
Using Technology-Supported Transfer of Care Systems: Informing Good Practice Recommendations

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
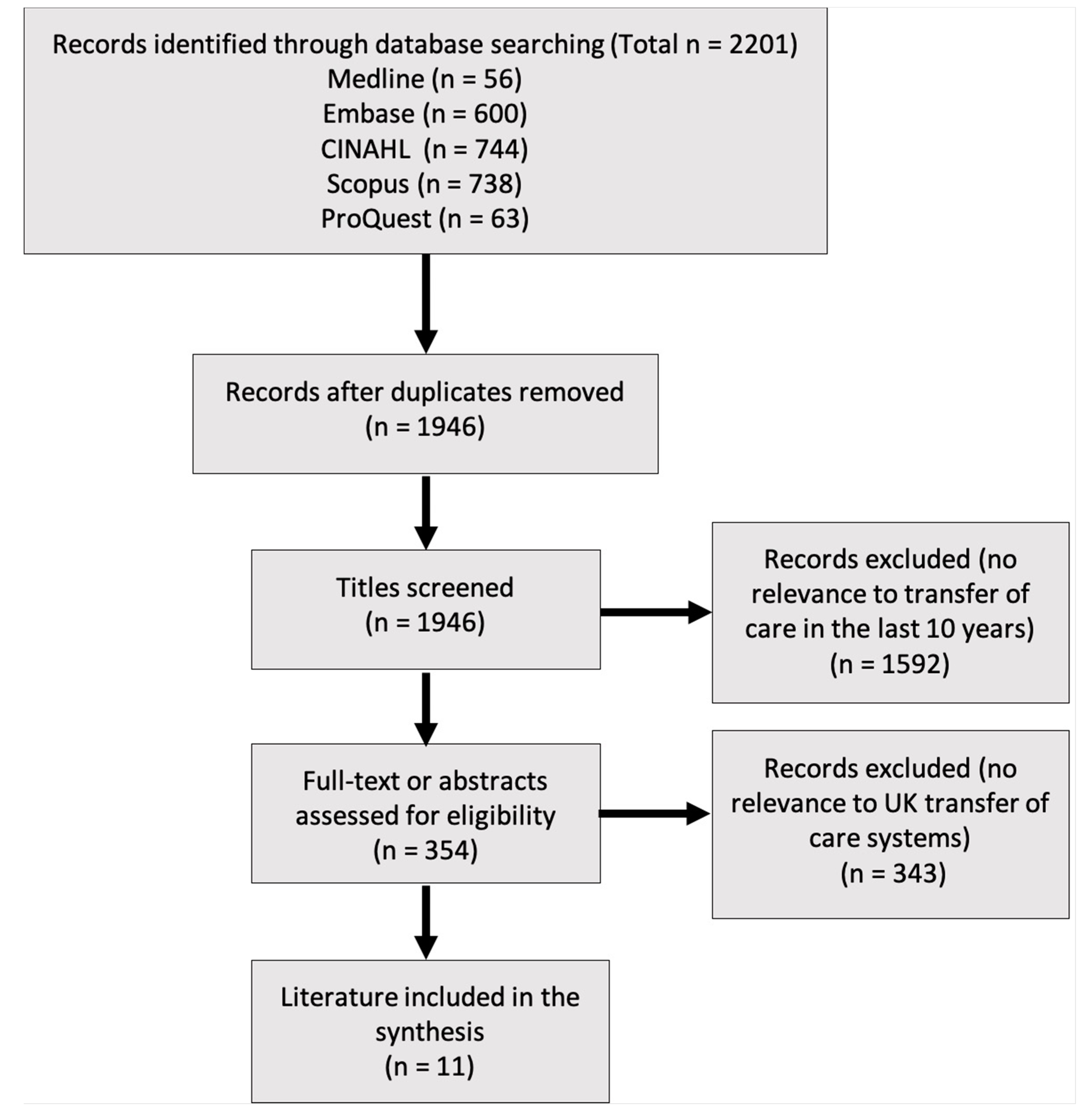
2.1. Method 1: Rapid Literature Review
2.1.1. Search Strategy and Resources
2.1.2. Quality Assessment
2.1.3. Synthesis of Literature
2.2. Method 2: Key Stakeholder Interviews (29th May to 8th July 2019)
2.2.1. Study Approvals
2.2.2. Participants and Recruitment
2.2.3. Data Collection and Analysis
2.2.4. Reflexivity
3. Results
3.1. Method 1 Results: Rapid Literature Review
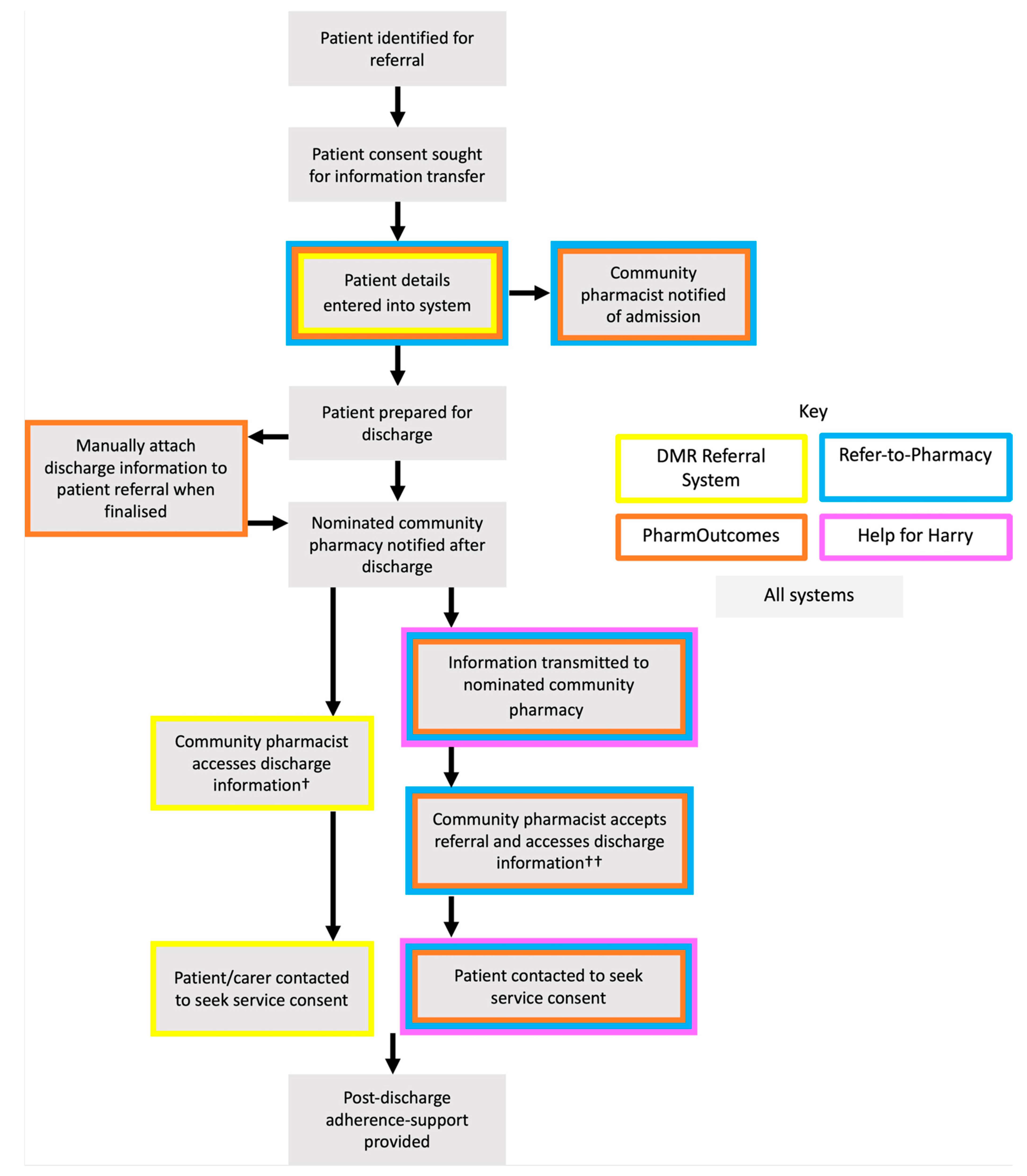
3.1.1. Transfer of Care System Processes
3.1.2. Identifying Differences
Notifications
IT Interoperability
Management of Patient Consent
Patient Referral Eligibility and Screening
System Enabled Dissemination of Service Outcomes
3.2. Method 2 Results: Key Informant Interviews
3.2.1. Theme 1. Implementation
Community Pharmacist Engagement
“There were some people who, again human factors, took a few phone calls to say “please fill the form in”, “oh yeah we’ll do it now we’ll do it now” and of course they didn’t so we had to phone them back so again this took a few months sort of to actually get around to filling out the form to receive the referrals”.(P2)
Marketing Strategies
“I wanted to create some sort of marketing strategy, so I got onto speaker’s circuit at various conferences, started sending out a newsletter to interested parties to keep them informed of developments and that helped sort of create an awareness of what we were actually doing”.(P2)
Collaboration
“So then as an LPC, we supported all the contractors, so we spent time showing them how to use [transfer of care system], how to set up accounts, how to use the system so by pulling down a report we can see who’s not regularly engaging and spending time with them making sure they do engage”.(P3)
Dedicated Staff
“Yeah yeah well that [funding] paid for me which really helped sort the meetings at the hospital, ring the pharmacies, develop guides, develop the [transfer of care system] cos all that takes time really and so we have engagement events so which is a lot of work we need to get the service up and running”.(P3)
Piloting
“No, no, no [we didn’t pilot], it was rolled out across our trust’s footprint in a big bang way”.(P2)
3.2.2. Theme 2. System Attributes
IT interoperability
“It [the transfer of care system] populates the form for you, that saves them [community pharmacists] time as well so all they’ve got to go is “is it the same?”, if it’s different, what’s different and tick boxes, so we’ve tried to make it as easy as possible for them. So, I think it’s probably removed a number of the barriers”.(P1)
“It’s still an extra step for them [referring practitioners] I think, it’d be better if it was integrated into the hospital IT system somehow cos we use a web-based platform and although it’s a quicker system than using a fax for the trust except for the departments in the hospital it’s still a lot of logging in and that’s what they said they’d use it if it was integrated”.(P3)
Referral Prompts
“It [transfer of care system] prompts to make a referral if they’re a blister pack patient or a care home resident so we’re pretty good at making those referrals”.(P2)
Referrals to Alternative Practitioners
“We also send referrals to what we called a medicines support team so a domiciliary pharmacy support service for people from [CCG name] so that’s to arrange home visits for people who are housebound or can’t easily access community pharmacy services and they can visit them in their home”.(P2)
3.2.3. Theme 3. Stakeholder Engagement
Accountability for Referrals
“I’ve seen some of the other platforms go live and they’ve had no support for community pharmacists and if you’ve got no-one pulling down a report to see which pharmacies are doing it, it just gets forgotten about, the pharmacists don’t know how to use the system and then it just falls, falls apart”.(P3)
Feedback of Service Outcomes to Hospitals
“We have regular meetings with the hospital as well so they can see what the pharmacy is doing, y’know it’s not just going into the ether like a fax was, they can see all the feedback and they’re loving seeing all the data that pharmacy’s doing and they’re like “let’s keep going cos, let’s send more referrals, who else could we refer because pharmacy is really engaging with this so”. So they’re really enjoying it as well, they’re really happy”.(P3)
Staff Training Tools
“So, I thought I’ll do a [transfer of care system] quiz and that’s been used by the staff to sort of get them into understanding why someone is eligible for referral”.(P2)
4. Discussion
Limitations
5. Conclusions
- Pre-plan implementation strategies with dedicated staff, focussing on stakeholder engagement;
- Flexible notification systems should be developed to inform community pharmacists of patient admission and discharge, including email and USB device notifications;
- Produce content such as videos to support patient consent for information transfer;
- Develop methods to keep hospital and community practitioners accountable for referrals;
- Develop interoperability with both hospital and community IT systems to make referrals seamless;
- Ensure post-discharge adherence-support services have broad eligibility criteria.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- (1)
- Could you explain a bit about the history of DMR/Refer-To-Pharmacy/Pharmoutcomes/Help for Harry?
- Why was it set up?
- (2)
- Could you please take me through a step by step process of the service from identification of patients to post-discharge follow-up
- (3)
- How is patient consent managed throughout the service?
- Hospital consent (what is this for?)
- Community consent (what is this for?)
- (4)
- What data are routinely collected through each service?
- Medication names
- Number of discrepancies
- Outcome of referral
- Demographics
- (5)
- How many pharmacies currently provide this service? (clarify if this is increasing)
- How many did it start with, as a pilot?
- Is this still increasing?
- How have you managed to get pharmacies on board?
- (6)
- Through research on DMRs, it was found that many hospital staff felt that they initiate the scheme but see no end-product. What feedback is routinely provided to hospital staff?
- How is this recorded?
- (7)
- How do community pharmacists receive notification that a patient has been discharged from hospital? (clarify whether personal/NHS email, etc.)
- Has this changed since inception of the service?
- Do you see any issues with these methods?
- Any additional notifications provided? (admission)
- (8)
- What do you consider are the barriers to the provision of RTF/DMR/PharmOutcomes?
- Have these changed over time?
- (9)
- What do you consider are the facilitators to the provision of RTP/DMR/Pharmoutcomes/Help for Harry?
- Have these changed over time?
- (10)
- What, if any, improvements or advances are planned in the foreseeable future for this service?
- Are changes in services based on service evaluations?
- What further service evaluations are planned and how do you hope these will implement further change?
Appendix B

{kind=link}
{kind=link}
| Summary for Reporting Qualitative Research Item | Corresponding Line(s) |
|---|---|
| Item 1. Title: Concise description of the nature and topic of the study. Identifying the study as qualitative or indicating the approach (e.g., ethnography, grounded theory) or data collection methods (e.g., interview, focus group) is recommended. | 2–3 |
| Item 2. Abstract: Summary of key elements of the study using the abstract format of the intended publication; typically includes background, purpose, methods, results, and conclusions. | 13–28 |
| Item 3. Problem Formulation: Description and significance of the problem/phenomenon studied; review of relevant theory and empirical work; problem statement. | 32–73 |
| Item 4. Purpose or research question: Purpose of the study and specific objectives or questions. | 70–76 |
| Item 5. Qualitative approach and research paradigm: Qualitative approach (e.g., ethnography, grounded theory, case study, phenomenology, narrative research) and guiding theory if appropriate; identifying the research paradigm (e.g., post-positivist, constructivist/interpretivist) is also recommended; rationale. | 115–118 |
| Item 6. Researcher characteristics and reflexivity: Researchers’ characteristics that may influence the research, including personal attributes, qualifications/experience, relationship with participants, assumptions, and/or presuppositions; potential or actual interaction between researchers’ characteristics and the research questions, approach, methods, results and/or transferability. | 143–149 |
| Item 7. Context: Setting/site and salient contextual factors; rationale. | 126–134 |
| Item 8. Sampling strategy: How and why research participants, documents, or events were selected; criteria for deciding when no further sampling was necessary (e.g., sampling saturation); rationale. | 126–134 |
| Item 9. Ethical issues pertaining to human subjects: Documentation of approval by an appropriate ethics review board and participant consent, or explanation for lack thereof; other confidentiality and data security issues. | 122–125 |
| Item 10. Data collection methods: Types of data collected; details of data collection procedures including (as appropriate) start and stop dates of data collection and analysis, iterative process, triangulation of sources/methods, and modification of procedures in response to evolving study findings; rationale. | 135–142 |
| Item 11. Data collection instruments and technologies: Description of instruments (e.g., interview guides, questionnaires) and devices (e.g., audio recorders) used for data collection; if/how the instrument(s) changed over the course of the study. | Appendix A 122–124 |
| Item 12. Units of study: Number and relevant characteristics of participants, documents, or events included in the study; level of participation. | 126–134 |
| Item 13. Data processing: Methods for processing data prior to and during analysis, including transcription, data entry, data management and security, verification of data integrity, data coding and anonymization/de-identification of excerpts. | 135–142 |
| Item 14. Data analysis: Process by which inferences, themes, etc., were identified and developed, including the researchers involved in data analysis; usually references a specific paradigm or approach; rationale. | 135–142 |
| Item 15. Techniques to enhance trustworthiness: Techniques to enhance trustworthiness and credibility of data analysis, (e.g., member checking, triangulation, audit trail); rationale. | 141–142 |
| Item 16. Synthesis and interpretation: Main findings (e.g., interpretations, inferences, and themes); might include development of a theory or model, or integration with prior research or theory. | 265–409 |
| Item 17. Links to empirical data: Evidence (e.g., quotes, field notes, text excerpts, photographs) to substantiate analytic findings. | 265–409 |
| Item 18. Integration with prior work, implications, transferability, and contribution(s) to the field: Short summary of main findings, explanation of how findings and conclusions connect to, support, elaborate on, or challenge conclusions of earlier scholarship; discussion of scope of application/generalizability; identification of unique contribution(s) to scholarship in a discipline or field. | 410–485 |
| Item 19. Limitations: Trustworthiness and limitations of findings. | 486–503 |
| Item 20. Conflicts of interest: Potential sources of influence or perceived influence on study conduct and conclusions; how these were managed. | 530 |
| Item 21. Funding: Sources of funding and other support; role of funders in data collection, interpretation, and reporting. | 527–528 |
References
- Greenwald, J.L.; Denham, C.R.; Jack, B.W. The hospital discharge: A review of a high risk care transition with highlights of a reengineered discharge process. J. Patient Saf. 2007, 3, 97–106. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Medication Without Harm WHO Global Patient Safety Challenge; WHO: Geneva, Switzerland, 2017; pp. 1–10. [Google Scholar]
- Naylor, C.; Imison, C.; Addicott, R.; Buck, D.; Goodwin, N.; Harrison, T.; Ross, S.; Sonola, L.; Tian, Y.; Curry, N. Transforming Our Health Care System: Ten Priorities for Commissioners; The Kings Fund: London, UK, 2015; pp. 1–13. [Google Scholar]
- Couturier, B.; Carrat, F.; Hejblum, G. A systematic review on the effect of the organisation of hospital discharge on patient health outcomes. BMJ Open 2016, 6, e012287. [Google Scholar] [CrossRef] [Green Version]
- Nazar, H.; Nazar, Z.; Portlock, J.; Todd, A.; Slight, S.P. A systematic review of the role of community pharmacies in improving the transition from secondary to primary care. Br. J. Clin. Pharmacol. 2015, 80, 936–948. [Google Scholar] [CrossRef] [Green Version]
- Hugtenburg, J.G.; Borgsteede, S.D.; Beckeringh, J.J. Medication review and patient counselling at discharge from the hospital by community pharmacists. Pharm. World Sci. 2009, 31, 630–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, K.; Nguyen, A.; Shakib, S.; Doecke, C.J.; Boyce, M.; March, G.; Anderson, B.A.; Gilbert, A.L.; Angley, M.T. Enhancing continuity of care in therapeutics: Development of a post-discharge home medicines review model. J. Pharm. Pract. Res. 2007, 37, 22–26. [Google Scholar] [CrossRef]
- NHS England. The NHS Long Term Plan; NHS England: London, UK, 2019; pp. 91–98. Available online: www.longtermplan.nhs.uk (accessed on 13 August 2019).
- Topol, E. Preparing the Healthcare Workforce to Deliver the Digital Future the Topol Review; Health Education England: London, UK, 2019; pp. 1–21. Available online: https://topol.hee.nhs.uk/wp-content/uploads/HEE-Topol-Review-2019.pdf (accessed on 10 January 2020).
- Institute for Government Devolution and the NHS. Available online: https://www.instituteforgovernment.org.uk/explainers/devolution-nhs (accessed on 25 January 2021).
- Royal Pharmaceutical Society. Hospital Referral to Community Pharmacy: An Innovators’ Toolkit to Support the NHS in England; Royal Pharmaceutical Society: London, UK, 2014; pp. 1–21. Available online: http://www.rpharms.com/promoting-pharmacy-pdfs/moc-report-full.pdf (accessed on 1 August 2019).
- Mantzourani, E.; Way, C.M.; Hodson, K.L. Does an integrated information technology system provide support for community pharmacists undertaking Discharge Medicines Reviews? An exploratory study. Integr. Pharm. Res. Pract. 2017, 6, 145–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantzourani, E.; Nazar, H.; Phibben, C.; Pang, J.; John, G.; Evans, A.; Thomas, H.; Way, C.; Hodson, K. Exploring the association of the discharge medicines review with patient hospital readmissions through national routine data linkage in Wales: A retrospective cohort study. BMJ Open 2020, 10, e33551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantzourani, E.; Hodson, K.; Way, C.; Evans, A. The Discharge Medicines Review Service in Wales: What is it and what are the benefits? Int. Pharm. J. 2020, 38, 34–37. [Google Scholar]
- Sabir, F.R.N.; Tomlinson, J.; Strickland-Hodge, B.; Smith, H. Evaluating the Connect with Pharmacy web-based intervention to reduce hospital readmission for older people. Int. J. Clin. Pharm. 2019, 41, 1239–1246. [Google Scholar] [CrossRef] [Green Version]
- Hodson, K.; Smith, M.; Blenkinsopp, A.; Hughes, L.; James, D.; Cohen, D.; Davies, P.; O’Briena, C.; Turnbull, L.; Alam, F.; et al. Evaluation of the Discharge Medicines Review Service in Wales: Content analysis of Discharge Medicines Reviews. Int. J. Pharm. Pract. 2014, 22, 65. [Google Scholar]
- Hodson, K.; James, D.; Smith, M.; Turnbull, L. Evaluation of the Discharge Medicines Review Service; Welsh Institute for Health and Social Care: Pontypridd, UK, 2014; pp. 33–51. [Google Scholar]
- World Health Organisation. Medication Safety in Transitions of Care; WHO: Geneva, Switzerland, 2019; pp. 5–15. [Google Scholar]
- Hesse-Biber, S.; Burke, J. The Oxford Handbook of Multimethod and Mixed Methods Research Inquiry, 1st ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Anguera, M.T.; Blanco-Villaseñor, A.; Losada, J.L.; Sánchez-Algarra, P.; Onwuegbuzie, A.J. Revisiting the difference between mixed methods and multimethods: Is it all in the name? Qual. Quant. 2018, 52, 2757–2770. [Google Scholar] [CrossRef]
- Sandelowski, M. Whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Kahlke, R.M. Generic Qualitative Approaches: Pitfalls and Benefits of Methodological Mixology. Int. J. Qual. Methods 2014, 13, 37–52. [Google Scholar] [CrossRef]
- Tricco, A.C.; Zarin, W.; Antony, J.; Hutton, B.; Moher, D.; Sherifali, D.; Straus, S.E. An international survey and modified Delphi approach revealed numerous rapid review methods. J. Clin. Epidemiol. 2016, 70, 61–67. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport. Exerc. Heal. 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Roberts, A. PharmOutcomes Instructional Video. Available online: https://www.youtube.com/watch?v=PXcH9JmRUEU (accessed on 14 October 2019).
- Gray, A. Refer to Pharmacy Presentation and Demo February 2017. Available online: https://www.youtube.com/watch?time_continue=1040&v=Q0R2arCDgaY (accessed on 19 November 2018).
- Pinnacle Media PharmOutcomes Media. Available online: https://media.pharmoutcomes.org/video.php?name=hospitalref2 (accessed on 24 November 2018).
- NHS Wales Informatics Service Choose Pharmacy User Guide Version 7.0. Available online: http://www.cpwales.org.uk/getattachment/Services-and-commissioning/Enhanced-Services/Seasonal-Influenza-Vaccination-Service/Choose-Pharmacy-User-Guide-v8-0919.pdf.aspx?lang=en-GB (accessed on 24 April 2020).
- Gray, A. Refer-To-Pharmacy: Pharmacy for the Next Generation Now! A Short Communication for Pharmacy. Pharmacy 2015, 3, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Pinnacle Health PharmOutcomes. Available online: https://pharmoutcomes.org/pharmoutcomes/ (accessed on 18 April 2019).
- Pinnacle Health Partnership LLP Home Page—PharmOutcomes. Available online: https://pharmoutcomes.org/pharmoutcomes/ (accessed on 28 October 2018).
- PSNC New Medicine Service (NMS). Available online: https://psnc.org.uk/services-commissioning/advanced-services/nms/ (accessed on 5 July 2019).
- PSNC Medicines Use Review (MUR). Available online: https://psnc.org.uk/services-commissioning/advanced-services/murs/ (accessed on 17 April 2019).
- Gray, A. Refer-to-Pharmacy Hospital Demo Featurig the New Hospital Admission Notification Message. Available online: https://www.youtube.com/watch?v=EGnTlFC1ZOc (accessed on 23 June 2020).
- Gray, A. Refer-to-Pharmacy Community Pharmacy Training Film February 2017. Available online: https://www.youtube.com/watch?v=CdvXPHnOKxM&t=189s (accessed on 25 October 2018).
- The Eastern Academic Health Science Network PharmOutcomes. Available online: https://www.youtube.com/watch?v=BQAHOjy8KxI (accessed on 13 August 2019).
- Ferguson, J.; Seston, L.; Ashcroft, D.M. Refer-to-pharmacy: A qualitative study exploring the implementation of an electronic transfer of care initiative to improve medicines optimisation following hospital discharge. BMC Health Serv. Res. 2018, 18, 424. [Google Scholar] [CrossRef] [Green Version]
- Nazar, H.; Brice, S.; Akhter, N.; Kasim, A.; Gunning, A.; Slight, S.P.; Watson, N.W. New transfer of care initiative of electronic referral from hospital to community pharmacy in England: A formative service evaluation. BMJ Open 2016, 6, e012532. [Google Scholar] [CrossRef] [Green Version]
- Gray, A. Refer-to-Pharmacy Hospital Pharmacy Training Film February 2017. Available online: https://www.youtube.com/watch?v=lpV6xOf6l4Q (accessed on 20 November 2019).
- Ramsbottom, H.; Fitzpatrick, R.; Rutter, P. Post discharge medicines use review service for older patients: Recruitment issues in a feasibility study. Int. J. Clin. Pharm. 2016, 38, 208–212. [Google Scholar] [CrossRef]
- Coleman, E.A.; Smith, J.D.; Raha, D.; Min, S.J. Posthospital medication discrepancies: Prevalence and contributing factors. Arch. Intern. Med. 2005, 165, 1842–1847. [Google Scholar] [CrossRef]
- Belfrage, B.; Koldestam, A.; Sjöberg, C.; Wallerstedt, S.M. Prevalence of suboptimal drug treatment in patients with and without multidose drug dispensing—A cross-sectional study. Eur. J. Clin. Pharmacol. 2014, 70, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Look, K.A.; Stone, J.A. Medication management activities performed by informal caregivers of older adults. Res. Soc. Adm. Pharm. 2018, 14, 418–426. [Google Scholar] [CrossRef]
- Pharmaceutical Services Negotiating Committee Discharge Medicines Service. Available online: https://psnc.org.uk/services-commissioning/essential-services/discharge-medicines-service/ (accessed on 25 January 2021).
- NHS England; NHS Improvement. NHS Discharge Medicines Service Essential Service: Toolkit for Pharmacy Staff in Community, Primary Care and Secondary Care; NHS England: London, UK, 2020; pp. 1–24.
- NHS England. Next Steps on the NHS Five Year Forward View; NHS England: London, UK, 2017; pp. 66–68.
- Greenhalgh, T.; Abimbola, S. The NASSS Framework A Synthesis of Multiple Theories of Technology Implementation. Stud. Health Technol. Inform. 2019, 263, 193–204. [Google Scholar]
- Jepson, R.G.; Robertson, R. Difficulties in giving fully informed consent. BMJ 2003, 326, 1039. [Google Scholar] [CrossRef] [Green Version]
- Sherlock, A.; Brownie, S. Patients’ recollection and understanding of informed consent: A literature review. ANZ J. Surg. 2014, 84, 207–210. [Google Scholar] [CrossRef]
- Nehme, J.; El-Khani, U.; Chow, A.; Hakky, S.; Ahmed, A.R.; Purkayastha, S. The Use of Multimedia Consent Programs for Surgical Procedures. Surg. Innov. 2013, 20, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Mawhinney, G.; Thakar, C.; Williamson, V.; Rothenfluh, D.A.; Reynolds, J. Oxford Video Informed Consent Tool (OxVIC): A pilot study of informed video consent in spinal surgery and preoperative patient satisfaction. BMJ Open 2019, 9, e027712. [Google Scholar] [CrossRef] [PubMed]
- May, C.; Finch, T. Implementing, Embedding, and Integrating Practices: An Outline of Normalization Process Theory I I. Sociology 2009, 43, 535–554. [Google Scholar] [CrossRef]
- NHS Wales Informatics Service. GPs Given Access to Welsh Clinical Portal. Available online: https://nwis.nhs.wales/news/latest-news/gps-given-access-to-welsh-clinical-portal/ (accessed on 7 August 2020).
- Ross, J.; Stevenson, F.; Lau, R.; Murray, E. Factors that influence the implementation of e-health: A systematic review of systematic reviews (an update). Implement. Sci. 2016, 11, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Social Care. New Pharmacy Referral Service to Help Patients Avoid Hospital Readmission. Available online: https://www.gov.uk/government/news/new-pharmacy-referral-service-to-help-patients-avoid-hospital-readmission (accessed on 26 June 2020).


| Eligibility Criteria | |
|---|---|
| Published between January 2009 and November 2018 Published in English Relates to UK technology-supported transfer of care systems | |
| Structured Literature Search | |
| Databases Searched | Search Terms |
| MEDLINE CINAHL EMBASE | “Patient transfer” OR “Care adj3 transfer” OR “Care adj3 transition” OR “hospital discharge” OR “information adj3 transfer” AND “Pharmac *” “community pharmacy” “community pharmacist” |
| SCOPUS PROQUEST | “Care w/3 transfer” OR “hospital discharge” OR “information transfer” OR AND “community pharm *” Including only literature indexed under ‘Nursing’, ‘Health professions’, ‘Medicine’, ‘Psychology’, ‘Social Sciences’, ‘Toxicology and Pharmacology’ and ‘Economics’ categories. |
| Targeted Literature Search | |
| Pharmaceutical Journal International Pharmaceutical Federation Clinical Pharmacist National Institute for Health and Care Excellence (NICE) Royal Pharmaceutical Society Pharmaceutical Service Negotiating Committee (PSNC) Community Pharmacy Wales East Lancashire NHS Trust YouTube | Hospital discharge Refer-to-Pharmacy PharmOutcomes Discharge Medicines Review DMR Help for Harry |
| DMR Referral System | Refer-to-Pharmacy | PharmOutcomes | Help for Harry | |
|---|---|---|---|---|
| Location [11,17,31,32] | Wales (only available from hospital wards that use the all-Wales electronic discharge IT system) | East Lancashire and Blackburn with Darwen Clinical Commissioning Groups (CCG) | Devon, Hampshire and Isle of Wight, North of Tyne, Thames Valley, Buckinghamshire, Cornwall and Isles of Sicily CCGs | Derbyshire NHS Trust |
| System developers [11,30,31,33] | NHS Wales Informatics Service | Webstar-Health in conjunction with East Lancashire CCG | Pinnacle Health Partnership LLP | Derbyshire NHS Trust |
| Funding for IT infrastructure [11,17,33] | Funded centrally by the Welsh Government. | Funded between CCGs and NHS Trust. | Funded by CCG. Payment varies depending on how much functionality is needed. | No IT infrastructure costs. The fax machine is supplied by the individual hospital. |
| The extent of information transfer [28,30] | Discharge medication information only. | Clinical information and discharge medication information. | Discharge medication information only. | Discharge medication information only. |
| Adherence-support service [11,30,31] | DMR service † | Medicines Use Review (MUR) or New Medicines Service (NMS) †† | MUR or NMS | MUR or NMS |
| Post-discharge service payment to pharmacy contractor [17,34,35] | GBP 37 per DMR | GBP 20–28 per NMS GBP 28 per MUR | GBP 20–28 per NMS GBP 28 per MUR | GBP 20–28 per NMS GBP 28 per MUR |
| Patient Inclusion Criteria | ||
|---|---|---|
| DMR | NMS | Discharge MUR |
| Medication change in hospital | New medication for type 2 diabetes, COPD, asthma, hypertension or anticoagulation | Taking two or more medications |
| More than four medications | Medication change in hospital | |
| The patient has their medication dispensed into a compliance aid | ||
| Professional judgement | ||
| Location of review | ||
|
|
|
| Who can receive the review? | ||
| Patient or carer | Patient only | Patient only |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
James, R.; Mantzourani, E.; Way, C.; Gray, A.; Burnley, M.; Hodson, K. Using Technology-Supported Transfer of Care Systems: Informing Good Practice Recommendations. Pharmacy 2021, 9, 36. https://doi.org/10.3390/pharmacy9010036
James R, Mantzourani E, Way C, Gray A, Burnley M, Hodson K. Using Technology-Supported Transfer of Care Systems: Informing Good Practice Recommendations. Pharmacy. 2021; 9(1):36. https://doi.org/10.3390/pharmacy9010036
Chicago/Turabian StyleJames, Robert, Efi Mantzourani, Cheryl Way, Alistair Gray, Melissa Burnley, and Karen Hodson. 2021. "Using Technology-Supported Transfer of Care Systems: Informing Good Practice Recommendations" Pharmacy 9, no. 1: 36. https://doi.org/10.3390/pharmacy9010036
APA StyleJames, R., Mantzourani, E., Way, C., Gray, A., Burnley, M., & Hodson, K. (2021). Using Technology-Supported Transfer of Care Systems: Informing Good Practice Recommendations. Pharmacy, 9(1), 36. https://doi.org/10.3390/pharmacy9010036