Impact of Up-Scheduling Medicines on Pharmacy Personnel, Using Codeine as an Example, with Possible Adaption to Complementary Medicines: A Scoping Review




Abstract
:1. Introduction
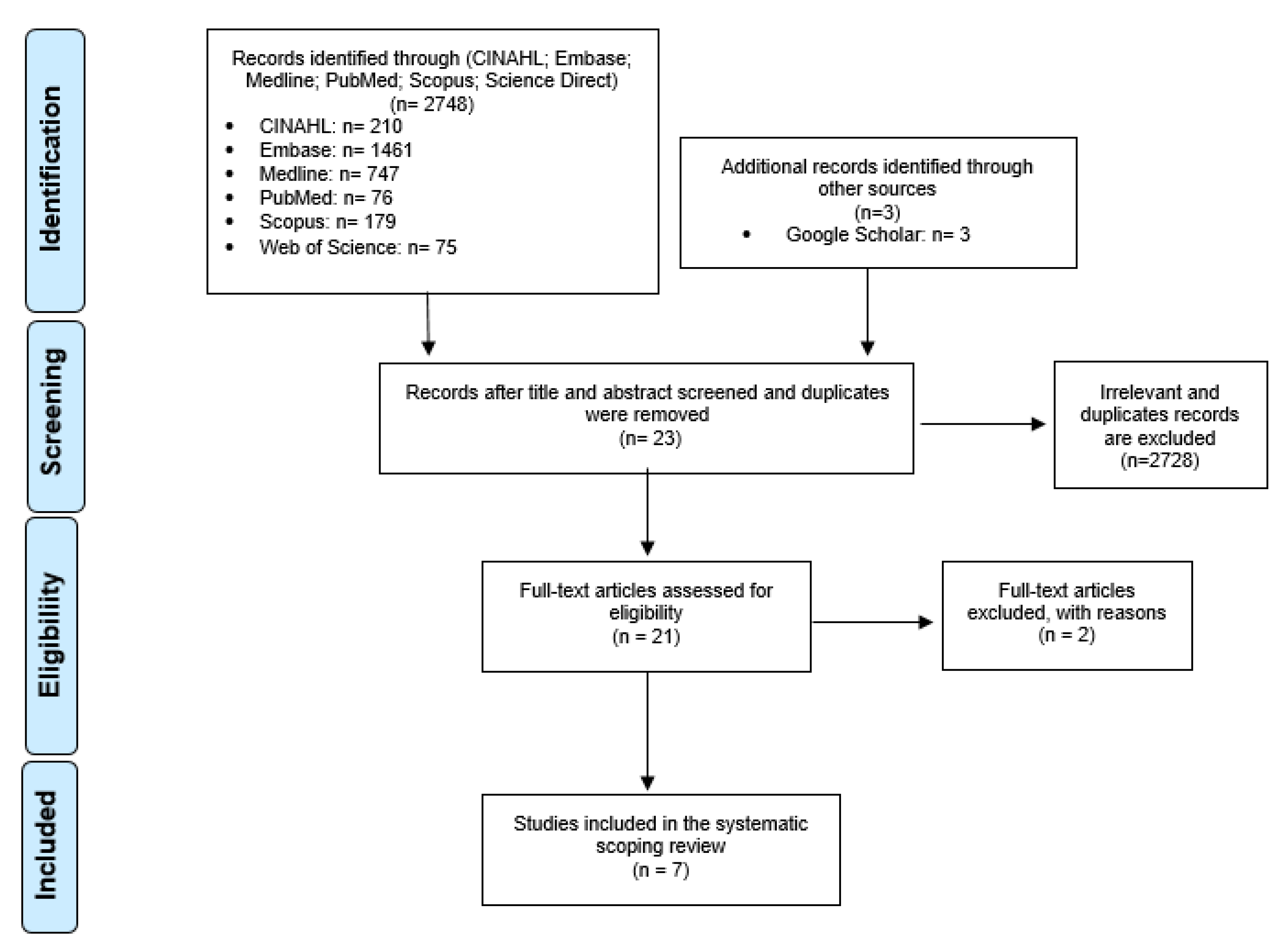
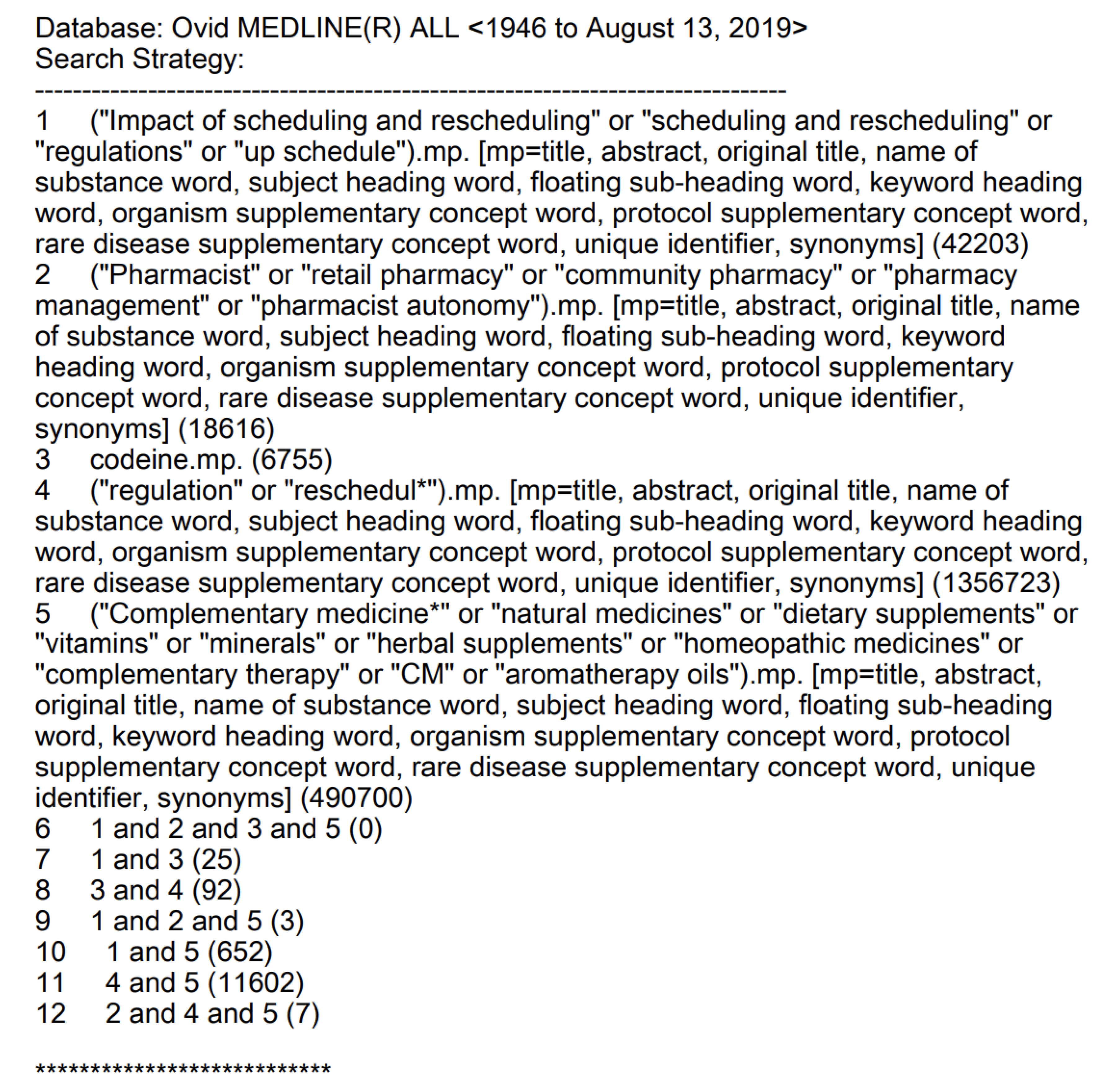
2. Methodology
- CMs: Complementary medicines, natural medicines, dietary supplements, vitamins, minerals, herbal supplements, homeopathic medicines, complementary therapy, CMs, and aromatherapy oils.
- Scheduling and rescheduling: regulations, up-schedule.
- Codeine.
- Pharmacist: Pharmacist, retail pharmacy, community pharmacy, pharmacy management and pharmacist autonomy.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A


References
- Therapeutic Goods Administration. Complementary Medicines; Therapeutic Goods Administration: Canberra, Australia, 2019. Available online: https://www.tga.gov.au/complementary-medicines (accessed on 2 March 2020).
- Xue, C.; Zhang, A.; Lin, V.; Da Costa, C.; Story, D. Complementary and alternative medicine use in Australia: A national population-based survey. J. Altern. Complement. Med. 2007, 13, 643–650. [Google Scholar] [CrossRef]
- Steel, A.; McIntyre, E.; Harnett, J.; Foley, H.; Adams, J.; Sibbritt, D.; Wardle, J.; Frawley, J. Complementary medicine use in the Australian population: Results of a nationally-representative cross-sectional survey. Sci. Rep. 2018, 8, 17325. [Google Scholar] [CrossRef] [Green Version]
- Cramer, H.; Shaw, A.; Wye, L.; Weiss, M. Over-the-counter advice seeking about complementary and alternative medicines (CAM) in community pharmacies and health shops: An ethnographic study. Health Soc. Care Community 2010, 18, 41–50. [Google Scholar] [CrossRef]
- Ung, C.O.L.; Harnett, J.; Hu, H. Community pharmacist’s responsibilities with regards to traditional medicine/complementary medicine products: A systematic literature review. Res. Soc. Adm. Pharm. 2017, 13, 686–716. [Google Scholar] [CrossRef]
- Pharmaceutical Society of Australia. Pharmacuetical Society of Australia Code of Ethics for Pharmacists; Pharmaceutical Society of Australia: Canberra, Australia, 2017; Available online: https://www.psa.org.au/membership/ethics/ (accessed on 13 April 2020).
- Soleymani, S.; Bahramsoltani, R.; Rahimi, R.; Abdollahi, M. Clinical risks of St John’s Wort (Hypericum perforatum) co-administration. Expert Opin. Drug Metab. Toxicol. 2017, 13, 1047–1062. [Google Scholar] [CrossRef]
- Chrubasik-Hausmann, S.; Vlachojannis, J.; McLachlan, A.J. Understanding drug interactions with St John’s wort (Hypericum perforatum L.): Impact of hyperforin content. J. Pharm. Pharmacol. 2019, 71, 129–138. [Google Scholar] [CrossRef] [Green Version]
- Hennessy, M.; Kelleher, D.; Spiers, J.; Barry, M.; Kavanagh, P.; Back, D.; Mulcahy, F.; Feely, J. St John’s wort increases expression of P-glycoprotein: Implications for drug interactions. Br. J. Clin. Pharmacol. 2002, 53, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Biffignandi, P.M.; Bilia, A.R. The growing knowledge of St. John’s wort (Hypericum perforatum L) drug interactions and their clinical significance. Curr. Ther. Res. 2000, 61, 389–394. [Google Scholar] [CrossRef]
- Ung, C.O.L.; Harnett, J.; Hu, H. Key stakeholder perspectives on the barriers and solutions to pharmacy practice towards complementary medicines: An Australian experience. BMC Complement. Altern. Med. 2017, 17, 394. [Google Scholar] [CrossRef] [Green Version]
- Pharmacy Board of Australia. Guidelines on Practice-Specific Issues; Australian Government Australia: Canberra, Australia, 2015. Available online: http//:www.pharmacyboard.gov.au (accessed on 13 April 2020).
- Emmerton, L. The ‘third class’ of medications: Sales and purchasing behavior are associated with pharmacist only and pharmacy medicine classifications in Australia. J. Am. Pharm. Assoc. 2009, 49, 31–37. [Google Scholar] [CrossRef]
- Cairns, R.; Brown, J.A.; Buckley, N.A. The impact of codeine re-scheduling on misuse: A retrospective review of calls to Australia’s largest poisons centre. Addiction 2016, 111, 1848–1853. [Google Scholar] [CrossRef]
- Harnett, J.E.; Ung, C.O.L.; Hu, H.; Sultani, M.; Desselle, S.P. Advancing the pharmacist’s role in promoting the appropriate and safe use of dietary supplements. Complement. Ther. Med. 2019, 44, 174–181. [Google Scholar] [CrossRef]
- Pharmaceutical Society of Australia. Complementary Medicines Position Statement. 2015. Available online: http://www.psa.org.au/downloads/ent/uploads/filebase/policies/position-statement-complementary-medicines.pdf (accessed on 13 April 2020).
- American Society of Health-System Pharmacists. Statement on the use of dietary supplements. Am. J. Health-SystPharm. 2004, 61, 1707–1711. [Google Scholar]
- The Australian Government Department of Education: The Australian Industry and Skills Committee. Community Pharmacy. The Australian Government. 2020. Available online: https://nationalindustryinsights.aisc.net.au/industries/retail-and-wholesale/community-pharmacy (accessed on 13 April 2020).
- The Australian Government Department of Health and Ageing Australia. Pharmacy Guild of Australia; Australian Government the Pharmacy Workforce Planning Study: Canberra Australia, 2020; Chapter 3, p. 14, Table 3.
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349. [Google Scholar] [CrossRef] [Green Version]
- Harnett, J.E.; McIntyre, E.; Steel, A.; Foley, H.; Sibbritt, D.; Adams, J. Use of complementary medicine products: A nationally representative cross-sectional survey of 2019 Australian adults. BMJ Open 2019, 9, 024198. [Google Scholar] [CrossRef] [Green Version]
- Carney, T.; Wells, J.; Bergin, M.; Dada, S.; Foley, M.; McGuiness, P.; Rapca, A.; Rich, E.; Van Hout, M.C. A Comparative exploration of community pharmacists’ views on the nature and management of over-the-counter (OTC) and prescription codeine misuse in three regulatory regimes: Ireland, South Africa and the United Kingdom. Int. J. Ment. Health Addict. 2016, 14, 351–369. [Google Scholar] [CrossRef]
- Kennedy, C.; Duggan, E.; Bennett, K.; Williams, D.J. Rates of reported codeine-related poisonings and codeine prescribing following new national guidance in Ireland. Pharmacoepidemiol. Drug Saf. 2019, 28, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Hamer, A.M.; Spark, M.J.; Wood, P.J.; Roberts, E. The upscheduling of combination analgesics containing codeine: The impact on the practice of pharmacists. Res. Soc. Adm. Pharm. 2014, 10, 669–678. [Google Scholar] [CrossRef]
- Mishriky, J.; Stupans, I.; Chan, V. Pharmacists’ views on the upscheduling of codeine-containing analgesics to ‘prescription only’medicines in Australia. Int. J. Clin. Pharm. 2019, 41, 538–545. [Google Scholar] [CrossRef]
- Izzo, A.A.; Hoon-Kim, S.; Radhakrishnan, R.; Williamson, E.M. A critical approach to evaluating clinical efficacy, adverse events and drug interactions of herbal remedies. Phytother. Res. 2016, 30, 691–700. [Google Scholar] [CrossRef]
- Posadzki, P.; Watson, L.; Ernst, E. Herb-drug interactions: An overview of systematic reviews. Br. J. Clin. Pharmacol. 2013, 75, 603–618. [Google Scholar] [CrossRef] [Green Version]
- De Souza Silva, J.E.; Souza, C.A.S.; da Silva, T.B.; Gomes, I.A.; de Carvalho Brito, G.; de Souza Araújo, A.A.; de Lyra-Júnior, D.P.; da Silva, W.B.; da Silva, F.A. Use of herbal medicines by elderly patients: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Tachjian, A.; Maria, V.; Jahangir, A. Use of herbal products and potential interactions in patients with cardiovascular diseases. J. Am. College Cardiol. 2010, 55, 515–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doucette, W.R.; Schommer, J.C. Pharmacy technicians’ willingness to perform emerging tasks in community practice. Pharmacy 2018, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Desselle, S.P.; Hoh, R.; Holmes, E.R.; Gill, A.; Zamora, L. Pharmacy technician self-efficacies: Insight to aid future education, staff development, and workforce planning. Res. Soc. Adm. Pharm. 2018, 14, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Ung, C.O.L.; Harnett, J.E.; Hu, H.; Desselle, S. Barriers to US pharmacists adopting professional responsibilities that support the appropriate and safe use of natural products by Americans—Key stakeholders perspectives. Am. J. Hosp. Pharm. 2019, 76, 980–990. [Google Scholar]

{kind=link}
{kind=link}
| Theme | Sub-themes | Key Findings | Reference | |
|---|---|---|---|---|
| 1 | Purpose | To address codeine misuse | ||
| 2 | Attitudes | 2.1 Positive | Pharmacists were proactive in prompting discussions with patients | [23] |
| Pharmacists recommended patients with appropriate medicines management | [23] | |||
| Less addiction and toxicity were reported due to restrictions | [24] | |||
| General Practitioners were in support of scheduling changes | [24] | |||
| Up scheduling positively impacted the practice of community pharmacists in Australia | [13] | |||
| Improvements to practice behaviors | [13] | |||
| 2.2 Negative | Did not solve misuse as patient shifted from “pharmacist-shopping” to “doctor-shopping” | [23] | ||
| Some pharmacists felt that it might have possibly lead to escalation of stronger medications | [23] | |||
| Limited pharmacists’ capacity in offering pain management | [23] | |||
| Some pharmacists viewed up scheduling of codeine as increasing GP’s burden | [23] | |||
| Opposition to the scheduling by pharmacists and users | ||||
| Had a negative impacts on consumers’ health, finances and pain management | ||||
| 3 | Potential impact on practice | 3.1 Treatment options | Concerns raised around treatment options and support for pain management after the restriction | [23] |
| Establishing therapeutic needs, inconsistent supplying issue between pharmacies and intervening with codeine-dependent individuals | [13] | |||
| 3.2 Challenges | Impact on business and environmental factors | [23] | ||
| 3.3 Funding models of payment | Implications to pharmacies income | [23] | ||
| 4 | Experiences of impact | 4.1 Positive | Resulted in a decrease in the reported poison cases involving non-prescription codeine products in 2011 | [24] |
| Pharmacists required to monitor supply and identify more cases of misuse | [25] | |||
| 4.2 Insignificant | Rate of codeine poisoning remained stable and at a lower level | [26] | ||
| 4.3 Negative | Had no impact on misuse; Possible reason to why Schedule 3 failed to make an impact: People misusing codeine did not necessarily fit the ‘addict’ stereotype | [14] | ||
| Pharmacists were not confident discussing possible codeine dependence with patients | [26] | |||
| 5 | Related issues | 5.1 Marketing and advertising | Misleading patients to think that codeine is an effective treatment for pain | [12] |
| 5.2 Compliance with legislation and professional guidelines | Greater staff involvement for scheduled medicines | [12] | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.A.; Harnett, J.E.; Ung, C.O.L.; Chaar, B. Impact of Up-Scheduling Medicines on Pharmacy Personnel, Using Codeine as an Example, with Possible Adaption to Complementary Medicines: A Scoping Review. Pharmacy 2020, 8, 65. https://doi.org/10.3390/pharmacy8020065
Lee KA, Harnett JE, Ung COL, Chaar B. Impact of Up-Scheduling Medicines on Pharmacy Personnel, Using Codeine as an Example, with Possible Adaption to Complementary Medicines: A Scoping Review. Pharmacy. 2020; 8(2):65. https://doi.org/10.3390/pharmacy8020065
Chicago/Turabian StyleLee, Kristenbella AYR, Joanna E. Harnett, Carolina Oi Lam Ung, and Betty Chaar. 2020. "Impact of Up-Scheduling Medicines on Pharmacy Personnel, Using Codeine as an Example, with Possible Adaption to Complementary Medicines: A Scoping Review" Pharmacy 8, no. 2: 65. https://doi.org/10.3390/pharmacy8020065
APA StyleLee, K. A., Harnett, J. E., Ung, C. O. L., & Chaar, B. (2020). Impact of Up-Scheduling Medicines on Pharmacy Personnel, Using Codeine as an Example, with Possible Adaption to Complementary Medicines: A Scoping Review. Pharmacy, 8(2), 65. https://doi.org/10.3390/pharmacy8020065