Helping Québec Pharmacists Seize the Vaccination Service Opportunity: The Pharmacy Best Practice Workshops

Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Methods
2.1. Identification of Best Practices and Competency Gaps
2.2. Development of Clinical Studies
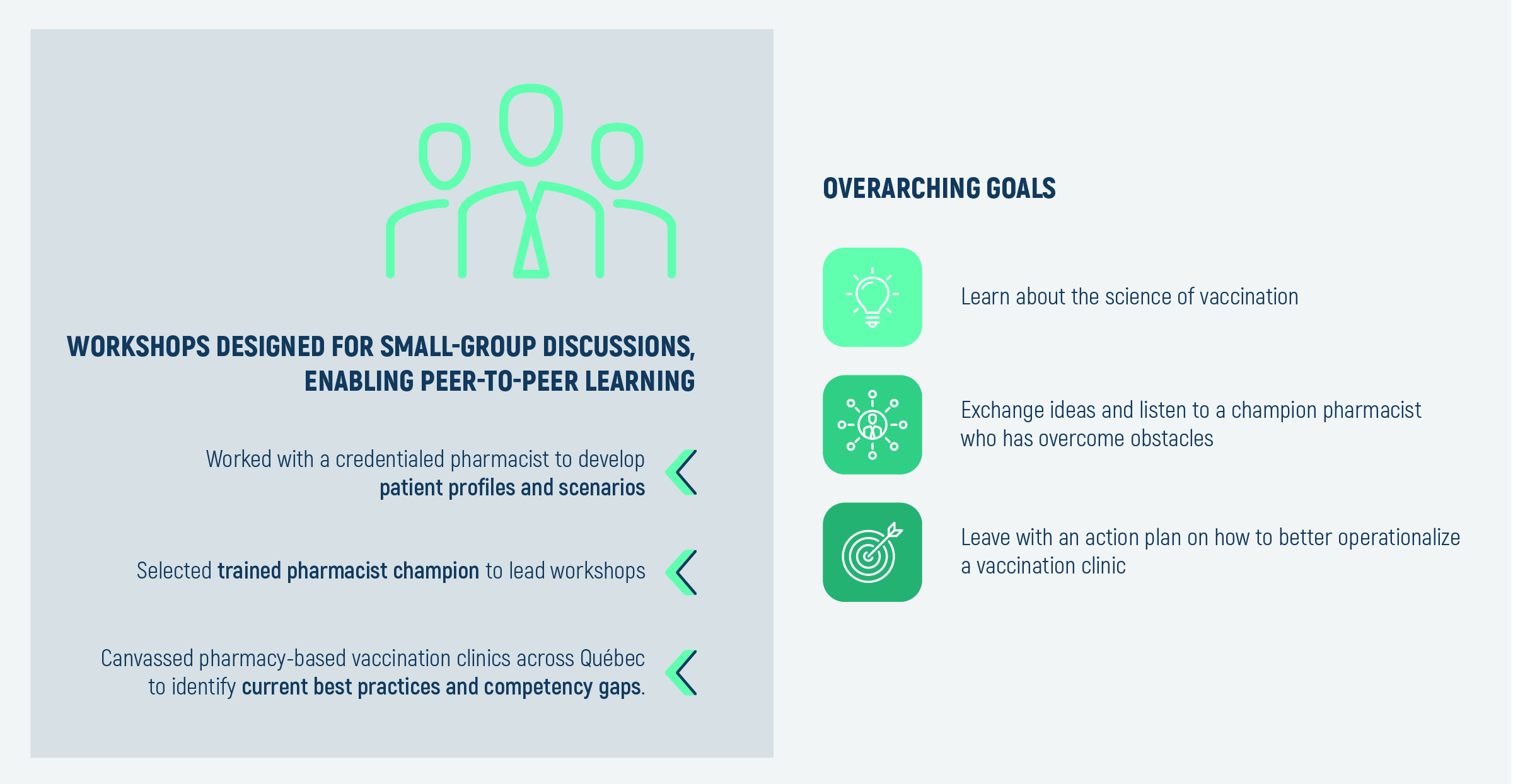
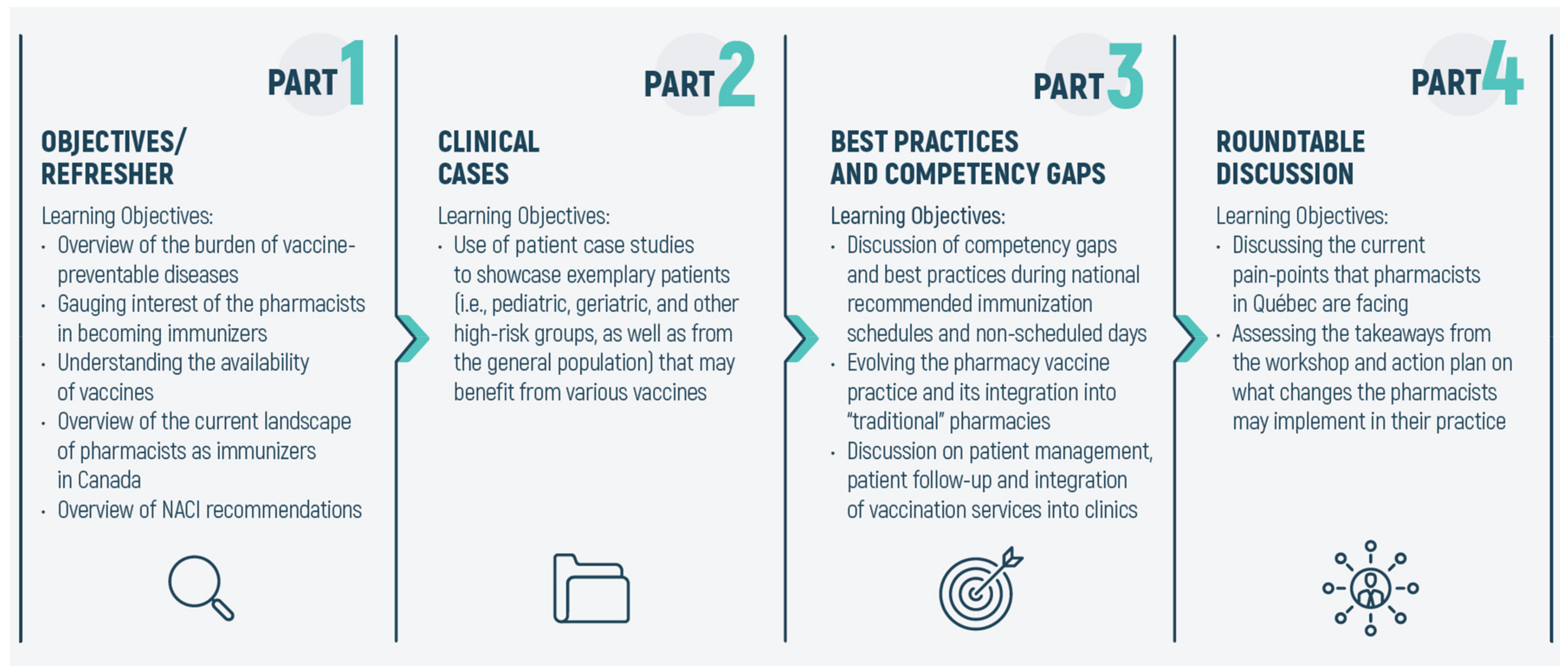
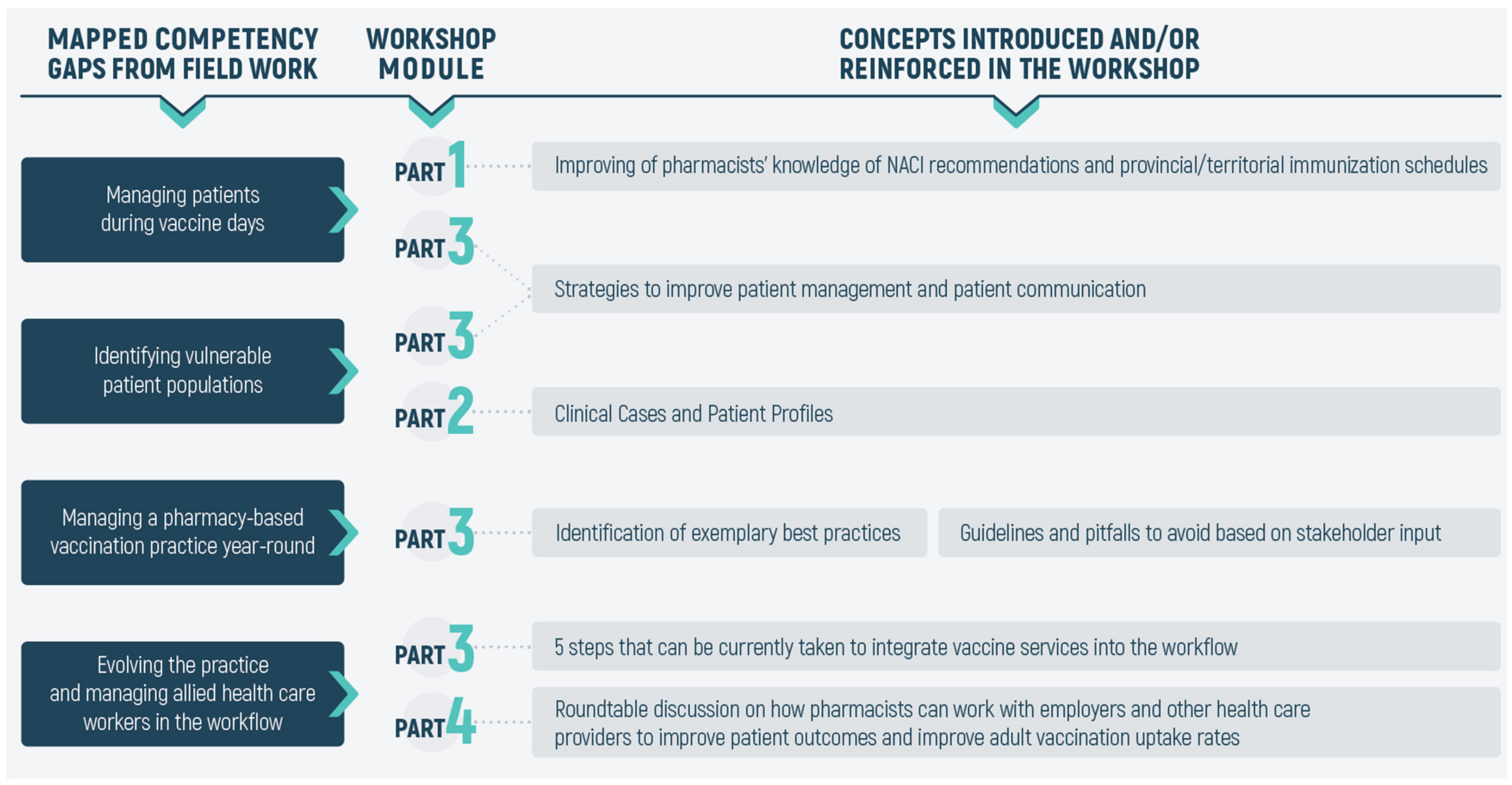
2.3. Developing the Expert-Led Interactive Workshops
2.4. Evaluation of the Workshop
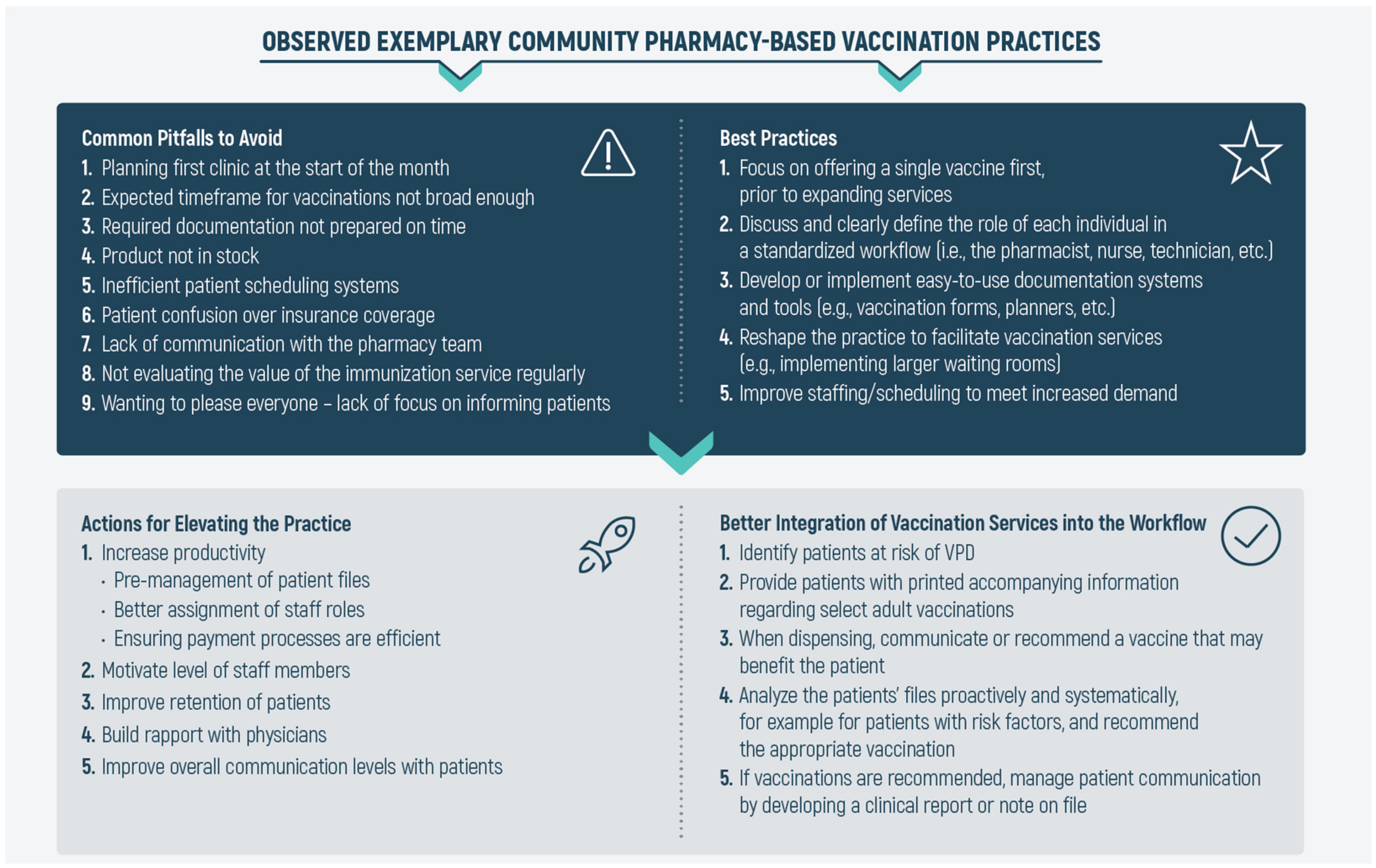
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Public Health Agency of Canada. Canadian Immunization Guide, 7th ed.; Publishing and Depository Services Public Works and Government Services Canada: Ottawa, ON, Canada, 2006. [Google Scholar]
- Violette, R.; Pullagura, G.R. Vaccine Hesitancy: Moving Practice beyond Binary Vaccination Outcomes in Community Pharmacy. Can. Pharm. J. Ott. 2019, 152, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Brousseau, N.; Gagnon, D.; Vivion, M.; Poliquin, V.; Boucoiran, I.; Tapiéro, B.; Dubé, E. Expected Challenges of Implementing Universal Pertussis Vaccination During Pregnancy in Quebec: A Cross-Sectional Survey. CMAJ Open 2018, 6, E391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ecarnot, F.; Maggi, S.; Michel, J.-P. Strategies to Improve Vaccine Uptake throughout Adulthood. In Vaccines for Older Adults: Current Practices and Future Opportunities; Karger Publishers: Basel, Switzerland, 2020; Volume 43, pp. 234–248. [Google Scholar]
- Buchan, S.A.; Rosella, L.C.; Finkelstein, M.; Juurlink, D.; Isenor, J.; Marra, F.; Patel, A.; Russell, M.L.; Quach, S.; Waite, N. Impact of pharmacist administration of influenza vaccines on uptake in Canada. CMAJ 2017, 189, E146–E152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skowronski, D.M.; Janjua, N.Z.; De Serres, G. Understanding Suboptimal Influenza Vaccine Effectiveness Within the Agent, Host, and Environment Paradigm. Clin. Infect. Dis. 2013, 57, 476–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacDonald, N. Improving Vaccination Rates: The Long and Winding Road to Improving Immunization Rates: Sharing Best Practices in Canada. Can. Commun. Dis. Rep. 2016, 42, 243–245. [Google Scholar] [CrossRef]
- Huot, C.; Sauvageau, C.; Tremblay, G.; Dubé, È.; Ouakki, M. Adult Immunization Services: Steps Have to Be Done. Vaccine 2010, 28, 1177–1180. [Google Scholar] [CrossRef]
- Dalla Torre, D.; Burtscher, D.; Sölder, E.; Widschwendter, A.; Rasse, M.; Puelacher, W. The Impact of Sexual Behavior on Oral HPV Infections in Young Unvaccinated Adults. Clin. Oral Investig. 2016, 20, 1551–1557. [Google Scholar] [CrossRef]
- Zoorob, R.; Sidani, M.; Vanbeber, M. Adult and Adolescent Immunizations: When to Recommend the New Vaccines. Infect. Med. 2009, 26, 501. [Google Scholar]
- Maltz, F.; Fidler, B. Updates in Adult Immunizations. J. Nurse Pract. 2020, 16, 218–223. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; DiClemente, R. The vaccine uptake continuum: Applying social science theory to shift vaccine hesitancy. Vaccines 2020, 8, 76. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 25 February 2021).
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for Addressing Vaccine Hesitancy–A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Gagnon, D.; MacDonald, N.E. Strategies Intended to Address Vaccine Hesitancy: Review of Published Reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef] [Green Version]
- Public Health Agency of Canada. Vaccine Coverage Amongst Adult Canadians: Results from the 2016 Adult National Immunization Coverage (aNIC) Survey. Available online: http://www.publications.gc.ca/pub?id=9.859558&sl=0 (accessed on 8 February 2021).
- Zhao, L.; Young, K.; Gemmill, I. Influenza: An Update: Summary of The NACI Seasonal Influenza Vaccine Statement For 2019–2020. Can. Commun. Dis. Rep. 2019, 45, 149. [Google Scholar] [CrossRef]
- Statistics Canada. The 10 Leading Causes of Death, Version Updated November 2015. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2014001/article/11896-eng.htm (accessed on 1 February 2021).
- Schanzer, D.L.; McGeer, A.; Morris, K. Statistical Estimates of Respiratory Admissions Attributable to Seasonal and Pandemic Influenza for Canada. Influenza Other Respir. Viruses 2013, 7, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Schanzer, D.L.; Sevenhuysen, C.; Winchester, B.; Mersereau, T. Estimating influenza deaths in Canada, 1992–2009. PLoS ONE 2013, 8, e80481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubé, E.; Bettinger, J.; Fisher, W.; Naus, M.; Mahmud, S.; Hilderman, T. Improving Vaccination Rates: Vaccine acceptance, hesitancy and refusal in Canada: Challenges and potential approaches. Can. Commun. Dis. Rep. 2016, 42, 246. [Google Scholar] [CrossRef] [PubMed]
- Warrington, R.; Ismail, S. Respiratory Infection: Summary of the NACI Update on Herpes Zoster Vaccines. Can. Commun. Dis. Rep. 2018, 44, 220. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, J.; Pearson Sharpe, J.; Houle, S.K.; Waite, N.M. Time For Harmonization: Pharmacists as Immunizers Across Canadian Jurisdictions. Can. Pharm. J. Ott. 2019, 152, 395–400. [Google Scholar] [CrossRef] [PubMed]
- The Canadian Pharmacists Association. Pharmacists’ Vaccination Authority Across Canada. Available online: http://www.pharmacists.ca/cpha-ca/assets/File/cpha-on-the-issues/Scope_of_Practice_Immunization_Dec2020.pdf (accessed on 8 February 2021).
- Tannenbaum, C.; Tsuyuki, R.T. The Expanding Scope of Pharmacists’ Practice: Implications for Physicians. CMAJ 2013, 185, 1228–1232. [Google Scholar] [CrossRef] [Green Version]
- Canadian Nursing Association and Canadian Medical Association. Joint Position Statement on Scopes of Practice. Available online: https://www.cna-aiic.ca/-/media/cna/page-content/pdf-en/ps66_scopes_of_practice_june_2003_e.pdf?la=en&hash=F346C4473B0C8154811834EEB34BC551805B6154 (accessed on 1 February 2021).
- Hughes, C.A.; Breault, R.R.; Hicks, D.; Schindel, T.J. Positioning Pharmacists’ Roles in Primary Health Care: A Discourse Analysis of the Compensation Plan in Alberta, Canada. BMC Health Serv. Res. 2017, 17, 770. [Google Scholar] [CrossRef] [Green Version]
- Poudel, A.; Lau, E.T.; Kyle, G.J.; Nissen, L.M. Pharmacy practice in Australia and New Zealand. In Encyclopedia of Pharmacy Practice and Clinical Pharmacy; Elsevier: Amsterdam, The Netherlands, 2019; pp. 488–498. [Google Scholar]
- McBane, S.E.; Dopp, A.L.; Abe, A.; Benavides, S.; Chester, E.A.; Dixon, D.L.; Dunn, M.; Johnson, M.D.; Nigro, S.J. Collaborative Drug Therapy Management and Comprehensive Medication Management. Pharmacotherapy 2015, 35, e39–e50. [Google Scholar]
- Raghunandan, R.; Tordoff, J.; Smith, A. Non-Medical Prescribing in New Zealand: An Overview of Prescribing Rights, Service Delivery Models and Training. Ther. Adv. Drug Saf. 2017, 8, 349–360. [Google Scholar] [CrossRef] [Green Version]
- Latter, S.; Blenkinsopp, A. Non-Medical Prescribing: Current and Future Contribution of Pharmacists and Nurses. Int. J. Pharm. Pract. 2011, 19, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Rosado, H.; Bates, I. An Overview of Current Pharmacy Impact on Immunisation: A Global Report; International Pharmaceutical Federation (FIP): The Hague, The Netherlands, 2016. [Google Scholar]
- Isenor, J.; Edwards, N.; Alia, T.; Slayter, K.; MacDougall, D.; McNeil, S.; Bowles, S. Impact of Pharmacists as Immunizers on Vaccination Rates: A Systematic Review and Meta-Analysis. Vaccine 2016, 34, 5708–5723. [Google Scholar] [CrossRef] [PubMed]
- Sepp, K.; Kukk, C.; Cavaco, A.; Volmer, D. How Involvement of Community Pharmacies Improves Accessibility to and Awareness about Flu Vaccination?–An Example From Estonia. Expert Rev. Vaccines 2020, 19, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Baroy, J.; Chung, D.; Frisch, R.; Apgar, D.; Slack, M.K. The Impact of Pharmacist Immunization Programs on Adult Immunization Rates: A Systematic Review and Meta-Analysis. J. Am. Pharm. Assoc. 2016, 56, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, L.A.; Williams, D.M.; Marciniak, M.W.; Weber, D.J. Community Pharmacists as Vaccine Providers. Int. J. Health Gov. 2017, 22, 167–182. [Google Scholar] [CrossRef]
- Tran, M.N.; Bacci, J.L.; Dillon-Sumner, L.; Odegard, P. Enhancing Adult Immunization Care by Community Pharmacists: A Qualitative Analysis of Project VACCINATE. J. Am. Pharm. Assoc. 2020, 61, e19–e25. [Google Scholar] [CrossRef]
- Burt, S.; Hattingh, L.; Czarniak, P. Evaluation of Patient Satisfaction and Experience towards Pharmacist-Administered Vaccination Services in Western Australia. Int. J. Clin. Pharm. 2018, 40, 1519–1527. [Google Scholar] [CrossRef]
- Papastergiou, J.; Folkins, C.; Li, W.; Zervas, J. Community Pharmacist–Administered Influenza Immunization Improves Patient Access to Vaccination. Can. Pharm. J. Ott. 2014, 147, 359–365. [Google Scholar] [CrossRef] [Green Version]
- Lau, E.T.; Rochin, M.E.; DelDot, M.; Glass, B.D.; Nissen, L.M. “There’s No Touching in Pharmacy”: Training Pharmacists for Australia’s First Pharmacist Immunization Pilot. Can. J. Hosp. Pharm. 2017, 70, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattingh, H.L.; Sim, T.F.; Parsons, R.; Czarniak, P.; Vickery, A.; Ayadurai, S. Evaluation of The First Pharmacist-Administered Vaccinations in Western Australia: A Mixed-Methods Study. BMJ Open 2016, 6, e011948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westrick, S.C.; Owen, J.; Hagel, H.; Owensby, J.K.; Lertpichitkul, T. Impact of the RxVaccinate program for pharmacy-based pneumococcal immunization: A cluster-randomized controlled trial. J. Am. Pharm. Assoc. 2016, 56, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Percy, J.N.; Crain, J.; Rein, L.; Hohmeier, K.C. The impact of a pharmacist-extender training program to improve pneumococcal vaccination rates within a community chain pharmacy. J. Am. Pharm. Assoc. 2020, 60, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merks, P.; Religioni, U.; Bilmin, K.; Lewicki, J.; Jakubowska, M.; Waksmundzka-Walczuk, A.; Czerw, A.; Barańska, A.; Bogusz, J.; Plagens-Rotman, K. Readiness and Willingness to Provide Immunization Services after Pilot Vaccination Training: A Survey among Community Pharmacists Trained and Not Trained in Immunization during the COVID-19 Pandemic in Poland. Int. J. Environ. Res. Public Health 2021, 18, 599. [Google Scholar] [CrossRef]
- Poudel, A.; Lau, E.T.; Campbell, C.; Nissen, L.M. Unleashing Our Potential—Pharmacists’ Role in Vaccination and Public Health. Sr. Care Pharm. 2020, 35, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Sim, T.F.; Wright, B.; Hattingh, L.; Parsons, R.; Sunderland, B.; Czarniak, P. A Cross-Sectional Survey of Enhanced and Extended Professional Services in Community Pharmacies: A Pharmacy Perspective. Res. Social. Adm. Pharm. 2020, 16, 511–521. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srirangan, K.; Lavenue, A. Helping Québec Pharmacists Seize the Vaccination Service Opportunity: The Pharmacy Best Practice Workshops. Pharmacy 2021, 9, 51. https://doi.org/10.3390/pharmacy9010051
Srirangan K, Lavenue A. Helping Québec Pharmacists Seize the Vaccination Service Opportunity: The Pharmacy Best Practice Workshops. Pharmacy. 2021; 9(1):51. https://doi.org/10.3390/pharmacy9010051
Chicago/Turabian StyleSrirangan, Kajan, and Arnaud Lavenue. 2021. "Helping Québec Pharmacists Seize the Vaccination Service Opportunity: The Pharmacy Best Practice Workshops" Pharmacy 9, no. 1: 51. https://doi.org/10.3390/pharmacy9010051
APA StyleSrirangan, K., & Lavenue, A. (2021). Helping Québec Pharmacists Seize the Vaccination Service Opportunity: The Pharmacy Best Practice Workshops. Pharmacy, 9(1), 51. https://doi.org/10.3390/pharmacy9010051