
Pharmacist Prescribing for Minor Ailments Service Development: The Experience in Ontario


Abstract
:1. Introduction
2. Ontario: Constructing the Approach
2.1. Defining the Regulatory Framework
2.2. Establishing an Expert Advisory Group
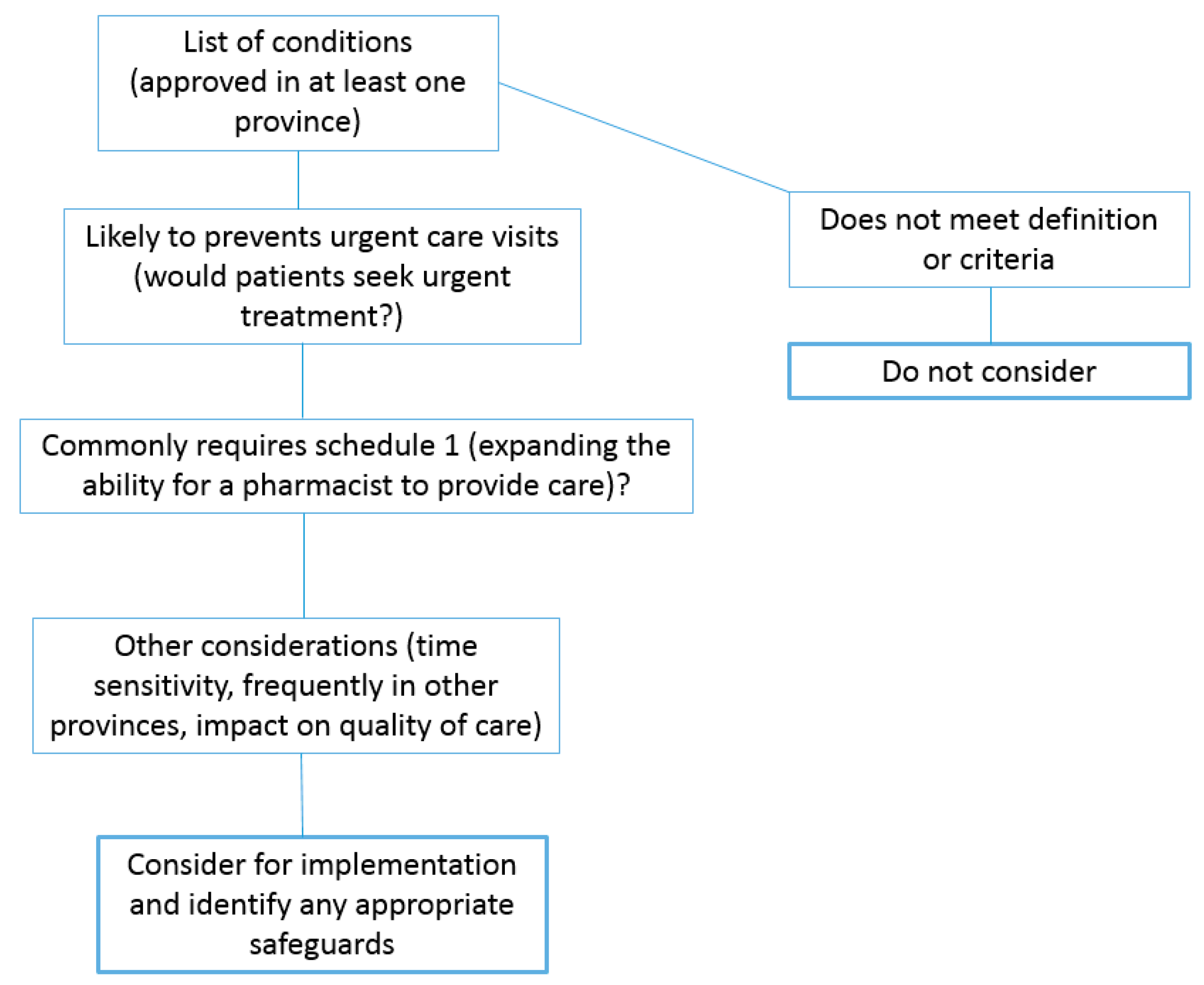
Environmental Scan and Assessment
- usually a short-term condition;
- lab tests are not usually required;
- low risk of treatment masking underlying conditions;
- medication and medical histories can reliably differentiate more serious conditions;
- only minimal or short-term follow-up is required.
2.3. Patient Involvement
2.4. Broad Stakeholder Engagement
3. Ontario: The Final Results
3.1. PPMA Service Components
3.1.1. List of Minor Ailments and Medication Categories
- Urinary tract infection (uncomplicated)
- Dermatitis (atopic/eczema, allergic and contact skin rashes)
- Insect bites (including tick bites) and urticaria (hives)
- Conjunctivitis (bacterial, allergic, viral)
- Allergic rhinitis (nasal symptoms from allergies)
- Candidal stomatitis (oral thrush)
- Herpes labialis (cold sores)
- Hemorrhoids
- Gastroesophageal reflux disease (GERD)
- Dysmenorrhea (menstrual cramps)
- Musculoskeletal sprains and strains
- Impetigo (bacterial skin infection common in children)
3.1.2. Safeguards
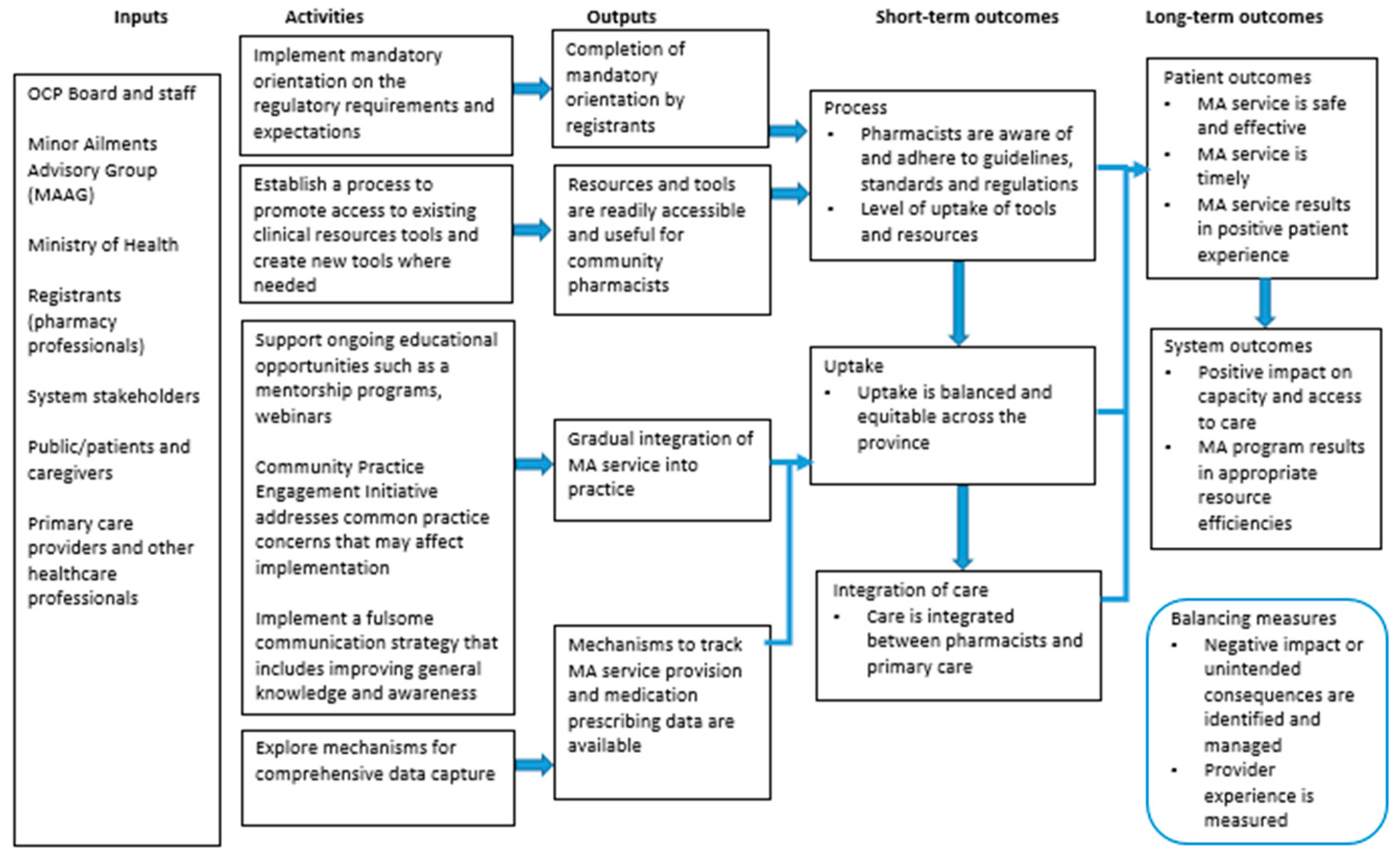
3.1.3. Implementation and Evaluation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- National Statistics. National Association of Pharmacy Regulatory Authorities (NAPRA). Available online: https://napra.ca/national-statistics (accessed on 1 February 2021).
- Taylor, J.G.; Joubert, R. Pharmacist-led minor ailment programs: A Canadian perspective. Int. J. Gen. Med. 2016, 9, 291–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielding, S.; Porteous, T.; Ferguson, J.; Maskrey, V.; Blyth, A.; Paudyal, V.; Barton, G.; Holland, R.; Bond, C.M.; Watson, M.C. Estimating the burden of minor ailment consultations in general practices and emergency departments through retrospective review of routine data in North East Scotland. Fam. Pract. 2015, 32, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Paudyal, V.; Watson, M.C.; Sach, T.; Porteous, T.; Bond, C.M.; Wright, D.J.; Cleland, J.; Barton, G.; Holland, R. Are pharmacy-based minor ailment schemes a substitute for other service providers? A systematic review. Br. J. Gen. Pract 2013, 63, e472-81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paudyal, V.; Hansford, D.; Cunningham, S.; Stewart, D. Pharmacy assisted patient self care of minor ailments: A chronological review of UK health policy documents and key events 1997–2010. Health Policy 2011, 101, 253–259. [Google Scholar] [CrossRef]
- Aly, M.; Garcia-Cardenas, V.; Williams, K.; Benrimoj, S.I. A review of international pharmacy-based minor ailment services and proposed service design model. Res. Social Adm. Pharm. 2018, 14, 989–998. [Google Scholar] [CrossRef]
- Watson, M.C.; Holland, R.; Ferguson, J.; Porteous, T.; Sach, T.; Cleland, J. Community Pharmacy Management of Minor Illness (the MINA Study). In Final Report to Pharmacy Research UK; Pharmacy Research UK: London, UK, 2014; Available online: https://pharmacyresearchuk.org/wp-content/uploads/2014/01/MINA-Study-Final-Report.pdf (accessed on 3 February 2021).
- Watson, M.C.; Ferguson, J.; Barton, G.R.; Maskrey, V.; Blyth, A.; Paudyal, V.; Bond, M.C.; Holland, R.; Porteous, T.; Sach, T.H.; et al. A cohort study of influences, health outcomes and costs of patients’ health-seeking behaviour for minor ailments from primary and emergency care settings. BMJ Open 2015, 5, e006261. [Google Scholar] [CrossRef] [PubMed]
- Scottish Government Health and Social Care Directorates. National Health Service (Scotland) Act 1978: Health Board Additional Pharmaceutical Services (Minor Ailment Service) Amendment Directions 2020. Available online: https://www.sehd.scot.nhs.uk/pca/PCA2020(P)06.pdf (accessed on 1 February 2021).
- Information Services Division. “Prescribing & Medicines: Minor Ailments Service (MAS).” NHS National Services Scotland. Available online: https://www.isdscotland.org/Health-Topics/Prescribing-and-Medicines/Publications/2017-09-26/2017-09-26-Prescribing-MinorAilmentsService-Report.pdf (accessed on 2 February 2021).
- Dineen-Griffin, S.; Garcia-Cardenas, V.; Rogers, K.; Williams, K.; Benrimoj, S.I. Evaluation of a Collaborative Protocolized Approach by Community Pharmacists and General Medical Practitioners for an Australian Minor Ailments Scheme: Protocol for a Cluster Randomized Controlled Trial (in eng). JMIR Res. Protoc. 2019, 8, e13973. [Google Scholar] [CrossRef] [Green Version]
- Sewak, N.; Cairns, J. A modelling analysis of the cost of a national minor ailments scheme in community pharmacies in England. Int. J. Pharm. Pract. 2011, 19, 50. [Google Scholar]
- Business Services Organisation. “Minor Ailments Scheme”. Health and Social Care Board. Available online: http://www.hscbusiness.hscni.net/services/2055.htm (accessed on 1 February 2021).
- Common Ailments Service. Cwm Taf Morgannwg University Health Board. Available online: https://cwmtafmorgannwg.wales/services/pharmacy-medicines-management/common-ailments-service/ (accessed on 1 February 2021).
- Welsh Government. Community Pharmacy Common Ailment Service—Service Specification. Available online: http://www.wales.nhs.uk/sites3/Documents/498/CAS%20Service%20Specification.pdf (accessed on 3 February 2021).
- Dineen-Griffin, S.; Vargas, C.; Williams, K.A.; Benrimoj, S.I.; Garcia-Cardenas, V. Cost utility of a pharmacist-led minor ailment service compared with usual pharmacist care. Cost Eff. Resour. Alloc. 2020, 18, 24. [Google Scholar] [CrossRef]
- Ontario College of Pharmacists. Expanded Scope of Practice. Available online: https://www.ocpinfo.com/about/key-initiatives/expanded-scope-of-practice/ (accessed on 1 September 2020).
- Ontario Ministry of Health and Long-Term Care. First Interim Report from the Premier’s Council on Improving Healthcare and Ending Hallway Medicine. Available online: http://www.health.gov.on.ca/en/public/publications/premiers_council/report.aspx (accessed on 1 February 2021).
- Minor Ailments Advisory Group (MAAG). Summary of Recommendations: Pharmacist Prescribing for Minor Ailments. Ontario College of Pharmacists. Available online: https:/www.ocpinfo.com/wp-content/uploads/2020/12/Minor-Ailments-Advisory-Group-MAAG-Summary-of-Recommendations-Pharmacist-Prescribing.pdf (accessed on 1 February 2021).
- Pharmacy Association of Nova Scotia. Assessing and Prescribing for Minor Ailments. Available online: https://pans.ns.ca/public/pharmacy-services/assessing-prescribing-minor-ailments (accessed on 1 February 2021).
- Nova Scotia College of Pharmacists. Standards of Practice: Prescribing Drugs. Available online: https://www.nspharmacists.ca/wp-content/uploads/2016/05/SOP_PrescribingDrugs.pdf (accessed on 2 February 2021).
- Cramm, D.; Kent, S. Authorization to Prescribe Regulations 2015. Government of Newfoundland and Labrador. Available online: https://www.assembly.nl.ca/legislation/sr/annualregs/2015/nr150073.htm (accessed on 2 February 2021).
- Shearer, B.; Ng, S.; Dunford, D.; Kuo, I.F. Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey. Pharmacy 2018, 6, 82. [Google Scholar] [CrossRef] [Green Version]
- Bishop, A.C.; Boyle, T.A.; Morrison, B.; Barker, J.R.; Zwicker, B.; Mahaffey, T.; Murphy, A. Public perceptions of pharmacist expanded scope of practice services in Nova Scotia. Can. Pharm. J. 2015, 148, 274–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feeley, D. The Triple Aim or the Quadruple Aim? Four Points to Help Set Your Strategy. Institute for Healthcare Improvement. Available online: http://www.ihi.org/communities/blogs/the-triple-aim-or-the-quadruple-aim-four-points-to-help-set-your-strategy (accessed on 3 February 2021).
- Ontario Ministry of Health. Chapter 2: The vision for health care in Ontario. Available online: https://www.ontario.ca/document/healthy-ontario-building-sustainable-health-care-system/chapter-2-vision-health-care-ontario (accessed on 1 February 2021).
- Mansell, K.; Bootsman, N.; Kuntz, A.; Taylor, J. Evaluating pharmacist prescribing for minor ailments. Int. J. Pharm. Pract. 2015, 23, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Research Power Inc. Evaluation of the Provision of Minor Ailment Services in the Pharmacy Setting Pilot Study: Final Report. Pharmacy Association of Nova Scotia (PANS). Available online: https://pans.ns.ca/wp-content/uploads/2013/11/2013-10-17-PANS-report_FINAL.pdf (accessed on 2 February 2021).
- Beahm, N.P.; Nicolle, L.E.; Bursey, A.; Smyth, D.J.; Tsuyuki, R.T. The assessment and management of urinary tract infections in adults: Guidelines for pharmacists. Can. Pharm. J. 2017, 150, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, J.G.; Mansell, K. Patient Feedback on Pharmacist Prescribing for Minor Ailments in a Canadian Province. Inov. Pharm. 2017, 8, 1. [Google Scholar] [CrossRef]
- Alsabbagh, M.W.; Houle, S.K.D. The proportion, conditions, and predictors of emergency department visits that can be potentially managed by pharmacists with expanded scope of practice. Res. Social Adm. Pharm. 2019, 15, 1289–1297. [Google Scholar] [CrossRef]
- Citizen Advisory Group (CAG). Report: Citizen Advisory Group Meeting. Saturday 8 February 2020. Available online: https://citizenadvisorygroup.files.wordpress.com/2020/04/citizen-advisory-group-8-feb-2020-final-report.pdf (accessed on 3 February 2021).
- Minor Ailments. Ontario College of Pharmacists. Available online: https://www.ocpinfo.com/practice-education/expanded-scope-of-practice/minor-ailments/?hilite=%27minor%27%2C%27ailments%27 (accessed on 2 February 2021).
- Public Health Ontario. Ontario Lyme Disease Map 2020 Estimated Risk Areas. Available online: https://www.publichealthontario.ca/-/media/documents/l/2020/lyme-disease-risk-area-map-2020.pdf (accessed on 1 March 2021).
- Aly, M.; Schneider, C.R.; Sukkar, M.B.; Lucas, C. Educational needs of community pharmacy staff in minor ailment service delivery: A systematic scoping review. Curr. Pharm. Teach. Learn. 2020, 12, 1269–1287. [Google Scholar] [CrossRef]
- Nazar, H.; Nazar, Z. Community pharmacy minor ailment services in England: Pharmacy stakeholder perspectives on the factors affecting sustainability. Res. Soc. Adm. Pharm. 2019, 15, 292–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakhla, N.; Black, E.; Abdul-Fattah, H.; Taylor, J. Self-care education across Canadian pharmacy schools: Curriculum survey findings. Can. Pharm. J. 2021, 154, 52–60. [Google Scholar] [CrossRef]
- Mantzourani, E.; Richards, T.G.; Hughes, M.L. New roles in pharmacy—learning from the All Wales Common Ailments Scheme. Int. J. Pharm. Pract. 2016, 24, 298–301. [Google Scholar] [CrossRef]
- Nazar, H.; Nazar, Z.; Yeung, A.; Maguire, M.; Connelly, A.; Slight, S.P. Consensus methodology to determine minor ailments appropriate to be directed for management within community pharmacy (in eng). Res. Social. Adm. Pharm. 2018, 14, 1027–1042. [Google Scholar] [CrossRef] [Green Version]
- Habicht, D.; Ng, S.; Dunford, D.; Shearer, B.; Kuo, I.F. Incorporating assessment and prescribing for ambulatory ailments skills into practice: An environmental scan of continuing education for pharmacist prescribing in Canada. Can. Pharm. J. 2017, 150, 316–325. [Google Scholar] [CrossRef] [Green Version]
- Public Health Agency of Canada. Canadian Antimicrobial Resistance Surveillance System 2017 Report. Government of Canada. Available online: https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-2017-report-executive-summary.html (accessed on 21 February 2021).
- Chief Public Health Officer of Canada’s 2019 Spotlight Report. Handle With Care: Preserving Antibiotics Now and Into the Future. Public Health Agency of Canada. Available online: https://www.canada.ca/content/dam/phac-aspc/documents/corporate/publications/chief-public-health-officer-reports-state-public-health-canada/preserving-antibiotics/Final_CPHO_Report_EN_June6_2019.pdf (accessed on 21 February 2021).
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M., Jr.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, K.P.; Fischer, M.A.; Linder, J.A. Appropriateness of outpatient antibiotic prescribing among privately insured US patients: ICD-10-CM based cross sectional study. BMJ 2019, 364, 5092. [Google Scholar] [CrossRef] [Green Version]
- Booth, J.L.; Mullen, A.B.; Thomson, D.A.M.; Johnston, C.; Galbraith, S.J.; Bryson, S.M.; McGovern, E.M. Antibiotic treatment of urinary tract infection by community pharmacists: A cross-sectional study. Br. J. Gen. Pract. 2013, 63, 244–249. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: London, UK, 2014. [Google Scholar]
- Tsao, N.W.; Lynd, L.D.; Gastonguay, L.; Li, K.; Nakagawa, B.; Marra, C.A. Factors associated with pharmacists’ perceptions of their working conditions and safety and effectiveness of patient care. Can. Pharm. J. 2016, 149, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isenor, J.E.; Minardf, L.V.; Stewart, S.A.; Curran, J.A.; Deal, H.; Rodrigues, G. Identification of the relationship between barriers and facilitators of pharmacist prescribing and self-reported prescribing activity using the theoretical domains framework. Res. Social. Adm. Pharm. 2018, 14, 784–791. [Google Scholar] [CrossRef]
- Paudyal, V.; Cunningham, S.; Gibson Smith, K.; MacLure, K.; Ryan, C.; Cordina, M. Methodological considerations in clinical outcomes assessment of pharmacy-based minor ailments management: A systematic review (in eng). PLoS ONE 2018, 13, e0205087. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Conditions ♾ | Alberta * | Manitoba | New Brunswick | Newfoundland and Labrador | Nova Scotia | Prince Edward Island | Quebec | Saskatchewan | Ontario ** |
|---|---|---|---|---|---|---|---|---|---|
| Acne vulgaris a | X | X | X | X | X | X | X | X | |
| Acute mountain sickness prevention | X | X | |||||||
| Allergic conjunctivitis | X | X | X | X | |||||
| Allergic rhinitis | X | X | X | X | X | X | X | X | X |
| Atopic dermatitis (eczema) b | X | X | X | X | X | X | X | X | X |
| Bacterial conjunctivitis | X | X | X | ||||||
| Calluses and corns | X | X 1 | X | X | X | X | |||
| Contraception (hormonal) | X | X 1 | X 3 | X | X | ||||
| Contact allergic dermatitis c | X | X | X | X | X | X | X | X | |
| Cough | X | X | X | X | X | ||||
| Candidal stomatitis (oral thrush) d | X | X | X | X | X | X | X | X | X |
| Dandruff | X | X | X | X | X | ||||
| Diaper rash/dermatitis, irritant and candidal | X | X | X | ||||||
| Diarrhea (noninfectious) | X | X | X | X | X | ||||
| Dysmenorrhea e | X | X 1 | X | X | X | X | X | X | X |
| Dyspepsia (indigestion) | X | X | X | X | X | X | |||
| Emergency contraception | X | X 1 | X | X | X | X | X | X | |
| Erectile dysfunction | X | X | |||||||
| Folliculitis | X | X | |||||||
| Fungal infections of the skin f | X | X | X | X | X | X | |||
| Gastroesophageal reflux disease (heartburn) | X | X 1 | X | X | X | X | X | X | X |
| Head lice | X | X | |||||||
| Headache g | X | X | X | X | X | X | |||
| Hemorrhoids h | X | X | X | X | X | X | X | X | X |
| Herpes labialis/simplex (cold sores) | X | X 1 | X | X | X | X | X | X | X |
| Herpes zoster (shingles) prevention | X | X 1 | X 2 | X 4 | X 5 | X | X | ||
| Impetigo | X | X 1 | X | X | X | X | X | ||
| Influenza treatment | X | X | X | ||||||
| Insect bites i | X | X | X | X | X | X | X | ||
| Irritant contact dermatitis c | X | X | X | X | |||||
| Joint pain (minor or mild) j | X | X | X | X | X | ||||
| Malaria prevention | X | X 3 | X | ||||||
| Mouth/oral/aphthous ulcers k | X | X | X | X | X | X | X | X | |
| Muscle pain (minor or mild) j | X | X | X | X | X | X | X | ||
| Nasal congestion p | X | X | X | X | X | ||||
| Nausea | X | X | X | X | X | ||||
| Nausea and Vomiting | X | X | X | ||||||
| Nausea/vomiting of pregnancy l | X | X | X | ||||||
| Obesity | X | X | |||||||
| Onychomycosis | X | X | |||||||
| Pinworms/threadworms | X | X 1 | X | X | X | X | X | ||
| Pregnancy (requiring prenatal vitamins) | X | X | |||||||
| Seborrhoeic dermatitis m | X | X | X | ||||||
| Sleep disorders (minor or mild) n | X | X | X | X | X | ||||
| Smoking cessation/nicotine dependence o | X | X | X | X | X | X | X | X | X |
| Sore throat p | X | X | X | X | X | X | |||
| Tinea corporis infection (ringworm) f | X | X 1 | X | X | X | X | X | X | |
| Tinea cruris infection (jock itch) f | X | X 1 | X | X | X | X | X | X | |
| Tinea pedis infection (athlete’s foot) f | X | X | X | X | X | X | X | ||
| Upper respiratory tract conditions q | X | X | X | ||||||
| Urinary tract infection (UTIs) r | X | X 1 | X | X 4 | X | X | X | X | |
| Urticaria i | X | X | X | X | X | X | X | X | |
| Vaginal candidiasis (yeast infection) | X | X 1 | X | X | X | X | X | ||
| Vasomotor rhinitis | X | X | |||||||
| Viral conjunctivitis | X | X | |||||||
| Warts s | X | X 1 | X | X | X | X | |||
| Xerophthalmia (dry eyes) | X | X | X | X | X |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakhla, N.; Shiamptanis, A. Pharmacist Prescribing for Minor Ailments Service Development: The Experience in Ontario. Pharmacy 2021, 9, 96. https://doi.org/10.3390/pharmacy9020096
Nakhla N, Shiamptanis A. Pharmacist Prescribing for Minor Ailments Service Development: The Experience in Ontario. Pharmacy. 2021; 9(2):96. https://doi.org/10.3390/pharmacy9020096
Chicago/Turabian StyleNakhla, Nardine, and Anastasia Shiamptanis. 2021. "Pharmacist Prescribing for Minor Ailments Service Development: The Experience in Ontario" Pharmacy 9, no. 2: 96. https://doi.org/10.3390/pharmacy9020096
APA StyleNakhla, N., & Shiamptanis, A. (2021). Pharmacist Prescribing for Minor Ailments Service Development: The Experience in Ontario. Pharmacy, 9(2), 96. https://doi.org/10.3390/pharmacy9020096