PRN Medicines Management for Psychotropic Medicines in Long-Term Care Settings: A Systematic Review





Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Search Strategy and Data Collection
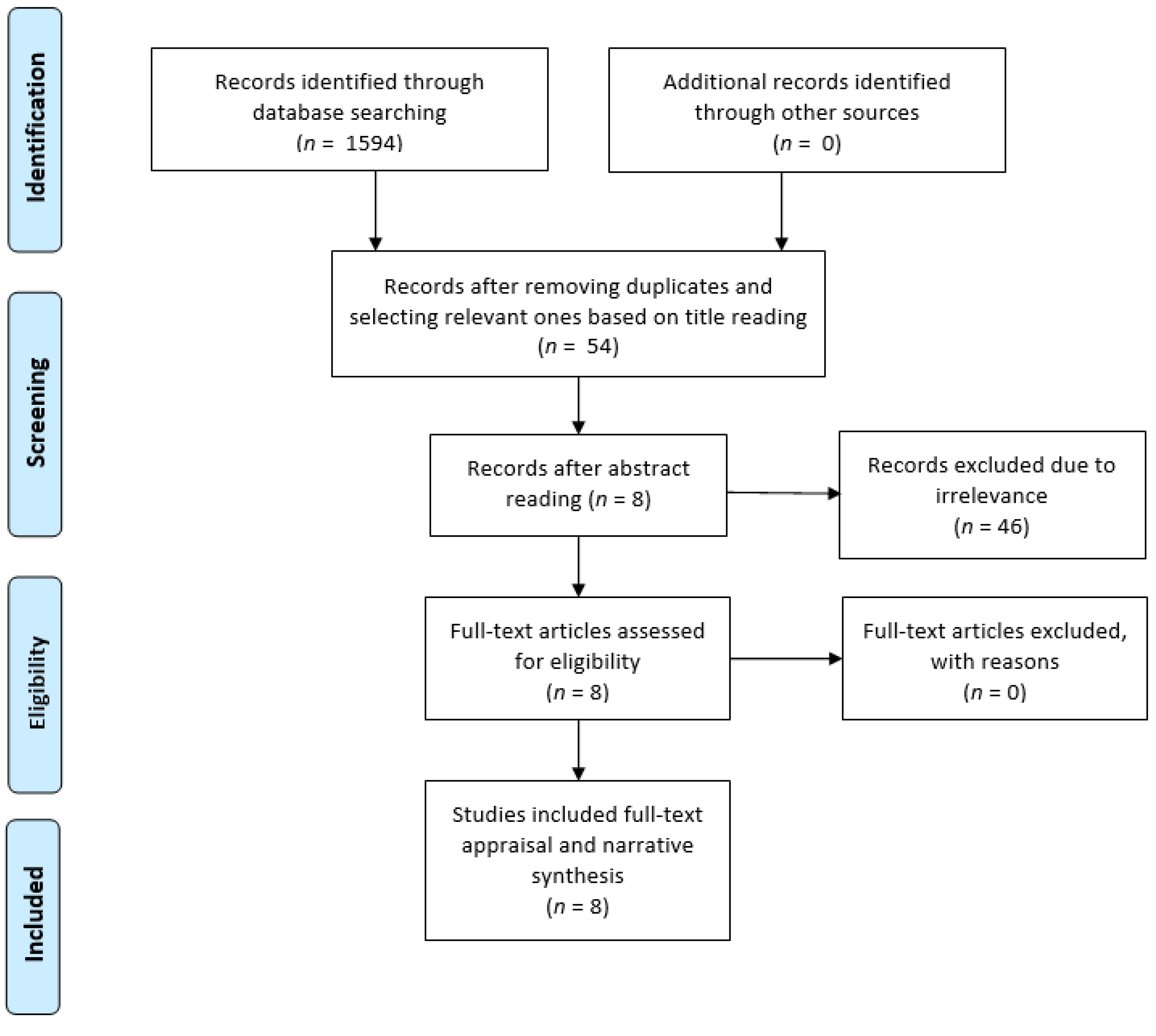
2.3. Systematic Review and Quality Appraisal
3. Results
3.1. Description of the Selected Studies
3.2. Prevalence and Type of PRN Prescription and Administration
3.3. Factors Affecting PRN Medicines Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vaismoradi, M.; Amaniyan, S.; Jordan, S. Patient Safety and Pro Re Nata Prescription and Administration: A Systematic Review. Pharmacy 2018, 6, 95. [Google Scholar] [CrossRef]
- Baumann, S.L.; Greif, N. The use of PRNs medications with hospitalized older adults. Geriatr. Nurs. 2017, 38, 596–598. [Google Scholar] [CrossRef]
- Cleary, M.; Horsfall, J.; Jackson, D.; O’Hara-Aarons, M.; Hunt, G.E.; O’Hara-Aarons, M. Patients’ views and experiences of pro re nata medication in acute mental health settings. Int. J. Ment. Health Nurs. 2012, 21, 533–539. [Google Scholar] [CrossRef]
- Jimu, M.; Doyle, L. The Administration of Pro re nata Medication by Mental Health Nurses: A Thematic Analysis. Issues Ment. Health Nurs. 2019, 40, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.; Arora, V.; Fischler, I.; Tremblay, R. Analysis of non-pharmacological interventions attempted prior to pro re nata medication use. Int. J. Ment. Health Nurs. 2018, 27, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Woo, J.E.; Lee, D.W.; Choi, W.C.; Yoon, J.L.; Kim, M.Y. Pro Re Nata Prescription and Perception Difference between Doctors and Nurses. Korean J. Fam. Med. 2014, 35, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Usher, K.; Lindsay, D.; Sellen, J. Mental health nurses’ PRN psychotropic medication administration practices. J. Psychiatr. Ment. Health Nurs. 2001, 8, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.; Arora, V.; Fischler, I.; Tremblay, R. Descriptive analysis of pro re nata medication use at a Canadian psychiatric hospital. Int. J. Ment. Health Nurs. 2017, 26, 402–408. [Google Scholar] [CrossRef]
- Douglas-Hall, P.; Whicher, E.V. ‘As required’ medication regimens for seriously mentally ill people in hospital. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Tong, Y.; Chen, J.; Chai, L.; Yang, L.; Zhang, C.; Liu, M. Current State of Pain Resource Nurse (PRN) Programs and Experiences of PRNs in China. Pain Manag. Nurs. 2019, 20, 174–182. [Google Scholar] [CrossRef]
- Lichtner, V.; Dowding, D.; Allcock, N.; Keady, J.; Sampson, E.L.; Briggs, M.; Corbett, A.; James, K.; Lasrado, R.; Swarbrick, C.; et al. The assessment and management of pain in patients with dementia in hospital settings: A multi-case exploratory study from a decision making perspective. BMC Health Serv. Res. 2016, 16, 427. [Google Scholar] [CrossRef]
- Stasinopoulos, J.; Bell, J.S.; Ryan-Atwood, T.E.; Tan, E.C.; Ilomäki, J.; Cooper, T.; Robson, L.; Sluggett, J.K. Frequency of and factors related to pro re nata (PRN) medication use in aged care services. Res. Soc. Adm. Pharm. 2018, 14, 964–967. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Patient Safety Curriculum Guide. Available online: https://www.who.int/patientsafety/education/mp_curriculum_guide/en/ (accessed on 26 October 2019).
- Dwyer, L.L.; Lau, D.T.; Shega, J.W. Medications That Older Adults in Hospice Care in the United States Take, 2007. J. Am. Geriatr. Soc. 2015, 63, 2282–2289. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.; Russ, M.J. Discontinuing the Use of PRN Intramuscular Medication for Agitation in an Acute Psychiatric Hospital. Psychiatr. Q. 2016, 87, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.; Ham, E.; Hilton, N.Z.; Hilton, Z. Documentation of psychotropic pro re nata medication administration: An evaluation of electronic health records compared with paper charts and verbal reports. J. Clin. Nurs. 2018, 27, 3171–3178. [Google Scholar] [CrossRef] [PubMed]
- McGrattan, M.; Ryan, C.; Barry, H.E.; Hughes, C.M. Interventions to Improve Medicines Management for People with Dementia: A Systematic Review. Drugs Aging 2017, 34, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Schmedt, N.; Jobski, K.; Kollhorst, B.; Krappweis, J.; Rüther, E.; Schink, T.; Garbe, E. Treatment patterns and characteristics of older antipsychotic users in Germany. Int. Clin. Psychopharmacol. 2016, 31, 159–169. [Google Scholar] [CrossRef]
- Hunnicutt, J.N.; Tjia, J.; Lapane, K.L. Hospice Use and Pain Management in Elderly Nursing Home Residents with Cancer. J. Pain Symptom Manag. 2017, 53, 561–570. [Google Scholar] [CrossRef]
- Lukas, A.; Mayer, B.; Fialová, D.; Topinkova, E.; Gindin, J.; Onder, G.; Bernabei, R.; Nikolaus, T.; Denkinger, M.D. Treatment of Pain in European Nursing Homes: Results from the Services and Health for Elderly in Long TERm Care (SHELTER) Study. J. Am. Med. Dir. Assoc. 2013, 14, 821–831. [Google Scholar] [CrossRef]
- Pokela, N.; Bell, J.S.; Lihavainen, K.; Sulkava, R.; Hartikainen, S.; Turunen, K. Analgesic use among community-dwelling people aged 75 years and older: A population-based interview study. Am. J. Geriatr. Pharmacother. 2010, 8, 233–244. [Google Scholar] [CrossRef]
- Browne, C.; Kingston, C.; Keane, C. Falls prevention focused medication review by a pharmacist in an acute hospital: Implications for future practice. Int. J. Clin. Pharm. 2014, 36, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.A.; Van Jaarsveld, H.J.; Houterman, S.; Van Der Stegen, J.C.; Wasylewicz, A.T.; Grouls, R.J.; Van Der Linden, C.M. Psychotropic Drug Prescription and the Risk of Falls in Nursing Home Residents. J. Am. Med. Dir. Assoc. 2016, 17, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Nyborg, G.; Brekke, M.; Straand, J.; Gjelstad, S.; Romøren, M. Potentially inappropriate medication use in nursing homes: An observational study using the NORGEP-NH criteria. BMC Geriatr. 2017, 17, 220. [Google Scholar] [CrossRef] [PubMed]
- Dörks, M.; Allers, K.; Hoffmann, F. Pro Re Nata Drug Use in Nursing Home Residents: A Systematic Review. J. Am. Med. Dir. Assoc. 2019, 20, 287–293. [Google Scholar] [CrossRef]
- Stokes, J.A.; Purdie, D.M.; Roberts, M.S. Factors influencing PRN medication use in nursing homes. Pharm. World Sci. 2004, 26, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Parsons, C.; Johnston, S.; Mathie, E.; Baron, N.; Machen, I.; Amador, S.; Goodman, C. Potentially inappropriate prescribing in older people with dementia in care homes: A retrospective analysis. Drugs Aging 2012, 29, 143–155. [Google Scholar] [CrossRef]
- Moermans, V.R.; Bleijlevens, M.H.; Verbeek, H.; Tan, F.E.; Milisen, K.; Hamers, J.P. The use of involuntary treatment among older adults with cognitive impairment receiving nursing care at home: A cross-sectional study. Int. J. Nurs. Stud. 2018, 88, 135–142. [Google Scholar] [CrossRef]
- Lindsey, P.L.; Buckwalter, K.C. Administration of PRN medications and use of nonpharmacologic interventions in acute geropsychiatric settings: Implications for practice. J. Am. Psychiatr. Nurses Assoc. 2012, 18, 82–90. [Google Scholar] [CrossRef]
- Pit, S.; Byles, J. Older Australians’ medication use: Self-report by phone showed good agreement and accuracy compared with home visit. J. Clin. Epidemiol. 2010, 63, 428–434. [Google Scholar] [CrossRef]
- Evans, D. Systematic reviews of nursing research. Intensiv. Crit. Care Nurs. 2001, 17, 51–57. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1; John Wiley & Sons: Chichester, UK, 2011; Available online: http://handbook-5-1.cochrane.org/ (accessed on 28 August 2019).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, J.; Harden, A.; Oakley, A.; Oliver, S.; Sutcliffe, K.; Rees, R.; Brunton, G.; Kavanagh, J. Integrating qualitative research with trials in systematic reviews. BMJ 2004, 328, 1010–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enhancing the QUAlity and Transparency of Health Research (EQUATOR). Available online: http://www.equator-network.org/ (accessed on 28 August 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Snowdon, J.; Galanos, D.; Vaswani, D. Patterns of psychotropic medication use in nursing homes: Surveys in Sydney, allowing comparisons over time and between countries. Int. Psychogeriatr. 2011, 23, 1520–1525. [Google Scholar] [CrossRef]
- Carder, P.C. “Learning about your residents”: How assisted living residence medication aides decide to administer pro re nata medications to persons with dementia. Gerontologist 2012, 52, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Rønningen, S.W.; Bakken, K.; Granås, A.G. Medication needs in nursing homes: Prescribing, use and documentation of effect. Sykepl. Forsk. 2013, 8, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Voyer, P.; McCusker, J.; Cole, M.G.; Monette, J.; Champoux, N.; Ciampi, A.; Belzile, E.; Richard, H. Behavioral and psychological symptoms of dementia: How long does every behavior last, and are particular behaviors associated with PRN antipsychotic agent use? J. Gerontol. Nurs. 2015, 41, 22–37. [Google Scholar] [CrossRef] [Green Version]
- Dörks, M.; Schmiemann, G.; Hoffmann, F. Pro re nata (as needed) medication in nursing homes: The longer you stay, the more you get? Eur. J. Clin. Pharmacol. 2016, 72, 995–1001. [Google Scholar] [CrossRef]
- Allers, K.; Dorks, M.; Schmiemann, G.; Hoffmann, F. Antipsychotic drug use in nursing home residents with and without dementia: Keep an eye on the pro re nata medication. Int. Clin. Psychopharmacol. 2017, 32, 213–218. [Google Scholar] [CrossRef]
- Westbury, J.L.; Gee, P.; Ling, T.; Brown, D.T.; Franks, K.H.; Bindoff, I.; Bindoff, A.; Peterson, G.M. RedUSe: Reducing antipsychotic and benzodiazepine prescribing in residential aged care facilities. Med. J. Aust. 2018, 208, 398–403. [Google Scholar] [CrossRef]
- Westbury, J.; Gee, P.; Ling, T.; Kitsos, A.; Peterson, G. More action needed: Psychotropic prescribing in Australian residential aged care. Aust. N. Z. J. Psychiatry 2019, 53, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Fog, A.F.; Kvalvaag, G.; Engedal, K.; Straand, J. Drug-related problems and changes in drug utilization after medication reviews in nursing homes in Oslo, Norway. Scand. J. Prim. Health Care 2017, 35, 329–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Mahony, D.; Gallagher, P.F. Inappropriate prescribing in the older population: Need for new criteria. Age Ageing 2008, 37, 138–141. [Google Scholar] [CrossRef] [Green Version]
- Jordan, S.; Banner, T.; Gabe-Walters, M.; Mikhail, J.M.; Panes, G.; Round, J.; Snelgrove, S.; Storey, M.; Hughes, D. Nurse-led medicines’ monitoring in care homes, implementing the Adverse Drug Reaction (ADRe) Profile improvement initiative for mental health medicines: An observational and interview study. PLoS ONE 2019, 14, e0220885. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Logan, P.A.; Panes, G.; Vaismoradi, M.; Hughes, D. Adverse Drug Reactions, Power, Harm Reduction, Regulation and the ADRe Profiles. Pharmacy 2018, 6, 102. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, P.; Ryan, C.; Byrne, S.; Kennedy, J.; O’Mahony, D. STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int. J. Clin. Pharmacol. Ther. 2008, 46, 72–83. [Google Scholar] [CrossRef]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Rognstad, S.; Brekke, M.; Fetveit, A.; Spigset, O.; Wyller, T.B.; Straand, J. The Norwegian General Practice (NORGEP) criteria for assessing potentially inappropriate prescriptions to elderly patients. Scand. J. Prim. Health Care 2009, 27, 153–159. [Google Scholar] [CrossRef]
- Harper, L.; Reddon, J.R.; Hunt, C.J.; Royan, H. PRN Medication Administration in a Geriatric Psychiatric Hospital: Chart Review and Nursing Perspective. Clin. Gerontol. 2017, 40, 392–400. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Essential Medicines and Health Products: Medicines Policy. Available online: https://www.who.int/medicines/areas/policy/en/ (accessed on 6 September 2019).
- Helvik, A.-S.; Benth, J.Š.; Wu, B.; Engedal, K.; Selbæk, G. Persistent use of psychotropic drugs in nursing home residents in Norway. BMC Geriatr. 2017, 17, 52. [Google Scholar] [CrossRef] [Green Version]
- Sasegbon, H.; Ismail, I.; Pushpanathan, M.; Haw, C. PRN medication: Beliefs and practices of psychiatrists and nurses working in PICUs and secure units. J. Psychiatr. Intensiv. Care 2015, 11, 1–10. [Google Scholar]
- Brooker, J.E.; Webber, L.; Julian, J.; Shawyer, F.; Graham, A.L.; Chan, J.; Meadows, G. Mindfulness-based Training Shows Promise in Assisting Staff to Reduce Their Use of Restrictive Interventions in Residential Services. Mindfulness 2014, 5, 598–603. [Google Scholar] [CrossRef]
- Nelson, R.; Coyle, C. Using Massage to Reduce Use of Sedative-Hypnotic Drugs with Older Adults: A Brief Report from a Pilot Study. J. Appl. Gerontol. 2010, 29, 129–139. [Google Scholar] [CrossRef]
- Abrahamson, K.; Nazir, A.; Pressler, K. A novel approach to deprescribing in long-term care settings: The SMART campaign. Res. Soc. Adm. Pharm. 2017, 13, 1202–1203. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Ilomäki, J.; Seaman, K.L.; Corlis, M.; Bell, J.S. Medication management policy, practice and research in Australian residential aged care: Current and future directions. Pharmacol. Res. 2017, 116, 20–28. [Google Scholar] [CrossRef]
- Barr, L.; Wynaden, D.; Heslop, K. Nurses’ attitudes towards the use of PRN psychotropic medications in acute and forensic mental health settings. Int. J. Ment. Health Nurs. 2018, 27, 168–177. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.S.; Ahonen, J.; Lavikainen, P.; Hartikainen, S. Potentially inappropriate drug use among older persons in Finland: Application of a new national categorization. Eur. J. Clin. Pharmacol. 2013, 69, 657–664. [Google Scholar] [CrossRef]
- Jordan, S.; Coleman, M.; Hardy, B.; Hughes, D. Assessing educational effectiveness: The impact of a specialist course on the delivery of care. J. Adv. Nurs. 1999, 30, 796–807. [Google Scholar] [CrossRef]
- Jordan, S.; Tunnicliffe, C.; Sykes, A. Minimizing side-effects: The clinical impact of nurse-administered ‘side-effect’ checklists. J. Adv. Nurs. 2002, 37, 155–165. [Google Scholar] [CrossRef]


{kind=link}
| Database | Total in Each Database | Title Selection | Abstract Selection | Full-Text Appraisal |
|---|---|---|---|---|
| PubMed (including Medline) | 618 | 4 | 2 | 2 |
| Scopus | 105 | 29 | 5 | 5 |
| Cochrane library | 326 | 1 | 0 | 0 |
| Cinahl | 142 | 5 | 0 | 0 |
| Norart (Nordic) | 2 | 2 | 1 | 1 |
| SweMed+ (Nordic) | 3 | 2 | 0 | 0 |
| IBECS (Spanish) | 5 | 0 | 0 | 0 |
| Cuiden (Spanish) | 194 | 2 | 0 | 0 |
| Medes (Spanish) | 199 | 9 | 0 | 0 |
| Manual search/backtracking references | 0 | 0 | 0 | 0 |
| Total | 1594 | 54 | 8 | 8 |
| Authors/Year | Country | Objective(s) | Method | Focus of Data Collection | Setting and Sample | Demographic Data |
|---|---|---|---|---|---|---|
| Snowdon et al. 2011 [37] | Australia | To understand and compare the patterns of psychotropic medications use in nursing homes. | A cross-sectional survey | Comparison of the patterns of psychotropic medication, using data from surveys from 1993, 1998, 2003, and 2009. Details of current prescription of medications during the last 14 days or since initiation of regular or PRN medication were recorded. Surveys reported the rate of PRN prescription and administration in the last 28 days. The administration of PRN medications at least 25 out of 28 days was considered regular medication use. | Number of nursing homes and percentage of their participation in the study were as follows: 46 (98%), 38 (97%), 51 (100%), and 44 (92%), in years 1993, 1998, 2003, and 2009, respectively. | Mean number of residents: 52.5, 52.0, 60.6, and 56.0, respectively. Percentages of 36% (n = 895, mean 78.7 years, SD = 12.1) and 64% (n = 1570, mean 84.2 years, SD = 9.6) were male and female, respectively. No information of their diagnosis was available. |
| Carder, 2012 [38] | USA | To identify if staff who were not registered nurses administered PRN medications to residents with dementia. | The qualitative analysis of interviews and medication record reviews | How is a decision on administering PRN medications to residents with dementia made? PRN administration staff were observed for 6 consecutive days, 16 h per day, including 72 scheduled medication rounds. Sixteen interviews were completed. | Sixteen unlicensed staff members supervised by registered nurses working at three assisted living settings with all 47 residents in urban and suburban areas. | Residents were mostly female. The mean age of staff was 38 years (SD = 8.3 years) and were mainly female (75%). Their job experience ranged 4 months to 8 years. |
| Rønningen et al., 2013 [39] | Norway | To document prescribing and administration of PRN medication in one nursing home, and to investigate how often, and how, the positive and negative effects of prescribed PRN medication are documented. | A cross-sectional survey of documentation of PRN medications | PRN prescription and administration prevalence. Description of documentation of PRN medication effects (beneficial and harmful) were documented in terms of quantity and quality. | PRN medicines management was documented and described for 108 patients in one nursing home over 15 weeks. | Mean age of residents was 84.5 years (SD = 9.4 years). They were mostly female (60.2%). No data on staff were provided. |
| Voyer et al., 2015 [40] | Canada | To identify behavioural and psychological symptoms in dementia that were associated with PRN antipsychotic medicine prescription and administration. | A secondary analysis on a prospective, observational, multisite cohort | Association between behavioural and psychological symptoms of dementia with PRN antipsychotic medicine use. Medication records of regular and PRN use of medication were reviewed. Atypical antipsychotic agents (risperidone (Risperdal®), olanzapine (Zyprexa®), and quetiapine (Seroquel®), and typical antipsychotic agents (haloperidol (Haldol®) were used. Prescription and administration of PRN antipsychotic agents during 7 days before the monthly assessment of behavioural and psychological symptoms of dementia assessments were considered. | A total of 146 nursing home residents from 7 settings. Subjects aged ≥65 years were included. Those without dementia, cognitive impairment, or behavioural and psychological symptoms were excluded. | Participants had a mean age of 85.6 years (SD = 7 years) and were mostly female (58.9%). They mainly were diagnosed with dementia (89.7%). Of 129 nurses, 76.7% were registered nurses and 90.7% were female. Their experience in geriatric wards was mainly greater than 10 years (72%). |
| Dörks et al., 2016 [41] | Germany | To examine the characteristics and potential predictors of PRN prescription and administration in nursing homes. | A multicentre survey | Investigation of characteristics and potential predictors of PRN medicine prescription and administration in nursing homes. | A total of 852 residents in 21 nursing homes organised by different institutions. | Their mean age was 83.5 years (SD = 10.5) and 76.5% were female. Their mean length of stay was 3.2 years (SD = 3.4). |
| Allers et al., 2017 [42] | Germany | To compare the use of antipsychotic medications in residents with and without dementia. | A cross-sectional survey | Assessment of the prevalence of antipsychotic medicine use and exploration of factors affecting their prescription. While data on all prescribed medications were collected from the residents’ medication schedules, antipsychotics prescribed as scheduled medication and on a PRN basis were studied and prescriptions of scheduled and PRN medication were compared. | All residents (n = 852) from 21 nursing homes without any exclusion criteria. | A percentage of 57.7% of the residents were diagnosed with dementia and their mean age was higher than those without it (84.9 vs. 81.4 years, but no standard deviations were presented). About three quarters of the residents were female and those with dementia were more commonly severely care-dependent (32.8 vs. 16.4%). |
| Westbury et al., 2018 [43] | Australia | To study the impact of an interdisciplinary intervention on the prescription of antipsychotics and benzodiazepines in older people’s residential care facilities. | A longitudinal study with comparisons over time | Investigation of the impact of an educational consultation intervention on the use of antipsychotics and benzodiazepines over 6 months. It assessed the possibility of substitution of medications prescribed regularly. The multi-strategic programme comprised: auditing psychotropic medication, staff education, and case reviews by the physician, pharmacist, and nurse at the beginning of the programme and at 3 and 6 months. | A national-level sample consisting of 150 older people’s residential care facilities hosting 12,157 people. | The residents’ mean age was 85.8 years (SD = 8.6). |
| Westbury et al., 2019 [44] | Australia | To analyse the use of psychotropics in a national sample of residential aged care facilities. | A retrospective cohort | Analysis of psychotropic use in a large national sample of residential aged care facility residents, derived from a project to promote the appropriate use of antipsychotics and benzodiazepines. A multi-strategic interdisciplinary intervention was devised consisting of a 6-month programme with cycles of audits, education, and a review of sedatives. Prescribing data were extracted via a custom-made website. | A large national-level sample of 150 residential aged care facilities consisting of 11,368 residents | Data on psychotropic prescribing was collected from for 139 of 150 facilities with a response rate of 93%. Clinical, diagnostic, and demographic data were not reported. |
| Authors/Year | Prevalence of PRN Prescription | Prevalence of PRN Administration | Medicines Prescribed or Administered PRN |
|---|---|---|---|
| Snowdon et al., 2011 [37] | Mean number of 1.3 per resident Mean number of 0.9 when topical applications such as ear, eye, nose, and dermatological preparations were excluded (no measures of dispersion reported.) | Once or more in every 5 prescriptions | Clonazepam and midazolam for six residents and antipsychotic and/or anxiolytic medications including haloperidol to 3.3% of residents and Risperidone to 1%. Numerators and denominators were not reported. |
| Carder, 2012 [38] | Nearly all residents had a PRN order, with a range from 0 to 14 per resident, and with a mean of 5.82 (no measures of dispersion reported.) | No data | No data |
| Rønningen et al., 2013 [39] | 1.1% (n = 183) of prescriptions | 519 of the 839 (61.9%) | Psychotropic medications such as oxazepam, clomethiazole, diazepam, zopiclone, tramadol, morphine, and oxycodone were among the most frequently prescribed and administered medications as different brand names or pharmaceutical formulations (e.g., tablets and suppositories). Percentages, numerators, and denominators were not reported. |
| Voyer et al., 2015 [40] | 19.9% of prescriptions | No data | Antipsychotics including risperidone (37.9%), haloperidol (34.5%), quetiapine (10.3%), olanzapine (10.3%), haloperidol, and quetiapine (3.4%) were prescribed. After 5 months, olanzapine was replaced by risperidone (3.4%). Numerators and denominators were not reported. |
| Dörks et al., 2016 [41] | A total of 2117 (27.9 %) prescriptions were PRN. Additionally, 638 (74.9 %) received at least one PRN medication. Each resident was treated with a mean of 2.5 ± 2.3 PRN medications. | No data | Lorazepam was prescribed to 67 (7.9%) of residents with a mean duration of 579 ± 627 days. |
| Allers et al., 2017 [42] | A percentage of 35.9% of prescriptions to residents with dementia vs. 23.0% for those without dementia were PRN. | No data | 23.8% of residents with dementia and 5.7% without dementia were prescribed PRN antipsychotics. Only a small percentage of residents without dementia received PRN antipsychotics alone, without any scheduled antipsychotic medications (3.1%), a lower proportion than residents with dementia (10.8%). Residents with dementia were prescribed both scheduled and PRN antipsychotics more often than residents without dementia (13.0 vs. 2.5%). Of typical antipsychotics, melperone and promethazine were most often prescribed. Numerators and denominators were not reported. |
| Westbury et al., 2018 [43] | PRN antipsychotics were prescribed to 10.8% (9.5-12.1%) and benzodiazepines to 30.1% (27.6-32.6%) of residents. | No data | Antipsychotics, excluding lithium and prochlorperazine, and all types of benzodiazepines were converted to diazepam equivalents, but no separate data on each medication were provided. |
| Westbury et al., 2019 [44] | Of 11368 residents, 1261 (11.1%) and 3461 (30.5%) were prescribed PRN antipsychotics and PRN benzodiazepines, respectively. | No data | A percentage of 11.1% of residents were prescribed PRN atypical antipsychotics, including risperidone, quetiapine, and olanzapine, and typical antipsychotics such as haloperidol. Benzodiazepine, as an anxiolytic, prescribing included oxazepam, diazepam, and alprazolam to 17.9% of residents. Hypnotics, temazepam, and nitrazepam were prescribed to 16.4%. Both regular and PRN benzodiazepines were prescribed to 1150 residents (47%). Additionally, 724 (29%) of them with regular antipsychotic orders were prescribed extra doses of PRN. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaismoradi, M.; Vizcaya Moreno, F.; Sletvold, H.; Jordan, S. PRN Medicines Management for Psychotropic Medicines in Long-Term Care Settings: A Systematic Review. Pharmacy 2019, 7, 157. https://doi.org/10.3390/pharmacy7040157
Vaismoradi M, Vizcaya Moreno F, Sletvold H, Jordan S. PRN Medicines Management for Psychotropic Medicines in Long-Term Care Settings: A Systematic Review. Pharmacy. 2019; 7(4):157. https://doi.org/10.3390/pharmacy7040157
Chicago/Turabian StyleVaismoradi, Mojtaba, Flores Vizcaya Moreno, Hege Sletvold, and Sue Jordan. 2019. "PRN Medicines Management for Psychotropic Medicines in Long-Term Care Settings: A Systematic Review" Pharmacy 7, no. 4: 157. https://doi.org/10.3390/pharmacy7040157
APA StyleVaismoradi, M., Vizcaya Moreno, F., Sletvold, H., & Jordan, S. (2019). PRN Medicines Management for Psychotropic Medicines in Long-Term Care Settings: A Systematic Review. Pharmacy, 7(4), 157. https://doi.org/10.3390/pharmacy7040157