
Experience of Patients with COPD of Pharmacists’ Provided Care: A Qualitative Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants: Sampling and Recruitment
2.3. Data Collection
2.4. Data Analysis
2.5. Trustworthiness and Reflexivity
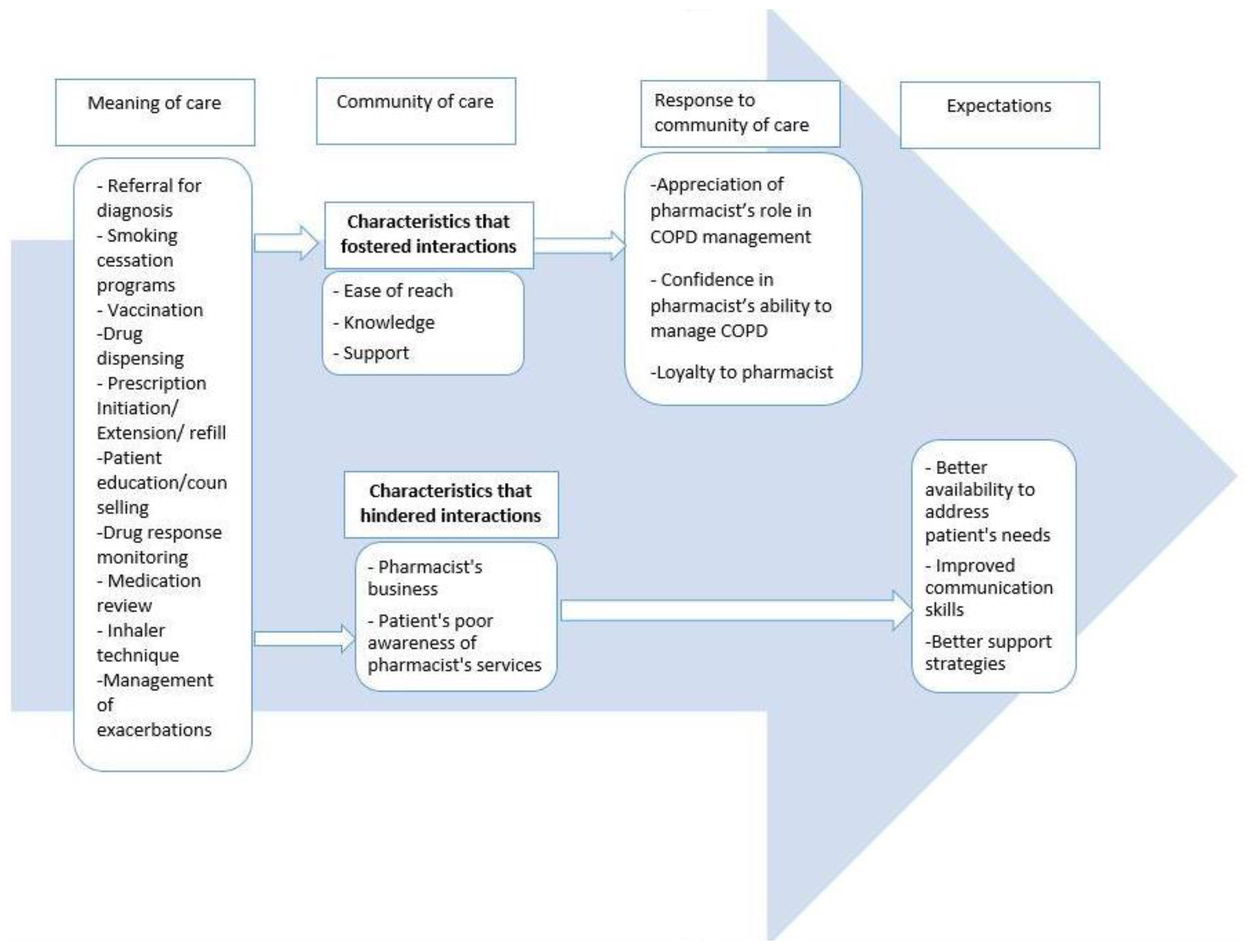
3. Results
3.1. Meaning of Care
‘I did have symptoms, but I didn’t know that it was COPD. I was always phlegmy, a lot of—wheezing, I guess, when I was laying down or resting… and tired. No energy… thinking back now, knowing now, there was all the symptoms, because, you don’t really have that intimate one-on-one conversation with your pharmacist about, “Hey, you know what?” So, I didn’t go to my pharmacist and say, “Hey, you know what, I’m wheezing today and having troubles. I bought over the counter cough syrup or halls or something like that, Vicks. I bought a humidifier…a couple of times when I did get Bronchitis, I went and got antibiotics for it. But, nobody put it together that I had COPD’.(Participant 5, Male)
‘Based on my symptoms and how much difficulty I would have with my asthma symptoms, and thinking that there was potentially something else going on… she did recommend that I get a lung function test done’.(Participant 11, Female)
‘So now because a lot of the cessation aids don’t help me we discuss a lot of the mental barriers and blocks and stuff like that regarding quitting; and that’s really where my struggle. It’s not so much the physical addiction but more the mental addiction and the anxiety of ‘what am I going to do if I can’t smoke’’. And so she helps talk me through a lot of that. We’ve spent a lot of time on that consultation. It hasn’t been fully successful yet but we keep working on it’.(Participant 11, Female)
‘So she can prescribe—I just think they prescribe certain medications, that you could continue for say one month, or a few days, or something like that, provided that probably you’re already on it, and you’re running out, and you can’t get to see the doctor, so they’ll provide a kind of a stopgap’.(Participant 7, Male)
‘When I go in to see him and I tell him I need this or that, he’s very interactive and suggests some of—like he’ll look at my other medications and say “You know what, maybe you might not want to take that because if you take it for too long it can affect asthma, so let’s try—” Like I mean he’s always educating me which is important because I didn’t know that and I now I do. So now I have a choice to decide whether or not I change it and, of course, I’m going to change it because the last thing I need is something else to worry about, you know. That to me, that’s important’.(Participant 1, Female)
‘Well, she’s always got lots of questions. Every time I go in to pick up refills she has a lot of questions… they would ask me almost pill by pill, medication by medication how it was working and how much was I taking. They would maybe make suggestions to change the amount I was taking or the time I was taking it or something like that…She lets me know what could go wrong and is it? You know, is that happening to you? No, it isn’t. Okay, that’s good and then she goes through the benefits and is that happening to you? Yeah. Good. So, you know, she gives you both sides of the medication story’.(Participant 8, Male)
‘Yeah, and if you say you’re experiencing this, well then you can go to the doctor and say, well, I’ve talked to the pharmacist, and they’re like, you know, suggesting this. And then they say, what do you think? So—and they say either yay or nay, and if they do say yay, they normally write you a prescription. So—but then again, too, that’s just confirmation that the pharmacist is correct. And so it’s a system—kind of a system with checks and balances, so to speak’.(Participant 7, Male)
3.2. Community of Care
3.2.1. Characteristics That Fostered Interactions
‘She cares on more than just a professional level… she’s always asking about how I’m doing not just about my medical issues or things like that. She’s concerned about why the symptoms are the way they are and if some other aspect of my lifestyle or health is impacting it’.(Participant 11, Female)
‘The other day, she was back in the corner, and she had a mortar and pestle, or whatever, and she was mixing something up. And all I said was double, double, toil and trouble. And she says, what, are you calling me a witch? And I said, no, I’m just quoting Shakespeare. So she’s got a sense of humor, I got a sense of humor… So we do have a nice rapport back and forth. So lots of fun. It’s always a joy to go in there’.(Participant 7, Male)
3.2.2. Characteristics That Hindered Interactions
‘…There’s always a line and they’re all running around trying to get everything done especially where I go. They don’t have a lot of time to spend with each individual person so…if I’m picking them up right away I have to wait sometimes an hour or more because there’s so many people ahead of me; so I think they’re very, very busy’.(Participant 12, Female)
‘I didn’t even know that pharmacists could give you a prescription without a doctor’s okay… Well, I don’t think they can prescribe a prescription for me without a doctor’s note, cause they don’t know my—they don’t have my health records, I don’t think. So, how would they know what to prescribe?’(Participant 6, Female)
3.3. Participants’ Response to Community of Care
‘Since I first met her she’s just been great… she’s probably the best in the city, that’s a doctor’s opinion. If she closed her doors, I’d be in dire straits. It sounds odd when you say that about somebody you deal with. But when you find somebody that you deal with whether its medicine or buying clothes or cars and you trust them, you don’t want them to leave. Knowing that I’ve got who I have behind me in my medical situation I feel well protected’.(Participant 9, Male)
‘I’ve been going to her for 25 years. I go out of my way because the hours that the pharmacy is open are limited compared to big commercial companies or, you know, the grocery stores that have the pharmacies in them. Honestly the reason I haven’t left is I like the personal attention that she… part of it I think is the longevity of the relationship that we’ve had, also she’s very personable and asks questions and it’s not just a service where you go in put your prescriptions in and you get your meds and out the door’.(Participant 11, Female)
3.4. Expectations
‘This is how you take the medication, this is what you’re supposed to do whether you rinse or gargle or whatever after. And this is how you actually do, like, inhale”. That’s how I would like it. Not just, “Here you go, this can cause this, do you understand? See you later”. I would like it if they went more into show you how to use it, explain more, give you some examples of some side effects. Because if they ask you, “Okay, do you have any side effects?” how do you know? I just might not be feeling well this day or, “Hey, I got a rash”, but I didn’t—it might affiliate with that’.(Participant 5, Male)
‘And then I tried [name of pharmacy], because they had the low dispensing fee, one of the lowest, and they were horrible. They were just horrible. They didn’t understand what you were saying. They didn’t have your medication ready. You know, there was, like a hassle after hassle’.(Participant 10, Female)
‘I don’t understand all the words that he says. I don’t understand everything. Sometimes, not often, because a lot of times—I think people, and myself included, feel less intelligent if somebody’s talking very big words or whatever, and so you’ll just agree, and even if you don’t understand them, you’ll just agree’.(Participant 5, Male)
4. Discussion
4.1. Limitations
4.2. Implications for Research and Practice
- Patients appreciate and anticipate meaningful interaction with their pharmacists about their overall health, the use of medications, managing side effects, and assistance with smoking cessation;
- Patients appreciate pharmacists being involved in prevention and timely management of exacerbations, e.g., pharmacist prescribing, standing orders for antibiotics;
- Patients value pharmacists being an active collaborator with other healthcare providers, including the patient’s physician (family or specialist), e.g., in addressing prescription errors, patients’ plan of care, and in the initiation of appropriate therapy;
- Patients value pharmacists connecting patients with resources, e.g., rehab programs;
- Patients appreciate pharmacists’ knowledge of them, i.e., recent hospitalisations, medication use that might signal an underlying condition (COPD), and other challenges (personal or otherwise) which may impair COPD management;
- Patients identified the importance of having knowledge of COPD, assessment of COPD symptoms and risk factors pre-disease diagnosis, and early disease identification.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Guide
- How were you diagnosed with COPD and what role did your pharmacist play in your diagnosis?
- Who helps you manage your COPD?
- Tell me about your experiences with your pharmacists’ provided care.
- What is the pharmacist role in caring for you?
- Imagine that your pharmacist can do more, what would help you to manage your COPD?
- Can you tell me more about that?
- How did that make you feel?
- Could you give me an example?
- Why was that important to you?
Appendix B. Participants’ Demographic Questionnaire
- Gender: Male ____ Female ______ Prefer not to say _______
- Year of birth: ______?
- What year were you diagnosed with COPD?
- How often do you visit a community pharmacy to access health services?
- □
- More than once a month
- □
- Monthly
- □
- Once in two months
- □
- Once in three months
- □
- Less than every three months
- □
- Never
- In the past year (past 12 months), how many times have you experienced a COPD flare-up which required either additional medications (e.g., antibiotic), a visit to the emergency room, or hospitalization?
- □
- 0
- □
- 1
- □
- 2
- □
- 3
- □
- Other: _____
- Do you have any of the following health conditions? Please select all that apply.
- □
- Diabetes
- □
- High blood pressure
- □
- Lung cancer
- □
- Sleep apnea
- □
- Heart disease
- □
- Asthma
- □
- Musculoskeletal disorder
- □
- Other ________________________________________________________
Appendix C. COREQ Checklist
| Item No | Guide Guides/Description | Location in Manuscript/Reported on Page No | |
| Domain 1: Research team and reflexivity | |||
| Personal Characteristics | |||
| Interviewer/facilitator | 1 | Which author/s conducted the interview or focus group? TM and OI conducted interviews 1 to 4 together. MQ and OI conducted interviews 7 to 9 together while OI conducted interviews 5,6,10 to 12 alone. | Methods-3 |
| Credentials | 2 | What were the researcher’s credentials? OI-BPharm MSc candidate MQ-RD MSc PhD TM-BS Pharm, PhD | Title page |
| Occupation | 3 | What was their occupation at the time of the study? OI-Master’s student MQ-Qualitative researcher TM-Assistant Professor | Methods-5 |
| Gender | 4 | Was the researcher male or female? Females | Methods-5 |
| Experience and training | 5 | What experience or training did the researcher have? OI-Took a graduate study course on qualitative research MQ-Over 11 years of experience as a qualitative researcher TM—moderate level of experience with qualitative research; formal training in qualitative research | Methods-5 |
| Relationship with participants | |||
| Relationship established | 6 | Was a relationship established prior to study commencement? No | |
| Participant knowledge of the interviewer | 7 | What did the participants know about the researcher? e.g., personal goals, reasons for doing the research Participants were briefed on the purpose of the study. Participants also reviewed the study information sheet before they gave written informed consent to be involved in the study. | Methods-3 |
| Interviewer characteristics | 8 | What characteristics were reported about the inter viewer/facilitator? e.g., Bias, assumptions, reasons and interests in the research topic OI and TM acknowledged to be non-practicing pharmacists with interests in improving pharmacy care of COPD patients | Methods-5 |
| Domain 2: Study design | |||
| Theoretical framework | |||
| Methodological orientation and Theory | 9 | What methodological orientation was stated to underpin the study? e.g., grounded theory, discourse analysis, ethnography, phenomenology, content analysis Qualitative descriptive methodology with qualitative content analysis | Methods-2 |
| Participant selection | |||
| Sampling | 10 | How were participants selected? e.g., purposive, convenience, consecutive, snowball Convenience | Methods-3 |
| Method of approach | 11 | How were participants approached? e.g., face-to-face, telephone, mail, email Recruitment involved use of posters and face-to-face invitation | Methods-3 to 4 |
| Sample size | 12 | How many participants were in the study? 12 | Methods-3 |
| Non-participation | 13 | How many people refused to participate or dropped out? Reasons? Two. One person declined to participate in the interview and another individual could not be interviewed due to the global pandemic. | Methods-3 |
| Setting | |||
| Setting of data collection | 14 | Where was the data collected? e.g., home, clinic, workplace Majority of the participants were interviewed at home. Other settings for data collection were: a meeting room at the University of Alberta and a pulmonary rehabilitation centre. | Methods-3 |
| Presence of non-participants | 15 | Was anyone else present besides the participants and researchers? A non-participant (participant’s spouse) was present during one of the interviews | Methods-3 |
| Description of sample | 16 | What are the important characteristics of the sample? e.g., demographic data, date Interviews were conducted from 1 October 2019 to 8 January 2020. Twelve participants- six females and six males. Their ages ranged from 46 to 85 years and they had been living with COPD between two to 22 years. | Methods-3 Results-5 |
| Data collection | |||
| Interview guide | 17 | Were questions, prompts, guides provided by the authors? Was it pilot tested? Interviews were semi-structured, using a guide which is attached as an appendix. The interview guide was iterated during the data collection process to enrich the collected data. | Methods-3 |
| Repeat interviews | 18 | Were repeat interviews carried out? If yes, how many? No | |
| Audio/visual recording | 19 | Did the research use audio or visual recording to collect the data? All interviews were audio-recorded and transcribed | Methods-3 |
| Field notes | 20 | Were field notes made during and/or after the interview or focus group? Field notes were made during and after the interviews. | Methods-3 |
| Duration | 21 | What was the duration of the inter views or focus group? The semi-structured interviews ranged from 20 to 114 min. | Methods-3 |
| Data saturation | 22 | Was data saturation discussed? In the methods section, we discussed data saturation was reached by the 12th interview. | Methods-3 |
| Transcripts returned | 23 | Were transcripts returned to participants for comment and/or correction No | |
| Domain 3: analysis and findings | |||
| Data analysis | |||
| Number of data coders | 24 | How many data coders coded the data? At the start, OI and MQ independently coded a transcript and discussed consistency of the codes and the coding process. Thereafter, OI coded all the transcripts, with supervision and feedback by MQ. | Methods-4 |
| Description of the coding tree | 25 | Did authors provide a description of the coding tree? Yes | Methods-4 |
| Derivation of themes | 26 | Were themes identified in advance or derived from the data? Themes were derived from the data | Methods-4 |
| Software | 27 | What software, if applicable, was used to manage the data? NVivo 12 software | Methods-4 |
| Participant checking | 28 | Did participants provide feedback on the findings? No | |
| Reporting | |||
| Quotations presented | 29 | Were participant quotations presented to illustrate the themes/findings? Was each quotation identified? e.g., participant number Comments were supported with direct quotes from participants who were anonymised by participant number and sex. | Results-6 to 13 |
| Data and findings consistent | 30 | Was there consistency between the data presented and the findings? Yes | |
| Clarity of major themes | 31 | Were major themes clearly presented in the findings? Yes | |
| Clarity of minor themes | 32 | Is there a description of diverse cases or discussion of minor themes? No | |
References
- Statistics Canada. Health Trends (Data from 2014). Statistics Canada Catalogue No. 82-213-XWE Ottawa. Available online: http://www12.statcan.gc.ca/health-sante/82-213/index.cfm?Lang=ENG (accessed on 26 February 2020).
- Bednarek, M.; Maciejewski, J.; Wozniak, M.; Kuca, P.; Zielinski, J. Prevalence, severity and underdiagnosis of COPD in the primary care setting. Thorax 2008, 63, 402–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHS National Institute for Clinical Excellence. Chronic Obstructive Pulmonary Disease: Management of Chronic Obstructive Pulmonary Disease in Adults in Primary and Secondary Care, Clinical Guideline 12; National Institute for Clinical Excellence: London, UK, 2004. [Google Scholar]
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [Green Version]
- Feenstra, T.L.; Van Genugten, M.L.L.; Hoogenveen, R.T.; Wouters, E.F.; Mölken, M.P.M.H.R.-V. The Impact of Aging and Smoking on the Future Burden of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2001, 164, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Roche, N.; Perez, T.; Neukirch, F.; Carré, P.; Terrioux, P.; Pouchain, D.; Ostinelli, J.; Suret, C.; Meleze, S.; Huchon, G. High prevalence of COPD symptoms in the general population contrasting with low awareness of the disease. Rev. Mal. Respir. 2011, 28, e58–e65. [Google Scholar] [CrossRef]
- Labonté, L.E.; Tan, W.C.; Li, P.Z.; Mancino, P.; Aaron, S.D.; Benedetti, A.; Chapman, K.R.; Cowie, R.; FitzGerald, M.; Hernandez, P.; et al. Undiagnosed COPD contributes to the burden of health care utilization: Data from the CanCOLD study. Am. J. Respir. Crit. Care Med. 2016, 194, 285–298. [Google Scholar] [CrossRef]
- Institute of Medicine Crossing the Quality Chasm. Crossing the Quality Chasm: A New Health System for the 21st Century; The National Academies Press: Washington, DC, USA, 2001.
- Olson, O.W. Patient-Centeredness in Pharmacist Practice: Filling a Foundation for What Counts to Patients. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2020. Available online: https://conservancy.umn.edu/bitstream/handle/11299/216353/Olson_umn_0130E_21514.pdf?sequence=1&isAllowed=y (accessed on 10 June 2021).
- Fathima, M.; Naik-Panvelkar, P.; Saini, B.; Armour, C.L. The role of community pharmacists in screening and subsequent management of chronic respiratory diseases: A systematic review. Pharm. Pract. 2013, 11, 228–245. [Google Scholar] [CrossRef] [Green Version]
- Tsuyuki, R.T.; Beahm, N.P.; Okada, H.; Al Hamarneh, Y.N. Pharmacists as accessible primary health care providers: Review of the evidence. Can. Pharm. J. 2018, 151, 4–5. [Google Scholar] [CrossRef] [Green Version]
- Todd, A.; Copeland, A.; Husband, A.; Kasim, A.S.; Bambra, C. Access all areas? An area-level analysis of accessibility to general practice and community pharmacy services in England by urbanity and social deprivation. BMJ Open 2015, 5, e007328. [Google Scholar] [CrossRef] [Green Version]
- Van Der Molen, T.; Van Boven, J.F.M.; Maguire, T.; Goyal, P.; Altman, P. Optimizing identification and management of COPD patients—Reviewing the role of the community pharmacist. Br. J. Clin. Pharmacol. 2016, 83, 192–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chisholm-Burns, M.A.; Lee, J.K.; Spivey, C.A.; Slack, M.; Herrier, R.N.; Hall-Lipsy, E.; Zivin, J.G.; Abraham, I.; Palmer, J.; Martin, J.; et al. US Pharmacists’ Effect as Team Members on Patient Care. Med. Care 2010, 48, 923–933. [Google Scholar] [CrossRef]
- Abraham, O.; Schleiden, L.J.; Brothers, A.L.; Albert, S.M. Managing sleep problems using non-prescription medications and the role of community pharmacists: Older adults’ perspectives. Int. J. Pharm. Pract. 2017, 25, 438–446. [Google Scholar] [CrossRef]
- Mishriky, J.; Stupans, I.; Chan, V. Expanding the role of Australian pharmacists in community pharmacies in chronic pain management—A narrative review. Pharm. Pract. 2019, 17, 1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Haqan, A.A.; Al-Taweel, D.M.; Awad, A.; Wake, D.J. Pharmacists’ Attitudes and Role in Diabetes Management in Kuwait. Med. Princ. Pract. 2017, 26, 273–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, X.; Zhou, S.; Luo, D.; Zhao, X.; Zhou, Y.; Cui, Y. Effect of pharmacist-led interventions on medication adherence and inhalation technique in adult patients with asthma or COPD: A systematic review and meta-analysis. J. Clin. Pharm. Ther. 2020, 45, 904–917. [Google Scholar] [CrossRef] [PubMed]
- Poitras, M.-E.; Maltais, M.-E.; Bestard-Denommé, L.; Stewart, M.; Fortin, M. What are the effective elements in patient-centered and multimorbidity care? A scoping review. BMC Health Serv. Res. 2018, 18, 446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, S.M. Living with failing lungs: The doctor-patient relationship. Fam. Pract. 2001, 18, 430–439. [Google Scholar] [CrossRef] [Green Version]
- Gysels, M.; Higginson, I.J. Access to Services for Patients with Chronic Obstructive Pulmonary Disease: The Invisibility of Breathlessness. J. Pain Symptom Manag. 2008, 36, 451–460. [Google Scholar] [CrossRef]
- Olson, A.W.; Vaidyanathan, R.; Stratton, T.P.; Isetts, B.J.; Hillman, L.A.; Schommer, J.C. Patient-Centered Care preferences & expectations in outpatient pharmacist practice: A three archetype heuristic. Res. Soc. Adm. Pharm. 2021. [Google Scholar] [CrossRef]
- Olufemi-Yusuf, D.T.; Gabriel, S.B.; Makhinova, T.; Guirguis, L.M. “Being in Control of My Asthma Myself” Patient Experience of Asthma Management: A Qualitative Interpretive Description. Pharmacy 2018, 6, 121. [Google Scholar] [CrossRef] [Green Version]
- Siaw, M.Y.L.; Toh, J.H.; Lee, J.Y.-C. Patients’ perceptions of pharmacist-managed diabetes services in the ambulatory care and community settings within Singapore. Int. J. Clin. Pharm. 2018, 40, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Young, D.C.; Autry, E.; Zobell, J.T.; Kormelink, L.; Homa, K.; Sabadosa, K.A.; Kanga, J.; Anstead, M.; Kuhn, R. Patients and families experience with pharmacist care at cystic fibrosis foundation accredited clinics. Pediatr. Pulmonol. 2019, 54, 1216–1224. [Google Scholar] [CrossRef] [PubMed]
- Bajorek, B.V.; LeMay, K.; Magin, P.J.; Roberts, C.; Krass, I.; Armour, C. Management of hypertension in an Australian community pharmacy setting—Patients’ beliefs and perspectives. Int. J. Pharm. Pract. 2017, 25, 263–273. [Google Scholar] [CrossRef]
- Sandelowski, M. What’s in a name? Qualitative description revisited. Res. Nurs. Health 2009, 33, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Barrett, D.; Twycross, A. Data collection in qualitative research. Evid. Based Nurs. 2018, 21, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, C.; Atkinson, S.; Doody, O. Employing a Qualitative Description Approach in Health Care Research. Glob. Qual. Nurs. Res. 2017, 4, 2333393617742282. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; Bunce, A.; Johnson, L. How Many Interviews Are Enough? Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Graneheim, U.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- MacDermid, J.C.; Walton, D.M.; Bobos, P.; Lomotan, M.; Carlesso, L. A Qualitative Description of Chronic Neck Pain has Implications for Outcome Assessment and Classification. Open Orthop. J. 2016, 10, 746–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. Eur. J. Gen. Pract. 2018, 24, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Lamb, G.S.; Huttlinger, K. Reflexivity in Nursing Research. West. J. Nurs. Res. 1989, 11, 765–772. [Google Scholar] [CrossRef]
- GF MacDonald Centre for Lung Health, Edmonton General Continuing Care Centre-Covenant Health. Available online: www.covenanthealth.ca/hospitals-care-centres/edmonton-general-continuing-care-centre/gf-macdonald-centre-for-lung-health/ (accessed on 16 November 2020).
- Anderson, C.; Blenkinsopp, A.; Armstrong, M. Feedback from community pharmacy users on the contribution of community pharmacy to improving the public’s health: A systematic review of the peer reviewed and non-peer reviewed literature 1990–2002. Health Expect. 2004, 7, 191–202. [Google Scholar] [CrossRef]
- Ogunbayo, O.J.; Schafheutle, E.I.; Cutts, C.; Noyce, P.R. Self-care of long-term conditions: Patients’ perspectives and their (limited) use of community pharmacies. Int. J. Clin. Pharm. 2017, 39, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Esmaeili, M.; Cheraghi, M.A.; Salsali, M. Cardiac patients’ perception of patient-centred care: A qualitative study. Nurs. Crit. Care 2014, 21, 97–104. [Google Scholar] [CrossRef]
- Guirguis, L.M.; AlGhurair, S.A.; Simpson, S.H. What elements of the patient-pharmacist relationship are associated with patient satisfaction? Patient Prefer. Adherence 2012, 6, 663–676. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.B.; Petrakis, B.A.; Gillespie, C.; Solomon, J.L.; Park, A.M.; Ourth, H.; Morreale, A.; Rose, A. Knowing the patient: A qualitative study on care-taking and the clinical pharmacist-patient relationship. Res. Soc. Adm. Pharm. 2016, 12, 78–90. [Google Scholar] [CrossRef]
- Kember, J.; Hodson, K.; James, D.H. The public’s perception of the role of community pharmacists in Wales. Int. J. Pharm. Pract. 2018, 26, 120–128. [Google Scholar] [CrossRef]
- Majchrowska, A.; Bogusz, R.; Nowakowska, L.; Pawlikowski, J.; Piątkowski, W.; Wiechetek, M. Public Perception of the Range of Roles Played by Professional Pharmacists. Int. J. Environ. Res. Public Health 2019, 16, 2787. [Google Scholar] [CrossRef] [Green Version]
- Barry, M.J.; Edgman-Levitan, S. Shared Decision Making—The Pinnacle of Patient-Centered Care. N. Engl. J. Med. 2012, 366, 780–781. [Google Scholar] [CrossRef] [Green Version]
- Nitadpakorn, S.; Farris, K.B.; Kittisopee, T. Factors affecting pharmacy engagement and pharmacy customer devotion in community pharmacy: A structural equation modeling approach. Pharm. Pract. 2017, 15, 999. [Google Scholar] [CrossRef]
- Hassali, M.A.; Palaian, S.; Shafie, A.A.; Ibrahim, M.I.M. Perceptions and Barriers Towards Provision of Health Promotion Activities Among Community Pharmacists in The State of Penang, Malaysia. J. Clin. Diagn. Res. 2009, 3, 1562–1568. [Google Scholar]
- Koehler, T.; Brown, A. Documenting the evolution of the relationship between the pharmacy support workforce and pharmacists to support patient care. Res. Soc. Adm. Pharm. 2017, 13, 280–285. [Google Scholar] [CrossRef]
- Horon, K.; Pro, T.H.; Gorman, S.K.; Con, S.H. Should Pharmacy Technicians Provide Clinical Services or Perform Patient Care Activities in Areas without a Pharmacist? Can. J. Hosp. Pharm. 2010, 63, 391–394. [Google Scholar] [CrossRef] [Green Version]
- Andreski, M.; Myers, M.; Gainer, K.; Pudlo, A. The Iowa new practice model: Advancing technician roles to increase pharmacists’ time to provide patient care services. J. Am. Pharm. Assoc. 2018, 58, 268–274.e1. [Google Scholar] [CrossRef]
- Merks, P.; Świeczkowski, D.; Jaguszewski, M.J. Patients’ perception of pharmaceutical services available in a community pharmacy among patients living in a rural area of the United Kingdom. Pharm. Pract. 2016, 14, 774. [Google Scholar] [CrossRef] [Green Version]
- Shrank, W.H.; Avorn, J. Educating Patients About Their Medications: The Potential and Limitations of Written Drug Information. Health Aff. 2007, 26, 731–740. [Google Scholar] [CrossRef] [Green Version]
- ASHP. guidelines on pharmacist-conducted patient education and counseling. Am. J. Health Pharm. 1997, 54, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Tashkin, N. Smoking Cessation in Chronic Obstructive Pulmonary Disease. Semin. Respir. Crit. Care Med. 2015, 36, 491–507. [Google Scholar] [CrossRef]
- Jordan, R.; Lam, K.B.H.; Cheng, K.K.; Miller, M.R.; Marsh, J.L.; Ayres, J.G.; Fitzmaurice, D.; Adab, P. Case finding for chronic obstructive pulmonary disease: A model for optimising a targeted approach. Thorax 2010, 65, 492–498. [Google Scholar] [CrossRef] [Green Version]
- Blackstock, F.C.; ZuWallack, R.; Nici, L.; Lareau, S.C. Why Don’t Our Patients with Chronic Obstructive Pulmonary Disease Listen to Us? The Enigma of Nonadherence. Ann. Am. Thorac. Soc. 2016, 13, 317–323. [Google Scholar] [CrossRef]
- Martin, A.; Badrick, E.; Mathur, R.; Hull, S. Effect of ethnicity on the prevalence, severity, and management of COPD in general practice. Br. J. Gen. Pract. 2012, 62, e76–e81. [Google Scholar] [CrossRef] [Green Version]
- Howarth, H.D.; Peterson, G.M.; Jackson, S.L. Does rural and urban community pharmacy practice differ? A narrative systematic review. Int. J. Pharm. Pract. 2020, 28, 3–12. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Meaning Unit | Condensed Unit | Code | Category | Theme |
|---|---|---|---|---|
| It’s really easy, like I go to the pharmacy and so it’s really easy for me to get any of the information I need. | Easy to reach | Ease of reach | Characteristics fostering interactions | Community of care |
| …I can’t get an appointment with the doctor until the next week, well then I can go to my pharmacist… | Short wait time | |||
| it’s easier to talk to your pharmacist, because a doctor, you got to wait, and then go in. | Easier access | |||
| She was so proud of him and she would encourage him I’m proud of you | Encouraging | Support | ||
| She’ll phone me and ask how I’m feeling. | Follow up | |||
| Just caring, concerned, very nice lady | Empathy | |||
| Yeah just I would go in and whine and she would tell me what to change or do and how often. | Shoulder to lean on | |||
| There might be other pharmacists that are not quite as busy that would have more time to interact. | Busy to interact | Pharmacists busyness | Characteristics hindering interactions | |
| Do you know, they’re so crazy busy there. How can they—they’re just so busy. | No time | |||
| They don’t have a lot of time to spend with each individual person so… I don’t know. | No time | |||
| I didn’t even know that pharmacists could give you a prescription without a doctor’s okay. | Don’t know | Participants’ awareness of pharmacy services |
| Gender | Age (Years) | Years of Living with COPD | Site of Recruitment | Smoking Status | Frequency of Pharmacy Visit | |
|---|---|---|---|---|---|---|
| 1 | Female | 64 | 7 | PRC | Former Smoker | 2 to 4 visits a month |
| 2 | Male | 61 | 8 | PRC | Former Smoker | >5 times per month |
| 3 | Female | 76 | 6 | PRC | Former Smoker | 2 to 4 visits a month |
| 4 | Male | 75 | 4 | PRC | Former Smoker | Less than every 3 months |
| 5 | Male | 51 | 2 | PRC | Former Smoker | 2 to 4 visits a month |
| 6 | Female | 85 | 8 | PRC | Former Smoker | Once in three months |
| 7 | Male | 72 | 5 | CP | Former Smoker | Monthly |
| 8 | Male | 77 | 22 | CP | Former smoker | Monthly |
| 9 | Male | 75 | 12 | CP | Former Smoker | Monthly |
| 10 | Female | 66 | 6 | CP | Current smoker | Monthly |
| 11 | Female | 46 | 4 | CP | Current smoker | 2 to 4 visits a month |
| 12 | Female | 67 | 10 | CP | Current smoker | Monthly |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idowu, O.; Makhinova, T.; Quintanilha, M.; Yuksel, N.; Schindel, T.J.; Tsuyuki, R.T. Experience of Patients with COPD of Pharmacists’ Provided Care: A Qualitative Study. Pharmacy 2021, 9, 119. https://doi.org/10.3390/pharmacy9030119
Idowu O, Makhinova T, Quintanilha M, Yuksel N, Schindel TJ, Tsuyuki RT. Experience of Patients with COPD of Pharmacists’ Provided Care: A Qualitative Study. Pharmacy. 2021; 9(3):119. https://doi.org/10.3390/pharmacy9030119
Chicago/Turabian StyleIdowu, Omowumi, Tatiana Makhinova, Maira Quintanilha, Nese Yuksel, Theresa J. Schindel, and Ross T. Tsuyuki. 2021. "Experience of Patients with COPD of Pharmacists’ Provided Care: A Qualitative Study" Pharmacy 9, no. 3: 119. https://doi.org/10.3390/pharmacy9030119
APA StyleIdowu, O., Makhinova, T., Quintanilha, M., Yuksel, N., Schindel, T. J., & Tsuyuki, R. T. (2021). Experience of Patients with COPD of Pharmacists’ Provided Care: A Qualitative Study. Pharmacy, 9(3), 119. https://doi.org/10.3390/pharmacy9030119