Knowledge and Attitudes of Student Pharmacists Regarding Polypharmacy and Deprescribing: A Cross-Sectional Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Development
2.3. Statistical Analysis
3. Results
3.1. Study Sample
3.2. Deprescribing in School of Pharmacy Curricula
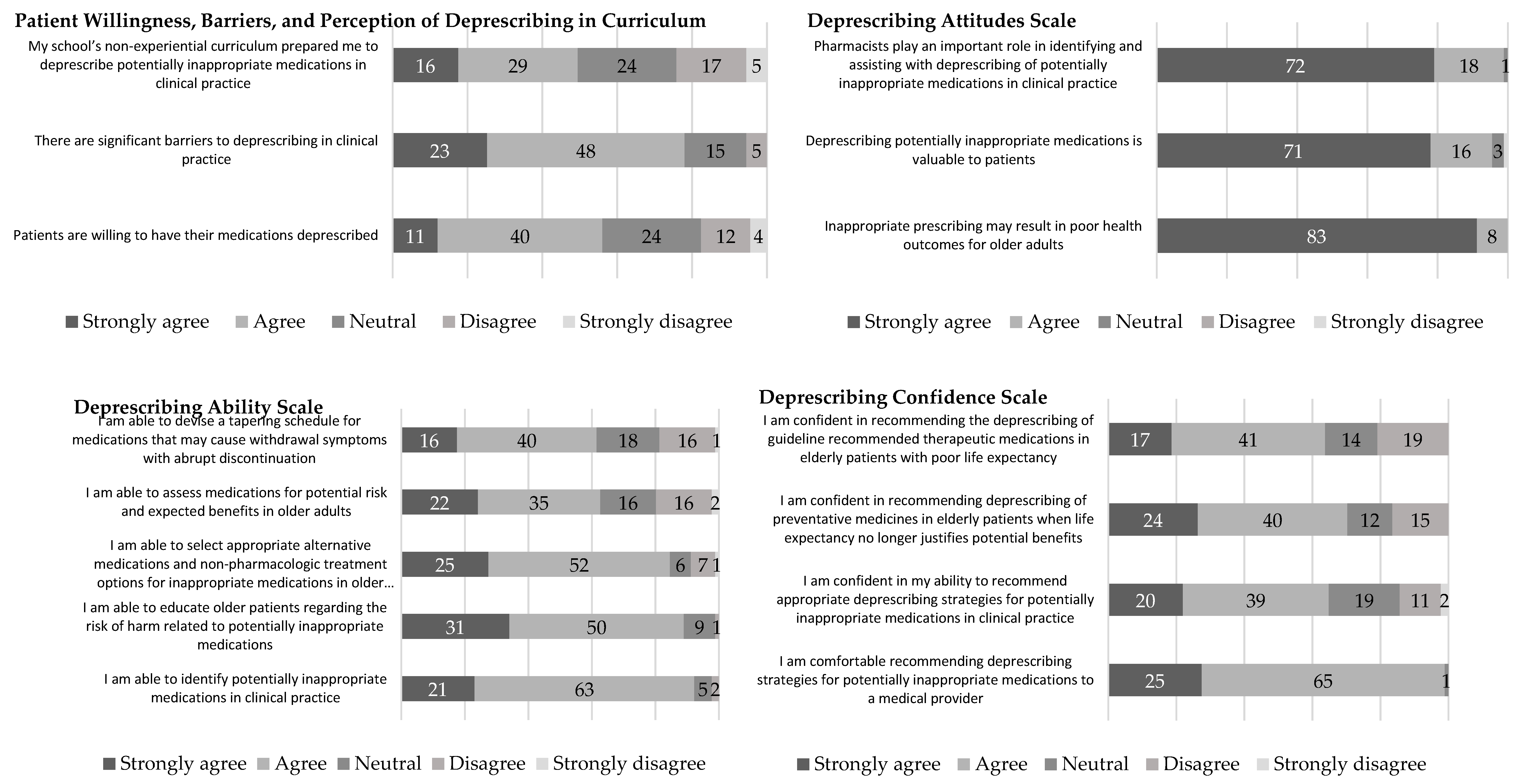
3.3. Student Attitudes and Perceptions Regarding Deprescribing
3.4. Comparison of Perceptions and Knowledge Assessment Score Based on Curricular Exposure to Deprescribing
4. Discussion
4.1. Student Pharmacist Curricular Exposure to Deprescribing
4.2. Student Perceptions of Polypharmacy and Deprescribing
4.3. Student Knowledge of Polypharmacy and Deprescribing
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Survey Instrument
Appendix A.1. Demographics and Curricular Exposure to Deprescribing
- At what school or college of pharmacy are you enrolled?
- How do you describe yourself?
| Male | |
| Female | |
| Prefer not to list | |
| Other: |
- 3.
- What is your race/ethnicity? (select all that apply)
| American Indian or Alaska Native | |
| Native Hawaiian or other Pacific Islander | |
| Asian | |
| White/Caucasian | |
| Black or African American | |
| Hispanic, Latino, or Spanish origin | |
| Other, please specify: |
- 4.
- What are your current plans upon your graduation from your college/school of pharmacy (select all that apply)
| Pharmacy Residency Program | |
| Pharmacy Ph.D Program | |
| JD or Other Law | |
| Masters; please specify | |
| Other Health Professions (MD, DDS, DVM, etc.) | |
| Non -pharmacy Ph.D Program | |
| Fellowship | |
| No Plans for further education in the coming year. |
- 5.
- What are your current plans for primary employment upon your graduation from your college/school of pharmacy? (check all that apply)
| Chain/Independent community pharmacy | |
| Hospital | |
| Clinic-based pharmacy | |
| Academia | |
| Pharmaceutical Industry/government agency | |
| Managed care/consultant/administration | |
| Nursing home/Long term care facility/Home care | |
| Other Pharmacy Related Field; please specify (Allow for free text) |
- 6.
- Please select the statement that best describes your stage of training at your school/college of pharmacy.
| I am finishing the didactic portion of the curriculum and starting Advanced Pharmacy Practice Experiences (APPE) in the 2019-2020 academic year | |
| I am currently completing my Advanced Pharmacy Practice Experiences (APPE) | |
| I am currently completing only didactic courses and/or Introductory Pharmacy Practice Experiences (IPPE) | |
| Other, Please specify (Allow for free text) |
- 7.
- Please select from the following settings in which you have had paid pharmacy work experience of greater than 1 month, completed Introductory Pharmacy Practice Experience (IPPE) rotations, or Advanced Pharmacy Practice Experience (APPE) rotations. (Select all that apply)
| Previous Pharmacy work experience greater than one month | Previous Introductory Pharmacy Practice Experience (IPPE) rotations | Previous Advanced Pharmacy Practice Experience (APPE) rotations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- 8.
- Was there instruction on deprescribing as part of your REQUIRED pharmacy curriculum?
| Yes | |
| No | |
| Don’t know |
- 9.
- Was there instruction on deprescribing as part of the elective coursework at your college/school of pharmacy?
| Yes | |
| No | |
| Don’t know |
- 10.
- If instruction on deprescribing was part of the curriculum (didactic or experiential) at your school/college of pharmacy, during what curricular activities did this occur? (Select all that apply)
| Lectures | |
| Patient-centered case problems | |
| Clinical simulations | |
| Community projects, service learning | |
| Online coursework | |
| Clinical labs | |
| IPPE | |
| APPE | |
| Research or Capstone projects | |
| Other, please specify (Allow for free text) | |
| Did not cover deprescribing in any educational activities |
Appendix A.2.
Appendix A.2.1. Patient Willingness, Barriers, and Perception of Deprescribing in Curriculum
- My school’s non-experiential curriculum prepared me to deprescribe potentially inappropriate medications in clinical practice
- There are significant barriers to deprescribing in clinical practice
- Patients are willing to have their medications deprescribed
Appendix A.2.2. Deprescribing Attitudes Scale
- 4.
- Inappropriate prescribing may result in poor health outcomes for older adults
- 5.
- Deprescribing potentially inappropriate medications is valuable to patients
- 6.
- Pharmacists play an important role in identifying and assisting with deprescribing of potentially inappropriate medications in clinical practice
Appendix A.2.3. Deprescribing Ability Scale
- 7.
- I am able to identify potentially inappropriate medications in clinical practice
- 8.
- I am able to educate older patients regarding the risk of harm related to potentially inappropriate medications
- 9.
- I am able to select appropriate alternative medications and non-pharmacologic treatment options for inappropriate medications in older adults
- 10.
- I am able to assess medications for potential risk and expected benefits in older adults
- 11.
- I am able to devise a tapering schedule for medications that may cause withdrawal symptoms with abrupt discontinuation
Appendix A.2.4. Deprescribing Confidence Scale
- 12.
- I am comfortable recommending deprescribing strategies for potentially inappropriate medications to a medical provider
- 13.
- I am confident in my ability to recommend appropriate deprescribing strategies for potentially inappropriate medications in clinical practice
- 14.
- I am confident in recommending deprescribing of preventative medicines in elderly patients when life expectancy no longer justifies potential benefits
- 15.
- I am confident in recommending the deprescribing of guideline recommended therapeutic medications in elderly patients with poor life expectancy
Appendix A.3.
Appendix A.3.1. Polypharmacy Knowledge Assessment Instrument
- Which of the following statements about sulfonylureas is true?
| Their effects diminish over time | |
| Glipizide has active metabolites and should be avoided in kidney disease | |
| They do not increase the risk of hypoglycemic events | |
| They decrease carbohydrate breakdown |
- 2.
- A 75-year old man takes warfarin for atrial fibrillation and wishes to reconsider the risks and benefits of anticoagulation. Which of the following statements is true?
| The CHA2DS2-VASc and HAS BLED scores both estimate the risk of stroke | |
| Gait impairment resulting in a fall is a contraindication to warfarin use | |
| Bleeding events are generally more devastating than strokes | |
| Poor nutrition may increase the risk of adverse effects from warfarin |
- 3.
- Which of the following is correct about age-related changes?
| The total body water increases and fat content decreases with age | |
| Decreases in lean muscle mass result in decreased creatinine production | |
| Medications are absorbed at the same rate, but to a lesser extent | |
| CYP 450 metabolism decreases predictably by 5% each year |
- 4.
- Which of the following interactions correctly describes why a patient taking warfarin may have difficulty maintaining INR levels within therapeutic range?
| St. John’s wort decreases sensitivity to warfarin | |
| Ciprofloxacin decreases sensitivity to warfarin | |
| Green, leafy salads increase sensitivity to warfarin | |
| Vitamin K increases sensitivity to warfarin |
- 5.
- A 70-year old woman has been taking omeprazole for years. She denies any heartburn in the past 6 months or any history of gastrointestinal bleeding. In your conversation with her, what concern related to adverse effects of proton pump inhibitors might you mention?
| Increased risk of clostridium difficile-associated diarrhea | |
| Increased risk of esophageal cancer | |
| Increased risk of osteonecrosis | |
| Increased risk of impaired glucose tolerance |
- 6.
- A 70-year old woman takes temazepam every night for insomnia, but she heard about safety issues surrounding the drug and wants to discontinue it. She states she has tried sleep hygiene counseling in the past without much success. Anticipating that tapering off temazepam will be difficult for her, what would you recommend as adjunctive therapy during the taper?
| Prescribe lorazepam because it is safer than temazepam | |
| Advise her to repeat sleep hygiene counseling | |
| Refer her to a health psychologist for cognitive behavioral therapy | |
| Prescribe zolpidem because it is safer than temazepam |
Appendix A.3.2. Deprescribing Multiple Choice Questions
- For an older patient who complains of chronic mild low back pain, which of the following medications would you NOT target for deprescribing from his regimen?
| Cyclobenzaprine | |
| Acetaminophen | |
| Celecoxib | |
| Ibuprofen |
- 2.
- Zolpidem has been identified as a drug to avoid in the elderly. Which of the following is an acceptable alternative?
| Temazepam | |
| Diphenhydramine | |
| Quetiapine | |
| None of the above |
- 3.
- Which of the following are considered potentially inappropriate for older patients due to anticholinergic activity?
| Citalopram | |
| Sertraline | |
| Paroxetine | |
| Trazodone |
- 4.
- When recommending deprescribing of alprazolam 0.5mg four times daily in patient of 65 years of age, which of the following is the BEST initial approach?
| Reduce to alprazolam 0.5 mg three times daily | |
| Reduce to alprazolam 0.25 mg four times daily | |
| Convert to diazepam 2 mg three times daily | |
| Convert to lorazepam 0.5 mg four times daily |
- 5.
- In a patient recently discharged home from the hospital where he was in the intensive care unit for 2 weeks, which of the following strategies should be used to deprescribe omeprazole 40mg daily which was started for stress ulcer prophylaxis?
| Discontinue omeprazole, start misoprostol 100 mcg four times daily | |
| Reduce omeprazole to 20 mg daily | |
| Discontinue omeprazole, start ranitidine 150 mg twice daily | |
| Discontinue omeprazole |
- 6.
- Antipsychotics should not be used on older patients with dementia. Which of the following is the rationale behind this black box warning?
| Antipsychotics increase the risk of death | |
| Antipsychotics cause tardive dyskinesia | |
| Antipsychotics cause neuroleptic malignant syndrome | |
| Antipsychotics cause parkinsonian symptoms |
References
- National Institute for Health and Care Excellence. Multimorbidity and Polypharmacy. Available online: www.nice.org.uk/guidance/ktt18 (accessed on 20 October 2020).
- Lund, B.C.; Carnahan, R.M.; Egge, J.A.; Chrischilles, E.A.; Kaboli, P.J. Inappropriate Prescribing Predicts Adverse Drug Events in Older Adults. Ann. Pharmacother. 2010, 44, 957–963. [Google Scholar] [CrossRef]
- Wastesson, J.W.; Morin, L.; Tan, E.C.; Johnell, K. An Update on the Clinical Consequences of Polypharmacy in Older Adults: A Narrative Review. Expert Opin. Drug Saf. 2018, 17, 1185–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- By the American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; O’Sullivan, D.; Byrne, S.; O’Connor, M.N.; Ryan, C.; Gallagher, P. STOPP/START Criteria for Potentially Inappropriate Prescribing in Older People: Version 2. Age Ageing 2014, 44, 213–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molokhia, M.; Majeed, A. Current and Future Perspectives on the Management of Polypharmacy. BMC Fam. Pract. 2017, 18, 70. [Google Scholar] [CrossRef] [Green Version]
- Reeve, E.; Gnjidic, D.; Long, J.; Hilmer, S. A Systematic Review of the Emerging Definition of ‘Deprescribing’ With Network Analysis: Implications for Future Research and Clinical Practice. Br. J. Clin. Pharmacol. 2015, 80, 1254–1268. [Google Scholar] [CrossRef] [Green Version]
- Scott, I.A.; Hilmer, S.N.; Reeve, E.; Potter, K.; Le Couteur, D.G.; Rigby, D.; Gnjidic, D.; Del Mar, C.; Roughead, E.E.; Page, A.; et al. Reducing Inappropriate Polypharmacy. JAMA Intern. Med. 2015, 175, 827–834. [Google Scholar] [CrossRef] [Green Version]
- Peterson, G.M.; Naunton, M.; Deeks, L.S.; Kosari, S.; Jackson, S.; Boom, K. Practice Pharmacists and the Opportunity to Support General Practitioners in Deprescribing in the Older Person. J. Pharm. Pr. Res. 2018, 48, 183–185. [Google Scholar] [CrossRef] [Green Version]
- Martin, P.; Tamblyn, R.; Benedetti, A.; Ahmed, S.; Tannenbaum, C. Effect of a Pharmacist-Led Educational Intervention on Inappropriate Medication Prescriptions in Older Adults. JAMA 2018, 320, 1889–1898. [Google Scholar] [CrossRef]
- Ammerman, C.A.; Simpkins, B.A.; Warman, N.; Downs, T.N. Potentially Inappropriate Medications in Older Adults: Deprescribing with a Clinical Pharmacist. J. Am. Geriatr. Soc. 2018, 67, 115–118. [Google Scholar] [CrossRef] [Green Version]
- Navy, H.J.; Weffald, L.; Delate, T.; Patel, R.J.; Dugan, J.P. Clinical Pharmacist Intervention to Engage Older Adults in Reducing Use of Alprazolam. Consult. Pharm. 2018, 33, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Lasota, S.T.; Merrey, W.; Ross, P.A.; Martin, A.; Feeser, S.A. Provider Responsiveness to Pharmacist Recommendations in a Population Health Setting. Sr. Care Pharm. 2019, 34, 308–316. [Google Scholar] [PubMed]
- Wallis, K.A.; Andrews, A.; Henderson, M. Swimming Against the Tide: Primary Care Physicians’ Views on Deprescribing in Everyday Practice. Ann. Fam. Med. 2017, 15, 341–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ailabouni, N.J.; Nishtala, P.S.; Mangin, D.; Tordoff, J.M. Challenges and Enablers of Deprescribing: A General Practitioner Perspective. PLoS ONE 2016, 11, e0151066. [Google Scholar] [CrossRef] [Green Version]
- Mishori, R. What Needs to Change to Make Deprescribing Doable. Fam. Pract. Manag. 2018, 25, 5–6. [Google Scholar]
- Raman-Wilms, L.; Farrell, B.J.; Sadowski, C.A.; Austin, Z. Deprescribing: An educational Imperative. Res. Soc. Adm. Pharm. 2019, 15, 790–795. [Google Scholar] [CrossRef]
- Odegard, P.S.; Breslow, R.M.; Koronkowski, M.J.; Williams, B.R.; Hudgins, G.A. Geriatric Pharmacy Education: A Strategic Plan for the Future. Am. J. Pharm. Educ. 2007, 71, 47. [Google Scholar] [CrossRef] [Green Version]
- Dutta, A.P.; Daftary, M.; Oke, F.; Mims, B.; Hailemeskel, E.; Sansgiry, S.S. Geriatric Education in U.S. Schools of Pharmacy: A Snapshot. Consult. Pharm. 2005, 20, 45–52. [Google Scholar] [CrossRef]
- Jimenez, S.; Geriatric Content in U.S. Doctor of Pharmacy Degree Curricula. Available online: https://fisherpub.sjfc.edu/education_etd/1 (accessed on 1 April 2020).
- Woodruff, A.E.; Albanese, N.P.; Prescott, W.A. Comparing Pharmacotherapy Instruction to the 2009 and 2016 ACCP Toolkit Recommendations. Am. J. Pharm. Educ. 2018, 82, 6771. [Google Scholar] [CrossRef]
- Schwinghammer, T.L.; Crannage, A.J.; Boyce, E.G.; Bradley, B.; Christensen, A.; Dunnenberger, H.M.; Fravel, M.; Gurgle, H.; Hammond, D.A.; Kwon, J.; et al. The 2016 ACCP Pharmacotherapy Didactic Curriculum Toolkit. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, e189–e194. [Google Scholar] [CrossRef]
- Flannery, A.H.; Soric, M.M.; Benavides, S.; Bobbitt, L.J.; Chan, A.; Crannage, A.J.; Flores, E.K.; Gibson, C.M.; Gurgle, H.E.; Kolanczyk, D.M.; et al. 2019 Update to the American College of Clinical Pharmacy Pharmacotherapy Didactic Curriculum Toolkit. J. Am. Coll. Clin. Pharm. 2019, 3, 455–464. [Google Scholar] [CrossRef]
- Bjerre, L.; Farrell, B.; Hogel, M.; Graham, L.; Lemay, G.; McCarthy, L.; Raman-Wilms, L.; Rojas-Fernandez, C.; Sinha, S.; Thompson, W.; et al. Deprescribing Antipsychotics for Behavioural and Psychological Symptoms of Dementia and Insomnia. Can. Fam. Physician 2018, 64, 17–27. [Google Scholar] [PubMed]
- Farrell, B.J.; Pottie, K.; Thompson, W.; Boghossian, T.; Pizzola, L.; Rashid, F.J.; Rojas-Fernandez, C.; Walsh, K.; Welch, V.; Moayyedi, P. Deprescribing Proton Pump Inhibitors. Can. Fam. Physician 2017, 63, 354–364. [Google Scholar] [PubMed]
- Pottie, K.; Thompson, W.; Davies, S.; Grenier, J.; Sadowski, C.A.; Welch, V.; Holbrook, A.; Boyd, C.; Swenson, R.; Ma, A.; et al. Deprescribing Benzodiazepine Receptor Agonists: Evidence-Based Clinical Practice Guideline. Can. Fam. Physician 2018, 64, 339–351. [Google Scholar]
- Farrell, B.J.; Conklin, J.; Dolovich, L.; Irving, H.; Maclure, M.; McCarthy, L.M.; Moriarty, F.; Pottie, K.; Raman-Wilms, L.; Reeve, E.; et al. Deprescribing Guidelines: An International Symposium on Development, Implementation, Research and Health Professional Education. Res. Soc. Adm. Pharm. 2019, 15, 780–789. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, K.M.; Bell, C.A.; Donohoe, K.L.; Salgado, T.M. Medicine, Pharmacy and Nursing Trainees’ Perceptions of Curriculum Preparation to Deprescribe and Interprofessional Roles in the Deprescribing Process. Gerontol. Geriatr. Educ. 2019, 41, 63–84. [Google Scholar] [CrossRef]
- Djatche, L.; Lee, S.; Singer, D.; Hegarty, S.E.; Lombardi, M.; Maio, V. How Confident Are Physicians in Deprescribing for the Elderly and What Barriers Prevent Deprescribing? J. Clin. Pharm. Ther. 2018, 43, 550–555. [Google Scholar] [CrossRef]
- Lee, K.C.; Rudolph, M.J.; Assemi, M.; Bray, B.S.; Daugherty, K.K.; Karpen, S.C.; Maerten-Rivera, J.L.; Pavuluri, N.; Sease, J.M.; Vellurattil, R.P.; et al. Factors Associated With Cultures of Assessment at US Schools and Colleges of Pharmacy. Curr. Pharm. Teach. Learn. 2019, 11, 129–138. [Google Scholar] [CrossRef]
- Thomas, J.M.; Mecca, M.C.; Niehoff, K.M.; Mecca, A.P.; Van Ness, P.H.; Brienza, R.; Hyson, A.; Jeffery, S. Development and Validation of a Polypharmacy Knowledge Assessment Instrument. Am. J. Pharm. Educ. 2019, 83, 6435. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making Sense of Cronbach’s Alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Harpe, S.E. How to Analyze Likert and Other Rating Scale Data. Curr. Pharm. Teach. Learn. 2015, 7, 836–850. [Google Scholar] [CrossRef]
- Norman, G.R. Likert Scales, Levels of Measurement and the “Laws” of Statistics. Adv. Health Sci. Educ. 2010, 15, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Carifio, J.; Perla, R. Resolving the 50-Year Debate Around Using and Misusing Likert Scales. Med. Educ. 2008, 42, 1150–1152. [Google Scholar] [CrossRef] [PubMed]
- Hsu, T.-C.; Feldt, L.S. The Effect of Limitations on the Number of Criterion Score Values on the Significance Level of the F-Test. Am. Educ. Res. J. 1969, 6, 515–527. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Reeve, E.; Low, L.-F.; Shakib, S.; Hilmer, S.N. Development and Validation of the Revised Patients’ Attitudes Towards Deprescribing (rPATD) Questionnaire: Versions for Older Adults and Caregivers. Drugs Aging 2016, 33, 913–928. [Google Scholar] [CrossRef] [PubMed]
- Reeve, E.; Shakib, S.; Hendrix, I.; Roberts, M.S.; Wiese, M.D. Development and Validation of the Patients’ Attitudes Towards Deprescribing (PATD) Questionnaire. Int. J. Clin. Pharm. 2013, 35, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Reeve, E.; Wolff, J.L.; Skehan, M.; Bayliss, E.A.; Hilmer, S.N.; Boyd, C.M. Assessment of Attitudes Toward Deprescribing in Older Medicare Beneficiaries in the United States. JAMA Intern. Med. 2018, 178, 1673–1680. [Google Scholar] [CrossRef] [Green Version]
- Galazzi, A.; Lusignani, M.; Chiarelli, M.T.; Mannucci, P.M.; Franchi, C.; Tettamanti, M.; Reeve, E.; Nobili, A. Attitudes Towards Polypharmacy and Medication Withdrawal Among Older Inpatients in Italy. Int. J. Clin. Pharm. 2016, 38, 454–461. [Google Scholar] [CrossRef]
- Kalogianis, M.J.; Wimmer, B.C.; Turner, J.P.; Tan, E.C.; Emery, T.; Robson, L.; Reeve, E.; Hilmer, S.N.; Bell, J.S. Are Residents of Aged Care Facilities Willing to Have Their Medications Deprescribed? Res. Soc. Adm. Pharm. 2016, 12, 784–788. [Google Scholar] [CrossRef]
- Sirois, C.; Ouellet, N.; Reeve, E. Community-Dwelling Older People’s Attitudes Towards Deprescribing in Canada. Res. Soc. Adm. Pharm. 2017, 13, 864–870. [Google Scholar] [CrossRef]
- Kutner, J.S.; Blatchford, P.J.; Taylor, D.H.; Ritchie, C.S.; Bull, J.H.; Fairclough, D.L.; Hanson, L.C.; Leblanc, T.W.; Samsa, G.P.; Wolf, S.; et al. Safety and Benefit of Discontinuing Statin Therapy in the Setting of Advanced, Life-Limiting Illness. JAMA Intern. Med. 2015, 175, 691–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garfinkel, D. Poly-de-Prescribing to Treat Polypharmacy: Efficacy and Safety. Ther. Adv. Drug Saf. 2017, 9, 25–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | n (%) |
|---|---|
| Professional Year | |
| P3 | 66 (72.5) |
| P4 | 25 (27.5) |
| Institution Type a | |
| Public | 68 (75.6) |
| Private | 22 (24.4) |
| Region | |
| South | 15 (16.7) |
| West | 8 (0.1) |
| Northeast | 56 (62.2) |
| Midwest | 11 (12.2) |
| Gender | |
| Male | 27 (29.7) |
| Female | 64 (70.3) |
| Race/Ethnicity | |
| White/Caucasian | 67 (73.6) |
| Black or African American | 1 (1.1) |
| Hispanic, Latino, or Spanish origin | 2 (2.2) |
| Asian | 16 (17.6) |
| Other | 5 (5.5) |
| Plans for further education upon your graduation b | |
| Residency or fellowship program | 55 (60.4) |
| Additional academic degree | 7 (7.7) |
| No plans | 34 (37.4) |
| Plans for primary employment upon graduation b | |
| Chain/Independent community pharmacy | 39 (42.9) |
| Hospital | 47 (51.7) |
| Clinic-based Pharmacy | 35 (38.5) |
| Academia | 13 (14.3) |
| Pharmaceutical Industry/government agency | 7 (7.7) |
| Managed Care/Consultant/Administration | 15 (16.5) |
| Nursing home/long-term care/home Care | 9 (9.9) |
| Other | 6 (6.6) |
| Previous pharmacy experience b | |
| Community pharmacy | 91 (100.0) |
| Hospital | 86 (94.5) |
| Clinic-based Pharmacy | 45 (49.5) |
| Nursing home/hospice/home care | 34 (37.4) |
| Academia | 8 (8.8) |
| Managed Care | 20 (22.0) |
| n (%) | |
|---|---|
| Instruction on deprescribing | |
| Required coursework a | 42 (46.2) |
| Elective coursework b | 32 (35.2) |
| Both required and elective | 20 (22.0) |
| None | 37 (40.7) |
| If instruction on deprescribing was part of the curriculum (didactic or experiential) at your school/college of pharmacy, during what curricular activities did this occur? c | |
| Lectures | 62 (68.1) |
| Patient-centered case problems | 46 (50.6) |
| Clinical simulations | 19 (20.9) |
| Community projects, service learning | 7 (7.7) |
| Online coursework | 5 (5.5) |
| Clinical labs | 10 (11.0) |
| IPPE | 20 (22.0) |
| APPE | 23 (25.3) |
| Research or Capstone projects | 4 (4.4) |
| Other | 2 (2.2) |
| Did not cover deprescribing in any education activities | 21 (23.1) |
| Cronbach Alpha (α) a | Deprescribing Curricular Exposure (n = 54) Mean (SD) | No. Deprescribing Curricular Exposure (n = 37) Mean (SD) | Total (n = 91) Mean (SD) | p-Value | Cohen’s d | Magnitude of Effect b | |
|---|---|---|---|---|---|---|---|
| Perception of Deprescribing in Curriculum | - | 3.6 (1.1) | 3.1 (1.1) | 3.4 (1.1) | 0.03 * | 0.48 | small |
| Barriers to Deprescribing | - | 4.0 (0.8) | 4.0 (0.7) | 4.0 (0.7) | 0.83 | 0.05 | very small |
| Patient Willingness to Deprescribe | - | 3.7 (0.8) | 3.2 (1.2) | 3.5 (1.0) | 0.03 * | 0.49 | small |
| Deprescribing Attitudes Scale | 0.70 | 4.9 (0.3) | 4.7 (0.5) | 4.8 (0.4) | 0.07 | 0.41 | small |
| Deprescribing Ability Scale | 0.79 | 3.9 (0.6) | 3.9 (0.6) | 3.9 (0.6) | 0.65 | 0.10 | very small |
| Deprescribing Confidence Scale | 0.82 | 3.9 (0.7) | 3.8 (0.8) | 3.8 (0.7) | 0.60 | 0.11 | very small |
| Polypharmacy Knowledge Assessment Instrument a (%) | 0.19 | 63.0 (23.3) | 58.1 (16.5) | 61.0 (20.8) | 0.25 | 0.24 | small |
| Deprescribing Assessment b (%) | 0.27 | 67.3 (21.0) | 60.4 (22.0) | 64.5 (21.5) | 0.14 | 0.32 | small |
| Combined Assessments c (%) | 0.36 | 65.1 (16.2) | 59.2 (16.4) | 62.7 (16.4) | 0.09 | 0.36 | very small |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clark, C.M.; Hejna, M.; Shao, E.; Maerten-Rivera, J.L.; Monte, S.V.; Wahler, R.G., Jr. Knowledge and Attitudes of Student Pharmacists Regarding Polypharmacy and Deprescribing: A Cross-Sectional Study. Pharmacy 2020, 8, 220. https://doi.org/10.3390/pharmacy8040220
Clark CM, Hejna M, Shao E, Maerten-Rivera JL, Monte SV, Wahler RG Jr. Knowledge and Attitudes of Student Pharmacists Regarding Polypharmacy and Deprescribing: A Cross-Sectional Study. Pharmacy. 2020; 8(4):220. https://doi.org/10.3390/pharmacy8040220
Chicago/Turabian StyleClark, Collin M., Mary Hejna, Elaine Shao, Jaime L. Maerten-Rivera, Scott V. Monte, and Robert G. Wahler, Jr. 2020. "Knowledge and Attitudes of Student Pharmacists Regarding Polypharmacy and Deprescribing: A Cross-Sectional Study" Pharmacy 8, no. 4: 220. https://doi.org/10.3390/pharmacy8040220
APA StyleClark, C. M., Hejna, M., Shao, E., Maerten-Rivera, J. L., Monte, S. V., & Wahler, R. G., Jr. (2020). Knowledge and Attitudes of Student Pharmacists Regarding Polypharmacy and Deprescribing: A Cross-Sectional Study. Pharmacy, 8(4), 220. https://doi.org/10.3390/pharmacy8040220