1. Introduction
Globally, cancer is the second leading cause of mortality accounting for approximately 9.6 million deaths [
1]. Breast cancer is the most common malignancy affecting women worldwide [
2]. In the United States (U.S.), breast cancer is the most commonly diagnosed cancer after skin cancers, with one in eight (13%) women being diagnosed with an invasive type of breast cancer during their lifetime [
3]. According to the American Cancer Society’s [
4] recent projected estimates, there will be approximately 284,200 new cases and 44,130 deaths attributed to breast cancer in the U.S. in 2021. The differential risk of breast cancer by nativity, racial, and ethnic characteristics was also reported with Asian American women bearing a disproportionate burden [
5,
6].
The incidence of breast cancer has been growing with a rate of 94 cases per 100,000 among Asian American women residing in the U.S. [
5,
7]. Previous reports confirmed that the odds of survival were associated with the Asian ethnicity overall [
8]. An analysis of this limited SEER registry data from 2019 indicated that there was a total of 47,401 Asian/Pacific Islander women diagnosed with invasive breast cancer between 2012 and 2016 [
3]. With regard to the nativity of Asian American women, 132 cases of women with diagnosed breast cancer were compared with 438 Asian American without breast cancer diagnosis [
6]. The results of the study suggested that the breast cancer risk is higher among immigrant Asian American women compared with their US-born counterparts or those who have lived less than 50% of their life in the U.S. [
6]. The rate of survival also varied across racial and ethnic groups, which highlights the need of detecting breast cancers at an early stage with the help of primary and secondary levels of prevention, including awareness and screening.
Mammography is a screening procedure that provides early diagnosis, which can lead to treatment and reduced premature mortality due to breast cancer (Centers for Disease Control & Prevention (CDC)) [
9]. However, the use of mammograms as a screening method is still a debatable issue due to the problems of false positives, over-diagnosis, and over-treatment [
10]. Additionally, health authorities differ in their stances on mammography recommendations across age groups. Four primary authorities in the U.S. proposed guidelines on mammography: American College of Obstetricians and Gynecologists (ACOG), U.S. Preventive Services Task Force, American Cancer Society (ACS), and National Comprehensive Cancer Network (NCCN) [
11]. There seems to be some general agreement in these four sets of guidelines that women ages 45–54 years should undergo annual mammograms, and this guideline was used for our study.
To our best knowledge, there are no national data available that summarize the rates of mammography screening among Asian American women through a country-wide population-based survey. However, some small-scale studies have reported low rates of mammography uptake [
12]. For instance, a study of Korean American women reported that 22.2% of women ages 45–49 years and 29% of women ages 50–54 years had a mammogram in the past year [
12]. According to a 2008 Behavioral Risk Factor Surveillance System (BRFSS) data-based study, 60.3% of Asian American women over the age of 40 years had mammograms in the past year, which was the lowest among all the groups studied [
13]. However, the estimates of mammography uptake or utilization are not yet available. Some studies reported regional differences across the U.S. for the mammography screening rates among Asian American women. For instance, a pooled weighted data analysis from five cycles of the California Health Interview Survey conducted between 2001 and 2009, reported an increase in mammograms across all ages in Asian American women from 76–82% from 2001 to 2009 [
14]. There is a caveat to this finding; the response rate to this survey was quite low (17.7% to 37.7% in different cycles), which emphasizes the need to conduct additional research pertaining to mammography screening utilization among Asian American women. The Asian American community is increasing rapidly in the U.S. and the present healthcare system and health research are not catering to the needs of this diverse community [
13]. In order to meet the growing needs and address the gap in the literature for this underserved minority group, this study is being undertaken [
13]. The findings of this study will help in designing behavior change interventions to increase mammography uptake or utilization among Asian American women.
Several factors were known to affect the utilization of mammography screening among Asian American women. Some determinants that are associated with increased rates of mammography screening in Asian American women are having (1) U.S. citizenship [
15], (2) longer residency in the U.S. [
14,
16], (3) a college education [
14,
17], (4) knowledge of the guidelines [
16], (5) health insurance [
13,
14], (6) a primary care provider who recommended a mammogram [
17,
18,
19], (7) a routine health check-up in the past year [
13], and (8) knowing someone with a history of breast cancer and/or having undergone mammography [
16]. Some factors that are barriers to getting mammograms among Asian American women are (1) being of Muslim religion [
19,
20], (2) perceived religious discrimination [
19], (3) impingement on modesty [
19], (4) being less acculturated [
21], and (5) logistical barriers [
22]. It is important to note that not all Asian Americans are a monolithic entity and there are variations among the determinants based on national origin.
There are few interventions that promote mammography among Asian American women. Some of the intervention approaches that have been used are the patient navigator care management model [
23], community workshops [
24], medical interpretation services for limited English proficiency patients [
25], use of primary care providers [
26], religiously tailored interventions [
27,
28], store-based education [
29], web-based education delivery [
30] among others. Further, very few studies have used behavioral theories as a basis for these interventions. For instance, Boxwala and colleagues [
17] and Lee and colleagues [
30] used the health belief model, Wu and West [
31] used the transtheoretical model, and Sun and colleagues [
32] used the prospect theory. Non-theory-based approaches and utilization of older theories do not improve the predictability of the health behavior change. Such approaches lead to doing “same old same old” without advancement of the scientific discipline of health behavior research (HBR). Furthermore, most of the older approaches were about behavior acquisition and newer fourth-generation approaches have been developed that promote behavior “change” instead of mere acquisition and lead to development of precision interventions [
33,
34]. The first-generation models were about knowledge transfer, the second-generation models were about skill acquisition, third generation models were about behavior acquisition, and the fourth-generation models are about behavior change utilizing constructs from multiple evidence-based theories [
33,
34]. Therefore, there is a need to utilize recent fourth-generation health behavior change models to explain the correlates of mammography screening and design precise interventions to promote mammography in this understudied and underserved population of Asian American women.
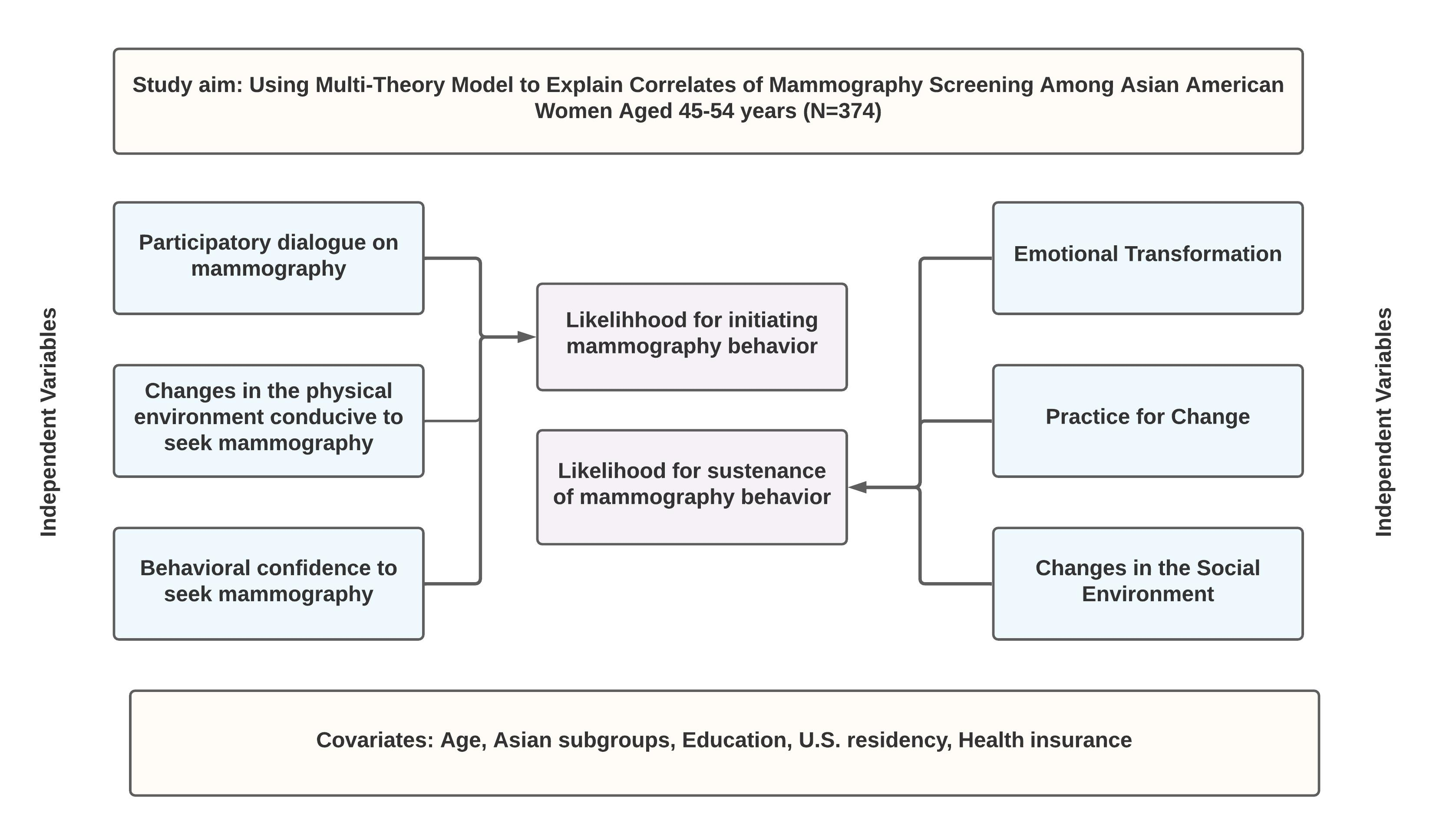
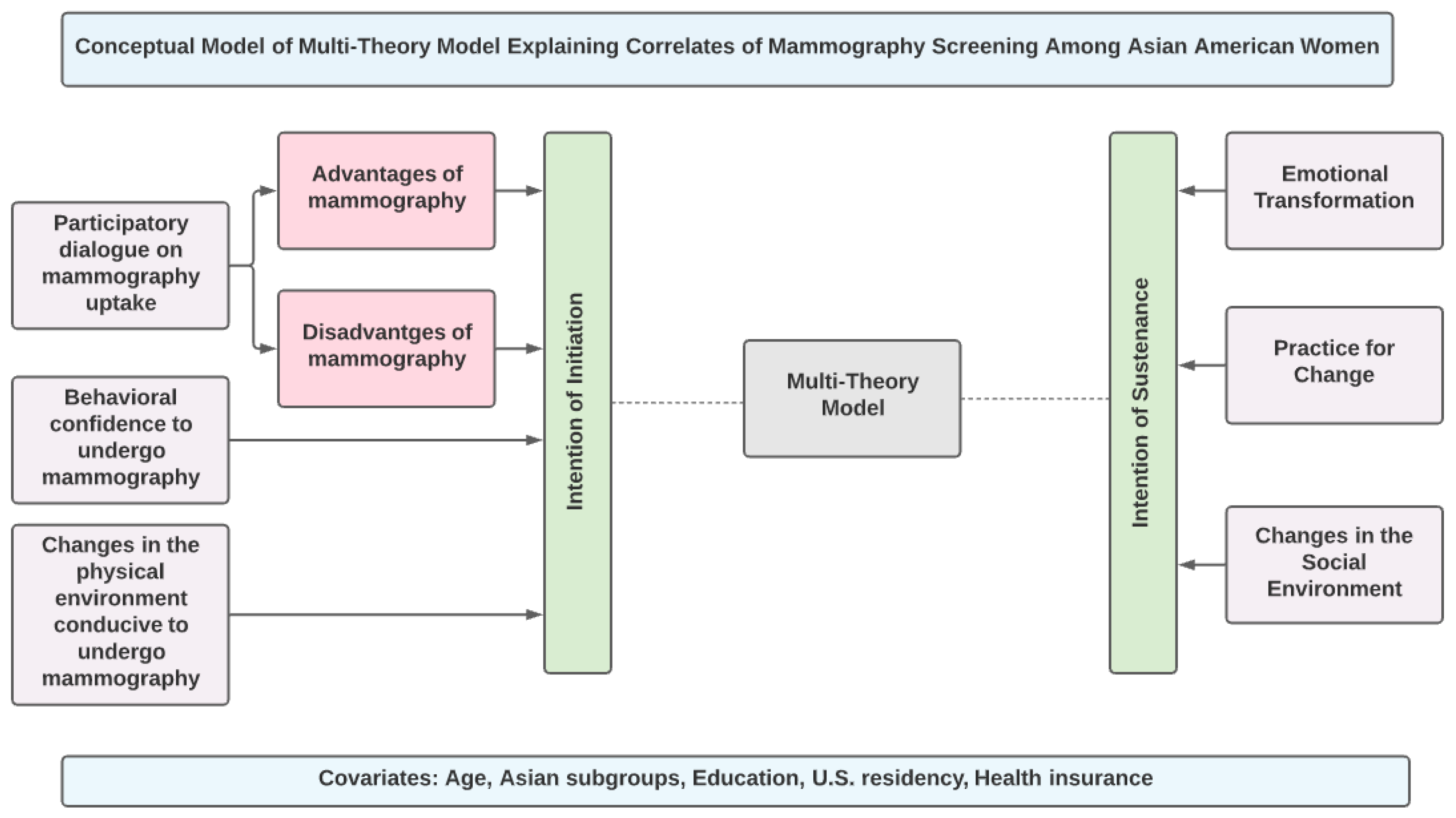
One emerging fourth-generation model is the multi-theory model (MTM) of health behavior change [
33,
34]. This model breaks down the complex health behavior change into two components of initiation and maintenance with three explanatory constructs for each of the two components (
Figure 1). This model has been used in qualitative [
35,
36], cross-sectional [
37,
38,
39,
40], and experimental studies [
41,
42,
43] with a variety of behaviors in different priority populations but has not been applied to understanding mammography screening behaviors. Therefore, the current study aims to utilize the multi-theory model (MTM) of health behavior change to explain the correlates of mammography screening in a sample of Asian American women between the ages of 45–54 years.
4. Discussion
The aim of this study was to explain the correlates of mammography screening using the paradigm of MTM in a nationally representative sample of Asian American women aged 45–54 years. The study found that for Asian American women
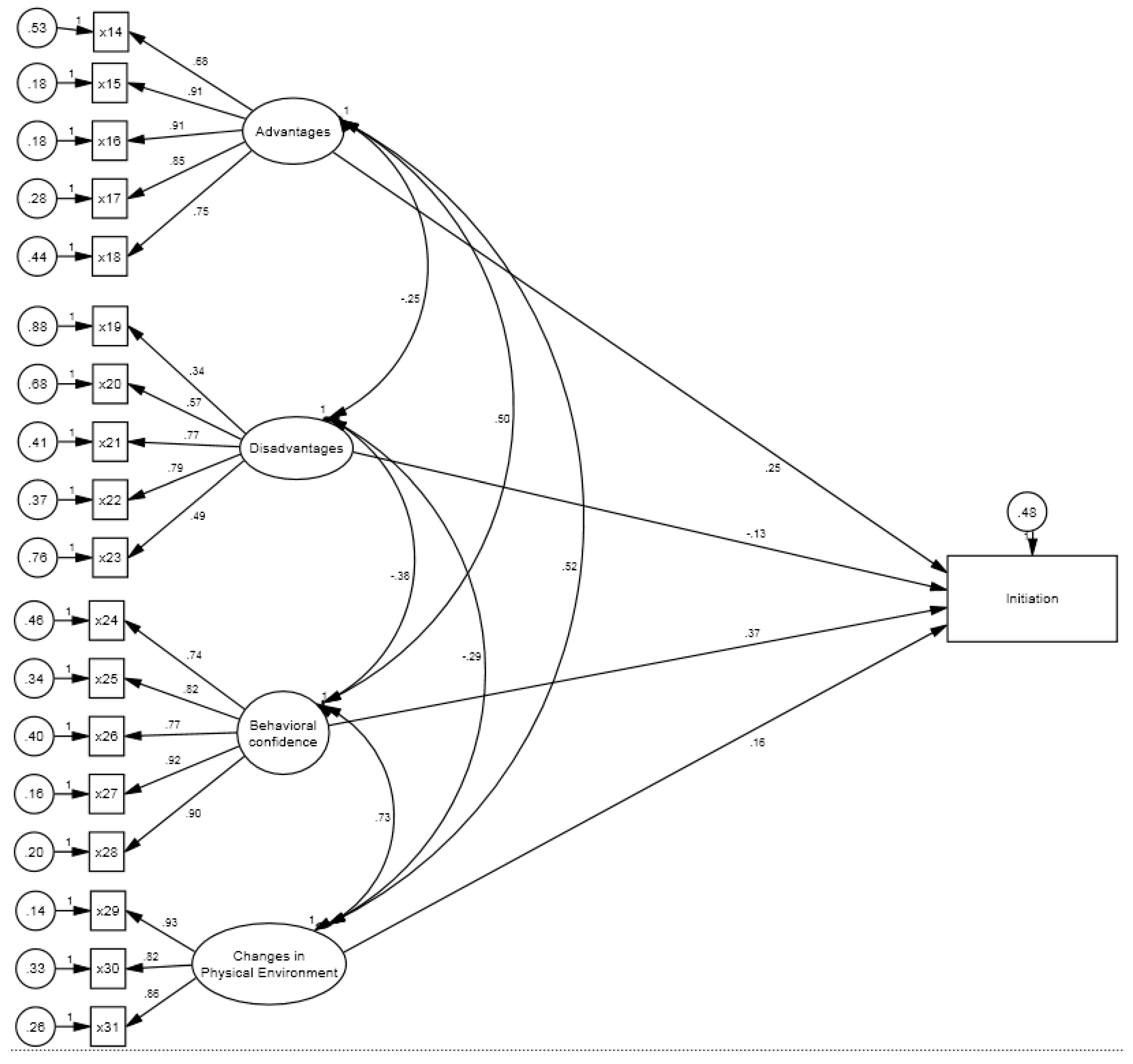
Who had received mammograms in the past 12 months as per recommendations, all three constructs of the MTM, namely, participatory dialogue (β = 0.156,
p < 0.05), behavioral confidence (β = 0.236,
p < 0.001), and changes in the physical environment (β = 0.426,
p < 0.001) were statistically significant and crucial in their decision to initiate getting the mammogram. In addition, health insurance status (β = 0.127,
p < 0.05) was also a significant contributor which is also supported by previous literature [
13,
14]. However, age, Asian subgroups, education, and U.S. residency were not significant contributors in the final model. The final model accounted for a substantial proportion of variance (49.9%) in explaining the decision to receive mammography, which is considered high in social and behavioral sciences [
33,
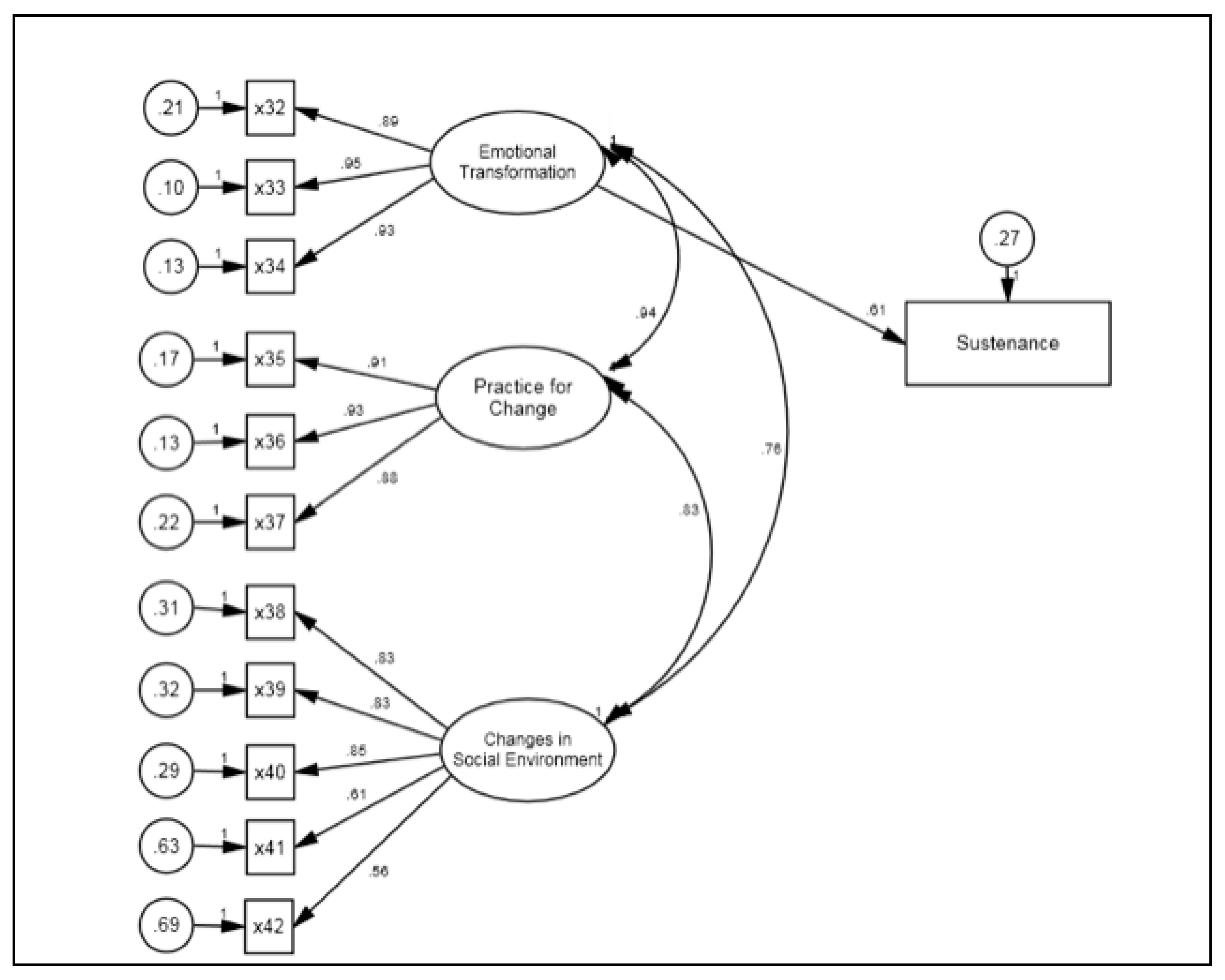
34]. While this analysis was not necessary because this group of women were indeed adhering to the guidelines, it was conducted to confirm that the putative MTM constructs are indeed crucial in achieving the starting of the behavior. The study also found that the MTM constructs of emotional transformation (β = 0.437,
p < 0.001) and practice for change (β = 0.303,
p < 0.001) were significant for maintaining the repeated behavior of getting mammograms and were responsible for 53.9% of the variance, which again is substantial [
33,
34]. Similar significant correlates of MTM were observed in the group of Asian American women who had not received a mammogram in the past 12 months, where participatory dialogue (β = 0.294,
p < 0.001) and behavior confidence (β = 0.310,
p < 0.001) accounted for 28.6% of the variance in the intention to get mammograms. It is worth noting that the construct of changes in physical environment which was significant for those following mammography recommendations was not significant for those not following the recommendations which is indicative of the barriers that this group may be encountering. These need to be addressed by interventions that promote mammography in Asian American women. Regarding the intention for getting repeat annual mammograms (sustenance), all MTM constructs of sustenance emotional transformation (β = 0.478,
p < 0.001), practice for change (β = 0.192,
p < 0.05) changes in the social environment (β = 0.165,
p < 0.05) were significant contributors accounting for 57.4% of the variance, which is quite considerable [
33,
34]. It is important to note that all the constructs of MTM are significant in their putative role of explaining continuation of mammography behavior for those Asian American women not following recommendations thus underscoring the relevance of the MTM in designing interventions to promote mammography.
It is worth noting that in this nationally representative sample of Asian American women aged 45–54 years, 46.8% of them had not received a mammogram as per the recommendations of getting one every year [
11]. These findings are similar to those from the BRFSS data that found that 39.7% of Asian American women over 40 years had not received mammograms [
13]. This is a sizable number of Asian American women who are not following the recommendations, underscoring the need for educational and policy efforts in promoting mammography screening to this subgroup of the population.
On close examination of each construct of MTM in its role associated with mammography screening among Asian American women aged 45–54 years old, we found several important outcomes. First, the participatory dialogue had, as expected, a significantly higher mean score (8.04 ± 5.3) among those who had received a mammogram as per recommendations compared to those who had not (3.86 ± 5.36) (
p < 0.001). Clearly, those who were convinced of the advantages of getting a mammography screening were motivated to get it. This is also supported by previous studies on determinants of mammography in Asian American women [
14,
15,
16,
17,
18,
19]. However, on hierarchical regression, the construct was found to be significant among those who were adhering to the recommendations but was not significant for those who were not adhering, after adding the construct of changes in the physical environment. This may point to the relative importance of changes in the physical environment construct which has also been supported in the literature in the form of access to health insurance [
13,
14] or the recommendations from health care providers [
17,
18,
19].
The second construct of MTM, behavioral confidence for initiating mammography screening, had the mean score that was significantly higher for those who had mammograms (14.91 ± 3.98) compared with those who had not had mammograms (10.05 ± 4.95) (
p < 0.001). It was also a significant predictor in the regression models. Previous studies have not examined the extent of the role of this construct, as most of the studies have not utilized behavioral theories for studying determinants of mammography screening among Asian American women [
17,
18,
19]. However, other studies, with other behaviors and other target populations, lend support to this construct of behavioral confidence as playing a significant role in the decision whether to seek mammograms or not [
38,
39,
40].
The third MTM construct of changes in the physical environment for initiating the mammography screening had a mean score that was significantly higher for those who had mammograms (10.12 ± 2.23) compared with those who had not had mammograms (8.01 ± 3.09) (
p < 0.001). It was also a significant predictor in regression models. As discussed earlier, there is evidence from previous research that aspects of the physical environment are very important for Asian American women to seek mammography [
13,
14,
17,
18,
19]. There is clearly a need to help Asian American women overcome logistical barriers that prevent them from seeking mammography screening [
22].
For getting repeated annual mammograms (sustenance), the first MTM construct that was significant was emotional transformation. The mean score for this construct was significantly higher for those who had mammograms (9.42 ± 2.65) compared to those who had not had mammograms (5.02 ± 3.26) (
p < 0.001). It was also a significant predictor in the regression models. Previous studies have not examined the extent of the role of this construct in improving adherence to mammography screening recommendations among Asian American women because this is a relatively new conceptualization where feelings are purported to be used for goal setting in behavior change [
33,
34]. However, its role has shown to be important with other behaviors and with other target populations [
37,
38,
39,
40] so there is a need to use this construct in planning educational interventions that promote mammography screening among Asian American women.
The mean score on the construct for practice for change, which is another construct that predicts maintenance of behavior, was significantly higher for those who had mammograms (8.85 ± 2.55) compared with those who had not had mammograms (4.82 ± 3.14) (
p < 0.001). However, on hierarchical regression, the construct was found to be significant among those who were adhering to the recommendations but was not significant for those who were not adhering, after adding the construct of changes in the social environment. This may point to the relative importance of changes in the social environment construct which may play a greater role in the Asian American culture. The role of friends and family members and what they think is an important influence in the lives of Asian Americans. This phenomenon has not been studied extensively in relation to mammography screening among Asian American women, but Somanchi and colleagues [
16] found that knowing someone with a history of breast cancer and/or having undergone mammography was a determinant in getting a mammogram for Asian American women. Therefore, this provides support to our conjecture about changes in the social environment playing a greater role. As predictable based on MTM, the mean score of the construct of changes in the social environment was also significantly higher for those who had mammograms (13.16 ± 4.71) compared with those who had not had mammograms (8.69 ± 4.40) (
p < 0.001). The role of this MTM construct is also supported from research with other behaviors in other target populations [
38,
39]. There is a need to garner support from social influences in educational programs that promote mammograms among Asian American women.
Since the Asian American community is not a monolithic entity, we collected data on the Asian subgroups. In our sample, the largest representation was from Chinese Americans (41.2%) followed by Filipino Americans (15.8%), followed by South Asian Americans (13.6%) which is more or less representative of the distribution of Asian Americans in the U.S. However, we did not find any significant explanatory potential of these subgroup classifications on predicting potential utilization of mammography screening when MTM constructs are included in the modeling. Future researchers may want to reexamine it more carefully. Previous studies have noted religion, especially being a Muslim, as being a deterrent for getting mammography screening [
19,
20]. In our sample only nine (2.4%) Asian American women practiced Islam, so we could not analyze this subgroup given the constraints of the small sample size. Future researchers may want to oversample this subgroup to discern if religion indeed is a putative determinant of mammography screening when MTM constructs are taken into consideration.
4.1. Implications for Practice
There is a need for both theory-based educational interventions and policy measures that promote mammography screening among Asian American women particularly in the 45–54 age group. The educational interventions can be delivered in primary care settings, OBGYN clinics, community organizations with which Asian American women are associated, faith-based organizations specific to various religions embraced by the Asian American women community, social media, and directed mHealth interventions specifically geared toward this subgroup. MTM can serve as a promising theoretical paradigm in designing and evaluating such interventions. The construct of participatory dialogue in educational interventions can be built by underscoring advantages such as early detection of breast cancer, having peace of mind for self and family, possibility of early treatment, and reduction in premature mortality. Potential barriers such as discomfort, invasion on modesty, inconvenience, and fear of getting a false positive must be discussed and reduced to the extent possible in educational interventions. The construct of behavioral confidence can be fostered through exploration of sources of confidence, using role models, and using stepwise strategies in overcoming barriers. The construct of changes in the physical environment can be mobilized through resources support and reminders. The construct of emotional transformation can be channelized in educational interventions by appealing to the feelings of Asian American women and harnessing these into concrete goals of getting timely mammograms, helping overcome self-doubt, and remaining motivated. The construct of practice for change can be operationalized by encouraging Asian American women to keep records and have reminder systems, overcoming barriers, and making alternate plans if faced with obstacles. Finally, the construct of changes in the social environment must be used by educational programs where family, friends, and healthcare providers should be encouraged to promote, remind, and help with mammography screening.
4.2. Strengths and Limitations
This study is among the few studies that are based on a behavioral theory to decipher determinants of mammography screening in the high-risk Asian American women community. The study collected data on a nationally representative adequately powered sample representing all subgroups of Asian American women aged 45–54 years. The study utilized a contemporary fourth-generation paradigm of MTM. The psychometric validation of the tool used in the study was done meticulously. However, there were also some limitations to this study. Self-reports were utilized to collect information about mammography. Objective data using medical records could have been used to provide more accuracy. The cross-sectional nature of the design always limits causal inferences because the data on the independent variables (MTM constructs) and dependent variables (intentions) are collected at the same point in time. Future research must look into longitudinal designs. Finally, as mentioned earlier, we did not have adequate representation of the Muslim Asian American women in our sample, so we could not examine the role of MTM constructs while controlling for religion.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}



