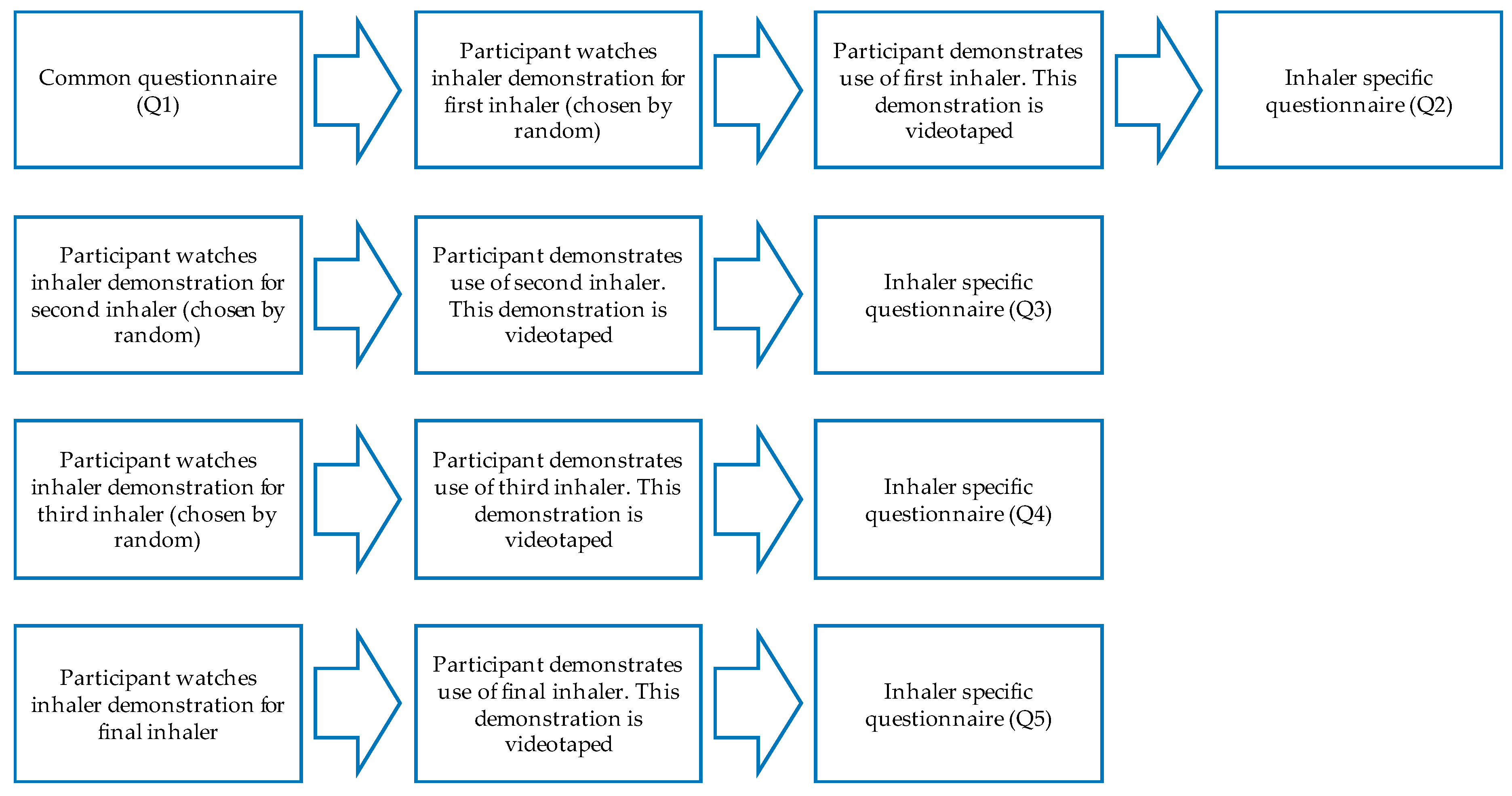
2.4. Data Collection
2.5. Educational Videos
2.6. Analysis of Data
2.6.1. Frequency and Characterization of Errors
2.6.2. Analysis of Semi-Structured Questionnaires
2.7. Ethics
3. Results
3.1. Frequency and Characterization of Errors
3.2. Results from Semi Structured Interviews
4. Discussion and Conclusions
4.1. Discussion
4.1.1. Potential Areas for Development in Educational Videos for Asthma
4.1.2. Limitations to This Study
4.2. Conclusions
4.3. Practical Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Inhaler | Instructions | Errors measured |
|---|---|---|
| Diskus |
|
|
| Easy-haler |
|
|
| Ellipta |
|
|
| Turbu-haler |
|
|
References
- Global Asthma Network. The Global Asthma Report 2014. Available online: http://www.globalasthmareport.org/ (accessed on 3 June 2017).
- Barnes, P.J. Cellular and molecular mechanisms of asthma and COPD. Clin. Sci. 2017, 131, 1541–1558. [Google Scholar] [CrossRef] [PubMed]
- Svedsater, H.; Dale, P.; Garrill, K.; Walker, R.; Woepse, M.W. Qualitative assessment of attributes and ease of use of the ELLIPTA™ dry powder inhaler for delivery of maintenance therapy for asthma and COPD. BMC Pulm. Med. 2013, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Islam, N.; Gladki, E. Dry powder inhalers (DPIs)—A review of device reliability and innovation. Int. J. Pharm. 2008, 360, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Crompton, G.K. How to achieve good compliance with inhaled asthma therapy. Respir. Med. 2004, 98, 35–40. [Google Scholar] [CrossRef]
- Fink, J.B.; Rubin, B.K. Problems with inhaler use: A call for improved clinician and patient education. Respir. Care 2005, 50, 1360–1375. [Google Scholar] [PubMed]
- Lenney, J.; Innes, J.A.; Crompton, G.K. Inappropriate inhaler use: Assessment of use and patient preference of seven inhalation devices. EDICI. Respir. Med. 2000, 94, 496–500. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Earnshaw, S.M.; Delaney, J.C. Pressurized aerosol inhalers: The cost of misuse. Br. J. Clin. Pract. 1991, 45, 48–49. [Google Scholar] [PubMed]
- Lavorini, F. The Challenge of Delivering Therapeutic Aerosols to Asthma Patients. ISRN Allergy 2013, 2013, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis, J.; Corrigan, C.; Levy, M.L.; Viejo, J.L. Inhaler devices-from theory to practice. Respir. Med. 2013, 107, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.J.; Robinson, J.D.; Doering, P.L.; Dallman, J.J.; Steeves, R.A. A comparison of various types of patient instruction in the proper administration of metered inhalers. Drug Intell. Clin. Pharm. 1982, 16, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Basheti, I.A.; Reddel, H.K.; Armour, C.L.; Bosnic-Anticevich, S.Z. Counseling about turbuhaler technique: Needs assessment and effective strategies for community pharmacist Counseling about turbuhaler technique: Needs assessment and effective strategies for community pharmacists. Respir. Care 2005, 50, 617–623. [Google Scholar] [PubMed]
- van der Palen, J.; Klein, J.J.; Kerkhoff, A.H.; van Herwaarden, C.L.; Seydel, E.R. Evaluation of the long-term effectiveness of three instruction modes for inhaling medicines. Patient Educ. Couns. 1997, 32, 87–95. [Google Scholar] [CrossRef]
- De Blaquiere, P.; Christensen, D.B.; Carter, W.B.; Martin, T.R. Use and misuse of metered-dose inhalers by patients with chronic lung disease. a controlled, randomized trial of two instruction methods. Am. Rev. Respir. Dis. 1989, 140, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Kesten, S.; Zive, K.; Chapman, K.R. Pharmacist knowledge and ability to use inhaled medication delivery systems. Chest 1993, 104, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.M.; Fink, J.B. Promoting adherence to inhaled therapy. Respir. Care Clin. N. Am. 2001, 7, 277–301. [Google Scholar] [CrossRef]
- Hämmerlein, A.; Müller, U.; Schulz, M. Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J. Eval. Clin. Pract. 2011, 17, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Self, T.H.; Brooks, J.B.; Lieberman, P.; Ryan, M.R. The value of demonstration and role of pharmacist in teaching the correct use of pressurized bronchodilators. Can. Med. Assoc. J. 1983, 128, 129–131. [Google Scholar] [PubMed]
- Wilson, E.A.H.; Park, D.C.; Curtis, L.M.; Cameron, K.A.; Clayman, M.L.; Makoul, G.; Eigen, K.V.; Wolf, M.S. Media and memory: The efficacy of video and print materials for promoting patient education about asthma. Patient Educ. Couns. 2010, 80, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Albert, N.M.; Buchsbaum, T.; Li, J. Randomized study of the effect of video education on heart failure healthcare utilization, symptoms, and self-care behaviors. Patient Educ. Couns. 2007, 69, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Tashakori, M.; Teddlie, C.B. (Eds.) Sage Handbook of Mixed Methods in Social & Behavioral Research, 2nd ed.; SAGE: Washington, DC, USA, 2010. [Google Scholar]
- Borodulin, K.; Levälahti, E.; Saarikoski, L.; Lund, L.; Juolevi, A.; Grönholm, M.; Jula, A.; Laatikainen, T.; Männistö, S.; Peltonen, M.; et al. National FINRISKI 2012-Health Study-Part 2: Study Table Annex, National Institute for Health and Welfare; THL: Helsinki, Finland, 2013; pp. 136–137. [Google Scholar]
- Jarvis, S.; Ind, P.W.; Shiner, R.J. Inhaled therapy in elderly COPD patients; time for re-evaluation? Age Ageing 2007, 36, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnish Association of Pharmacists Dosing Videos. Available online: https://www.apteekki.fi/apteekin-neuvot/annosteluvideot.html (accessed on 1 March 2017).
- Melani, A.S.; Bonavia, M.; Cilenti, V.; Cinti, C.; Lodi, M.; Martucci, P.; Serra, M.; Scichilone, N.; Sestini, P.; Aliani, M.; et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Resp. Med. 2011, 105, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, A.L. Implementing a Video Education Program to Improve Health Literacy. J. Nurse Pract. 2012, 8, 17–22. [Google Scholar] [CrossRef]
- Göriş, S.; Taşci, S.; Elmali, F. The effects of training on inhaler technique and quality of life in patients with COPD. J. Aerosol Med. Pulm. Drug Deliv. 2013, 26, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Ovchinikova, L.; Smith, L.; Bosnic-Anticevich, S. Inhaler technique maintenance: Gaining an understanding from the patient’s perspective. J. Asthma 2011, 48, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Takemura, M.; Kobayashi, M.; Kimura, K.; Mitsui, K.; Masui, H.; Koyama, M.; Itotani, R.; Ishitoko, M.; Suzuki, S.; Aihara, K. Repeated instruction on inhalation technique improves adherence to the therapeutic regimen in asthma. J. Asthma 2010, 47, 202–208. [Google Scholar] [CrossRef] [PubMed]
- O’Bey, K.A.; Jim, L.K.; Gee, J.P.; Cowen, M.E.; Quigley, A.E. An education program that improves the psychomotor skills needed for metaproterenol inhaler use. Drug Intell. Clin. Pharm. 1982, 16, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Takaku, Y.; Kurashima, K.; Ohta, C.; Ishiguro, T.; Kagiyama, N.; Yanagisawa, T.; Takayanagi, N. How many instructions are required to correct inhalation errors in patients with asthma and chronic obstructive pulmonary disease? Resp. Med. 2017, 123, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Erickson, S.R.; Horton, A.; Kirking, D.M. Assessing metered-dose inhaler technique: Comparison of observation vs. patient self-report. J. Asthma 1998, 35, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhou, L.; Briggs, R.O.; Nunamaker, J.F. Instructional video in e-learning: Assessing the impact of interactive video on learning effectiveness. Inf. Manag. 2006, 43, 15–27. [Google Scholar] [CrossRef]
- Orion Corporation. Easyhaler Budesonide Patient Information Leaflet; Orion Corporation: Espoo, Finland, 2016. [Google Scholar]
- Melani, A.S.; Zanchetta, D.; Barbato, N.; Sestini, P.; Cinti, C.; Canessa, P.A.; Aiolfi, S.; Neri, M.; for the Associazione Italiana Pneumologi Ospedalieri Educational Group. Inhalation technique and variables associated with misuse of conventional metered-dose inhalers and newer dry powder inhalers in experienced adults. Ann. Allergy Asthma Immunol. 2004, 93, 439–446. [Google Scholar] [CrossRef]
- Melani, A.S.; Bracci, L.S.; Rossi, M. Reduced peak inspiratory effort through the Diskus® and the Turbuhaler® due to mishandling is common in clinical practice. Clin. Drug Investig. 2006, 25, 543–549. [Google Scholar] [CrossRef]
- Price, D.; Bosnic-Anticevich, S.; Briggs, A.; Chrystyn, H.; Rand, C.; Scheuch, G.; Bousquet, J. Inhaler competence in asthma: Common errors, barriers to use and recommended solutions. Respir. Med. 2012, 107, 37–46. [Google Scholar] [CrossRef] [PubMed]
- van der Palen, J.; Klein, J.J.; Kerkhoff, A.H.M.; Van Herwaarden, C.L. Evaluation of the effectiveness of four different inhalers in patients with chronic obstructive pulmonary disease. Thorax 1995, 50, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Khassawneh, B.; Al-Ali, M.; Alzoubi, K.H.; Batarseh, M.Z.; Al-Safi, S.A.; Sharara, A.M.; Alnasr, H.M. Handling of Inhaler Devices in Actual Pulmonary Practice: Metered-Dose Inhaler Versus Dry Powder Inhalers. Respir. Care 2008, 53, 324–328. [Google Scholar] [PubMed]



| Example of Ended Questions in Q2–Q5 |
|---|
|
| Diskus | Easyhaler 1 | Ellipta | Turbuhaler | |
|---|---|---|---|---|
| Number of participants who believed they had used inhaler without making a single inhalation error | 84% 26/31 | 77% 24/31 | 84% 26/31 | 61% 19/31 |
| Number of participants who actually used the inhaler without making a single inhalation error | 48% 15/31 | 19% 6/31 | 55% 16/31 | 16% 5/31 |
| Category | Sub-Category | Explanatory Quote |
|---|---|---|
| Visual instructions | “I like visual material, so videos worked well for me. This video was short, concise and easy to understand.” PN9 | |
| Factors enhancing performance | Step-by-step instructions | “In order to learn, I would need clear instructions of each step of the inhaler use. This video was enough.” PN2 |
| Type of inhaler | “The video was good and the inhaler was fairly easy to use. I don’t think you need any other instructions (than the video).” PN31 | |
| Spoken track | “I think the video was good and the tempo was fast enough. I think spoken instructions would have been a good addition to the video instructions.” PN21 | |
| Ideas on improving video education | Close-up pictures | “I think the video could have been improved by adding close-up pictures of the stages, a spoken track or background music.” PN27 |
| Complementary material | “A checklist on the steps to go with the inhaler would probably be good.” PN18 | |
| Uncertainty of own technique | “I do think that I used the inhaler correctly but I still feel a little uncertain. I think I would feel better if I could check my technique.” PN10 “I do think that I used the inhaler correctly but I still feel a little uncertain. I think I would feel better if I could check my technique.” | |
| Unanswered questions | “I would have liked to know why I had to shake this inhaler but not the others. PN7 | |
| Inhaler | “I don’t think I learned how to use this inhaler, at least not very well. The video was good, but using the inhaler was too hard.” PN22 | |
| Factors that were perceived as difficult | Unclear instructions | “The video started out simple but became confusing as it progressed. I don’t remember what should be done and in which order.” PN28 |
| Lack of feedback | “I think video instructions are much better than text instructions alone. Still, I would like to receive feedback from a pharmacist or someone else who knows how to use it.” PN20 | |
| Tempo of videos | “The tempo of the videos was quite fast and I did not have time to read all of the instructions on the screen.” PN19 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Von Schantz, S.; Katajavuori, N.; Juppo, A.M. The Use of Video Instructions in Patient Education Promoting Correct Technique for Dry Powder Inhalers: An Investigation on Inhaler-Naïve Individuals. Pharmacy 2018, 6, 106. https://doi.org/10.3390/pharmacy6040106
Von Schantz S, Katajavuori N, Juppo AM. The Use of Video Instructions in Patient Education Promoting Correct Technique for Dry Powder Inhalers: An Investigation on Inhaler-Naïve Individuals. Pharmacy. 2018; 6(4):106. https://doi.org/10.3390/pharmacy6040106
Chicago/Turabian StyleVon Schantz, Sofia, Nina Katajavuori, and Anne M. Juppo. 2018. "The Use of Video Instructions in Patient Education Promoting Correct Technique for Dry Powder Inhalers: An Investigation on Inhaler-Naïve Individuals" Pharmacy 6, no. 4: 106. https://doi.org/10.3390/pharmacy6040106
APA StyleVon Schantz, S., Katajavuori, N., & Juppo, A. M. (2018). The Use of Video Instructions in Patient Education Promoting Correct Technique for Dry Powder Inhalers: An Investigation on Inhaler-Naïve Individuals. Pharmacy, 6(4), 106. https://doi.org/10.3390/pharmacy6040106