Impact of the 2016 Policy Change on the Delivery of MedsCheck Services in Ontario: An Interrupted Time-Series Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Sources
2.3. Analytical Approach
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Long-Term Care. Preventing and Managing Chronic Disease: Ontario’s Framework; Queen’s Printer for Ontario: Toronto, ON, Canada, 2007.
- Institute of Medicine Committee on Identifying and Preventing Medication Errors. Preventing Medication Errors; National Academies Press: Washington, DC, USA, 2007. [Google Scholar]
- Sichieri, K.; Rodrigues, A.R.B.; Takahashi, J.A.; Secoli, S.R.; Nobre, M.R.C.; Mónica, M.A.; Julio, F.G. Mortality associated with the use of inappropriate drugs according Beers criteria: A systematic review. Adv. Pharmacol. Pharm. 2013, 1, 74–84. [Google Scholar]
- Dormann, H.; Criegee-Rieck, M.; Neubert, A.; Egger, T.; Geise, A.; Krebs, S.; Schneider, T.; Levy, M.; Hahn, E.; Brune, K. Lack of awareness of community-acquired adverse drug reactions upon hospital admission: Dimensions and consequences of a dilemma. Drug Saf. 2003, 26, 353–362. [Google Scholar] [CrossRef]
- Tsuyuki, R.T.; Beahm, N.P.; Okada, H.; Al Hamarneh, Y.N. Pharmacists as accessible primary health care providers: Review of the evidence. Can. Pharm. J. 2018, 151, 4–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnipper, J.L.; Kirwin, J.L.; Cotugno, M.C.; Wahlstrom, S.A.; Brown, B.A.; Tarvin, E.; Kachalia, A.; Horng, M.; Roy, C.L.; McKean, S.C.; et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch. Intern. Med. 2006, 166, 565. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, P.; Herborg, H.; Mortensen, A.R.; Knudsen, M.; Hellebek, A. Preventing medication errors in community pharmacy: Frequency and seriousness of medication errors. Qual. Saf. Health Care 2007, 16, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.S.; Benrimoj, S.I.; Chen, T.F.; Williams, K.A.; Hopp, T.R.; Aslani, P. Understanding practice change in community pharmacy: A qualitative study in Australia. Res. Soc. Adm. Pharm. 2005, 1, 546–564. [Google Scholar] [CrossRef] [PubMed]
- Houle, S.K.D.; Carter, C.A.; Tsuyuki, R.T.; Grindrod, K.A. Remunerated patient care services and injections by pharmacists: An international update. Can. Pharm. J. 2019, 152, 92–108. [Google Scholar] [CrossRef] [PubMed]
- Latif, A.; Pollock, K.; Boardman, H.F. Medicines use reviews: A potential resource or lost opportunity for general practice? BMC Fam. Pract. 2013, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Miller, A.P.; Quesnel-Vallée, A.; Caron, N.R.; Vissandjée, B.; Marchildon, G.P. Canada’s universal health-care system: Achieving its potential. Lancet 2018, 391, 1718–1735. [Google Scholar] [CrossRef]
- Ontario Ministry of Health and Long-Term Care. The MedsCheck Program Guidebook, 2nd ed.; Queen’s Printer for Ontario: Toronto, ON, Canada, 2008.
- Ontario Ministry of Health and Long-Term Care. Professional Pharmacy Services Guidebook, 3rd ed.; Queen’s Printer for Ontario: Toronto, ON, Cananda, 2016.
- MacCallum, L.; Consiglio, G.; MacKeigan, L.; Dolovich, L.; MacCallum, L. Uptake of community pharmacist-delivered MedsCheck diabetes medication review service in Ontario between 2010 and 2014. Can. J. Diabetes 2017, 41, 253–258. [Google Scholar] [CrossRef]
- Government of Ontario. Central Forms Repository. Available online: http://www.forms.ssb.gov.on.ca/mbs/ssb/forms/ssbforms.nsf?opendatabase&ENV=WWE (accessed on 7 August 2019).
- Canadian Council on Continuing Education in Pharmacy MedsCheck (Diabetes) Ontario. Available online: https://www.cccep.ca/pages/meds_check_diabetes_ontario.html (accessed on 17 May 2019).
- Jandoc, R.; Burden, A.M.; Mamdani, M.; Lévesque, L.E.; Cadarette, S.M. Interrupted time series analysis in drug utilization research is increasing: Systematic review and recommendations. J. Clin. Epidemiol. 2015, 68, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2016, 46, 348–355. [Google Scholar]
- Lagarde, M. How to do (or not to do)... Assessing the impact of a policy change with routine longitudinal data. Health Policy Plan. 2012, 27, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Durbin, J.; Watson, G.S. Testing for serial correlation in least squares regression: I. Biometrika 1950, 37, 409–428. [Google Scholar] [PubMed]
- Dickey, D.A.; Fuller, W.A. Distribution of the estimators for autoregressive time series with a unit root. J. Am. Stat. Assoc. 1979, 74, 427–431. [Google Scholar]
- Zhang, F.; Wagner, A.K.; Soumerai, S.B.; Ross-Degnan, D. Methods for estimating confidence intervals in interrupted time series analyses of health interventions. J. Clin. Epidemiol. 2009, 62, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Dolovich, L.; Consiglio, G.; MacKeigan, L.; Abrahamyan, L.; Pechlivanoglou, P.; Rac, V.E.; Pojskic, N.; Bojarski, E.A.; Su, J.; Krahn, M.; et al. Uptake of the MedsCheck annual medication review service in Ontario community pharmacies between 2007 and 2013. Can. Pharm. J. 2016, 149, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Tracy, C.S.; Upshur, R.E.G. MedsCheck: An opportunity missed. CMAJ 2008, 178, 440. [Google Scholar] [CrossRef]
- Pechlivanoglou, P.; Abrahamyan, L.; Mackeigan, L.; Consiglio, G.P.; Dolovich, L.; Li, P.; Cadarette, S.M.; Rac, V.E.; Shin, J.; Krahn, M. Factors affecting the delivery of community pharmacist-led medication reviews: Evidence from the MedsCheck annual service in Ontario. BMC Health Serv. Res. 2016, 16, 666. [Google Scholar] [CrossRef]
- Ontario Public Drug Programs, Ministry of Health and Long-Term Care. Notice from the Executive Officer: MedsCheck Program Enhancements Standardization. Available online: http://www.health.gov.on.ca/en/pro/programs/drugs/opdp_eo/notices/exec_office_20160704.pdf (accessed on 20 May 2019).
- Ontario Pharmacists Association. MedsCheck Program. Available online: https://www.opatoday.com/professional/resources/for-pharmacists/programs/medscheck (accessed on 2 July 2019).
- Ontario Ministry of Health and Long-Term Care. MedsCheck Resources for Pharmacists—Health Care Professionals. Available online: http://www.health.gov.on.ca/en/pro/programs/drugs/medscheck/resources.aspx (accessed on 2 July 2019).
- Ontario Ministry of Heath and Long-Term Care. Reforming Ontario’s Drug System. Available online: https://news.ontario.ca/mohltc/en/2010/04/reforming-ontarios-drug-system.html (accessed on 29 May 2019).
- Canadian Institute for Health Information; Canadian Patient Safety Institute; Institute for Safe Medication Practices Canada. Medication Reconciliation in Canada: Raising the Bar; Accreditiation Canada: Ottawa, ON, Canada, 2012. [Google Scholar]
- Canadian Institute for Health Information. Prescribed Drug Spending in Canada, 2018: A Focus on Public Drug Programs; Accreditiation Canada: Ottawa, ON, Canada, 2018. [Google Scholar]
- Strauss, M.; Howlett, K. Pharmacies Take Hit as Ontario Cuts Generic Drug Payments Again. Available online: https://www.theglobeandmail.com/globe-investor/pharmacies-take-hit-as-ontario-cuts-generic-drug-payments-again/article4170794/ (accessed on 29 May 2019).
- Ministry of Finance; Ministry of Heath and Long-Term Care. Stronger, Healthier Ontario Act (Budget Measures). 2017. Available online: https://news.ontario.ca/mof/en/2017/05/stronger-healthier-ontario-act-budget-measures-2017.html (accessed on 29 May 2019).
- Barnes, B.; Hincapie, A.L.; Luder, H.; Kirby, J.; Frede, S.; Heaton, P.C. Appointment-based models: A comparison of three model designs in a large chain community pharmacy setting. J. Am. Pharm. Assoc. 2018, 58, 156–162. [Google Scholar] [CrossRef] [PubMed]
- MacCallum, L.; Dolovich, L. Follow-up in community pharmacy should be routine, not extraordinary. Can. Pharm. J. 2018, 151, 79–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipolle, R.J.; Strand, L.M.; Morley, P.C. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management Services, 3rd ed.; McGraw-Hill Education: New York, NY, USA, 2012. [Google Scholar]
- Ontario Ministry of Health and Long Term Care. MedsCheck at Home. Available online: http://www.health.gov.on.ca/en/pro/programs/drugs/medscheck/medscheck_home.aspx (accessed on 23 May 2019).
- Ontario Long Term Care Association. This Is Long-Term Care 2018; Ontario Long Term Care Association: Toronto, ON, Canada, 2018. [Google Scholar]
- Lipscombe, L.L.; Hux, J.E. Trends in diabetes prevalence, incidence, and mortality in Ontario, Canada 1995–2005: A population-based study. Lancet 2007, 369, 750–756. [Google Scholar] [CrossRef]
- Statistics Canada Diabetes, by Age Group and Sex (Number of Persons). Available online: http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/health53a-eng.htm (accessed on 22 May 2018).
- Ontario Ministry of Health and Long-Term Care. Diabetes: Strategies for Prevention. Available online: http://www.health.gov.on.ca/en/common/ministry/publications/reports/diabetes/diabetes.aspx (accessed on 22 May 2019).
- Ontario Long Term Care Association. This Is Long-Term Care 2016; Ontario Long Term Care Association: Toronto, ON, Canada, 2016. [Google Scholar]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M.; Medical Research Council guidance. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337. [Google Scholar] [CrossRef] [PubMed]
- Bleijenberg, N.; de Man-van Ginkel, J.M.; Trappenburg, J.C.A.; Ettema, R.G.A.; Sino, C.G.; Heim, N.; Hafsteindóttir, T.B.; Richards, D.A.; Schuurmans, M.J. Increasing value and reducing waste by optimizing the development of complex interventions: Enriching the development phase of the Medical Research Council (MRC) Framework. Int. J. Nurs. Stud. 2018, 79, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drugs and Devices Division: Ministry of Health and Long-Term Care. Proposals to Establish More Efficient Pharmacy Reimbursement Policies. Available online: http://www.health.gov.on.ca/en/pro/programs/drugs/opdp_eo/notices/exec_office_20190426.pdf (accessed on 2 July 2019).
- Office of the Auditor General of Ontario. Chapter 3: Reports on Value-for-Money, 3.09: Ontario Public Drug Programs. 2017 Annual Report Volume 2; Queen’s Printer for Ontario: Toronto, ON, Canada, 2017.
- Ministry of Finance. 2019 Ontario Budget|Chapter 3: Ontario’s Fiscal Plan and Outlook. Available online: http://budget.ontario.ca/2019/chapter-3.html (accessed on 2 July 2019).
- Al-Rashed, S.A.; Wright, D.J.; Roebuck, N.; Sunter, W.; Chrystyn, H. The value of inpatient pharmaceutical counselling to elderly patients prior to discharge. Br. J. Clin. Pharmacol. 2002, 54, 657–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, B.W.; Chetty, V.K.; Anthony, D.; Greenwald, J.L.; Sanchez, G.M.; Johnson, A.E.; Forsythe, S.R.; O’Donnell, J.K.; Paasche-Orlow, M.K.; Manasseh, C.; et al. A reengineered hospital discharge program to decrease rehospitalization: A randomized trial. Ann. Intern. Med. 2009, 150, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Nazar, H.; Nazar, Z.; Portlock, J.; Todd, A.; Slight, S.P. A systematic review of the role of community pharmacies in improving the transition from secondary to primary care. Br. J. Clin. Pharmacol. 2015, 80, 936–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.; Schifano, F.; Robinson, P.; Phillips, G.; Doherty, L.; Melnick, P.; Laming, L.; Sinclair, A.; Dhillon, S. Impact of community pharmacy diabetes monitoring and education programme on diabetes management: A randomized controlled study. Diabet. Med. 2012, 29, e326–e333. [Google Scholar] [CrossRef] [PubMed]
- Krass, I.; Armour, C.L.; Mitchell, B.; Brillant, M.; Dienaar, R.; Hughes, J.; Lau, P.; Peterson, G.; Stewart, K.; Taylor, S.; et al. The Pharmacy diabetes care program: Assessment of a community pharmacy diabetes service model in Australia. Diabet. Med. 2007, 24, 677–683. [Google Scholar] [CrossRef]
- Al Hamarneh, Y.N.; Charrois, T.; Lewanczuk, R.; Tsuyuki, R.T. Pharmacist intervention for glycaemic control in the community (the RxING study). BMJ Open 2013, 3, e003154. [Google Scholar] [CrossRef] [Green Version]
- Kallio, S.E.; Kiiski, A.; Airaksinen, M.S.A.; Mäntylä, A.T.; Kumpusalo-Vauhkonen, A.E.J.; Järvensivu, T.P.; Pohjanoksa-Mäntylä, M.K. Community pharmacists’ contribution to medication reviews for older adults: A systematic review. J. Am. Geriatr. Soc. 2018, 66, 1613–1620. [Google Scholar] [CrossRef]
- Jokanovic, N.; Tan, E.C.; Sudhakaran, S.; Kirkpatrick, C.M.; Dooley, M.J.; Ryan-Atwood, T.E.; Bell, J.S. Pharmacist-led medication review in community settings: An overview of systematic reviews. Res. Soc. Adm. Pharm. 2017, 13, 661–685. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before October 2016 | Since October 2016 Policy Change |
|---|---|
| Patient Assessment Summary with Pharmacist’s Signature and Date |
|
Specific to MCH
Specific to MCLTC
|
| Service | PIN | Fee |
|---|---|---|
| MedsCheck (MC) 1 | ||
| MC annual | 93899979 | $60 1 |
| MC follow-up | ||
| • Hospital discharge ≤ 2 weeks | 93899981 | |
| • Pharmacist decision | 93899982 | $25 |
| • Physician or nurse practitioner referral | 93899983 | |
| • Planned hospital admission | 93899984 | |
| MedsCheck Diabetes (MCD) 2 | ||
| MCD annual | 93899988 | $75 |
| MCD follow-up | 93899989 | $25 |
| MedsCheck at Home (MCH) 3 | ||
| MCH annual | 93899987 | $150 |
| MedsCheck Long Term Care (MCLTC) 4 | ||
| MCLTC annual | 93899985 | $90 |
| MCLTC quarterly | 93899986 | $50 |
| Service Type | MedsCheck (Annual or Follow-Up) | MedsCheck Diabetes (Annual or Follow-Up) | MedsCheck at Home | MedsCheck Long Term Care (Annual or Quarterly) |
|---|---|---|---|---|
| Number of recipients | 647,740 | 209,060 | 57,583 | 95,191 |
| Number of Service claims | 2,952,434 | 848,911 | 103,591 | 1,084,410 |
| Age, mean (SD) | 58.3 (17.3) | 60.6 (14.2) | 74.4 (16.4) | 82.6 (10.5) |
| Women, % | 52.4 | 45.2 | 62.1 | 64.0 |
| MedsCheck | MedsCheck Diabetes | MedsCheck at Home | MedsCheck Long Term Care | ||||
|---|---|---|---|---|---|---|---|
| Parameter | Annual | Follow-Up | Annual | Follow-Up | Annual | Quarterly | |
| Total Claims | 2,356,615 | 595,819 | 664,483 | 184,428 | 103,591 | 285,403 | 799,007 |
| Monthly Claims | |||||||
| • Minimum number | 22,973 | 5768 | 4314 | 896 | 1151 | 4493 | 14,000 |
| • Maximum number | 70,554 | 21,353 | 23,443 | 8304 | 3482 | 7074 | 18,687 |
| Results of Segmented Regression Models | |||||||
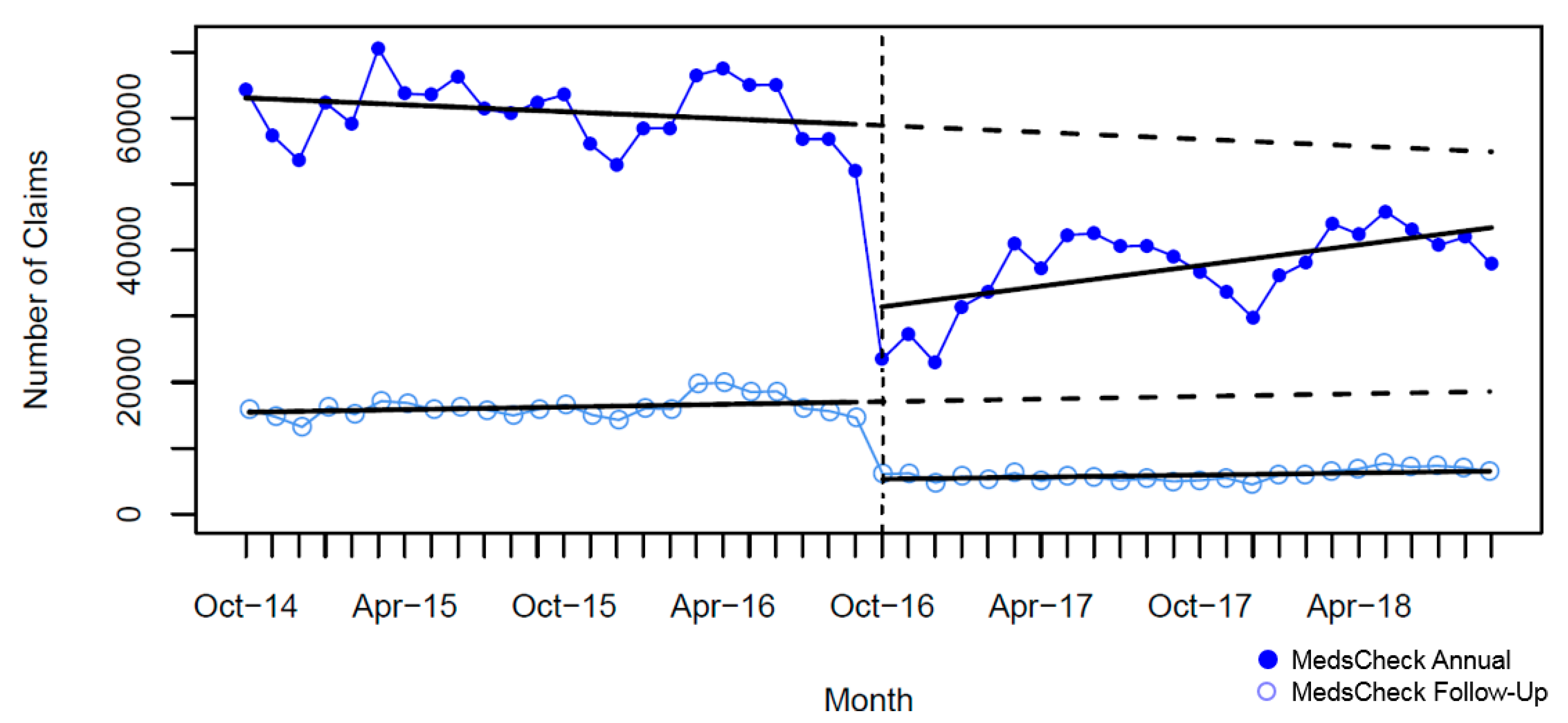
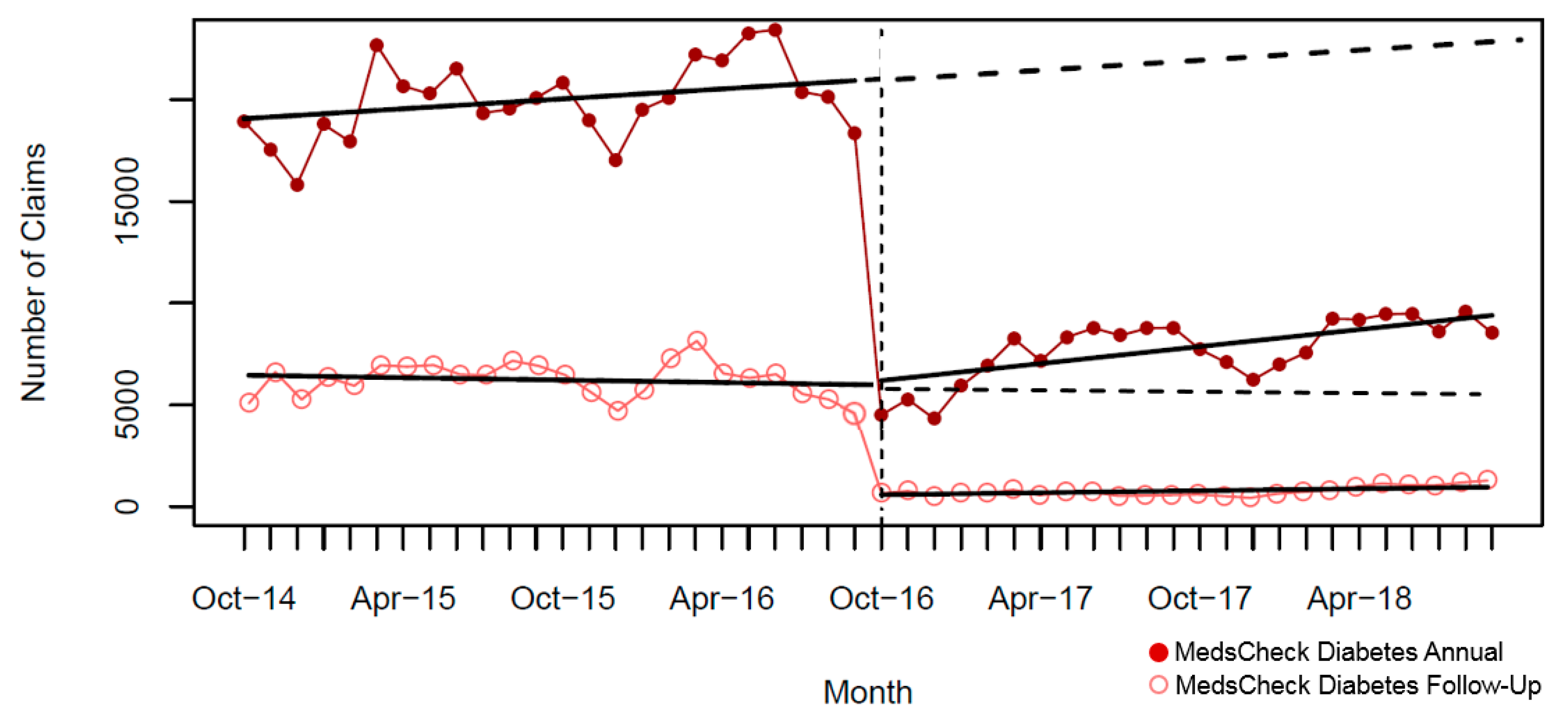
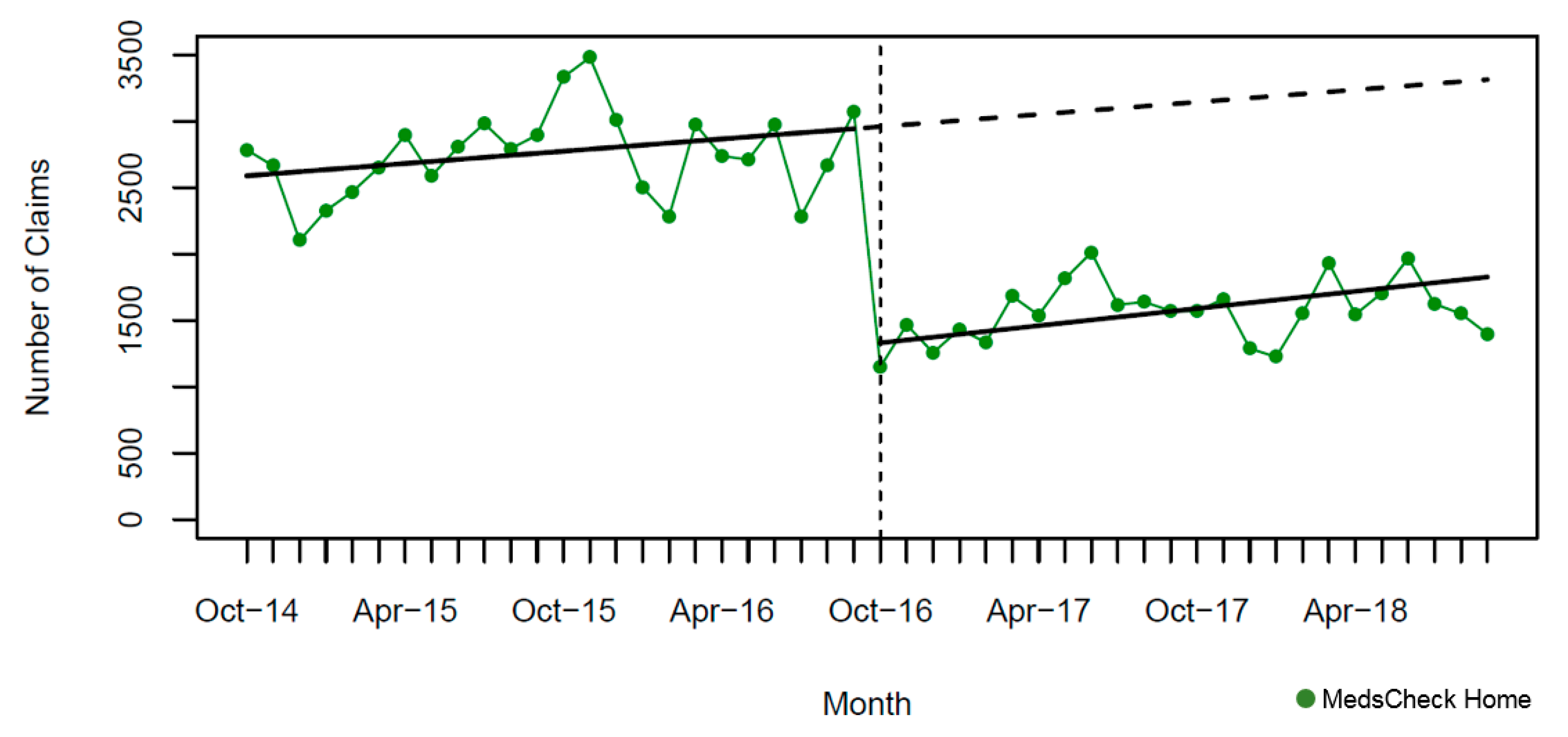
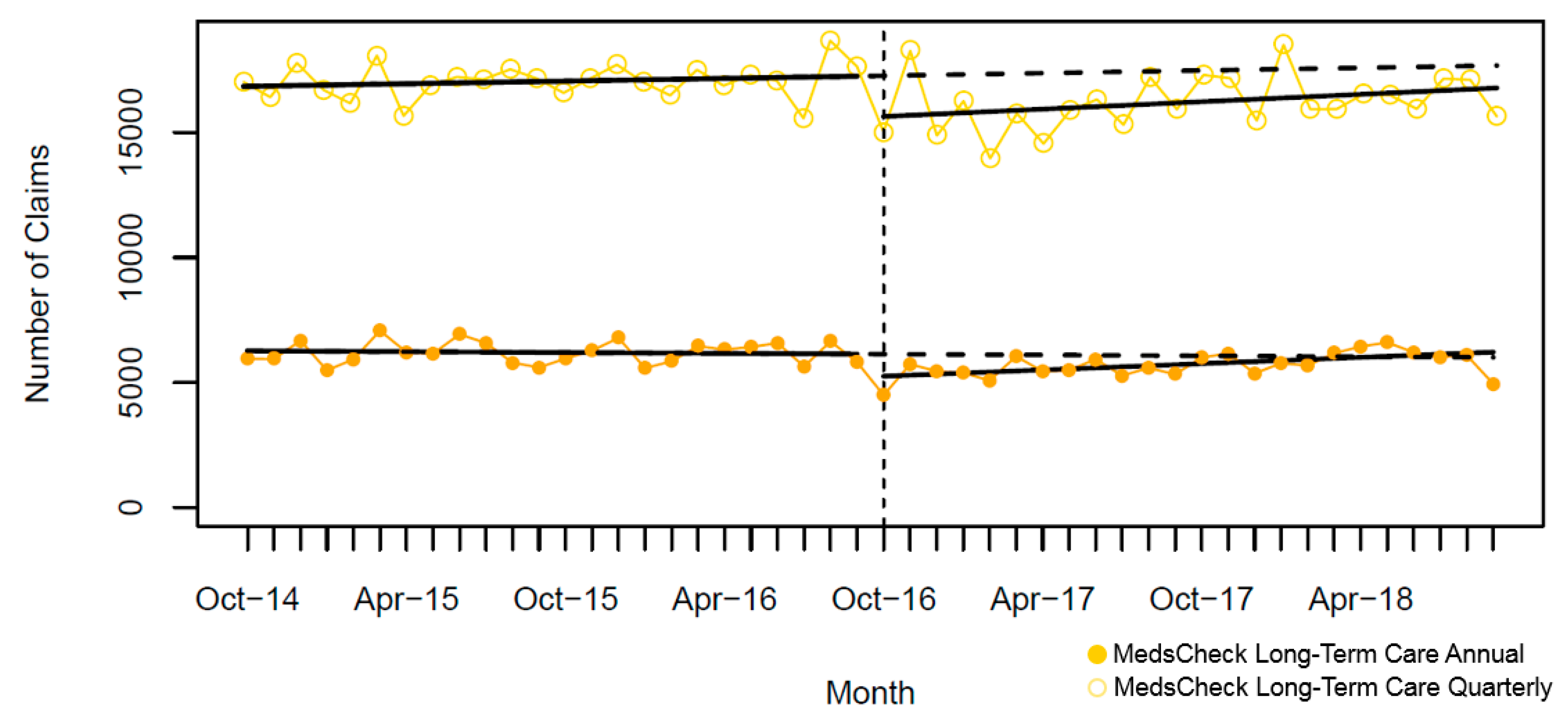
| Baseline (October 2014), number (95% CI) | 63,223 (60,452, 65,994) | 16,698 (15,826, 17,771) | 18,984 (18,069, 19,899) | 6704 (6157, 7251) | 2575 (2454, 2697) | 6274 (6199, 6349) | 16,848 (16,355, 17,341) |
| Pre-intervention slope, mean monthly claims (95%CI) | −173 (−373, 27) | 67 (−1, 135) | 81 (14, 149) | −19 (−57, 19) | 15 (6, 24) | −6 (−11, −0.3) | 18 (−17, 52) |
| Level Change at Intervention (October 2016) | |||||||
| • Number of claims (95% CI) | −28,167 (−32,034, −24,302) | −11,854 (−13,205, −10,503) | −14,876 (−16,244, −13,508) | −5214 (−5942, −4487) | −1635 (−1828, −1442) | −929 (−1034, −825) | −1656 (−2348, −965) |
| • Relative percent change (95% CI) | −46.7 (−52.9, −40.4) | −64.3 (−71.1, −57.3) | −70.5 (−76.7, −64.3) | −83.2 (−94.3, −72.1) | −55.0 (−61.2, −48.8) | −14.4 (−16.0, −12.8) | −9.4 (−13.2, −5.6) |
| Post-intervention slope, mean monthly claims (95% CI) | 521 (42, 1002) | 52 (−110, 215) | 139 (−17, 296) | 16 (−77, 108) | 22 (4, 40) | 42 (30, 54) | 50 (-33, 132) |
| Relative difference to forecast (September 2018), proportion (95% CI) | −21.0 (−27.7, −14.3) | −61.0 (−67.3, −54.5) | −58.9 (−64.6, −53.2) | −75.8 (−87.7, −63.8) | −44.9 (−50.4, −39.3) | 3.5 (1.8, 5.1) | −5.1 (−8.8, −1.3) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shakeri, A.; Dolovich, L.; MacCallum, L.; Gamble, J.-M.; Zhou, L.; Cadarette, S.M. Impact of the 2016 Policy Change on the Delivery of MedsCheck Services in Ontario: An Interrupted Time-Series Analysis. Pharmacy 2019, 7, 115. https://doi.org/10.3390/pharmacy7030115
Shakeri A, Dolovich L, MacCallum L, Gamble J-M, Zhou L, Cadarette SM. Impact of the 2016 Policy Change on the Delivery of MedsCheck Services in Ontario: An Interrupted Time-Series Analysis. Pharmacy. 2019; 7(3):115. https://doi.org/10.3390/pharmacy7030115
Chicago/Turabian StyleShakeri, Ahmad, Lisa Dolovich, Lori MacCallum, John-Michael Gamble, Limei Zhou, and Suzanne M. Cadarette. 2019. "Impact of the 2016 Policy Change on the Delivery of MedsCheck Services in Ontario: An Interrupted Time-Series Analysis" Pharmacy 7, no. 3: 115. https://doi.org/10.3390/pharmacy7030115
APA StyleShakeri, A., Dolovich, L., MacCallum, L., Gamble, J. -M., Zhou, L., & Cadarette, S. M. (2019). Impact of the 2016 Policy Change on the Delivery of MedsCheck Services in Ontario: An Interrupted Time-Series Analysis. Pharmacy, 7(3), 115. https://doi.org/10.3390/pharmacy7030115